
Two Cases of Chronic Tubular Necrosis Presenting as Fanconi Syndrome Induced by Red Yeast Rice Choleste-Help

 ,
,
Abstract
1. Introduction
2. Case Reports
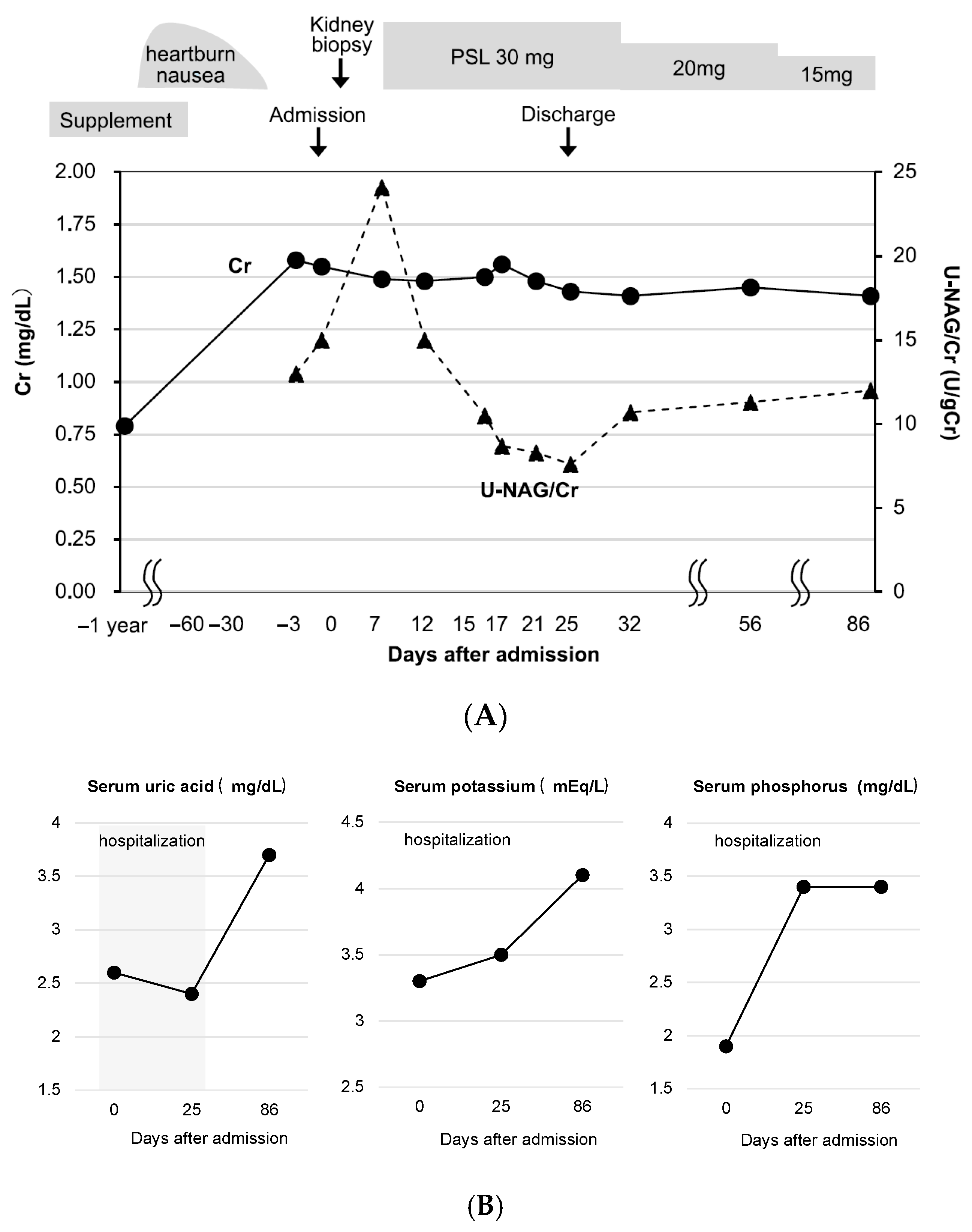
2.1. Case 1
2.2. Case 2
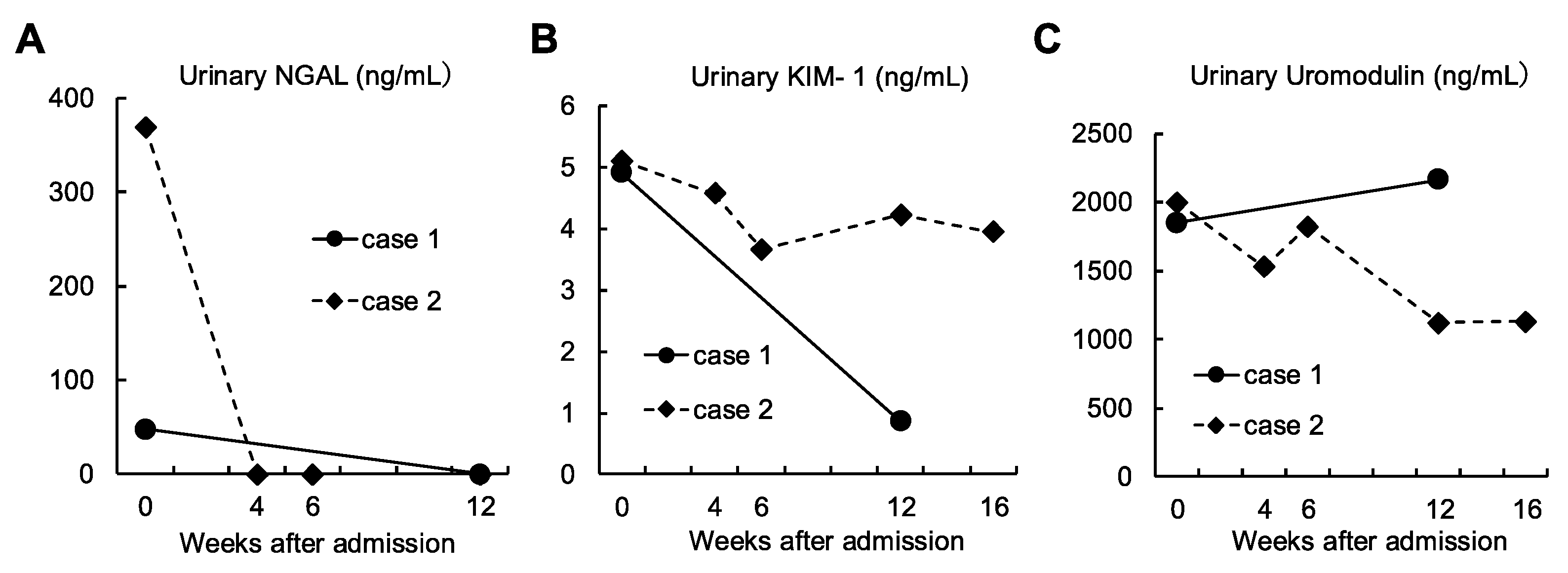
2.3. Evaluation of AKI Markers
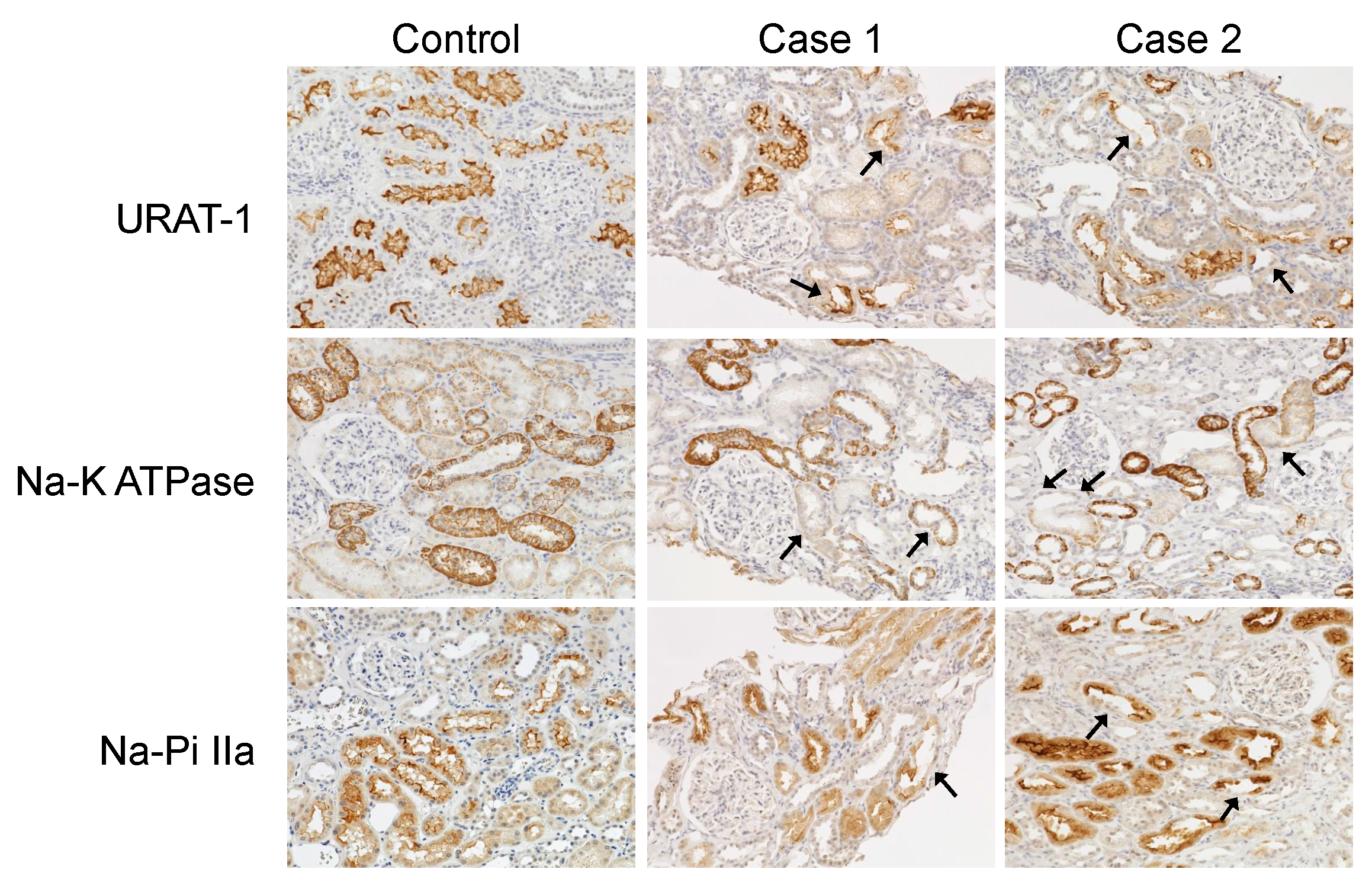
2.4. Renal Transporter Expression by Immunostaining
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vanherweghem, J.L.; Depierreux, M.; Tielemans, C.; Abramowicz, D.; Dratwa, M.; Jadoul, M.; Richard, C.; Vandervelde, D.; Verbeelen, D.; Vanhaelen-Fastre, R.; et al. Rapidly progressive interstitial renal fibrosis in young women: Association with slimming regimen including Chinese herbs. Lancet 1993, 341, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Depierreux, M.; Van Damme, B.; Vanden Houte, K.; Vanherweghem, J.L. Pathologic aspects of a newly described nephropathy related to the prolonged use of Chinese herbs. Am. J. Kidney Dis. 1994, 24, 172–180. [Google Scholar] [CrossRef]
- Cronin, A.J.; Maidment, G.; Cook, T.; Kite, G.C.; Simmonds, M.S.; Pusey, C.D.; Lord, G.M. Aristolochic acid as a causative factor in a case of Chinese herbal nephropathy. Nephrol. Dial. Transplant. 2002, 17, 524–525. [Google Scholar] [CrossRef] [PubMed]
- Debelle, F.D.; Vanherweghem, J.L.; Nortier, J.L. Aristolochic acid nephropathy: A worldwide problem. Kidney Int. 2008, 74, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.T.; Chen, Y.C.; Fang, J.T.; Huang, C.C. Star fruit (Averrhoa carambola) intoxication: An important cause of consciousness disturbance in patients with renal failure. Ren. Fail. 2002, 24, 379–382. [Google Scholar] [CrossRef]
- Hashimoto, T.; Ozaki, A.; Hakariya, H.; Takahashi, K.; Tanimoto, T. The Beni-Koji scandal and Japan’s unique health food system. Lancet 2024, 403, 2287–2288. [Google Scholar] [CrossRef]
- Shinzawa, M.; Matsui, I.; Doi, Y.; Matsumoto, A.; Takahashi, A.; Nangaku, M.; Isaka, Y. A nationwide questionnaire study evaluated kidney injury associated with Beni-koji tablets in Japan. Kidney Int. 2024, 107, 530–540. [Google Scholar] [CrossRef]
