1. Introduction
Multiple myeloma (MM) is a hematological cancer derived from plasma cells, often defined by the presence of a monoclonal immunoglobulin. It accounts for 1% of cancers and about 10% of hematological malignancies. And findings during the course of the disease may include anemia, leukopenia, thrombocytopenia, renal failure, severe pain, bone fractures, and hypercalcemia [
1,
2,
3,
4]. However, almost all multiple myelomas arise from an asymptomatic premalignant condition called monoclonal gammopathy of undetermined significance (MGUS). This is diagnosed after more than 10 years of the disorder in 50% [
5,
6,
7]. Effective multi-drug regimens are available for most forms of MM, resulting in long-term remission. However, because of the disease’s biology, relapse remains frequent, and MM remains incurable due to the emergence of treatment resistance [
8,
9,
10]. MM has variable clinical findings, non-specific symptoms, as seen in diabetes, arthritis, or chronic renal failure, which can all lead to a late diagnosis [
11], especially in elderly patients, where there are many differential diagnoses mimicking MM. MGUS affects ~3% of individuals over age 50, while SMM is found in 0.5–1%. In comparison, hypertension and diabetes affect ~40% and ~25% of the same population, respectively [
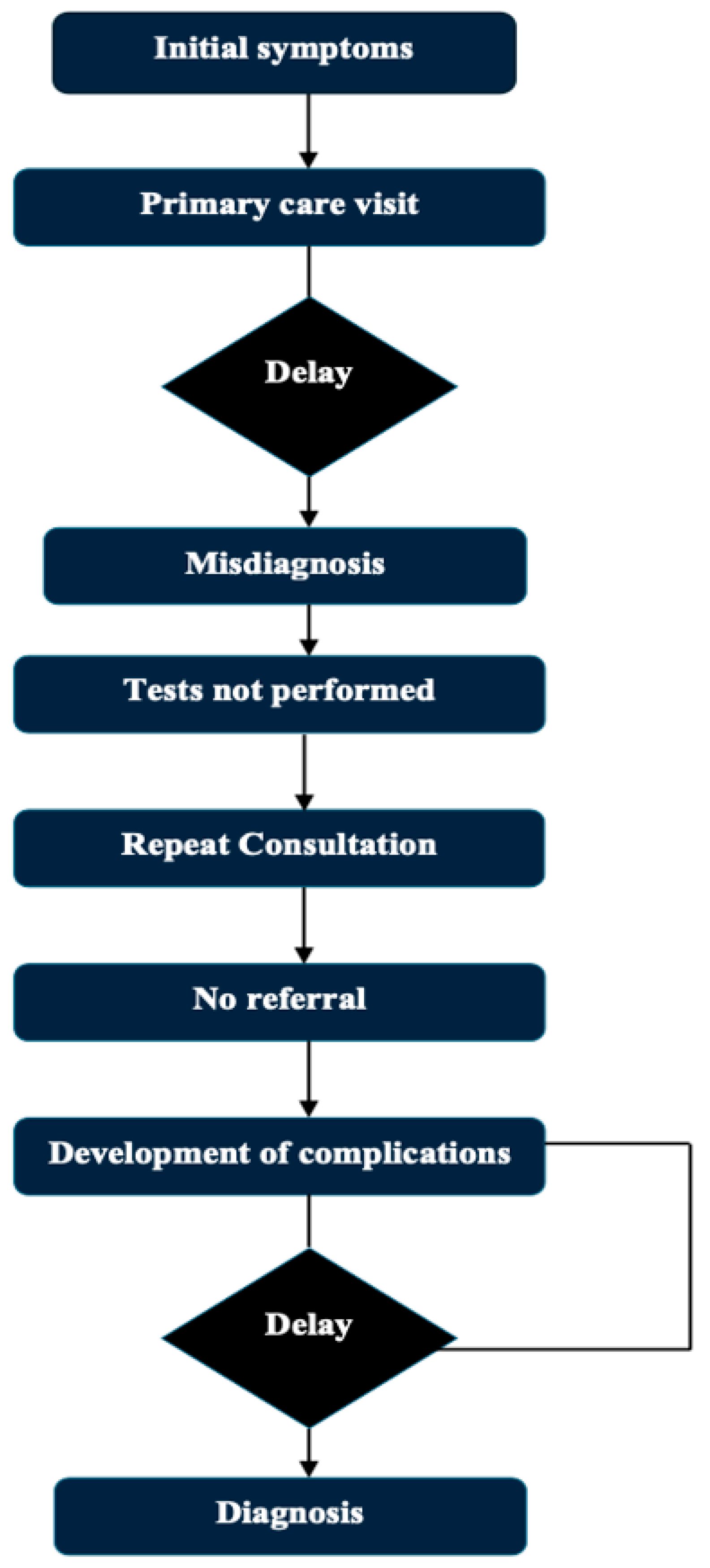
11]. Patients often develop these symptoms and present to primary healthcare providers or other specialists, giving rise to delays in referrals to hematologists. Delayed diagnosis of the disease can negatively impact patients’ quality of life and prognosis [
12]. The routine path to diagnosis of multiple myeloma and possible delays is presented in
Figure 1. Existing reviews and articles on this topic are sparse. The objective of this review is to present and evaluate the multifactorial factors which create and perpetuate delays in the diagnoses of multiple myeloma, highlight barriers that exist at the patient, physician, and system perspective level, present potential strategies that may facilitate earlier diagnoses and earlier interventions, and provide supplemental data to fill gaps in the existing literature to foster academic progress in this area.
