1. Introduction
According to the Malaysia National Cancer Registry Report 2012–2016, breast cancer is the most common form of cancer affecting women in Malaysia, with an age-standardized incidence rate (ASR) as high as 34.1 per 100,000—this makes it three times more common than colorectal cancer (with an ASR of 11.1), the second most common form of cancer. Most breast cancer cases in Malaysia are diagnosed at stage II, accounting for 37% of all new cases of breast cancer detected from 2007 to 2011 [
1]. Many breast cancer patients experience a decrease in quality of life. This disease can have significant psychological impacts and can induce stress in patients; it is life-threatening, and mastectomies, chemotherapy effects, and disrupted social and daily living activities can cause body image issues. Furthermore, breast cancer can also cause psychological distress or even depression in the patient’s caregiver [
2,
3,
4].
Since the first description of microcalcifications in mastectomy specimens by Solomon in 1913, there were many studies on the relationship and association between microcalcifications and breast diseases and the importance of the radiological–pathological correlation in diagnosing these diseases; this is especially true when assessing radiologically detected microcalcifications in surgically removed breast specimens, which became apparent in the 1970s. The introduction of mammography screening substantially increased the number of diagnosed microcalcification cases and led to physicians realizing their importance in detecting breast carcinomas early [
5].
Mammograms remain the primary screening tool for breast cancer, as recommended by the American College of Radiology and Clinical Practice Guideline (CPG) Malaysia [
6,
7,
8]. According to CPG Malaysia, a screening mammogram is recommended every other year for women aged 50–74 with no risk factor. For women with a high breast cancer risk factor but in whom no genetic variants were identified, an annual screening mammogram is recommended from ages 40 to 59 and every other year after 60 [
6]. At Hospital Canselor Tuanku Muhriz (HCTM), complementary Ultrasounds (USGs) are performed with mammogram studies. Studies showed that combining digital breast tomosynthesis mammograms with USGs can significantly improve diagnostic sensitivity [
9].
Over the years, more women in Malaysia enrolled in the mammography screening program; hence, the identification and investigation of microcalcifications found in mammography became more common [
10]. In some cases, women may not benefit from screening programs because mammogram calcifications might be over-diagnosed. Several studies in the literature report an overdiagnosis rate for mammographic calcifications ranging from 0 to 54% [
11,
12].
There are several manifestations of breast carcinoma in mammography, such as ill-defined, spiculated masses, and clustered, parallel linear, or irregular intraductal calcification microcalcifications [
13,
14]. Microcalcifications in mammograms can exhibit many subtle variations in number, size, shape, extent, density, and distribution patterns. Careful examination is needed to detect mammographic lesions and calcifications; categorize them as benign, suspicious, or malignant; and recommend proper surgical interventions and prognostication [
15]. Therefore, accurately correlating mammographic findings with corresponding histopathologic features is considered one of the essential aspects of mammographic evaluation [
13]. The fifth edition of the BI-RADS lexicon, published in 2013, describes breast microcalcifications and provides diagnostic categories with standardized biopsy recommendations. Despite this, linking descriptive findings with assessment categories is still a challenging diagnostic task in evaluating microcalcifications.
4. Discussion
Mammography is an effective screening test for the timely identification of microcalcifications and can detect 25–43% of non-palpable cancers [
20]. In our study, two BI-RADS 3 lesions were HPE-proven benign lesions, consistent with a malignancy rate of <2%, as stated in ACR BI-RADS Atlas 2013. For BI-RADS 4 lesions, the malignancy rate is 33.3%, consistent with a malignancy rate of 2–95%. However, this study’s malignancy rate for BIRADS 5 microcalcifications/lesions was 88.9%, which was slightly lower than the estimated malignancy rate of >95% [
16,
21]. This lower observed malignancy rate of 88.9% may be attributed to the small sample size, which is a limitation in this study. With a larger sample size, the malignancy rate may closely align with the reference malignancy rates according to the ACR BI-RADS Atlas 2013. One subject with benign histopathology had a BI-RADS 5 lesion. When a benign pathologic test result from a percutaneous biopsy of a BI-RADS 5 lesion is obtained, this is often considered discordant; a repeated biopsy or surgical excision is recommended. However, some benign entities were possibly classified as BI-RADS 5 lesions, including an atypical infection, a complex sclerosing lesion, a radial scar, fat necrosis, fibromatosis, mastitis, and myofibroblastoma [
22]. In this study, HPEs showed fibroadenomatous changes.
Fine pleomorphic calcifications were the most common morphology in our study, at 65.4% among all microcalcification types, followed by amorphous calcifications at 10.9%. However, these two microcalcifications had low PPVs in predicting malignancy: 38.9% and 16.7%. The most common HPE result for these two calcifications was benign breast tissue. These microcalcifications were also commonly seen in benign conditions, such as fibrocystic changes. On the other hand, the morphologies associated with a high PPV were heterogeneous and fine linear or branching pleomorphic microcalcifications, at 75.0% and 66.7% (
Table 8). However, these findings cannot be generalized due to the small sample size. Further studies involving larger cohorts should be conducted to assess the validity of these findings.