- Tanaka, S.; Masumoto, N.; Makino, T.; Matsushima, Y.; Morikawa, T.; Ito, M. Novel compounds isolated from health food products containing beni-koji (red yeast rice) with adverse event reports. J. Nat. Med. 2024, 78, 845–848. [Google Scholar] [CrossRef]
- Foreman, J.W. Fanconi Syndrome. Pediatr. Clin. N. Am. 2019, 66, 159–167. [Google Scholar] [CrossRef]
- Hall, A.M.; Bass, P.; Unwin, R.J. Drug-induced renal Fanconi syndrome. QJM Int. J. Med. 2013, 107, 261–269. [Google Scholar] [CrossRef]
- Habuka, M.; Hosojima, M.; Yata, Y.; Kurumada, K.; Yamagiwa, M.; Yonezawa, M.; Sudo, M.; Kabasawa, H.; Ogawa, A.; Hama, H.; et al. Fanconi syndrome with acute proximal tubular injury induced by a dietary supplement containing beni-koji: A case series report. BMC Nephrol. 2024, 25, 446. [Google Scholar] [CrossRef] [PubMed]
- Iwamura, N.; Tsutsumi, K.; Yamada, S.; Uesugi, N.; Hamashoji, T.; Arita, Y.; Deguchi, T.; Nakano, T. Subclinical acute tubular necrosis potentially associated with red yeast rice consumption unexpectedly detected in a patient with membranous nephropathy. CEN Case Rep. 2024. [Google Scholar] [CrossRef] [PubMed]
- Kawai, Y.; Ozawa, M.; Isomura, A.; Mitsuhashi, H.; Yamaguchi, S.; Nagayama, S.; Tanaka, S.; Abe, E.; Saka, S.; Nagahama, K. A case of Fanconi syndrome that developed following a year of consumption of a red yeast rice supplement. CEN Case Rep. 2024, 14, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Maiguma, M.; Kihara, M.; Hamaguchi, M.; Kobayashi, T.; Yamada, K.; Takagi, M.; Saeki, H.; Gohda, T.; Suzuki, Y. Successful treatment of acute tubulointerstitial nephritis probably due to Benikoji CholesteHelp®, a supplement containing red yeast rice. CEN Case Rep. 2025, 14, 24–28. [Google Scholar] [CrossRef]
- Matsui-Hosoya, R.; Sato, K.; Yagasaki, M.; Hirose, H.; Fukao, Y.; Kano, T.; Io, H.; Suzuki, Y. Fanconi syndrome following administration of oral supplements containing red yeast rice: Several months follow-up of three cases. CEN Case Rep. 2025, 14, 468–476. [Google Scholar] [CrossRef]
