
Assessing Sternal Dimensions for Sex Classification: Insights from a Greek Computed Tomography-Based Study

 ,
,  ,
,  ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Multidetector Computed Tomography (MDCT) Protocol
2.3. Image Post-Processing and Analysis
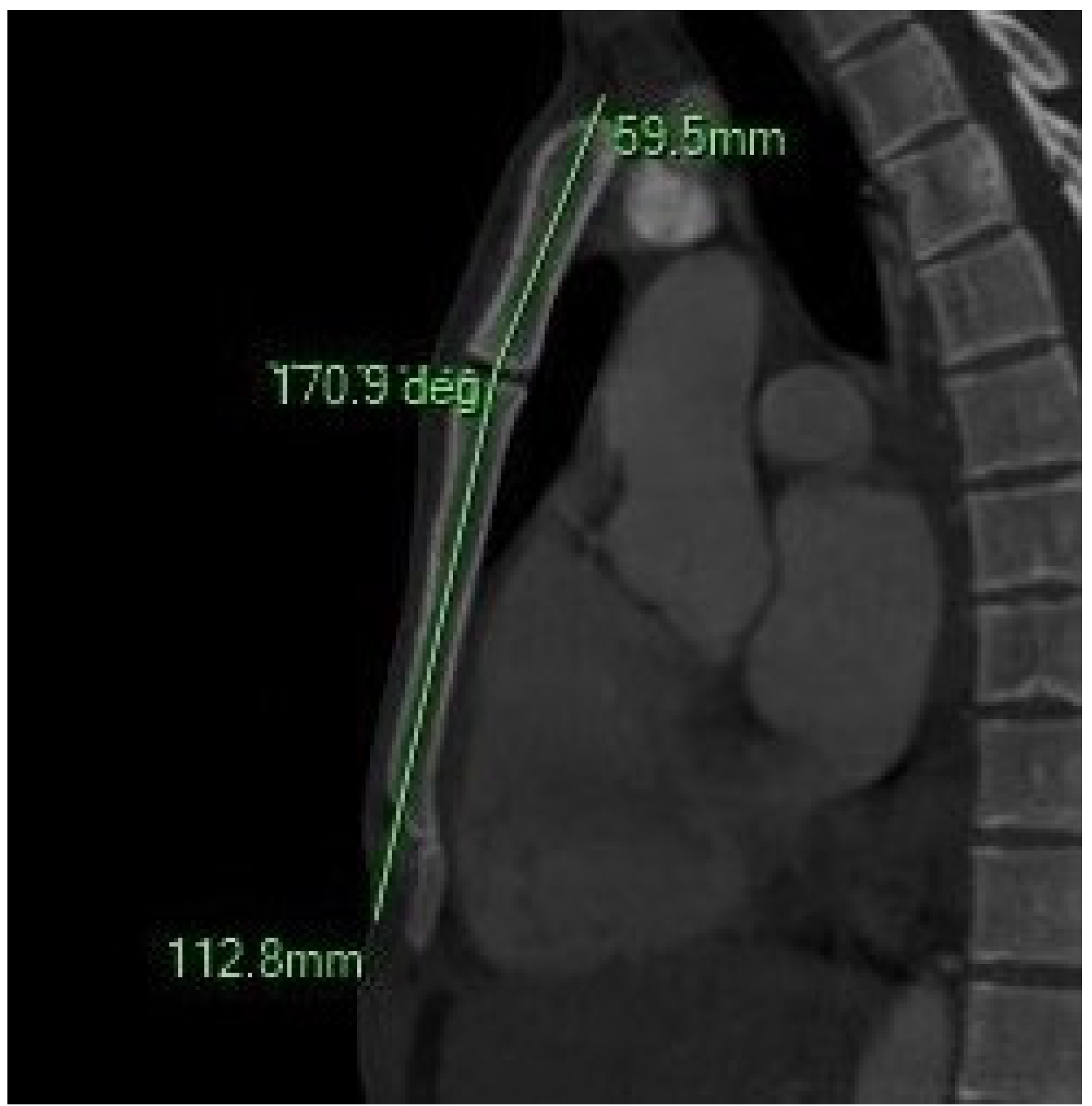
2.4. Sternum Measurements and Morphological Variants
2.4.1. Manubrium (MB) Measurements
- -
- MB length (MBL): Longest linear distance from the midpoint of the jugular notch (JN) to the MBSJ.
- -
- MB width (MBW): Transverse distance between the midpoints of the first costal notches on the right and left.
- -
- MB maximum Thickness (MBTmax): Maximum anteroposterior thickness at the central point of the clavicular notch, measured perpendicular to the central longitudinal axis.
- -
- MB minimum Thickness (MBTmin): Minimum anteroposterior thickness at the midportion of the MB along the central longitudinal line.
2.4.2. Sternum Body (SB) Measurements
- -
- SB Length (SBL): Longest linear distance from the MBSJ to the SXJ.
- -
- SB Width (SBW): Transverse distances between right and left costal notches at the 2nd intercostal space, 3rd, and 4th intercostal spaces (SBWa, SBWb, and SBWc).
