
Can Mammography and Magnetic Resonance Imaging Predict the Preoperative Size and Nuclear Grade of Pure Ductal Carcinoma In Situ?

 ,
,
Abstract
1. Introduction
2. Materials and Methods
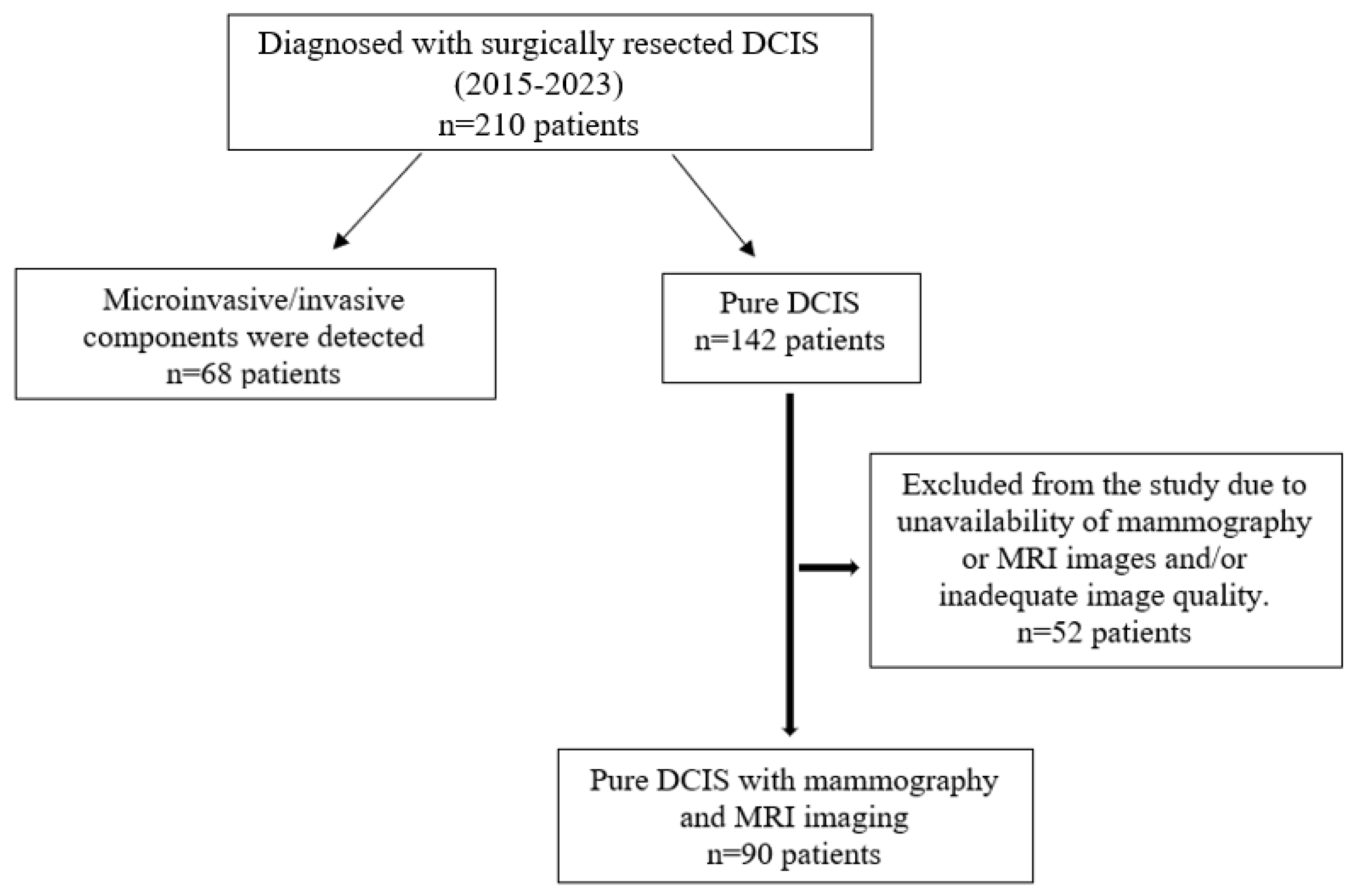
2.1. Patient Selection
2.2. Breast Imaging Technique
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
3.1. Mammographic Findings
3.2. Magnetic Resonance Imaging Findings
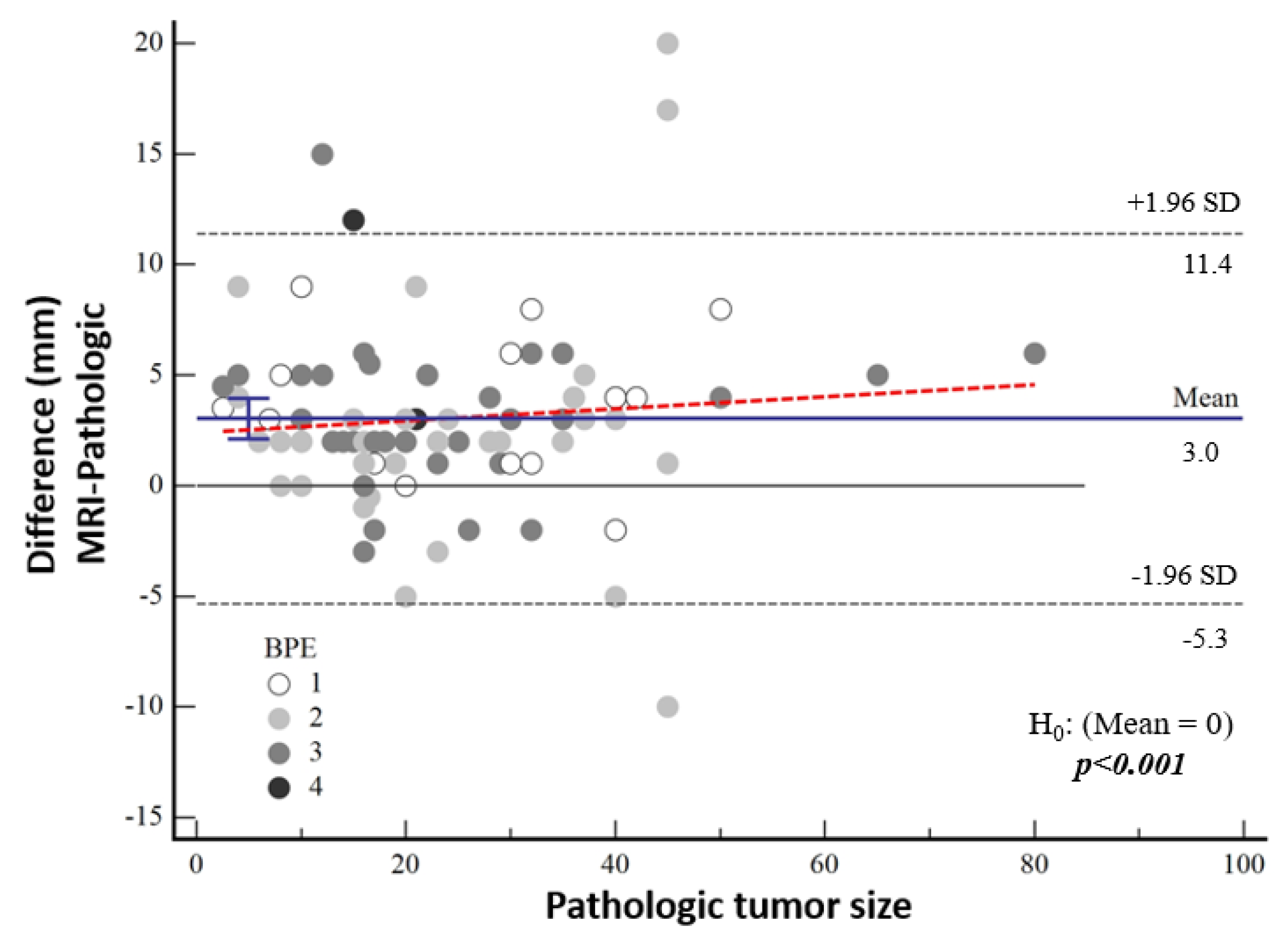
3.3. Comparison of Imaging Methods and Pathological Size
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| DCIS | Ductal carcinoma in situ |
| MRI | Magnetic resonance imaging |
| BIRADS | Breast Imaging Reporting and Database System |
| NME | Non-mass enhancement |
| DWI | Diffusion-weighted imaging |
| TR | Time to repetition |
| TE | Time to echo |
| ADC | Apparent diffusion coefficient |
References
- Badve, S.S.; Gökmen-Polar, Y. Ductal carcinoma In Situ of breast: Update 2019. Pathology 2019, 51, 563–569. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ernster, V.L.; Barclay, J.; Kerlikowske, K.; Grady, D.; Henderson, I.C. Incidence of and treatment for ductal carcinoma In Situ of the breast. JAMA 1996, 275, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Luiten, J.D.; Voogd, A.C.; Luiten, E.J.; Duijm, L.E. Trends in incidence and tumour grade in screen-detected ductal carcinoma In Situ and invasive breast cancer. Breast Cancer Res. Treat. 2017, 166, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Singh, B. Ductal Carcinoma In Situ—Pathological Considerations. Curr. Breast Cancer Rep. 2020, 12, 107–117. [Google Scholar] [CrossRef]
- Fowler, A.M. Survival outcomes for women with ductal carcinoma In Situ in the era of supplemental screening. Radiology 2019, 292, 49–50. [Google Scholar] [CrossRef]
- Youngwirth, L.M.; Boughey, J.C.; Hwang, E.S. Surgery versus monitoring and endocrine therapy for low-risk DCIS: The COMET trial. Bull. Am. Coll. Surg. 2017, 102, 62–63. [Google Scholar]