- Miyazaki, R.; Takahashi, Y.; Kawamura, T.; Ueda, H.; Tsuboi, N.; Yokoo, T. Acute kidney tubular injury after ingestion of red yeast rice supplement. Clin. Kidney J. 2024, 17, sfae151. [Google Scholar] [CrossRef]
- Oda, K.; Murata, T.; Tanaka, F.; Oda, H.; Tsujimoto, K.; Fukumori, A.; Yamawaki, M.; Saiki, R.; Suzuki, Y.; Katayama, K. A case of acute kidney injury and Fanconi syndrome while taking multiple supplements, including Red Yeast Rice Cholesterol Help®. CEN Case Rep. 2025, 14, 47–51. [Google Scholar] [CrossRef]
- Takeuchi, K.; Kawamura, S.; Wada, Y.; Sakamoto, E.; Kuno, H.; Sakurabayashi, S.; Motohashi, T.; Okawa, H.; Kawamura, N.; Naito, S. Renal Impairment of Proximal Tubular Injury Caused by Red Yeast Rice Supplement: Report of 2 Cases. Case Rep. Nephrol. Dial. 2024, 14, 128–137. [Google Scholar] [CrossRef]
- Maruyama, H.; Sada, K.-E.; Oka, M.; Yanai, M.; Hidaka, S.; Kobayashi, S. Successful Resolution of Suspected Red Yeast Rice-Induced Nephropathy. Intern. Med. 2025. [Google Scholar] [CrossRef]
- Katayama, Y.; Miyazaki, R.; Takahashi, Y.; Kawamura, T.; Tsuboi, N.; Yokoo, T. Recurrent acute kidney injury with Fanconi syndrome related to red yeast rice supplement. CEN Case Rep. 2025, 14, 178–182. [Google Scholar] [CrossRef]
- Chikasue, A.; Taguchi, K.; Iwatani, R.; Kimura, K.; Okuda, S.; Uesugi, N.; Fukami, K. Three Cases of Red Yeast Rice-Containing Supplement-Induced Acute Kidney Injury and Fanconi Syndrome. Am. J. Kidney Dis. 2025, 85, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Kamada, A.; Hirose, T.; Hashimoto, H.; Konya, Y.; Sato, F.; Ishiyama, K.; Joh, K.; Yumura, W.; Mori, T. Tubular damage and SGLT2 expression in a patient with Beni-koji tablet-associated acute kidney injury and Fanconi syndrome. CEN Case Rep. 2025, 14, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Abe, M.; Ogawa, T.; Magome, N.; Ono, Y.; Tojo, A. Element analysis applied to investigate acute kidney injury induced by red yeast rice supplement. Med. Mol. Morphol. 2025, 58, 53–61. [Google Scholar] [CrossRef]