- -
- SB Thickness (SBT): Measured at the junctions of the 2nd–3rd and 4th–5th SBr, representing the anteroposterior depth.
2.4.3. Xiphoid Process (XP) Measurements
- -
- XP Length (XPL): Linear distance from the SXJ to the distal tip of the XP.
- -
- XP Thickness (XPT): Maximum thickness measured between the SXJ and the XP’s distal endpoint.
2.4.4. Combined and Index-Based Parameters
- -
- Sternum Total Length (SL): Sum of the manubrium and body lengths: SL = MBL + SBL.
- -
- Sternal Angle (SA): Formed between the following:
- A line parallel to the body and intersecting the midpoint of the JN.
- A second line parallel to the body and intersecting its midpoint.
2.4.5. Indices
- -
- Sternal Index (SI): (MBL/SBL) × 100 Reflects the proportion of manubrium length to sternum body length.
- -
- MB Index (MBI): (MBW/MBL) × 100 Reflects the transverse-to-longitudinal ratio of the manubrium.
- -
- SB Index (SBI): (SBWa/SBWc) × 100. Assesses the tapering pattern of the sternum body width.
- -
- SSA (mm2): The estimated surface area of the sternum is calculated as ((MBL + SBL) × (MBW + SBWa + SBWc)/3)
2.5. Statistical Analysis
3. Results
3.1. Descriptive Morphometry and Statistical Significance
3.2. Sternal Morphological Variants
4. Discussion
4.1. Morphometric Details of the Sternum and Sex Determination Among Studies
- -
- Ashley’s “149 rule” for Europeans [28].
- -
- Jit’s “136 rule” for North Indians [3].
- -
- Dahiphale’s “129 rule” for the Marathwada region [32].
- -
- Hunnargi’s “131 rule” for West India [2].
- -
- Atesoglu’s “144 rule” for South-Eastern Anatolia [29]. However, absolute length-based thresholds may be unreliable across or even within populations due to secular trends and age-related variation in sternal growth [28,40]. Thus, morphometric values must be interpreted in a population-specific context. Based on our findings, a “143 mm rule” could be proposed for the Greek population, wherein an SL above 143 mm suggests male classification. This aligns with population-specific rules previously suggested by Ashley, Jit, and others, and could assist rapid field estimation where only sternal measurements are available. Our study confirms that the mean MBL and SBL in the Greek population align well with previous findings:
- -
- -
- -
4.2. Sternum Morphological Variants
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Akin, K.; Kosehan, D.; Topcu, A.; Koktener, A. Anatomic Evaluation of the Xiphoid Process with 64-Row Multidetector Computed Tomography. Skelet. Radiol. 2011, 40, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Hunnargi, S.A.; Menezes, R.G.; Kanchan, T.; Lobo, S.W.; Binu, V.S.; Uysal, S.; Kumar, H.R.S.; Baral, P.; Herekar, N.G.; Garg, R.K. Sexual Dimorphism of the Human Sternum in a Maharashtrian Population of India: A Morphometric Analysis. Leg. Med. 2008, 10, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Jit, I.; Jhingan, V.; Kulkarni, M. Sexing the Human Sternum. Am. J. Phys. Anthropol. 1980, 53, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Pathak, R.K.; Singh, D. Morphometric Sex Determination from Various Sternal Widths of Northwest Indian Sternums Collected from Autopsy Cadavers: A Comparison of Sexing Methods. Egypt. J. Forensic Sci. 2012, 2, 18–28. [Google Scholar] [CrossRef]
- Singh, J.; Pathak, R.K. Morphometric Sexual Dimorphism of Human Sternum in a North Indian Autopsy Sample: Sexing Efficacy of Different Statistical Techniques and a Comparison with Other Sexing Methods. Forensic Sci. Int. 2013, 228, 174.e1–174.e10. [Google Scholar] [CrossRef]
- Bongiovanni, R.; Spradley, M.K. Estimating Sex of the Human Skeleton Based on Metrics of the Sternum. Forensic Sci. Int. 2012, 219, 290.e1–290.e7. [Google Scholar] [CrossRef]
- Chandrakanth, H.V.; Kanchan, T.; Krishan, K.; Arun, M.; Pramod Kumar, G.N. Estimation of Age from Human Sternum: An Autopsy Study on a Sample from South India. Int. J. Leg. Med. 2012, 126, 863–868. [Google Scholar] [CrossRef]
- Uysal Ramadan, S.; Türkmen, N.; Dolgun, N.A.; Gökharman, D.; Menezes, R.G.; Kacar, M.; Koşar, U. Sex Determination from Measurements of the Sternum and Fourth Rib Using Multislice Computed Tomography of the Chest. Forensic Sci. Int. 2010, 197, 120.e1–120.e5. [Google Scholar] [CrossRef]