To the best of our knowledge, there is currently no systematic integrative review that combines diagnostic delays to multiple myeloma with system gaps in healthcare, AI-guided approaches, or biomarker-related strategies. This gap is addressed in the present manuscript, which offers an interdisciplinary synthesis covering clinical, diagnostic, and technological fields.
2. Literature Search Strategy
A scoping literature review was conducted to evaluate studies addressing diagnostic dilemmas and delays in multiple myeloma (MM), early detection strategies, and the use of artificial intelligence (AI) and biomarker-based tools. The search was performed in PubMed, Embase, and the Cochrane Library covering the period from January 2010 to March 2024.
The following keywords and Boolean combinations were used: “multiple myeloma” AND (“diagnostic delay” OR “delayed diagnosis”) AND (“artificial intelligence” OR “biomarkers” OR “early detection” OR “MGUS” OR “smoldering myeloma”).
Only peer-reviewed original articles, meta-analyses, clinical trials, and systematic reviews published in English were included. Studies focusing on adult populations, reporting on diagnostic pathways, delays, outcomes, and systemic barriers to early diagnosis were prioritized.
Titles and abstracts were screened independently by two reviewers, and full-text evaluation was performed for eligible articles. After removing duplicates, a total of 85 studies were included in the final synthesis.
3. Clinical Spectrum of Multiple Myeloma
The symptoms in multiple myeloma are usually non-specific. Its defining symptoms are the CRAB symptoms (hypercalcemia, renal insufficiency, anemia, and bone findings) [
1,
2,
3,
4]. Among 1027 multiple myeloma patients included in the Czech post-marketing observational study, bone pain was reported at diagnosis by 58% of the patients, and fatigue by 32% of the patients. A total of 73% of the patients had anemia, 48% had elevated creatinine levels, 13% had hypercalcemia, and 79% had bone abnormalities (primarily but not limited to lytic lesions, fractures, and osteoporosis). Other features typically noted are neuropathy, developing infections (recurrent), loss of weight (involuntary), and easy bruising/bleeding [
13].
