
An Additional 30-s Observation of the Right-Sided Colon Using a Novel Endoscopic System with Texture and Color Enhancement Imaging Decreases Polyp Miss Rates: A Multicenter Study

 ,
,  , and
, and
Abstract
1. Introduction
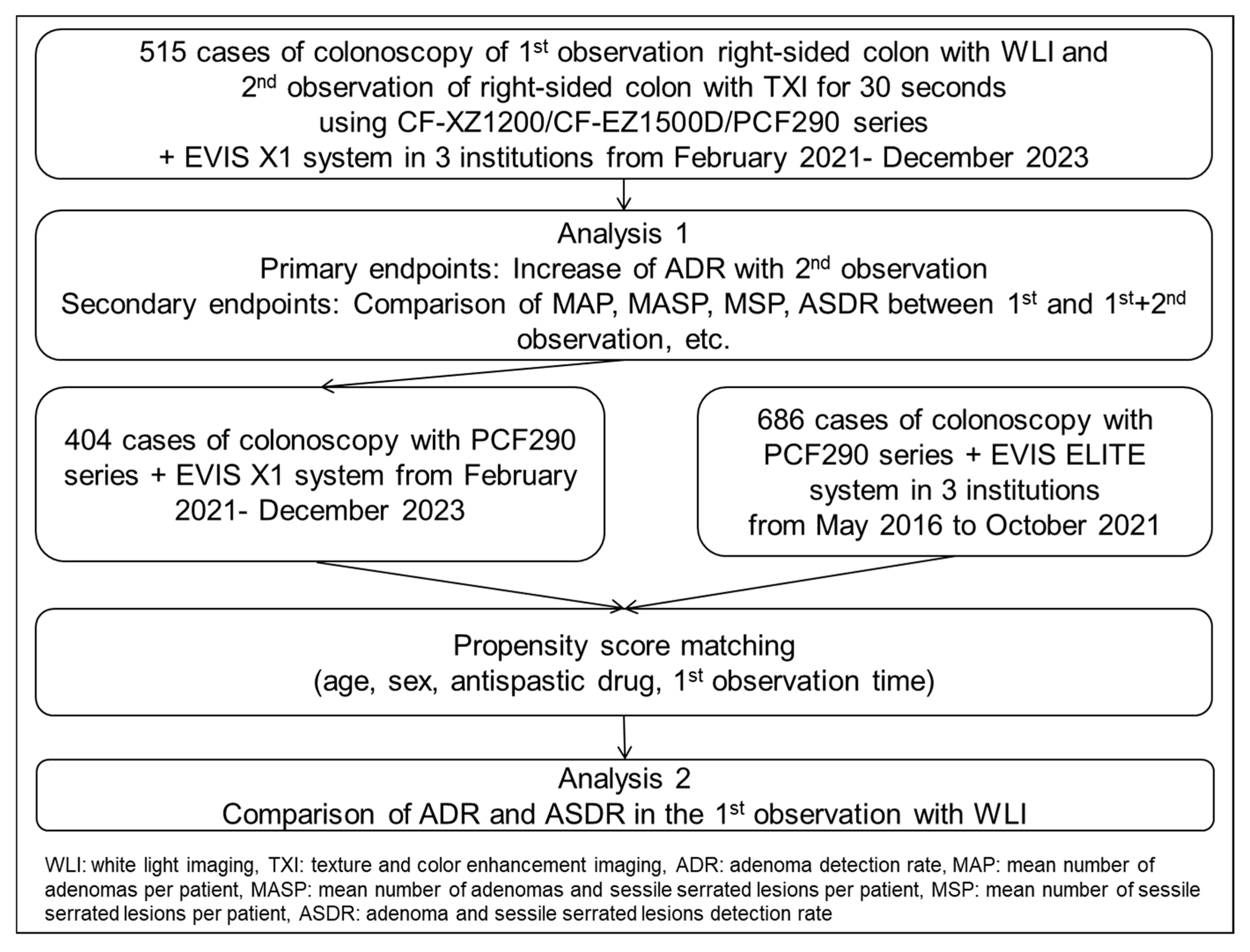
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Winawer, S.J.; Zauber, A.G.; Ho, M.N.; O’Brien, M.J.; Gottlieb, L.S.; Sternberg, S.S.; Waye, J.D.; Schapiro, M.; Bond, J.H.; Panish, J.F.; et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N. Engl. J. Med. 1993, 329, 1977–1981. [Google Scholar] [CrossRef] [PubMed]
- Winawer, S.J.; Zauber, A.G.; O’Brien, M.J.; Ho, M.N.; Gottlieb, L.; Sternberg, S.S.; Waye, J.D.; Bond, J.; Schapiro, M.; Stewart, E.T.; et al. Randomized comparison of surveillance intervals after colonoscopic removal of newly diagnosed adenomatous polyps. The National Polyp Study Workgroup. N. Engl. J. Med. 1993, 328, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Zauber, A.G.; Winawer, S.J.; O’Brien, M.J.; Lansdorp-Vogelaar, I.; van Ballegooijen, M.; Hankey, B.F.; Shi, W.; Bond, J.H.; Schapiro, M.; Panish, J.F.; et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N. Engl. J. Med. 2012, 366, 687–696. [Google Scholar] [CrossRef]
- Zhao, S.; Wang, S.; Pan, P.; Xia, T.; Chang, X.; Yang, X.; Guo, L.; Meng, Q.; Yang, F.; Qian, W.; et al. Magnitude, risk factors, and factors associated with adenoma Miss Rate of tandem colonoscopy: A systematic review and meta-analysis. Gastroenterology 2019, 156, 1661–1674.e11. [Google Scholar] [CrossRef]
- Kim, N.H.; Jung, Y.S.; Jeong, W.S.; Yang, H.J.; Park, S.K.; Choi, K.; Park, D.I. Miss rate of colorectal neoplastic polyps and risk factors for missed polyps in consecutive colonoscopies. Intest. Res. 2017, 15, 411–418. [Google Scholar] [CrossRef]
- Lee, J.; Park, S.W.; Kim, Y.S.; Lee, K.J.; Sung, H.; Song, P.H.; Yoon, W.J.; Moon, J.S. Risk factors of missed colorectal lesions after colonoscopy. Medicine 2017, 96, e7468. [Google Scholar] [CrossRef]
- Leufkens, A.M.; van Oijen, M.G.H.; Vleggaar, F.P.; Siersema, P.D. Factors influencing the miss rate of polyps in a back-to-back colonoscopy study. Endoscopy 2012, 44, 470–475. [Google Scholar] [CrossRef]
- Zimmermann-Fraedrich, K.; Sehner, S.; Rex, D.K.; Kaltenbach, T.; Soetikno, R.; Wallace, M.; Leung, W.K.; Guo, C.; Gralnek, I.M.; Brand, E.C.; et al. Right-sided location not associated with missed colorectal adenomas in an individual-level reanalysis of tandem colonoscopy studies. Gastroenterology 2019, 157, 660–671.e2. [Google Scholar] [CrossRef]