Compared with ACR BI-RADS and other studies, our study found that heterogeneous microcalcification was the only morphology with a high PPV. The other microcalcification morphologies were similar, although Kim et al. described the fine pleomorphic morphology as having a higher PPV (63.2%). For the microcalcification distributions, our study found that the regional distribution had a higher PPV (57.1%) than ACR BI-RADS (26%), which was similar to Liberman et al. (46%), while the PPVs of the other distributions were consistent with other studies [
16,
23,
24].
In our study, five patients had increasing calcifications at 1-to-2-year follow-up intervals; however, none of these were malignant lesions. According to a study by Lev-Toaff et al., the fact that microcalcifications appear or increase does not necessarily indicate malignancy, but if microcalcifications give the impression of suspicious characteristics, regardless of their stability over time, histological studies are necessary. However, Lev-Toaff et al. also concluded that the temporal stability of microcalcifications significantly decreases the risk of invasive carcinoma, but not necessarily of carcinoma in situ [
25].
Our study showed that the segmental distribution of microcalcifications had the highest association (OR: 5.5, 95%; CI: 1.146–26.718) with DCIS, followed by the fine linear and branching pleomorphic morphology, with an OR of 3.9 and a 95% CI of 0.744–21.004.
Our study also showed that linear distribution had the highest risk (OR: 6.2, 95% CI: 0.368–104.532) associated with invasive carcinoma, followed by a regional distribution (OR: 2.5, CI 0.449–14.4). Regarding the association between microcalcifications and invasive breast cancer, Lilleborge et al. reported that the fine linear or branching pleomorphic morphology has an OR of 20.0, as compared with fine linear or fine pleomorphic microcalcifications, and the regional distribution has an OR of 2.8, as compared with the segmental or linear distribution [
26]. A comparison of ORs is summarized in
Table 9.
The more specific the test, the less likely an individual with a positive test will be free from disease and the greater the positive predictive value (PPV). The fine pleomorphic morphology showed lower PPV in our study, whereas heterogeneous morphology showed higher PPV in our study as compared to the study by Kim et al. Our study also showed higher PPV in regional distribution as compared to the study by Kim et al. This indicates that our study has a more specific test in terms of detecting heterogenous morphology and regional distribution; but has a less-specific test in terms of detecting fine pleomorphic morphology as compared to the study by Kim et al. [
23]
Nyante et al. reported that calcifications in breast cancer were at the in situ tumor component [
27]. However, our study compared the calcification patterns in benign, in situ, and invasive tumors, and we believe it does not matter whether the calcifications are in the in situ or invasive component, as our objective was to determine the calcification patterns association with different categories. Our focus was to show that in situ and invasive carcinoma have different patterns of calcification.
In our study, there were four cases of TNBC (12.1%) among 33 breast cancers. Two were in the 41–45 age group, and two were in the 61–65 and 66–70 age groups. The incidence of TNBCs in this study was similar to that in previous studies, which reported that they account for approximately 8.1–21.4% of all breast cancers [
