
Perioperative Risk Prediction in Major Gynaecological Oncology Surgery: A National Diagnostic Survey of UK Clinical Practice

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Survey Development
2.2. Participants and Distribution
- Consultant gynaecological oncologists based at tertiary cancer centres,
- Obstetrics and gynaecology (O&G) consultants as part of cancer units,
- Subspecialty and specialty trainees in GO based at tertiary cancer centres,
- Clinical nurse specialists (CNS) in GO based at tertiary cancer centres.
2.3. Data Analysis
3. Results
3.1. Demographics
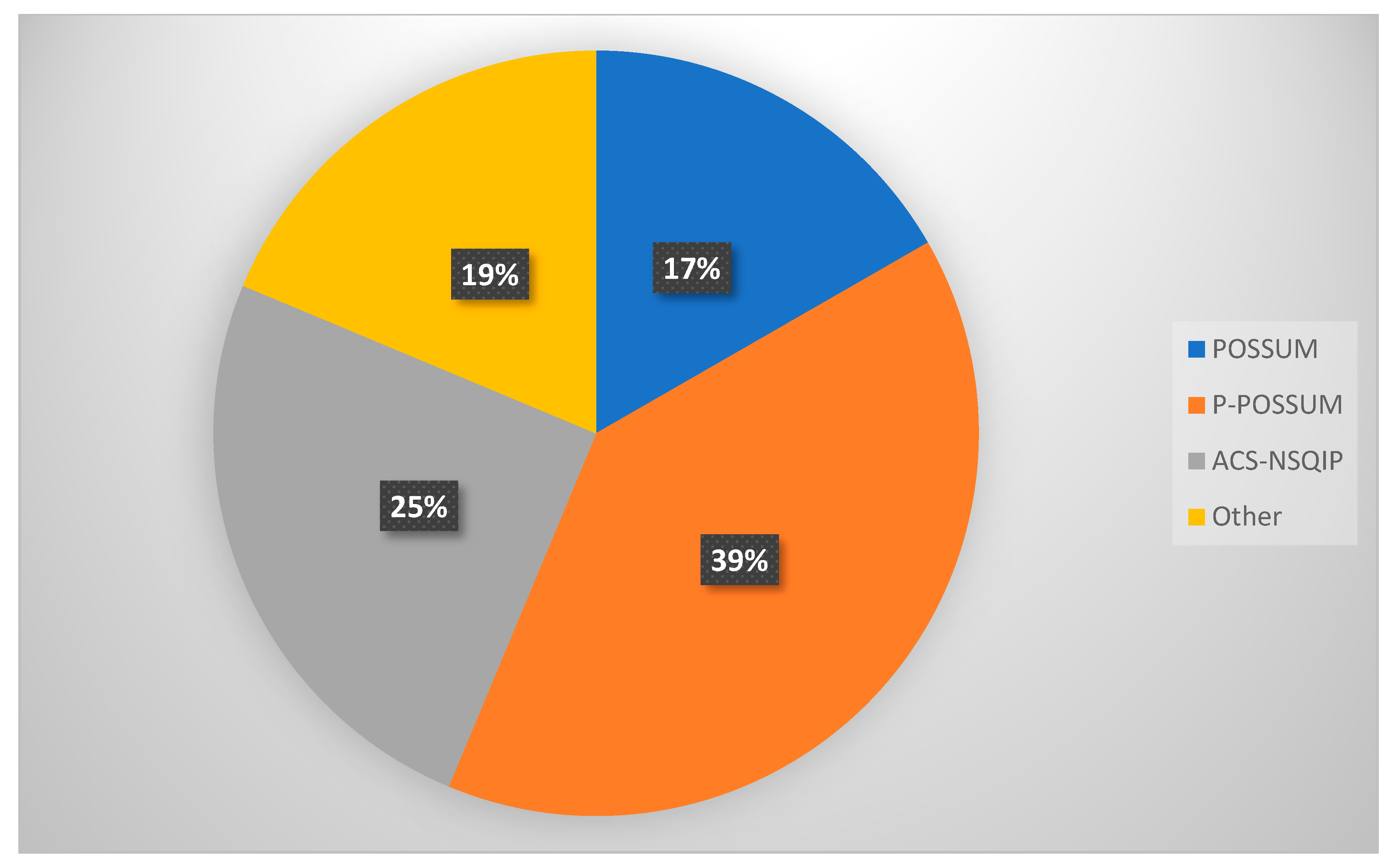
3.2. Utilisation of Morbidity Prediction Algorithms
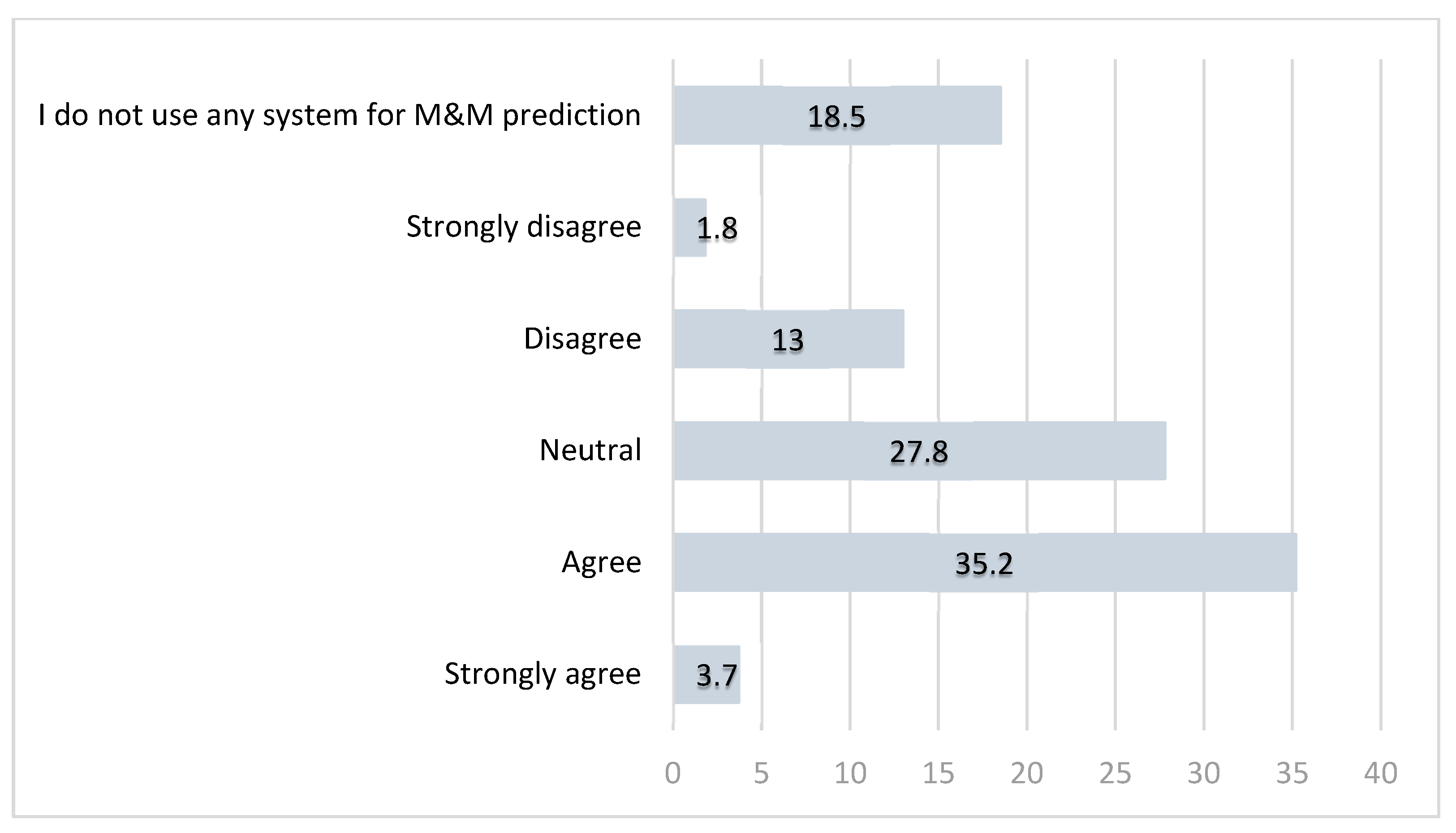
3.3. Perceived Reliability of Risk Prediction Tools
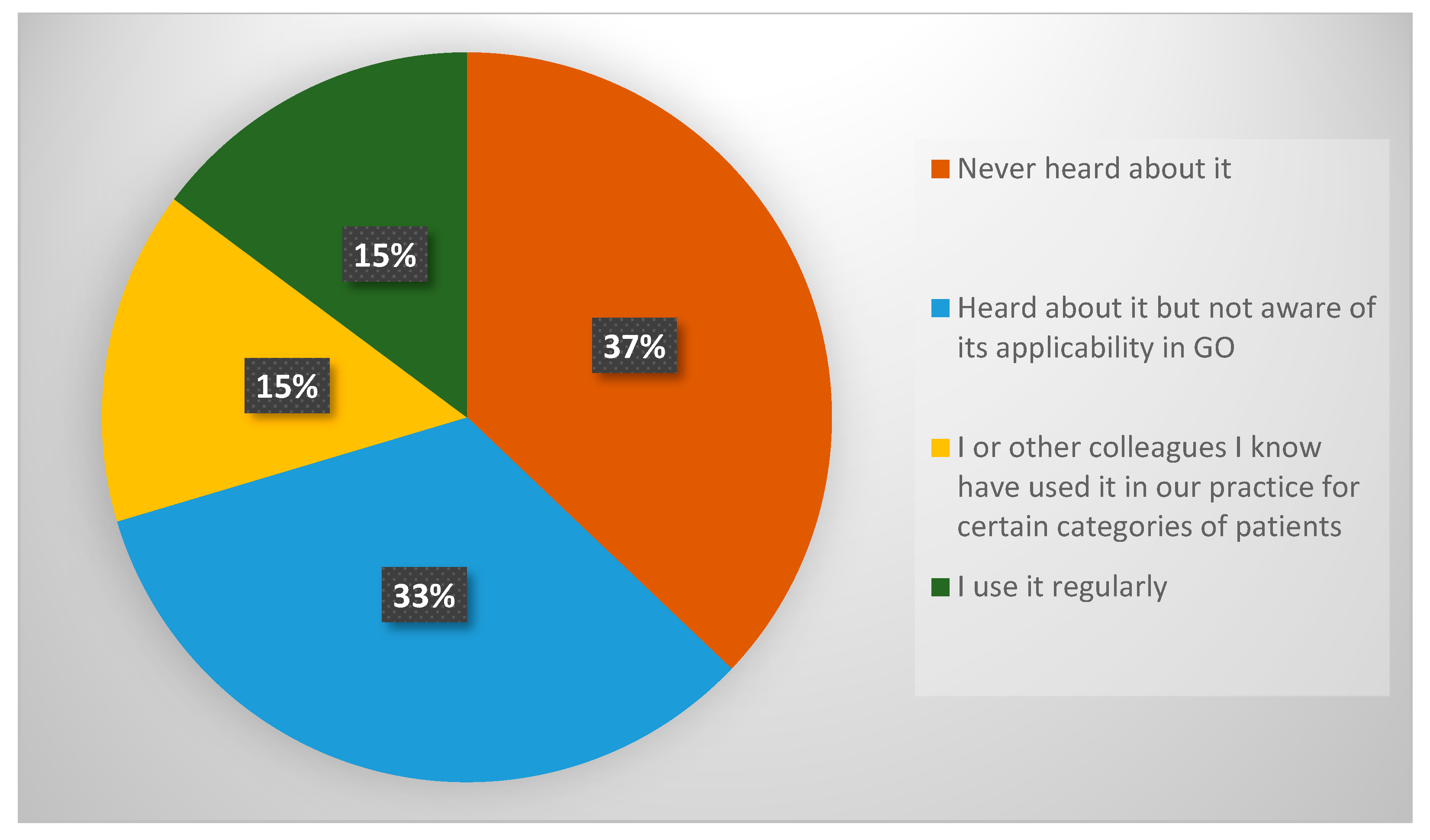