- Laiyemo, A.O.; Doubeni, C.; Sanderson, A.K., 2nd; Pinsky, P.F.; Badurdeen, D.S.; Doria-Rose, V.P.; Marcus, P.M.; Schoen, R.E.; Lanza, E.; Schatzkin, A.; et al. Likelihood of missed and recurrent adenomas in the proximal versus the distal colon. Gastrointest. Endosc. 2011, 74, 253–261. [Google Scholar] [CrossRef]
- Bisschops, R.; East, J.E.; Hassan, C.; Hazewinkel, Y.; Kamiński, M.F.; Neumann, H.; Pellisé, M.; Antonelli, G.; Bustamante Balen, M.; Coron, E.; et al. Advanced imaging for detection and differentiation of colorectal neoplasia: European Society of Gastrointestinal Endoscopy (ESGE) Guideline—Update 2019. Endoscopy 2019, 51, 1155–1179. [Google Scholar]
- Dos Santos, C.E.O.; Malaman, D.; Pereira-Lima, J.C.; Onófrio, F.Q.; Ribas Filho, J.M. Impact of linked-color imaging on colorectal adenoma detection. Gastrointest. Endosc. 2019, 90, 826–834. [Google Scholar] [CrossRef]
- Leung, W.K.; Tsui, V.W.M.; Mak, L.L.Y.; Cheung, M.K.S.; Hui, C.K.Y.; Lam, C.P.M.; Wong, S.Y.; Liu, K.S.H.; Ko, M.K.L.; To, E.W.P.; et al. Blue-light imaging or narrow-band imaging for proximal colonic lesions: A prospective randomized tandem colonoscopy study. Gastrointest. Endosc. 2023, 98, 813–821. [Google Scholar] [CrossRef]
- Atkinson, N.S.S.; Ket, S.; Bassett, P.; Aponte, D.; De Aguiar, S.; Gupta, N.; Horimatsu, T.; Ikematsu, H.; Inoue, T.; Kaltenbach, T.; et al. Narrow-band imaging for detection of neoplasia at colonoscopy: A meta-analysis of data from individual patients in randomized controlled trials. Gastroenterology 2019, 157, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Sato, T. Txi: Texture and color enhancement imaging for endoscopic image enhancement. J. Healthc. Eng. 2021, 2021, 5518948. [Google Scholar] [CrossRef]
- Okumura, T.; Hotta, K.; Imai, K.; Ito, S.; Kishida, Y.; Takada, K.; Kawaguchi, D.; Mori, Y.; Tanaka, Y.; Tsushima, T.; et al. Efficacy of texture and color enhancement imaging for the visibility and diagnostic accuracy of non-polypoid colorectal lesions. DEN Open 2024, 5, e380. [Google Scholar] [CrossRef]
- Yoshida, N.; Inoue, K.; Dohi, O.; Kobayashi, R.; Tomita, Y.; Hashimoto, H.; Sugino, S.; Hirose, R.; Murakami, T.; Inada, Y.; et al. The analysis of texture and color enhancement imaging for improving the visibility of non-polypoid colorectal lesions. Dis. Dig. Sci. 2022, 67, 5657–5665. [Google Scholar] [CrossRef]