- Uchiyama, K.; Otani, M.; Chigusa, N.; Sugita, K.; Matsuoka, R.; Hosoya, K.; Komuta, M.; Ito, J.; Washida, N. Acute Kidney Injury Associated With Red Yeast Rice (Beni-Kōji) Supplement: A Report of Two Cases. Kidney Med. 2024, 6, 100908. [Google Scholar] [CrossRef]
- Murata, Y.; Hemmi, S.; Akiya, Y.; Miyasato, K.; Kobayashi, H.; Maruyama, T.; Abe, M. Certain Red Yeast Rice Supplements in Japan Cause Acute Tubulointerstitial Injury. Kidney Int. Rep. 2024, 9, 2824–2828. [Google Scholar] [CrossRef] [PubMed]
- Koshida, T.; Fukuhara, K.; Abe, K.; Kato, A.; Fukuda, H.; Takahara, H.; Tomita, S.; Suzuki, Y.; Suzuki, H. Renal Injuries Induced by Supplements Containing Red Yeast Rice. Intern. Med. 2025, 64, 1195–1198. [Google Scholar] [CrossRef]
- Yoshikawa, Y.; Anzai, H.; Odajima, K.; Asakawa, S.; Arai, S.; Yamazaki, O.; Tamura, Y.; Ohashi, R.; Shibata, S.; Fujigaki, Y. Fanconi syndrome and renal tubular necrosis in patients following ingestion of potentially contaminated red yeast rice supplement: Two case reports. Physiol. Rep. 2024, 12, e70049. [Google Scholar] [CrossRef]
- Pruijm, M.; Ponte, B.; Ackermann, D.; Paccaud, F.; Guessous, I.; Ehret, G.; Pechère-Bertschi, A.; Vogt, B.; Mohaupt, M.G.; Martin, P.-Y. Associations of urinary uromodulin with clinical characteristics and markers of tubular function in the general population. Clin. J. Am. Soc. Nephrol. 2016, 11, 70–80. [Google Scholar] [CrossRef]
- Tojo, A.; Asaba, K.; Kinugasa, S.; Ikeda, Y.; Shintani, Y.; Fukayama, M.; Nangaku, M. The reduced expression of proximal tubular transporters in acquired Fanconi syndrome with κ light chain deposition. Med. Mol. Morphol. 2016, 49, 48–52. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Fanconi Syndrome | K (mEq/L) | FEK (%) | P (mg/dL) | FEP (%) | UA (mg/dL) | FEUA (%) | Urine Glucose | Metabolic Acidosis | HCO3- (mEq/L) | Reference No. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 49 | F | + | 2.2 | 19.9 | 1.2 | 27.2 | 1.4 | 51.2 | 4+ | + | 16.7 | [12] |
| 2 | 68 | F | + | 2.4 | 64.2 | 2.4 | unknown | 2.4 | unknown | 3+ | + | 13.6 | [12] |
| 3 | 74 | M | - | 4.1 | unknown | unknown | unknown | 7.9 | unknown | - | - | unknown | [13] |
| 4 | 56 | F | + | 3.2 | 16.9 | 1.4 | 59.2 | 1.4 | 68.7 | 3+ | + | 15.6 | [14] |