3.4. Familiarity with ACS NSQIP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| UK | The United Kingdom |
| O&G | Obstetrics and Gynaecology |
| BGCS | British Gynaecological Cancer Society |
| GO | Gynaecological Oncology |
| POSSUM | Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity |
| P-POSSUM | Portsmouth POSSUM |
| ACS NSQIP | The American College of Surgeons National Surgical Quality Improvement Program |
| GLOBOCAN | Global Cancer Statistics |
| WHO | World Health Organisation |
| MIS | Minimally Invasive Surgery |
| QoL | Quality of life |
| RCOG | Royal College of Obstetricians and Gynaecologists |
| M&M | Morbidity and Mortality |
| SORT | Surgical Outcome Risk Tool |
| CCI | Charlson Comorbidity Index |
| ASA | American Society of Anesthesiologists |
| APACHE | Acute Physiology And Chronic Health Evaluation |
| SRS | Surgical Risk Scale |
| SAS | Surgical Apgar Score |
| ECOG | Eastern Cooperative Oncology Group |
| CNS | Clinical Nurse Specialist |
| GO SOAR | Global Gynaecological Oncology Surgical Outcomes Collaborative |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Answer Choices | |
|---|---|---|
| Q1 | Which of the below best describes you? |
|
| Q2 | Please specify your place of work. |
|
| Q3 | Do you use any algorithms to predict morbidity prior to their major surgery? |
|
| Q4 | What algorithms or risk scoring systems do you use? |
|
| Q5 | The system I use is reliable for predicting peri-operative morbidity and mortality. |
|
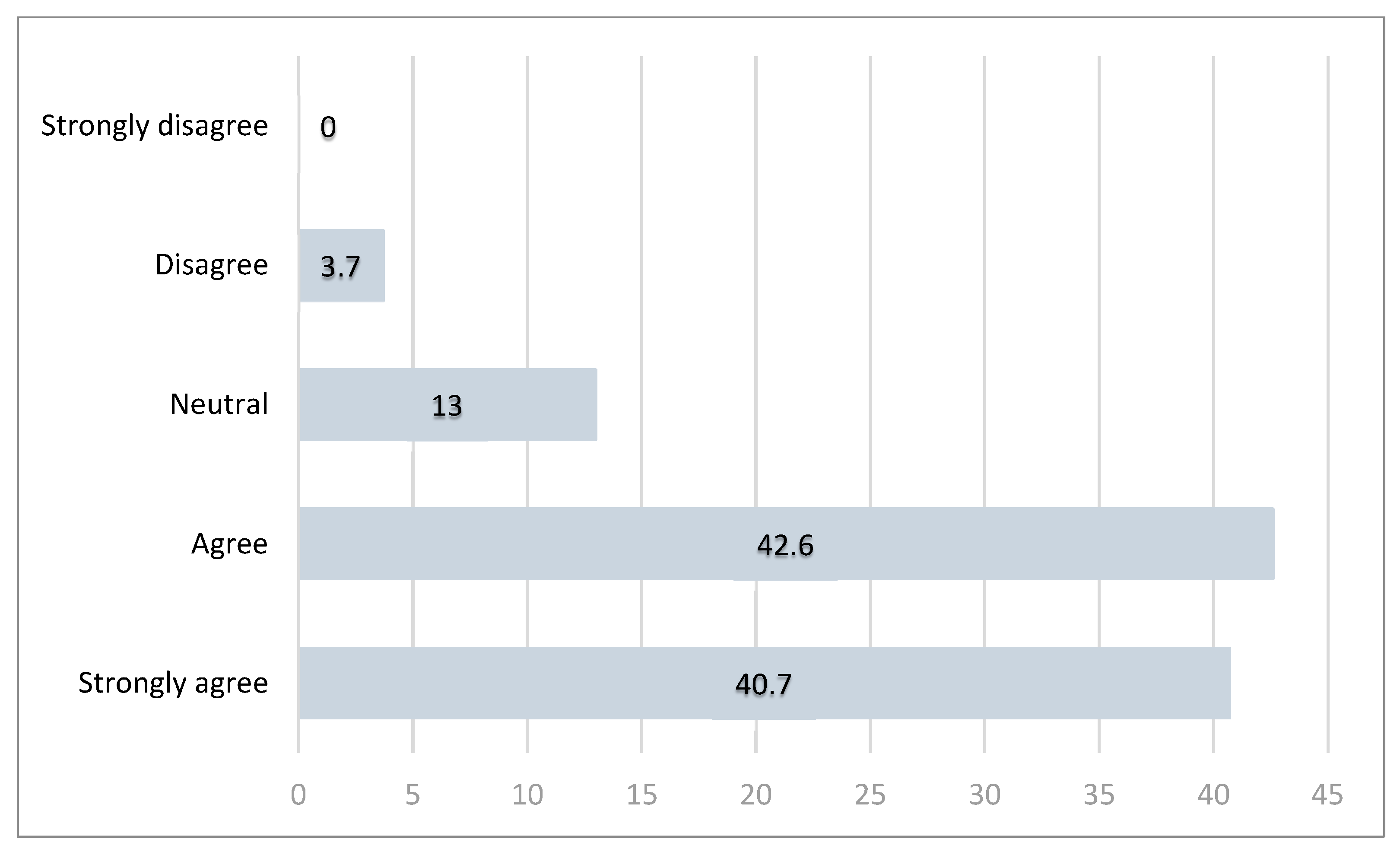
| Q6 | There is a clinical need for a more accurate risk prediction algorithm for patients undergoing gynae-oncological surgical procedures. |
|
| Q7 | Are you familiar with ACS NSQIP (American College of Surgeons National Surgical Quality Improvement Program) surgical risk calculator? |
|
| Q8 | Would you be interested in being invited to participate in retrospective/prospective study exploring risk scoring for patients undergoing surgery for gynaecological cancers? |
|
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2024, 74, 1–35. [Google Scholar] [CrossRef]
- Clair, K.H.; Tewari, K.S. Robotic surgery for gynecologic cancers: Indications, techniques and controversies. J. Obstet. Gynaecol. Res. 2020, 46, 828–843. [Google Scholar] [CrossRef]
- Part 3: Adult Overweight and Obesity—NDRS. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/statistics-on-obesity-physical-activity-and-diet-england-2019/part-3-adult-obesity (accessed on 24 June 2025).