- Antonelli, G.; Bevivino, G.; Pecere, S.; Ebigbo, A.; Cereatti, F.; Akizue, N.; Di Fonzo, M.; Coppola, M.; Barbaro, F.; Walter, B.M.; et al. Texture and color enhancement imaging versus high definition white-light endoscopy for detection of colorectal neoplasia: A randomized trial. Endoscopy 2023, 55, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Desai, M.; Bilal, M.; Hamade, N.; Gorrepati, V.S.; Chandrasekar, V.T.; Jegadeesan, R.; Gupta, N.; Bhandari, P.; Repici, A.; Hassan, C.; et al. Increasing adenoma detection rates in the right side of the colon comparing retroflexion with a second forward view: A systematic review. Gastrointest. Endosc. 2019, 89, 453–459.e3. [Google Scholar] [CrossRef]
- Yoshida, N.; Inoue, K.; Yasuda, R.; Hirose, R.; Dohi, O.; Naito, Y.; Murakami, T.; Inada, Y.; Ogiso, K.; Morinaga, Y.; et al. An Additional 30-s Observation of the Right-Sided Colon with Narrow Band Imaging Decreases Missed Polyps: A Pilot Study. Dig. Dis. Sci. 2018, 63, 3457–3464. [Google Scholar] [CrossRef]
- Yoshida, N.; Inagaki, Y.; Inada, Y.; Kobayashi, R.; Tomita, Y.; Hashimoto, H.; Dohi, O.; Hirose, R.; Inoue, K.; Murakami, T.; et al. Additional 30-Second Observation of the Right-Sided Colon for Missed Polyp Detection with Texture and Color Enhancement Imaging Compared with Narrow Band Imaging: A Randomized Trial. Am. J. Gastroenterol. 2024, 119, 539–546. [Google Scholar] [CrossRef]
- Tamai, N.; Horiuchi, H.; Matsui, H.; Furuhashi, H.; Kamba, S.; Dobashi, A.; Sumiyama, K. Visibility evaluation of colorectal lesion using texture and color enhancement imaging with video. DEN Open 2022, 2, e90. [Google Scholar] [CrossRef]
- ASGE Standards of Practice Committee; Saltzman, J.R.; Cash, B.D.; Pasha, S.F.; Early, D.S.; Muthusamy, V.R.; Khashab, M.A.; Chathadi, K.V.; Fanelli, R.D.; Chandrasekhara, V.; et al. Bowel preparation before colonoscopy. Gastrointest. Endosc. 2015, 81, 781–794. [Google Scholar] [CrossRef] [PubMed]
- Sano, Y.; Tanaka, S.; Kudo, S.E.; Saito, S.; Matsuda, T.; Wada, Y.; Fujii, T.; Ikematsu, H.; Uraoka, T.; Kobayashi, N.; et al. Narrow-band imaging (NBI) magnifying endoscopic classification of colorectal tumors proposed by the Japan NBI Expert Team. Dig. Endosc. 2016, 28, 526–533. [Google Scholar] [CrossRef]
- Yamashina, T.; Takeuchi, Y.; Uedo, N.; Aoi, K.; Matsuura, N.; Nagai, K.; Matsui, F.; Ito, T.; Fujii, M.; Yamamoto, S.; et al. Diagnostic features of sessile serrated adenoma/polyps on magnifying narrow band imaging: A prospective study of diagnostic accuracy. J. Gastroenterol. Hepatol. 2015, 30, 117–123. [Google Scholar] [CrossRef]
- Tanaka, S.; Kashida, H.; Saito, Y.; Yahagi, N.; Yamano, H.; Saito, S.; Hisabe, T.; Yao, T.; Watanabe, M.; Yoshida, M.; et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection. Dig. Endosc. 2015, 27, 417–434. [Google Scholar] [CrossRef] [PubMed]