| 5 | 58 | F | + | 4.3 | unknown | 2.9 | unknown | 1.7 | unknown | 3+ | - | unknown | [15] |
| 6 | 59 | F | + | 2.5 | unknown | 3.3 | (%TRP) 61.7 | 1.9 | 45.3 | 4+ | + | 14.3 | [16] |
| 7 | 48 | M | - | 3.9 | unknown | 2.7 | unknown | 6.6 | unknown | - | - | unknown | [16] |
| 8 | 47 | F | + | 4.1 | unknown | 1.6 | (%TRP) 73.8 | 3.1 | 23.7 | 1+ | - | unknown | [16] |
| 9 | 47 | F | + | 3.6 | unknown | 3.7 | unknown | 2.5 | unknown | 4+ | - | unknown | [17] |
| 10 | 62 | M | + | 2.8 | 10.8 | 1.1 | 55.3 | 1 | 51.1 | 4+ | - | unknown | [18] |
| 11 | 66 | F | + | 3.6 | unknown | 1 | unknown | 1.4 | unknown | 3+ | unknown | unknown | [19] |
| 12 | 54 | M | + | 3.3 | unknown | 3.1 | unknown | 2.8 | unknown | - | unknown | unknown | [19] |
| 13 | 52 | F | + | 3.3 | unknown | 2 | unknown | 1.7 | unknown | 4+ | + | 18.9 | [20] |
| 14 | 51 | F | + | 2.7 | unknown | 2.6 | unknown | 2.2 | unknown | 3+ | + | 17.9 | [21] |
| 15 | 49 | F | + | 3.3 | unknown | 3 | unknown | 8.1 | unknown | 3+ | + | 13.5 | [22] |
| 16 | 55 | M | + | 2.5 | unknown | 2 | unknown | 1.2 | unknown | 4+ | + | 15.5 | [22] |
| 17 | 60 | F | + | 1.9 | unknown | 3 | unknown | 1.8 | unknown | 4+ | + | 10.5 | [22] |
| 18 | 51 | F | + | 4.1 | unknown | 1.6 | 73.8 | 3.1 | 23.7 | 1+ | - | unknown | [23] |
| 19 | 50 | M | + | 2.8 | 48.8 | 2.4 | (%TRP) 20.4 | 1.8 | 84 | 4+ | + | 9.6 | [24] |
| 20 | 56 | F | + | 3.5 | unknown | 1.9 | unknown | 1.9 | unknown | 4+ | + | 20.4 | [25] |
| 21 | 56 | M | unknown | unknown | unknown | unknown | unknown | unknown | unknown | 4+ | + | unknown | [25] |
| 22 | 73 | F | + | 3.2 | unknown | 1.4 | unknown | 1.6 | unknown | unknown | + | 15.4 | [26] |
| 23 | 53 | F | + | 3.4 | unknown | 1.7 | unknown | 1.2 | unknown | unknown | + | 15.7 | [26] |
| 24 | 55 | F | - | 4.2 | unknown | 3.8 | unknown | 3.5 | unknown | unknown | - | unknown | [26] |
| 25 | 42 | M | + | 2.9 | 24.9 | 2 | unknown | 1.2 | 83.4 | 4+ | + | 16.8 | [27] |
| 26 | 83 | F | unknown | 2.7 | unknown | 3.3 | unknown | unknown | unknown | unknown | unknown | unknown | [27] |