- Voices of Our Ageing Population—Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/voicesofourageingpopulation/livinglongerlives (accessed on 24 June 2025).
- Iyer, R.; Gentry-Maharaj, A.; Nordin, A.; Burnell, M.; Liston, R.; Manchanda, R.; Das, N.; Desai, R.; Gornall, R.; Beardmore-Gray, A.; et al. Predictors of complications in gynaecological oncological surgery: A prospective multicentre study (UKGOSOC-UK gynaecological oncology surgical outcomes and complications). Br. J. Cancer 2015, 112, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, L.; Casarin, J.; Mara, K.C.; Weaver, A.L.; Multinu, F.; Glaser, G.E.; Cliby, W.A.; Scambia, G.; Mariani, A.; Kumar, A. Prediction of short-term surgical complications in women undergoing pelvic exenteration for gynecological malignancies. Gynecol. Oncol. 2019, 152, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Kengsakul, M.; Nieuwenhuyzen-de Boer, G.M.; Udomkarnjananun, S.; Kerr, S.J.; van Doorn, H.C.; van Beekhuizen, H.J. Factors Predicting 30-Day Grade IIIa–V Clavien–Dindo Classification Complications and Delayed Chemotherapy Initiation after Cytoreductive Surgery for Advanced-Stage Ovarian Cancer: A Prospective Cohort Study. Cancers 2022, 14, 4181. [Google Scholar] [CrossRef] [PubMed]
- Joseph, N.; Clark, R.M.; Dizon, D.S.; Lee, M.S.; Goodman, A.; Boruta, D.; Schorge, J.O.; Del Carmen, M.G.; Growdon, W.B. Delay in chemotherapy administration impacts survival in elderly patients with epithelial ovarian cancer. Gynecol. Oncol. 2015, 137, 401–405. [Google Scholar] [CrossRef]
- Heikkinen, J.; Kärkkäinen, H.; Eloranta, M.-L.; Anttila, M. Postoperative Complications of Upfront Ovarian Cancer Surgery and Their Effects on Chemotherapy Delay. Curr. Oncol. 2024, 31, 5630–5642. [Google Scholar] [CrossRef]
- Angeles, M.A.; Hernández, A.; Pérez-Benavente, A.; Cabarrou, B.; Spagnolo, E.; Rychlik, A.; Daboussi, A.; Migliorelli, F.; Bétrian, S.; Ferron, G.; et al. The effect of major postoperative complications on recurrence and long-term survival after cytoreductive surgery for ovarian cancer. Gynecol. Oncol. 2022, 166, 8–17. [Google Scholar] [CrossRef]
- Cornellà, N.; Sancho, J.; Sitges-Serra, A. Short and Long-Term Outcomes After Surgical Procedures Lasting for More Than Six Hours. Sci. Rep. 2017, 7, 9221. [Google Scholar] [CrossRef]
- Baker, J.; Janda, M.; Gebski, V.; Forder, P.; Hogg, R.; Manolitsas, T.; Obermair, A. Lower preoperative quality of life increases postoperative risk of adverse events in women with endometrial cancer: Results from the LACE trial. Gynecol. Oncol. 2015, 137, 102–105. [Google Scholar] [CrossRef]
- Guo, Y.; Chang, E.; Bozkurt, M.; Park, M.; Liu, D.; Fu, J.B. Factors affecting hospital length of stay following pelvic exenteration surgery. J. Surg. Oncol. 2018, 117, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Davenport, D.L.; Henderson, W.G.; Khuri, S.F.; Mentzer, R.M. Preoperative risk factors and surgical complexity are more predictive of costs than postoperative complications: A case study using the National Surgical Quality Improvement Program (NSQIP) database. Ann. Surg. 2005, 242, 463–468; discussion 468–471. [Google Scholar] [CrossRef] [PubMed]
- Kolh, P.; De Hert, S.; De Rango, P. The Concept of Risk Assessment and Being Unfit for Surgery. Eur. J. Vasc. Endovasc. Surg. Off. J. Eur. Soc. Vasc. Surg. 2016, 51, 857–866. [Google Scholar] [CrossRef]
- Lees, N.; Peden, C.; Dhesi, J.; Quiney, N.; Lockwood, S.; Symons, N.; Pearse, R.; Moug, S.; Damaskos, D.; Stephenson, J.; et al. The High-Risk General Surgical Patient: Raising the Standard; Royal College of Surgeons of England: London, UK, 2018. [Google Scholar]
- Inci, M.G.; Richter, R.; Woopen, H.; Rasch, J.; Heise, K.; Anders, L.; Mueller, K.; Nasser, S.; Siepmann, T.; Sehouli, J. Role of predictive markers for severe postoperative complications in gynecological cancer surgery: A prospective study (RISC-Gyn Trial). Int. J. Gynecol. Cancer 2020, 30, 1975–1982. [Google Scholar] [CrossRef]