- Elshof, L.E.; Tryfonidis, K.; Slaets, L.; van Leeuwen-Stok, A.E.; Skinner, V.P.; Dif, N.; Pijnappel, R.M.; Bijker, N.; Rutgers, E.J.T.; Wesseling, J. Feasibility of a prospective, randomised, open-label, international multicentre, phase III, non-inferiority trial to assess the safety of active surveillance for low risk ductal carcinoma In Situ-the LORD study. Eur. J. Cancer 2015, 51, 1497–1510. [Google Scholar] [CrossRef]
- Francis, A.; Thomas, J.; Fallowfield, L.; Wallis, M.; Bartlett, J.M.; Brookes, C.; Roberts, T.; Pirrie, S.; Gaunt, C.; Young, J.; et al. Addressing overtreatment of screen detected DCIS; the LORIS trial. Eur. J. Cancer 2015, 51, 2296–2303. [Google Scholar] [CrossRef]
- Preibsch, H.; Beckmann, J.; Pawlowski, J.; Kloth, C.; Hahn, M.; Staebler, A.; Wietek, B.M.; Nikolaou, K.; Wiesinger, B. Accuracy of Breast Magnetic Resonance Imaging Compared to Mammography in the Preoperative Detection and Measurement of Pure Ductal Carcinoma In Situ: A Retrospective Analysis. Acad. Radiol. 2019, 26, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Holland, R.; Hendriks, J.H. Microcalcifications associated with ductal carcinoma In Situ: Mammographic-pathologic correlation. Semin. Diagn. Pathol. 1994, 11, 181–192. [Google Scholar]
- Hofvind, S.; Iversen, B.F.; Eriksen, L.; Styr, B.M.; Kjellevold, K.; Kurz, K.D. Mammographic morphology and distribution of calcifications in ductal carcinoma In Situ diagnosed in organized screening. Acta. Radiol. 2011, 52, 481–487. [Google Scholar] [CrossRef]
- Barreau, B.; de Mascarel, I.; Feuga, C.; MacGrogan, G.; Dilhuydy, M.-H.; Picot, V.; Dilhuydy, J.-M.; de Lara, C.T.; Bussières, E.; Schreer, I. Mammography of ductal carcinoma In Situ of the breast: Review of 909 cases with radiographicpathologic correlations. Eur. J. Radiol. 2005, 54, 55–61. [Google Scholar] [CrossRef]
- Roque, R.; Cordeiro, M.R.; Armas, M.; Caramelo, F.; Caseiro-Alves, F.; Figueiredo-Dias, M. The accuracy of magnetic resonance imaging in predicting the size of pure ductal carcinoma In Situ: A systematic review and meta-analysis. NPJ Breast Cancer 2022, 8, 77. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Solin, L.J. Counterview: Pre-operative breast MRI (magnetic resonance imaging) is not recommended for all patients with newly diagnosed breast cancer. Breast 2010, 19, 7–9. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, P.C.K.; Schrading, S.; Bieling, H.B.; Wardelmann, E.; Leutner, C.C.; Koenig, R.; Kuhn, W.; Schild, P.H.H. MRI for diagnosis of pure ductal carcinoma In Situ: A prospective observational study. Lancet 2007, 370, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Vag, T.; Baltzer, P.A.; Renz, D.M.; Pfleiderer, S.O.; Gajda, M.; Camara, O.; Kaiser, W.A. Diagnosis of ductal carcinoma In Situ using contrast-enhanced magnetic resonance mammography compared with conventional mammography. Clin. Imaging 2008, 32, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.; Chen, J.H.; Agrawal, G.; Lin, M.; Mehta, R.S.; Carpenter, P.M.; Nalcioglu, O.; Su, M.Y. Characterization of Pure Ductal Carcinoma In Situ on Dynamic Contrast-Enhanced MR Imaging: Do Nonhigh-grade and High-grade Show Different Imaging Features? J. Oncol. 2010, 1, 431341. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Menell, J.H.; Morris, E.A.; Dershaw, D.D.; Abramson, A.F.; Brogi, E.; Liberman, L. Determination of the presence and extent of pure ductal carcinoma In Situ by mammography and magnetic resonance imaging. Breast J. 2005, 11, 382–390. [Google Scholar] [CrossRef]
- Schouten van der Velden, A.P.; Schlooz-Vries, M.S.; Boetes, C.; Wobbes, T. Magnetic resonance imaging of ductal carcinoma In Situ: What is its clinical application? A review. Am. J. Surg. 2009, 198, 262–269. [Google Scholar] [CrossRef]
- Petrillo, A.; Fusco, R.; Petrillo, M.; Triunfo, F.; Filice, S.; Vallone, P.; Setola, S.V.; Rubulotta, M.; Di Bonito, M.; Rinaldo, M.; et al. Added Value of Breast MRI for pre-operative diagnosis of ductal carcinoma In Situ: Diagnostic Performance on 362 Patients. Clin. Breast Cancer 2017, 17, e127–e134. [Google Scholar] [CrossRef]
- Jansen, S.A.; Newstead, G.M.; Abe, H.; Shimauchi, A.; Schmidt, R.A.; Karczmar, G.S. Pure ductal carcinoma In Situ: Kinetic and morphologic MR characteristics compared with mammographic appearance and nuclear grade. Radiology 2007, 245, 684–691. [Google Scholar] [CrossRef] [PubMed]