- Uraoka, T.; Takizawa, K.; Tanaka, S.; Kashida, H.; Saito, Y.; Yahagi, N.; Yamano, H.; Saito, S.; Hisabe, T.; Yao, T.; et al. Guidelines for Colorectal Cold Polypectomy (supplement to “Guidelines for Colorectal Endoscopic Submucosal Dissection/Endoscopic Mucosal Resection”). Dig. Endosc. 2022, 34, 668–675. [Google Scholar] [CrossRef]
- The Paris endoscopic classification of superficial neoplastic lesions: Esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest. Endosc. 2003, 58, S3–S43. [CrossRef]
- Hamilton, S.R.; Aaltonen, L.A. (Eds.) World Health Organization classification of tumors. In Pathology and Genetics of Tumours of the Digestive System; IARC Press: Lyon, France, 2010; pp. 104–109. [Google Scholar]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours. Digestive System Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2019. [Google Scholar]
- Sakamoto, T.; Ikematsu, H.; Tamai, N.; Mizuguchi, Y.; Takamaru, H.; Murano, T.; Shinmura, K.; Sasabe, M.; Furuhashi, H.; Sumiyama, K.; et al. Detection of colorectal adenomas with texture and color enhancement imaging: Multicenter observational study. Dig. Endosc. 2023, 35, 529–537. [Google Scholar] [CrossRef]
- Toyoshima, N.; Mizuguchi, Y.; Takamaru, H.; Nakamura, K.; Kakugawa, Y.; Sakamoto, T.; Shiroyama, M.; Kawagoe, R.; Tsuchiya, K.; Shinmura, K.; et al. The Efficacy of Texture and Color Enhancement Imaging Observation in the Detection of Colorectal Lesions: A Multicenter, Randomized Controlled Trial (deTXIon Study). Gastroenterology 2025. Online ahead of print. [Google Scholar] [CrossRef]
- Shergill, A.K.; Conners, E.E.; McQuaid, K.R.; Epstein, S.; Ryan, J.C.; Shah, J.N.; Inadomi, J.; Somsouk, M. Protective association of colonoscopy against proximal and distal colon cancer and patterns in interval cancer. Gastrointest. Endosc. 2015, 82, 529–537.e1. [Google Scholar] [CrossRef]
- Singh, H.; Nugent, Z.; Demers, A.A.; Kliewer, E.V.; Mahmud, S.M.; Bernstein, C.N. The reduction in colorectal cancer mortality after colonoscopy varies by site of the cancer. Gastroenterology 2010, 139, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Tang, R.S.Y.; Lee, J.W.J.; Chang, L.C.; Ong, D.E.H.; Chiu, H.M.; Matsuda, T.; Kim, H.S.; Sekiguchi, M.; Leong, R.W.; Ho, A.M.Y.; et al. Two vs one forward view examination of right colon on adenoma detection: An international multicenter randomized trial. Clin. Gastroenterol. Hepatol. 2022, 20, 372–380.e2. [Google Scholar] [CrossRef] [PubMed]