- Tortorella, L.; Marco, C.; Loverro, M.; Carmine, C.; Persichetti, E.; Bizzarri, N.; Barbara, C.; Francesco, S.; Foschi, N.; Gallotta, V.; et al. Predictive factors of surgical complications after pelvic exenteration for gynecological malignancies: A large single-institution experience. J. Gynecol. Oncol. 2024, 35, e4. [Google Scholar] [CrossRef]
- General Medical Council Guidance on Professional Standards and Ethics for Doctors Decision Making and Consent. 2020. Available online: https://www.gmc-uk.org/-/media/documents/gmc-guidance-for-doctors---decision-making-and-consent-english_pdf-84191055.pdf (accessed on 24 May 2025).
- Royal College of Obstetricians and Gynaecologists. Clinical Governance Advice No.6 on Obtaining Valid Consent. January 2025. Available online: https://www.rcog.org.uk/media/pndfv5qf/cga6.pdf (accessed on 24 May 2025).
- Jungmann, E. Obtaining valid consent. J. Fam. Plan. Reprod. Health Care 2006, 32, 259–260. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence Guidance About shared decision making. Available online: https://www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-guidelines/shared-decision-making (accessed on 24 May 2025).
- ASA Physical Status Classification System | American Society of Anesthesiologists (ASA). Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 24 May 2025).
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- Schag, C.C.; Heinrich, R.L.; Ganz, P.A. Karnofsky performance status revisited: Reliability, validity, and guidelines. J. Clin. Oncol. 1984, 2, 187–193. [Google Scholar] [CrossRef]
- Copeland, G.P.; Jones, D.; Walters, M. POSSUM: A scoring system for surgical audit. Br. J. Surg. 1991, 78, 355–360. [Google Scholar] [CrossRef]
- Prytherch, D.R.; Whiteley, M.S.; Higgins, B.; Weaver, P.C.; Prout, W.G.; Powell, S.J. POSSUM and Portsmouth POSSUM for predicting mortality. Br. J. Surg. 1998, 85, 1217–1220. [Google Scholar] [CrossRef]
- Protopapa, K.L.; Simpson, J.C.; Smith, N.C.E.; Moonesinghe, S.R. Development and validation of the Surgical Outcome Risk Tool (SORT). Br. J. Surg. 2014, 101, 1774–1783. [Google Scholar] [CrossRef] [PubMed]
- LeGall, J.R.; Loirat, P.; Alpérovitch, A. APACHE II--a severity of disease classification system. Crit. Care Med. 1986, 14, 754–755. [Google Scholar] [CrossRef]
- Gawande, A.A.; Kwaan, M.R.; Regenbogen, S.E.; Lipsitz, S.A.; Zinner, M.J. An Apgar Score for Surgery. J. Am. Coll. Surg. 2007, 204, 201–208. [Google Scholar] [CrossRef]
- Sutton, R.; Bann, S.; Brooks, M.; Sarin, S. The Surgical Risk Scale as an improved tool for risk-adjusted analysis in comparative surgical audit. Br. J. Surg. 2002, 89, 763–768. [Google Scholar] [CrossRef] [PubMed]
- Donati, A.; Ruzzi, M.; Adrario, E.; Pelaia, P.; Coluzzi, F.; Gabbanelli, V.; Pietropaoli, P. A new and feasible model for predicting operative risk. Br. J. Anaesth. 2004, 93, 393–399. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef] [PubMed]
- Bihorac, A.; Ozrazgat-Baslanti, T.; Ebadi, A.; Motaei, A.; Madkour, M.; Pardalos, P.M.; Lipori, G.; Hogan, W.R.; Efron, P.A.; Moore, F.; et al. MySurgeryRisk: Development and Validation of a Machine-Learning Risk Algorithm for Major Complications and Death after Surgery. Ann. Surg. 2019, 269, 652–662. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Liu, Y.; Paruch, J.L.; Zhou, L.; Kmiecik, T.E.; Ko, C.Y.; Cohen, M.E. Development and evaluation of the universal ACS NSQIP surgical risk calculator: A decision aid and informed consent tool for patients and surgeons. J. Am. Coll. Surg. 2013, 217, 833–842e3. [Google Scholar] [CrossRef]
- ACS Risk Calculator—Home Page. Available online: https://riskcalculator.facs.org/RiskCalculator/index.jsp (accessed on 24 May 2025).