- D’Orsi, C.J.; Sickles, E.A.; Mendelson, E.B.; Morris, E.A. ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System; American College of Radiology: Reston, VA, USA, 2013. [Google Scholar]
- Shehata, M.; Grimm, L.; Ballantyne, N.; Lourenco, A.; Demello, L.R.; Kilgore, M.R.; Rahbar, H. Ductal Carcinoma In Situ: Current Concepts in Biology, Imaging, and Treatment. J. Breast Imaging 2019, 1, 166–176. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gradishar, W.J.; Anderson, B.O.; Balassanian, R.; Blair, S.L.; Burstein, H.J.; Cyr, A.; Elias, A.D.; Farrar, W.B.; Forero, A.; Giordano, S.H. Breast cancer, Version 1.2016. J. Natl. Compr. Cancer Netw. 2015, 13, 1475–1485. [Google Scholar] [CrossRef] [PubMed]
- Lester, S.C.; Bose, S.; Chen, Y.-Y.; Connolly, J.L.; de Baca, M.; Fitzgibbons, P.L.; Hayes, D.F.; Kleer, C.; O’Malley, F.P.; Page, D.L.; et al. Protocol for the examination of specimens from patients with ductal carcinoma In Situ of the breast. Arch. Pathol. Lab. Med. 2009, 133, 15–25. [Google Scholar] [CrossRef]
- Joekel, J.; Eggemann, H.; Costa, S.D.; Ignatov, A. Should the hyperechogenic halo around malignant breast lesions be included in the measurement of tumor size? Breast Cancer Res. Treat. 2016, 156, 311–317. [Google Scholar] [CrossRef]
- Onesti, J.K.; Mangus, B.E.; Helmer, S.D.; Osland, J.S. Breast cancer tumor size: Correlation between magnetic resonance imaging and pathology measurements. Am. J. Surg. 2008, 196, 844–850. [Google Scholar] [CrossRef]
- Daniel, O.K.; Lim, S.M.; Kim, J.H.; Park, H.S.; Park, S.; Kim, S.I. Preoperative prediction of the size of pure ductal carcinoma In Situ using three imaging modalities as compared to histopathological size: Does magnetic resonance imaging add value? Breast Cancer Res. Treat. 2017, 164, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Baur, A.; Bahrs, S.D.; Speck, S.; Wietek, B.M.; Krämer, B.; Vogel, U.; Claussen, C.D.; Siegmann-Luz, K.C. Breast MRI of pure ductal carcinoma In Situ: Sensitivity of diagnosis and influence of lesion characteristics. Eur. J. Radiol. 2013, 82, 1731–1737. [Google Scholar] [CrossRef]