| 27 | 43 | M | + | 3.4 | 17.5 | 1.8 | (Tmp/GFP) 0.87 mg/dL | 1.7 | 42 | 3+ | + | 18.1 | [28] |
| 28 | 57 | F | + | 3.7 | 13.7 | 1.7 | (Tmp/GFP) 0.87 mg/dL | 1.6 | 43.4 | 4+ | + | 20.3 | [28] |
| Our Case 1 | 44 | M | + | 3.5 | 14 | 2.7 | (%TRP) 74.6 | 3.4 | 22.3 | 3+ | - | 24.2 | |
| Our Case 2 | 57 | F | + | 3.2 | 17.8 | 1.5 | (%TRP) 53.0 | 1.3 | 58.4 | 4+ | + | 22.1 |
| Case | Glomerular Injury | Acute Tubular Necrosis | Tubular Atrophy | Tubulointerstitial Cell Infiltration | Immunostaining | Reference No. |
|---|---|---|---|---|---|---|
| 1 | Minor glomerular abnormality | + | + | - | Megalin was expressed in the injured tubular epithelium. | [12] |
| 2 | Minor glomerular abnormality | + | + | - | Megalin was expressed in the injured tubular epithelium. | [12] |
| 3 | Membranous nephropathy | + | + | - | not performed | [13] |
| 4 | Minor glomerular abnormality | + | + | ± | not performed | [14] |
| 5 | Minor glomerular abnormality | + | + | Lymphocyte and plasmacyte | not performed | [15] |
| 6 | Minor glomerular abnormality | + | + | + | not performed | [16] |
| 7 | unknown | unknown | unknown | unknown | not performed | [16] |
| 8 | unknown | unknown | unknown | unknown | not performed | [16] |
| 9 | Some glomeruli showed global sclerosis, while others showed no abnormality. | + | - | - | not performed | [17] |
| 10 | Minor glomerular abnormality | + | - | - | not performed | [18] |
| 11 | Minor glomerular abnormality | + | - | - | not performed | [19] |
| 12 | Minor glomerular abnormality | + | - | Inflammatory cells | not performed | [19] |
| 13 | Minor glomerular abnormality | + | - | Mild lymphocytic infiltration | not performed | [20] |
| 14 | Minor glomerular abnormality | + | + | ± | not performed | [21] |
| 15 | Minor glomerular abnormality | + | + | Mainly CD3+ T lymphocytes | not performed | [22] |
| 16 | unknown | unknown | unknown | unknown | not performed | [22] |
| 17 | unknown | unknown | unknown | unknown | not performed | [22] |
| 18 | Minor glomerular abnormality | + | + | - | SGLT2 expression was reduced in KIM-1 positive injured tubular cells. SGLT1 or GLUT2 staining showed no remarkable change. | [23] |