Because most symptoms are non-specific, they can resemble many other conditions. Diabetes shares some symptoms with multiple myeloma, including excessive thirst and urination, fatigue, frequent infections, and neuropathy [
14]. Likewise, renal sufficiency due to multiple myeloma is difficult to separate from renal insufficiency from diabetes or chronic kidney disease in the absence of directed testing [
15]. Bone pain or low back pain is frequently shrugged off as arthritis or osteoporosis and not taken seriously. This results in delayed diagnosis, which consequently leads to increased morbidity and mortality [
16]. The most frequent presenting clinical symptoms for multiple myeloma, along with potential misunderstandings and diagnostic delays, are outlined in
Table 1.
It has been shown that patients consult at least three specialists before arriving at a hematologist, which can cause a lapse of 3 to 6 months in the diagnostic workup [
17]. Delayed diagnosis is linked with a higher rate of myeloma-related complications and a significant decrease in disease-free survival, but it does not affect the overall survival rate [
18]. Worse outcomes have also been associated with presenting with advanced complications (e.g., severe infections, spinal cord compression, fractures, and renal failure) [
19].
5. Consequences of Early Diagnosis
These challenges result in patients being diagnosed later, receiving treatment more slowly, and experiencing worse clinical outcomes [
48]. Late identification raises the risk of potentially fatal issues in patients [
48]. This results in increased morbidity and mortality, leading to more aggressive initial treatments, which drive up costs [
49]. Those who present with renal failure at diagnosis have limited therapeutic options, and those who present with vertebral fractures have limited mobility, chronic pain, and reduced quality of life [
50]. Moreover, the higher demand for treatment associated with late-stage disease manifests as an increased number of patients requiring hospitalization and intensive care, and it has an impact on the healthcare system, which, in turn, has economic implications [
51]. Delays in diagnosis also lead to more long-term problems, including lower treatment compliance, lower quality of life, loss of workforce productivity, and psychosocial effects [
52]. Hence, early diagnosis of the disease not only has clinical but also economic and social significance in multiple myeloma [
53].
Table 8 provides the clinical and prognostic implications of delayed diagnosis in multiple myeloma.
6. Strategies to Prevent Diagnostic Delays
Diagnostic interval in multiple myeloma is one of the longest in all types of cancer that adversely affect both patient outcomes and a burden on the healthcare system [
36]. Such delays often occur in primary care, since general practitioners (GPs) rarely observe this rare disease clinically [
54]. Moreover, an average GP will see multiple myeloma only once every 8–10 years, making it very unlikely to be suspected early on [
26]. Hence, the enhancement of a GP’s familiarity with myeloma symptomatology and diagnostic pathways, as well as the implementation of diagnostic safety nets for persistent and unexplained symptoms, remains a key strategic priority [
55].
Early diagnosis may easily be established through the recognition of minor abnormalities in routine blood tests, along with the implementation of reflex myeloma screening [
56]. Clinical risk algorithms created for this approach seek to identify high-risk patients based on their electronic health records, utilizing parameters including symptoms, hemoglobin, creatinine, and inflammatory markers [
57] There are technical challenges that still exist with it being integrated into decision support systems, including, alignment with clinical workflows, and figuring out triggering thresholds. Active surveillance of precursor conditions such as MGUS and smoldering multiple myeloma (SMM) is also potentially valuable [
58]. A population-based screening study conducted in Iceland provides one valuable model, during which all MGUS patients were studied, applying different follow-up strategies [
59].
In addition, working with laboratories on early warning systems and proactive collaboration with hematologists can help facilitate diagnoses, particularly in less obvious cases. To facilitate timely referral decisions, critical test results must be interpreted according to pre-defined algorithms and communicated to the clinician with the correct reflex tests [
60]. In addition to their reliance on technological integration, cost-effectiveness, sustainability of their impact on the healthcare system, and diagnostic accuracy must be used to assess early diagnostic strategies. This approach can enhance the early detection of myeloma at a much earlier stage with minimal complications and improve basic clinical endpoints, such as survival [
61]. A graphic comparison of two chosen diagnostic tools according to their speed and sensitivity is presented in
Figure 2.