- ACS NSQIP | ACS. Available online: https://www.facs.org/quality-programs/data-and-registries/acs-nsqip/ (accessed on 24 May 2025).
- Giannella, L.; Ciavattini, A. Screening and Early Diagnosis in Gynecological Cancers. Cancers 2023, 15, 5152. [Google Scholar] [CrossRef]
- Mahdi, H.; Jernigan, A.M.; Aljebori, Q.; Lockhart, D.; Moslemi-Kebria, M. The impact of obesity on the 30-day morbidity and mortality after surgery for endometrial cancer. J. Minim. Invasive Gynecol. 2015, 22, 94–102. [Google Scholar] [CrossRef]
- Scholtz, K.; Spies, C.D.; Mörgeli, R.; Eckardt, R.; von Dossow, V.; Braun, S.; Sehouli, J.; Bahra, M.; Stief, C.G.; Wernecke, K.-D.; et al. Risk factors for 30-day complications after cancer surgery in geriatric patients: A secondary analysis. Acta Anaesthesiol. Scand. 2018, 62, 451–463. [Google Scholar] [CrossRef]
- Langstraat, C.; Aletti, G.; Cliby, W. Short-term morbidity and mortality in the elderly undergoing ovarian cancer debulking: A delicate balance requiring individualization. Gynecol. Oncol. 2010, 116, S126–S127. [Google Scholar] [CrossRef]
- Fu, H.; Zhang, J.; Zhao, S.; He, N. Survival outcomes of robotic-assisted laparoscopy versus conventional laparoscopy and laparotomy for endometrial cancer: A systematic review and meta-analysis. Gynecol. Oncol. 2023, 174, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Gaba, F.; Ash, K.; Blyuss, O.; Chandrasekaran, D.; Nobbenhuis, M.; Ind, T. Robotic Surgery from a Gynaecological Oncology Perspective: A Global Gynaecological Oncology Surgical Outcomes Collaborative Led Study (GO SOAR3). Diseases 2025, 13, 9. [Google Scholar] [CrossRef]
- Pradhan, N.; Dyas, A.R.; Bronsert, M.R.; Lambert-Kerzner, A.; Henderson, W.G.; Qiu, H.; Colborn, K.L.; Mason, N.J.; Meguid, R.A. Attitudes about use of preoperative risk assessment tools: A survey of surgeons and surgical residents in an academic health system. Patient Saf. Surg. 2022, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Rivard, C.; Nahum, R.; Slagle, E.; Duininck, M.; Isaksson Vogel, R.; Teoh, D. Evaluation of the performance of the ACS NSQIP surgical risk calculator in gynecologic oncology patients undergoing laparotomy. Gynecol. Oncol. 2016, 141, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Szender, J.B.; Frederick, P.J.; Eng, K.H.; Akers, S.N.; Lele, S.B.; Odunsi, K. Evaluation of the National Surgical Quality Improvement Program Universal Surgical Risk Calculator for a gynecologic oncology service. Int. J. Gynecol. Cancer 2015, 25, 512–520. [Google Scholar] [CrossRef]
- Panton, J.; Beaulieu-Jones, B.R.; Marwaha, J.S.; Woods, A.P.; Nakikj, D.; Gehlenborg, N.; Brat, G.A. How Surgeons Use Risk Calculators and Non-Clinical Factors for Informed Consent and Shared Decision Making: A Qualitative Study. Am. J. Surg. 2023, 226, 660–667. [Google Scholar] [CrossRef]
- Farzandipour, M.; Meidani, Z.; Riazi, H.; Sadeqi Jabali, M. Task-specific usability requirements of electronic medical records systems: Lessons learned from a national survey of end-users. Inform. Health Soc. Care 2018, 43, 280–299. [Google Scholar] [CrossRef]
- Das, N.; Talaat, A.S.; Naik, R.; Lopes, A.D.; Godfrey, K.A.; Hatem, M.H.; Edmondson, R.J. Risk adjusted surgical audit in gynaecological oncology: P-POSSUM does not predict outcome. Eur. J. Surg. Oncol. 2006, 32, 1135–1138. [Google Scholar] [CrossRef] [PubMed]
- Sevinyan, L.; Asaalaarchchi, H.; Tailor, A.; Williams, P.; Evans, M.; Hodnett, D.; Arakkal, D.; Prabhu, P.; Flint, M.S.; Madhuri, T.K. Head-to-Head Comparison: P-POSSUM and ACS-NSQIP® in Predicting Perioperative Risk in Robotic Surgery for Gynaecological Cancers. Cancers 2024, 16, 2297. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Surgeons_morbidity_and_mortality_2015. Available online: https://www.rcseng.ac.uk/-/media/Files/RCS/Library-and-publications/Non-journal-publications/Morbidity-and-mortality--a-guide-to-good-practice.pdf (accessed on 24 June 2025).