- Lv, X.H.; Lu, Q.; Sun, Y.N.; Deng, K.; Yang, J.L. Retroflexed view for reexamination of the right colon after forward view examination: Systematic review and meta-analysis. Dig. Endosc. 2022, 34, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Tziatzios, G.; Gkolfakis, P.; Lazaridis, L.D.; Facciorusso, A.; Antonelli, G.; Hassan, C.; Repici, A.; Sharma, P.; Rex, D.K.; Triantafyllou, K. High-definition colonoscopy for improving adenoma detection: A systematic review and meta-analysis of randomized controlled studies. Gastrointest. Endosc. 2020, 91, 1027–1036. [Google Scholar] [CrossRef]
- Hashimoto, H.; Yoshida, N.; Inagaki, Y.; Fukumoto, K.; Hasegawa, D.; Okuda, K.; Tomie, A.; Yasuda, R.; Morimoto, Y.; Murakami, T.; et al. Additional 30-second observation of the right-sided colon for missed polyp detection with linked color imaging compared with narrow band imaging. Endosc. Int. Open 2024, 12, E1092–E1101. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Patient number | 515 |
| Age, years, mean ± SD | 67.1 ± 11.0 |
| Sex, % (n) male/female | 60.6/39.4 (312/203) |
| Insertion time, s, mean ± SD | 359 ± 203 |
| Bowel preparation, % (n) excellent/good/fair/poor | 20.2/54.0/23.9/1.9 (104/278/123/10) |
| Good preparation (excellent + good), % (n) | 74.2 (382) |
| Antispastic drug, % (n) | 75.7 (390) |
| Type of scope, % (n) novel scope/previous scope | 21.6/78.4 (111/404) |
| Sedation, % (n) | 26.6 (137) |
| 1st WLI | 2nd TXI | p Value | |
|---|---|---|---|
| Observation time for right-sided colon, s, mean ± SD | 186 ± 117 | 30 ± 0 | |
| Detected polyp number, n | 326 | 141 | - |
| Polyp size, mm, mean ± SD, (range) | 4.8 ± 3.9 (2–30) | 3.9 ± 3.9 (1–24) | <0.01 |
| Polyp size, % (n) <5 mm/≥5 mm | 63.2/36.8 (206/120) | 75.2/24.8 (106/35) | 0.01 |
| Location, % (n) C/A | 26.4/73.6 (86/240) | 15.6/84.4 (22/119) | 0.01 |
| Morphology, % (n) polypoid/non-polypoid | 65.6/34.4 (214/112) | 67.4/32.6 (95/46) | 0.75 |
| Histopathology, % (n) HP/SSL/Ad | 4.0/21.8/74.2 (13/71/242) | 5.7/20.6/73.8 (8/29/104) | 0.85 |
| MAP, [95% CI] (n) | 0.47 [0.43–0.51] (242) | 0.20 [0,17–0.24] (104) | |
| MASP, [95% Cl] (n) | 0.61 [0.56–0.65] (313) | 0.26 [0.22–0.30] (133) | |
| MSP, [95% CI] (n) | 0.14 [0.11–0.17] (71) | 0.06 [0.04–0.08] (29) |
| 1st WLI | 1st WLI + 2nd TXI | p Value | |
|---|---|---|---|
| Right-sided ADR, % [95% CI] (n) | 30.3 [26.5–34.4] (156) | 37.7 [33.6–41.9] (194) | <0.01 |
| Increase in ADR, % [95% CI] | - | 7.4 [5.4–10.0] | - |
| Right-sided ASDR, % [95% CI] (n) | 38.3 [34.2–42.5] (197) | 47.8 [43.5–52.1] (246) | <0.01 |
| Increase in ASDR, % [95% CI] | - | 9.5 [7.3–12.4] | - |
| MAP, [95% CI] (n) | 0.47 [0.43–0.51] (242) | 0.67 [0.63–0.071] (346) | <0.01 |
| MASP, [95% Cl] (n) | 0.61 [0.56–0.65] (313) | 0.87 [0.83–0.89] (446) | <0.01 |
| MSP, [95% CI] (n) | 0.14 [0.11–0.17] (71) | 0.19 [0.16–0.23] (100) | <0.01 |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| Adenoma/SSL-Detected Group | Non-Detected Group | p Value | Odds Ratio (95% Cl) | p Value | |