Early diagnosis of MM may lead to the prevention of end-organ damage, but it is unclear whether this also affects overall survival (OS). Some investigations (e.g., Mateos et al., 2018) indicate that there is no OS benefit, likely emphasizing the relevance of disease biology and cytogenetic profile as more impactful to outcomes than diagnosis timing in general [
62].
The AQUILA trial was a randomized phase III trial investigating the clinical benefit of early treatment in high-risk SMM and was reported in NEJM in 2024. The trial included more than 200 patients who were considered high-risk based on the percentage of bone marrow plasma cells, ratio of serum free light chains, and levels of M-protein. The patients were assigned to up-front, lenalidomide-based therapy or observation. Results The results indicated that the early therapy group had a statistically significant PFS benefit compared with the observation group. But there was no significant difference in OS at the time of data cutoff. Crucially, the organ-protective potential for early intervention seemed restricted. Although there were fewer complications of anemia in the treatment group, there were no significant differences between the two groups in the incidence of bone disease or renal failure. These results indicate that early treatment may postpone disease progression, but that its effect on longer-term outcomes, such as OS and irreversible organ damage, is unknown, which further argues for a personalized treatment strategy in high-risk SMM patients [
63].
Although published cumulative prospective data correlating such delays with survival from multiple myeloma is scant, the studies that have been published show an overwhelming association between late diagnosis and the endpoint of irreversible end-organ damage. For example, Gonsalves et al. (2015) [
64] demonstrated that 21% of the newly diagnosed MM patients had renal failure (defined as serum creatinine ≥ 2 mg/dL), of which 58% fell into ISS stage III at diagnosis. By comparison, just 29% of individuals who did not have renal failure received their diagnosis at this late stage. While diagnostic delay duration was not explicitly addressed by the study, these results suggest that longer symptomatic duration before diagnosis can result in silent disease progression and ensuing renal dysfunction and more aggressive presenting disease. As renal impairment in MM typically progresses gradually, this supports the clinical benefit for early identification and referral in patients with no obvious cause for anemia, energy, or an elevated creatinine [
64]. The association between diagnostic delay and complication onset in multiple myeloma (MM) is complicated. In a previous large retrospective study of 5483 patients using Medicare-SEER linked data, the authors reported a median interval of diagnosis of 99 days after clinical presentation, most often manifested as anemia or back pain. Interestingly, bone pain was reported in 47.5% of patients up to two years before diagnosis, with a median delay of 220 days (interquartile range (IQR) of 80 to 476) from the first symptom of bone pain to the MM diagnosis. Contrary to the belief that long-term delay may contribute to skeletal or renal complications, multivariate analysis revealed that diagnostic delay in itself was not an independent risk factor for complications (OR 0.9, 95% CI: 0.8–1.1). Complicated rather than non-complicated lesions were more closely related to indicators of disease severity and co-morbidities. However, the results also underscore that nearly half of MM patients presented with early musculoskeletal symptoms; however, imaging or appropriate diagnostic workup was not performed in a significant number, with only 60% undergoing imaging in the setting of bone symptoms. This highlights the need for clinical awareness in patients with unknown bone pain, anemia, and renal involvement, particularly in elderly patients [
24,
29]. As summarized in
Table 9, several studies have investigated the association between diagnostic delay and clinical complications in MM.
While the discovery of precursor conditions such as MGUS and SMM theoretically can identify who will ultimately progress to active disease, identification and early intervention are currently controversial. Bianchi et al. (Blood 2010) noted that the finding of MGUS in screening or other settings (e.g., incidental discovery during workup for some nonsymptomatic matter) might result in overdiagnosis and unnecessary counseling, testing, or procedures for the condition [
65].
In addition, the current iStopMM (Iceland Screens, Treats, or Prevents Multiple Myeloma) trial is designed to determine the value of population-wide screening, although final results are pending, and to date, no data exist to support routine screening practices [
62].