- Liu, H.; Peng, W. MRI morphological classification of ductal carcinoma In Situ (DCIS) correlating with different biological behavior. Eur. J. Radiol. 2012, 81, 214–217. [Google Scholar] [CrossRef]
- Marcotte-Bloch, C.; Balu-Maestro, C.; Chamorey, E.; Ettore, F.; Raoust, I.; Flipo, B.; Chapellier, C. MRI for the size assessment of pure ductal carcinoma In Situ (DCIS): A prospective study of 33 patients. Eur. J. Radiol. 2011, 77, 462–467. [Google Scholar] [CrossRef]
- Kim, D.Y.; Moon, W.K.; Cho, N.; Ko, E.S.; Yang, S.K.; Park, J.S.; Kim, S.M.; Park, I.-A.; Cha, J.H.; Lee, E.H. MRI of the breast for the detection and assessment of the size of ductal carcinoma In Situ. Korean J. Radiol. 2007, 8, 32–39. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Reference | Univariate | Multivariate | ||
|---|---|---|---|---|---|
| OR [95%CI] | p a | OR [95%CI] | p b | ||
| Microcalcification distribution | (Regional-Linear-Segmental/Grouped-None) | 3.86 [1.59–9.34] | 0.003 | 4.64 [1.76–12.21] | 0.002 |
| BI-RADS | (3-4A-4B/4C-5) | 3.73 [1.53–9.08] | 0.004 | 4.52 [1.70–12.00] | 0.003 |
| Diffusion Restriction | (Yes/No) | 2.71 [1.12–6.56] | 0.027 | — | ns |
| Breast composition | (A-B/C-D) | 2.20 [0.94–5.16] | 0.070 | — | ns |
| Variable | Total | High-Grade Group | Low-Grade Group | p | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| BI-RADS category | 3-4A-4B 4C-5 | 54 36 | 60% 40% | 16 22 | 42% 58% | 38 14 | 27% 73% | 0.006 |
| Breast composition | Type A-B Type C-D | 48 42 | 53% 47% | 16 22 | 42% 58% | 32 20 | 62% 38% | 0.107 |
| Microcalcification morphology | Amorphous Pleomorphic Uniform None | 34 24 12 20 | 38% 27% 13% 22% | 12 16 4 6 | 32% 42% 11% 16% | 22 8 8 14 | 42% 15% 15% 27% | 0.043 |
| Microcalcification distribution | Regional-Linear-Segmental Grouped-None | 40 50 | 44% 56% | 24 14 | 63% 37% | 16 36 | 31% 69% | 0.005 |
| Architectural distortion | Yes No | 4 86 | 4% 96% | 2 36 | 5% 95% | 2 50 | 4% 96% | 1.000 |
| Background parenchymal enhancement | 1 2 3-4 | 14 36 40 | 16% 40% 44% | 4 14 20 | 11% 37% 53% | 10 22 10 | 19% 42% 38% | 0.329 |