28,
29,
30].
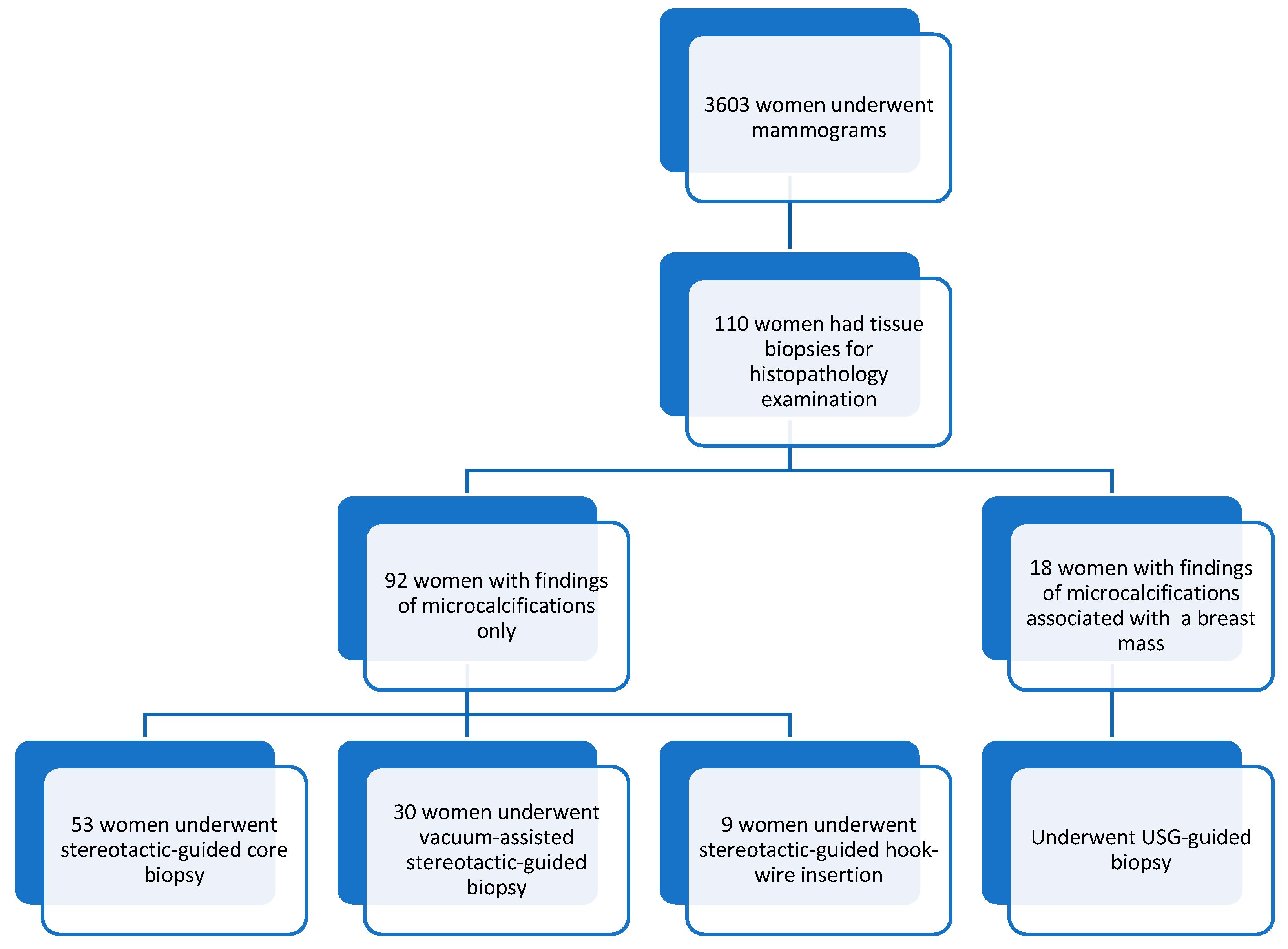
In our study, 17 out of 110 patients (15.5%) with microcalcifications also had an associated breast mass. According to Chotiyano et al., mass findings are a predominant indicator of breast cancer. These malignant masses usually present as high-density lesions with irregular shapes and ill-defined or spiculated margins [
31]. In our study, masses with spiculated, obscured, and microlobulation margins were seen in invasive carcinoma, and high-density masses were more commonly found in invasive carcinoma.
Our study showed that high-density masses have a higher PPV (75%) than equal-density masses (60% PPV). The masses found in mammograms with microlobulation and circumscribed margins had 100% PPVs, followed by those with spiculated margins (75% PPV) and obscured margins (63.5% PPV). These findings were similar to those reported by Liberman et al. [
24].
There were several limitations to this study. First, this study was conducted during the COVID-19 pandemic period, during which Malaysia implemented the Malaysia Government Movement Control Order from 18 March 2020 to 31 December 2021. These measures included restrictions on movement, assembly, and international travel, as well as the closure of business, industry, government, and educational institutions to curb the spread of COVID-19. As a result of these restrictions, the availability of participants for our study was significantly limited. Specifically, all outpatient mammogram screening studies were temporarily withheld for several months. During this time, mammogram studies were only conducted on symptomatic women. Additionally, the screening program resumed with a limited number of appointments due to the deployment of almost half of the working forces to manage COVID-19 wards, emergency department rotations, and quarantine centers. Given these challenging circumstances, our study faced inherent limitations in terms of the available population size. Despite the constraints, we believe that our findings provide valuable insights into the specific population of symptomatic women during the COVID-19 pandemic. However, we acknowledge the importance of expanding the study population in future research to obtain more comprehensive results.
Second, it included a relatively small number of patients presenting at a single center; therefore, the results cannot be generalized. Third, in view of the retrospective design, case selection bias possibly occurred because we included only patients who underwent imaging-guided biopsies or surgeries for suspicious microcalcifications. Fourth, unavoidably uneven suspicious microcalcification distributions were included in this study, with a high incidence of fine pleomorphic morphology and grouped distribution and a low incidence of the other morphologies and distributions.
Additionally, we took the opportunity to expand upon the limitations of our study and acknowledge the need for future research to address these limitations. This includes considerations for larger sample sizes, multicenter collaborations, and further investigations into the associations between microcalcification patterns and specific breast cancer subtypes.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}