| 19 | Minor glomerular abnormality | + | + | - | not performed | [24] |
| 20 | Minor glomerular abnormality | + | + | insignificant | not performed | [25] |
| 21 | No abnormalities except diabetic nephropathy | + | + | insignificant | not performed | [25] |
| 22 | Minor glomerular abnormality | + | + | + | not performed | [26] |
| 23 | Minor glomerular abnormality | + | + | Severe inflammatory cell infiltration | not performed | [26] |
| 24 | Minor glomerular abnormality | + | + | Severe inflammatory cell infiltration | not performed | [26] |
| 25 | Minor glomerular abnormality | + | + | - | not performed | [27] |
| 26 | unknown | unknown | unknown | unknown | not performed | [27] |
| 27 | Minor glomerular abnormality | + | + | Mild mononuclear cell infiltration | NCC positive cells occasionally desquamated. | [28] |
| 28 | Minor glomerular abnormality | + | + | Focal inflammatory cell infiltration | NCC were preserved. | [28] |
| Our Case 1 | Mild mesangial matrix expansion | + | - | Focal inflammatory cell infiltration | Decreased staining of URAT-1, Na-K ATPase, and Na-Pi II was observed in some tubular segments. | |
| Our Case 2 | Some glomeruli showed segmental sclerosis, while others showed no abnormality. | + | - | Focal inflammatory cell infiltration | Decreased staining of URAT-1, Na-K ATPase, and Na-Pi II was observed in some tubular segments. |
| Case | Treatment | Serum Cr Level (mg/dL) | Reference No. | |
|---|---|---|---|---|
| Before Treatment | After Treatment | |||
| 1 | - | 1.5 | 0.74 | [12] |
| 2 | - | 3 | 1.34 | [12] |
| 3 | PSL 40 mg | 1.21 | 0.98 | [13] |
| 4 | PSL 30 mg | 1.39 | 0.93 | [14] |
| 5 | PSL 20 mg | 1.57 | unknown | [15] |
| 6 | - | 2.32 | 0.96 | [16] |
| 7 | - | 0.87 | 0.92 | [16] |
| 8 | - | 1.05 | 1.13 | [16] |
| 9 | PSL 40 mg | 4.7 | 1.72 | [17] |
| 10 | - | 1.43 | 1.21 | [18] |
| 11 | - | 1.74 | 1.09 | [19] |
| 12 | - | 1.31 | unknown | [19] |
| 13 | - | 2.28 | 0.73 | [20] |
| 14 | - | 3.18 | 1.59 | [21] |
| 15 | PSL 50 mg | 21.9 | 1.66 | [22] |
| 16 | - | 2.33 | 1.08 | [22] |
| 17 | - | 3.71 | 1.11 | [22] |