| Case number | 104 | 411 | |||
| Age, years, mean ± SD | 68.7 ± 10.9 | 66.7 ± 11.0 | 0.08 | 1.02 (0.99–1.04) | 0.10 |
| Sex, % (n), male/female | 62.5/37.5 (65/39) | 60.1/39.9 (247/164) | 0.14 | 1.06 (0.65–1.74) | 0.81 |
| Bowel preparation, % (n), excellent/good/fair/poor | 23.1/51.0/23.1/2.9 (24/53/24/3) | 19.5/54.7/24.1/1.7 (80/225/99/7) | 0.88 | ||
| Good preparation, (good, excellent), % (n) | 74.0 (77) | 74.2 (305) | 0.80 | ||
| Antispastic drug, % (n) | 76.9 (80) | 75.4 (310) | 0.43 | 1.28 (0.73–2.25) | 0.40 |
| Sedation, % (n) | 32.7 (34) | 25.1 (103) | 0.07 | 1.53 (0.94–2.50) | 0.08 |
| Novel scope, % (n) | 34.6 (36) | 18.2 (75) | <0.01 | 2.41 (1.47–3.94) | <0.01 |
| 1st WLI observation time, s, mean ± SD | 192 ± 118 | 184 ± 117 | 0.32 | 1.00 (0.99–1.00) | 0.37 |
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| Adenoma-Detected Group | Non-Detected Group | p Value | Odds Ratio (95% Cl) | p Value | |
| Case number | 83 | 432 | |||
| Age, years, mean ± SD | 69.1 ± 10.4 | 66.7 ± 11.1 | 0.29 | 1.03 (1.00–1.05) | 0.10 |
| Sex, % (n), male/female | 68.7/31.3 (57/26) | 59.0/41.0 (255/177) | 0.11 | 1.65 (0.96–2.85) | 0.07 |
| Bowel preparation, % (n), excellent/good/fair/poor | 25.3/50.6/21.7/2.4 (21/42/18/2) | 19.2/54.6/24.3/1.9 (83/236/105/8) | 0.61 | ||
| Good preparation, (good, excellent), % (n) | 75.9 (63) | 73.8 (319) | 0.78 | ||
| Antispastic drug, % (n) | 78.3 (65) | 75.2 (325) | 0.68 | 1.62 (0.86–3.07) | 0.14 |
| Sedation, % (n) | 32.5 (27) | 25.5 (110) | 0.22 | 1.61 (0.94–2.77) | 0.08 |
| Novel scope, % (n) | 34.9 (29) | 19.0 (82) | <0.01 | 2.11 (1.25–3.57) | 0.01 |
| 1st WLI observation time, s, mean ± SD | 356 ± 224 | 359 ± 199 | 0.65 | 1.00 (0.99–1.00) | 0.89 |
| Pre Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Scope | Novel Scope | Previous Scope | p Value | Novel Scope | Previous Scope | p Value |
| Patient number, n | 111 | 404 | 111 | 111 | ||
| Age, years, mean ± SD | 68.4 ± 10.9 | 66.7 ± 10.0 | 0.19 | 68.4 ± 10.9 | 69.4 ± 11.2 | 0.54 |
| Sex, % (n) male/female | 75.7/24.3 (84/27) | 56.4/43.6 (228/176) | <0.01 | 75.7/24.3 (84/27) | 75.7/24.3 (84/27) | 0.56 |
| Antispastic drug, % (n) | 75.7 (84) | 75.7 (306) | 1.00 | 75.7 (84) | 67.6 (75) | 0.12 |
| 1st WLI observation time, s, mean ± SD | 169 ± 117 | 190 ± 117 | 0.04 | 169 ± 117 | 177 ± 122 | 0.33 |
| 1st WLI ADR, %, (n) | 39.6 (44) | 27.4 (111) | 0.01 | 39.6 (44) | 29.7 (33) | 0.08 |
| 2nd TXI ADR, %, (n) | 25.2 (28) | 13.4 (54) | <0.01 | 25.2 (28) | 15.3 (17) | 0.04 |