7. Future Perspectives and Research Areas
Sufficient studies on enhanced diagnostic and prognostic markers are ongoing due to the rising incidence of multiple myeloma (MM) cases and the burdens and delays in diagnosis [
66]. MiRNAs, angiogenic factors, Extracellular Matrix proteins, telomeres, and telomerase activities are newer biomarkers with promising capabilities in the diagnostics and prognostics of MM [
67]. Ongoing studies on methodologies such as blood biopsy, which could permit earlier disease detection than the still gold-standard invasive bone marrow biopsy but still allow more frequent and less painful measurements through the variants in circulating tumor cells (CTCs), miRNAs, and cell-free circulating DNA (cfDNA) in peripheral circulation [
68].
As with other sectors, there is a growing use of artificial intelligence in medicine. As the number of cases of multiple myeloma increases, so does the volume of data that has been gathered [
69]. Such data can be processed using machine learning and deep learning models to expand the knowledge and better understand myeloma mechanisms to better manage MM patients [
70,
71].
AI-based diagnostic support systems have held great promise in the early detection of multiple myeloma (MM) and its precursor states. Some recent works have used machine learning (ML) models on routine laboratory results to increase diagnostic performance. For instance, Fan et al. (2022) constructed a random forest classifier model combining CBC and metabolic panel information, with an AUC of 0.968 and an accuracy of 92.6% for differentiation of MGUS and active MM [
72]. Similarly, Allegra et al. (2022) reviewed several deep learning-based approaches and reported that convolutional neural networks (CNNs) applied to bone marrow aspirate images and clinical datasets achieved diagnostic accuracies exceeding 90% [
70]. These results highlight that AI tools could be integrated into electronic medical records to serve as early alert systems, especially for patients with non-specific symptoms like fatigue or anemia. Concurrently, biology-based approaches, including the sFLC ratio, B2M, and bone-marrow-derived B-cell maturation antigen, are gaining more traction as potential diagnostic adjuncts. Instead, emerging markers such as BCMA have the potential to be prioritized in both diagnosis and therapeutic targets, like sFLC and beta-2 microglobulin, which are part of the current diagnostic criteria. But, in spite of encouraging retrospective results, there is a paucity of prospective validation and real-world adoption for these technologies, particularly for resource-limited health systems [
70,
72]. These findings suggest that AI-powered tools can be effectively integrated into electronic medical records as early alert systems, particularly for patients presenting with non-specific symptoms such as fatigue or anemia. In parallel, biology-driven approaches—such as the serum free light chain (sFLC) ratio, beta-2 microglobulin (B2M), and bone marrow–derived B-cell maturation antigen (BCMA)—are also gaining prominence as valuable diagnostic adjuncts. Emerging markers like BCMA not only offer diagnostic utility but also serve as potential therapeutic targets, similar to sFLC and B2M, which are already part of current diagnostic criteria. However, despite promising retrospective data, there remains a significant lack of prospective validation and limited real-world application of these technologies, particularly in resource-limited healthcare systems.
Despite the potential shown by AI models and biomarkers for multiple myeloma, there are several obstacles to their real-world use. First, many AI models that show high diagnostic accuracy have been trained and tested on retrospective data, often in artificial academic settings. Even if an algorithm is already ready for use in primary care or community oncology, this often necessitates standardized data entry, tight integration with electronic health records, and trained clinicians. These resources may be scarce beyond the walls of a large academic medical center. In addition, many healthcare systems lack developed frameworks for the regulatory approval of AI-assisted diagnostics, leading to a legal vacuum around clinical responsibility. The same is true for biomarkers like serum free light chains and BCMA, which are both diagnostically and prognostically useful. However, cost, laboratory platform variation, and the lack of established clinical cutoffs for screening in the absence of symptoms limit implementation. These limitations are magnified in low- and middle-income countries where resource constraints, laboratory infrastructure, and reimbursement policies serve as even more onerous barriers. Thus, while AI and biomarker approaches may be promising, their application in the real world will require prospective testing, clinician education, economic evaluation, and policy reform [
73].