| MRI morphology | Mass Non-Mass Enhancement | 31 59 | 34% 66% | 10 28 | 26% 74% | 21 31 | 40% 60% | 0.245 |
| Non-mass enhancement distribution | Linear Segmental Regional | 4 33 18 | 7% 60% 33% | 4 19 9 | 13% 59% 28% | 0 14 9 | 0% 61% 39% | na |
| Diffusion restriction | Yes No | 33 57 | 37% 63% | 19 19 | 50% 50% | 14 38 | 27% 73% | 0.043 |
| Kinetic curve type | Persistent Plateau Washout | 40 40 6 | 47% 47% 6% | 13 21 4 | 34% 55% 11% | 27 19 2 | 56% 40% 4% | na |
| Diff. Mean (mm) (95%CI) | p (H0: Mean = 0) | |
|---|---|---|
| Mammographic tumor size (mm) | 4.43 [3.01–5.83] | <0.001 |
| MRI tumor size (mm) | 3.03 [2.12–3.95] | <0.001 |
| Pathologic Tumor Size (mm) | ||
|---|---|---|
| Mammographic tumor size (mm) | 0.872 (0.8142–0.9126) | Poor |
| MRI tumor size (mm) | 0.939 (0.9101–0.9587) | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Çetin Tunçez, H.; Bulut, M.G.; Adıbelli, Z.H.; Bozer, A.; Kart, B.A.; Kocatepe Çavdar, D. Can Mammography and Magnetic Resonance Imaging Predict the Preoperative Size and Nuclear Grade of Pure Ductal Carcinoma In Situ? Diagnostics 2025, 15, 1801. https://doi.org/10.3390/diagnostics15141801
Çetin Tunçez H, Bulut MG, Adıbelli ZH, Bozer A, Kart BA, Kocatepe Çavdar D. Can Mammography and Magnetic Resonance Imaging Predict the Preoperative Size and Nuclear Grade of Pure Ductal Carcinoma In Situ? Diagnostics. 2025; 15(14):1801. https://doi.org/10.3390/diagnostics15141801
Chicago/Turabian StyleÇetin Tunçez, Hülya, Merve Gürsoy Bulut, Zehra Hilal Adıbelli, Ahmet Bozer, Bülent Ahmet Kart, and Demet Kocatepe Çavdar. 2025. "Can Mammography and Magnetic Resonance Imaging Predict the Preoperative Size and Nuclear Grade of Pure Ductal Carcinoma In Situ?" Diagnostics 15, no. 14: 1801. https://doi.org/10.3390/diagnostics15141801
APA StyleÇetin Tunçez, H., Bulut, M. G., Adıbelli, Z. H., Bozer, A., Kart, B. A., & Kocatepe Çavdar, D. (2025). Can Mammography and Magnetic Resonance Imaging Predict the Preoperative Size and Nuclear Grade of Pure Ductal Carcinoma In Situ? Diagnostics, 15(14), 1801. https://doi.org/10.3390/diagnostics15141801