| 1st WLI ASDR, %, (n) | 49.5 (55) | 35.1 (142) | <0.01 | 49.5 (55) | 41.4 (46) | 0.14 |
| 2nd TXI ASDR, %, (n) | 32.4 (36) | 16.8 (68) | <0.01 | 32.4 (36) | 18.9 (21) | 0.02 |
| Pre Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| System | Novel System | Previous System | p Value | Novel System | Previous System | p Value |
| Patient number, n | 404 | 686 | 402 | 402 | ||
| Age, years, mean ± SD | 66.7 ± 10.0 | 66.8 ± 11.9 | 0.65 | 66.7 ± 11.3 | 67.4 ± 11.9 | 0.39 |
| Sex, % (n) male/female | 56.4/43.6 (228/176) | 384/304 | 0.46 | 56.5/43.5 (227/175) | 58.5/41.5 (235/167) | 0.62 |
| Antispastic drug, % (n) | 75.7 (306) | 62.8 (431) | <0.01 | 76.1 (306) | 76.1 (306) | 1.00 |
| 1st WLI observation time, s, mean ± SD | 190 ± 117 | 214 ± 123 | <0.01 | 187 ± 121 | 192 ± 125 | 0.52 |
| 1st WLI ADR, %, (n) | 27.4 (111) | 25.8 (177) | 0.30 | 27.4 (110) | 22.6 (91) | 0.14 |
| 1st WLI ASDR, %, (n) | 35.1 (142) | 29.8 (205) | 0.04 | 34.8 (140) | 25.9 (104) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inagaki, Y.; Yoshida, N.; Hashimoto, H.; Inada, Y.; Murakami, T.; Shimomura, T.; Kassai, K.; Tomita, Y.; Kobayashi, R.; Inoue, K.; et al. An Additional 30-s Observation of the Right-Sided Colon Using a Novel Endoscopic System with Texture and Color Enhancement Imaging Decreases Polyp Miss Rates: A Multicenter Study. Diagnostics 2025, 15, 1759. https://doi.org/10.3390/diagnostics15141759
Inagaki Y, Yoshida N, Hashimoto H, Inada Y, Murakami T, Shimomura T, Kassai K, Tomita Y, Kobayashi R, Inoue K, et al. An Additional 30-s Observation of the Right-Sided Colon Using a Novel Endoscopic System with Texture and Color Enhancement Imaging Decreases Polyp Miss Rates: A Multicenter Study. Diagnostics. 2025; 15(14):1759. https://doi.org/10.3390/diagnostics15141759
Chicago/Turabian StyleInagaki, Yoshikazu, Naohisa Yoshida, Hikaru Hashimoto, Yutaka Inada, Takaaki Murakami, Takahito Shimomura, Kyoichi Kassai, Yuri Tomita, Reo Kobayashi, Ken Inoue, and et al. 2025. "An Additional 30-s Observation of the Right-Sided Colon Using a Novel Endoscopic System with Texture and Color Enhancement Imaging Decreases Polyp Miss Rates: A Multicenter Study" Diagnostics 15, no. 14: 1759. https://doi.org/10.3390/diagnostics15141759
APA StyleInagaki, Y., Yoshida, N., Hashimoto, H., Inada, Y., Murakami, T., Shimomura, T., Kassai, K., Tomita, Y., Kobayashi, R., Inoue, K., Hirose, R., Dohi, O., & Itoh, Y. (2025). An Additional 30-s Observation of the Right-Sided Colon Using a Novel Endoscopic System with Texture and Color Enhancement Imaging Decreases Polyp Miss Rates: A Multicenter Study. Diagnostics, 15(14), 1759. https://doi.org/10.3390/diagnostics15141759