Table 10 summarizes the performance characteristics of selected AI models that have been evaluated for the early detection of multiple myeloma.
MGUS (monoclonal gammopathy of undetermined significance) is a prolonged premalignant phase prior to the development of multiple myeloma [
74]. This phase allows for the study of cancer evolution, for understanding plasma cell neoplasm malignant evolution mechanisms, for identifying MGUS patients with a high risk of progression early, and for eventually designing new therapeutic targets considering previous achievements. This may also delay or extend the process of malignant transformation [
75,
76].
The application of rapid advances in genomic techniques to study how premalignant cells evolve should also allow for the identification and subsequent targeting of driver events during clonal evolution in MM and in cancer more broadly [
76,
77].
Recent advancements have led to the development of AI-driven models aimed at predicting MM risk from routine clinical data. For instance, an XGBoost algorithm trained on 200 electronic health record (EHR) parameters achieved an AUC of 0.84 for 5-year MM risk prediction in a large Clalit dataset (
n = 4256 cases vs. 20:1 controls) [
78]. A simplified logistic regression model from the same study, using only 20 laboratory variables, also showed promising performance (AUC 0.72) [
78]. In addition, natural language processing (NLP) models have been applied to unstructured clinical notes, enabling earlier detection of MGUS/MM cases by several months [
79].
Regarding biomarkers, elevated serum levels of DKK1—linked to skeletal disease—have been proposed as diagnostic markers in MM; capillary electrophoresis assays identified optimal cutoff values (approximately 10 ng/mL) for clinical use [
80]. Moreover, DKK1 and sclerostin—both Wnt pathway inhibitors—correlated with the extent of bone disease and decreased significantly post-treatment [
81]. Although these biomarkers are not yet part of standard diagnostic criteria, they hold potential both for disease monitoring and for guiding therapeutic decisions.
These additions provide concrete evidence and real-world metrics, strengthening the narrative and addressing reviewer concerns about the lack of specific AI and biomarker examples.
8. Conclusions
Multiple myeloma (MM) is the second most common hematological malignancy, yet its diagnosis is frequently delayed due to non-specific symptoms, lack of awareness, and multifactorial barriers involving patients, physicians, and healthcare systems. The majority of MM cases are diagnosed at an advanced stage, increasing morbidity and reducing patients’ quality of life. Although microbiological, serological, and imaging techniques have advanced, their widespread implementation remains limited by standardization issues and resource constraints.
This review highlights multiple avenues for early diagnosis, including raising awareness through educational programs, development of algorithm-based approaches for primary care, integration of artificial intelligence (AI) tools, and the use of biomarker-based risk assessment—especially during the MGUS premalignant phase. Removing obstacles to early diagnosis may effectively reduce morbidity and late-stage complications. However, current evidence does not clearly support a direct correlation between early diagnosis and reduced early mortality, as emphasized by recent studies and ongoing trials (e.g., iStopMM).
Moreover, the early detection of low-risk MGUS, particularly in younger individuals, may lead to overdiagnosis, increased patient anxiety, and unnecessary follow-up or overtreatment. These psychosocial and healthcare burdens should be considered when developing population-based screening strategies. Although guidelines exist for the follow-up of MGUS and SMM, it is not yet proven that such monitoring prevents progression to symptomatic MM or organ damage.
The average interval between initial symptoms and a confirmed MM diagnosis ranges from 6 to 11 months in the literature, with delays exceeding 3 months being associated with higher rates of complications such as anemia or bone disease.
This review contributes to the literature by providing a structured synthesis of diagnostic delays in MM, supported by recent data, and integrating evolving diagnostic approaches including AI and biomarkers. By exposing the interplay between clinical uncertainty, systemic barriers, and delayed recognition, our study offers both practical suggestions and research perspectives that can support earlier and more effective diagnosis strategies in real-world settings.


 ,
, 


{kind=link}
{kind=link}