- Gaba, F.; Ash, K.; Blyuss, O.; Bizzarri, N.; Kamfwa, P.; Saiz, A.; Cibula, D. International Variations in Surgical Morbidity and Mortality Post Gynaecological Oncology Surgery: A Global Gynaecological Oncology Surgical Outcomes Collaborative Led Study (GO SOAR1). Cancers 2023, 15, 5001. [Google Scholar] [CrossRef] [PubMed]

| Variable | Number | % |
|---|---|---|
| Clinical role (Question 1) * | ||
| Consultant GO | 36 | 66.7 |
| Subspecialty GO | 5 | 9.3 |
| Consultant O&G | 7 | 13.0 |
| Speciality trainee O&G | 4 | 7.4 |
| CNS | 1 | 1.8 |
| Other | 1 | 1.8 |
| Clinical setting (Question 2) * | ||
| Gynaecological cancer centre | 36 | 66.7 |
| District general hospital | 17 | 31.5 |
| Other | 1 | 1.8 |
| Question | Response Variable | Number | % |
|---|---|---|---|
| 3. Do you use any algorithms to predict morbidity prior to their major surgery? * | Never | 12 | 22.2 |
| Selectively for certain categories of patients | 28 | 51.9 | |
| Frequently | 10 | 18.5 | |
| Always | 4 | 7.4 | |
| I do not perform surgery | 0 | 0 | |
| 4. What algorithms or risk scoring systems do you use? ** | POSSUM | 8 | 16.7 |
| P-POSSUM | 19 | 39.6 | |
| ACS NSQIP | 12 | 25.0 | |
| Other (please specify) | 9 | 18.7 | |
| 5. The system I use is reliable for predicting peri-operative morbidity and mortality  . * . * | Strongly agree | 2 | 3.7 |
| Agree | 19 | 35.2 | |
| Neutral | 15 | 27.8 | |
| Disagree | 7 | 13.0 | |
| Strongly disagree | 1 | 1.8 | |
| I do not use any system for predicting M&M | 10 | 18.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sevinyan, L.; Tailor, A.; Prabhu, P.; Williams, P.; Flint, M.; Madhuri, T.K. Perioperative Risk Prediction in Major Gynaecological Oncology Surgery: A National Diagnostic Survey of UK Clinical Practice. Diagnostics 2025, 15, 1723. https://doi.org/10.3390/diagnostics15131723
Sevinyan L, Tailor A, Prabhu P, Williams P, Flint M, Madhuri TK. Perioperative Risk Prediction in Major Gynaecological Oncology Surgery: A National Diagnostic Survey of UK Clinical Practice. Diagnostics. 2025; 15(13):1723. https://doi.org/10.3390/diagnostics15131723
Chicago/Turabian StyleSevinyan, Lusine, Anil Tailor, Pradeep Prabhu, Peter Williams, Melanie Flint, and Thumuluru Kavitha Madhuri. 2025. "Perioperative Risk Prediction in Major Gynaecological Oncology Surgery: A National Diagnostic Survey of UK Clinical Practice" Diagnostics 15, no. 13: 1723. https://doi.org/10.3390/diagnostics15131723
APA StyleSevinyan, L., Tailor, A., Prabhu, P., Williams, P., Flint, M., & Madhuri, T. K. (2025). Perioperative Risk Prediction in Major Gynaecological Oncology Surgery: A National Diagnostic Survey of UK Clinical Practice. Diagnostics, 15(13), 1723. https://doi.org/10.3390/diagnostics15131723