| 18 | PSL 30 mg→discontinued five days after initiation | 1.1 | 0.79 | [23] |
| 19 | - | 3.99 | 1.88 | [24] |
| 20 | - | 1.89 | 1.04 | [25] |
| 21 | PSL 30 mg | 13.55 | 1.69 | [25] |
| 22 | PSL (dosage was not mentioned) | 1.27 | unknown | [26] |
| 23 | Steroid pulse and PSL (dosage was not mentioned) | 1.41 | unknown | [26] |
| 24 | Steroid pulse and PSL (dosage was not mentioned) | 2.38 | unknown | [26] |
| 25 | mPSL 500 mg for 3 days, followed by PSL 30 mg | 2.12 | 1.03 | [27] |
| 26 | - | 3.52 | Not recovered | [27] |
| 27 | - | 1.96 | 0.9 | [28] |
| 28 | - | 1.75 | 1.3 | [28] |
| Our Case 1 | PSL 30 mg | 1.58 | 1.41 | |
| Our Case 2 | PSL 30 mg | 1.27 | 1.09 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mita, K.; Takahashi, S.; Yanagida, S.; Aoyama, A.; Shiraishi, T.; Hamada, T.; Nakamura, Y.; Sato, M.; Hirose, K.; Yamamoto, R.; et al. Two Cases of Chronic Tubular Necrosis Presenting as Fanconi Syndrome Induced by Red Yeast Rice Choleste-Help. Diagnostics 2025, 15, 1722. https://doi.org/10.3390/diagnostics15131722
Mita K, Takahashi S, Yanagida S, Aoyama A, Shiraishi T, Hamada T, Nakamura Y, Sato M, Hirose K, Yamamoto R, et al. Two Cases of Chronic Tubular Necrosis Presenting as Fanconi Syndrome Induced by Red Yeast Rice Choleste-Help. Diagnostics. 2025; 15(13):1722. https://doi.org/10.3390/diagnostics15131722
Chicago/Turabian StyleMita, Kanako, Shunsuke Takahashi, Satoshi Yanagida, Akihiro Aoyama, Takayuki Shiraishi, Takayuki Hamada, Yumiko Nakamura, Mariko Sato, Kento Hirose, Ryo Yamamoto, and et al. 2025. "Two Cases of Chronic Tubular Necrosis Presenting as Fanconi Syndrome Induced by Red Yeast Rice Choleste-Help" Diagnostics 15, no. 13: 1722. https://doi.org/10.3390/diagnostics15131722
APA StyleMita, K., Takahashi, S., Yanagida, S., Aoyama, A., Shiraishi, T., Hamada, T., Nakamura, Y., Sato, M., Hirose, K., Yamamoto, R., Shioda, Y., Takayanagi, K., Nagayama, I., Ono, Y., Hasegawa, H., & Maeshima, A. (2025). Two Cases of Chronic Tubular Necrosis Presenting as Fanconi Syndrome Induced by Red Yeast Rice Choleste-Help. Diagnostics, 15(13), 1722. https://doi.org/10.3390/diagnostics15131722