- Vatzia, K.; Fanariotis, M.; Makridis, K.G.; Vlychou, M.; Fezoulidis, I.V.; Vassiou, K. Frequency of Sternal Variations and Anomalies in Living Individuals Evaluated by MDCT. Eur. J. Radiol. 2021, 142, 109828. [Google Scholar] [CrossRef]
- Changani, M.; Javia, M.; Varma, K. Determination of Sex from Various Measurements of Human Sternum and Manubrium in Gujarat Population. J. Res. Med. Dent. Sci. 2014, 2, 59. [Google Scholar] [CrossRef]
- Ekizoglu, O.; Hocaoglu, E.; Inci, E.; Bilgili, M.G.; Solmaz, D.; Erdil, I.; Can, I.O. Sex Estimation From Sternal Measurements Using Multidetector Computed Tomography. Medicine 2014, 93, e240. [Google Scholar] [CrossRef] [PubMed]
- Sahin, M.; Sahin, N.E.; Oner, S.; Toy, S.; Oner, Z. Evaluating Sternum Development and Ossification through Computed Tomography Images: A Comparative Analysis across Age and Sex. Folia Morphol. 2025. Online ahead of print. [Google Scholar] [CrossRef]
- Abdualhadi, E.M.; Hegazy, N.I.; Abdelaal, G.M. Brief Overview of Sex Identification from the Sternum. NeuroQuantology 2022, 20, 12060–12067. [Google Scholar]
- Klales, A. Current State of Sex Estimation in Forensic Anthropology. Forensic Anthropol. 2021, 4, 118–133. [Google Scholar] [CrossRef]
- Bacci, N.; Nchabeleng, E.K.; Billings, B.K. Forensic Age-at-Death Estimation from the Sternum in a Black South African Population. Forensic Sci. Int. 2018, 282, 233.e1–233.e7. [Google Scholar] [CrossRef]
- Brooks, S.; Suchey, J.M. Skeletal Age Determination Based on the Os Pubis: A Comparison of the Acsádi-Nemeskéri and Suchey-Brooks Methods. Hum. Evol. 1990, 5, 227–238. [Google Scholar] [CrossRef]
- Lovejoy, C.O.; Meindl, R.S.; Pryzbeck, T.R.; Mensforth, R.P. Chronological Metamorphosis of the Auricular Surface of the Ilium: A New Method for the Determination of Adult Skeletal Age at Death. Am. J. Phys. Anthropol. 1985, 68, 15–28. [Google Scholar] [CrossRef]
- Mulhern, D.M.; Jones, E.B. Test of Revised Method of Age Estimation from the Auricular Surface of the Ilium. Am. J. Phys. Anthropol. 2005, 126, 61–65. [Google Scholar] [CrossRef]
- Passalacqua, N.V. Forensic Age-at-Death Estimation from the Human Sacrum*. J. Forensic Sci. 2009, 54, 255–262. [Google Scholar] [CrossRef]
- Triantafyllou, G.; Botis, G.G.; Piagkou, M.; Papanastasiou, K.; Tsakotos, G.; Paschopoulos, I.; Matsopoulos, G.K.; Papadodima, S. Sex Estimation Through Orbital Measurements: A Machine Learning Approach for Forensic Science. Diagnostics 2024, 14, 2773. [Google Scholar] [CrossRef]
- Cho, H.-J.; Hong, E.; Kwak, D.-S. The Sex Difference of the Volume and Surface Area of the Human Axial Skeleton. Anthropol. Anz. 2022, 79, 331–339. [Google Scholar] [CrossRef]
- Fernández, E.D.; Sáez, A.S.; Moro, J.I. Anthropological Determination of Sex by Studying the Sternum. Rev. Esc. DeMed Leg. 2007, 6, 27–42. [Google Scholar]
- Franklin, D.; Flavel, A.; Kuliukas, A.; Cardini, A.; Marks, M.K.; Oxnard, C.; O’Higgins, P. Estimation of Sex from Sternal Measurements in a Western Australian Population. Forensic Sci. Int. 2012, 217, 230.e1–230.e5. [Google Scholar] [CrossRef] [PubMed]
- Macaluso, P.J.; Lucena, J. Estimation of Sex from Sternal Dimensions Derived from Chest Plate Radiographs in Contemporary Spaniards. Int. J. Leg. Med. 2014, 128, 389–395. [Google Scholar] [CrossRef]
- Torimitsu, S.; Makino, Y.; Saitoh, H.; Sakuma, A.; Ishii, N.; Inokuchi, G.; Motomura, A.; Chiba, F.; Hoshioka, Y.; Iwase, H. Estimation of Sex in Japanese Cadavers Based on Sternal Measurements Using Multidetector Computed Tomography. Leg. Med. 2015, 17, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Adhvaryu, A.V.; Adhvaryu, M.A.; Rathod, S.P.; Chauhan, P.R.; Joshi, H.G. A Study of Sexual Dimorphism in Human Sterna. Int. J. Med. Res. Health Sci. 2013, 2, 577. [Google Scholar] [CrossRef]
- Ahmed, A.A.; Alshammari, F.O.; Alrafiaah, A.S.; Almohaisani, A.A.; Al-Mohrej, O.A.; Alkubaidan, F.O. Estimation of Sex in a Contemporary Saudi Population Based on Sternal Measurements Using Multidetector Computed Tomography. HOMO 2017, 68, 411–421. [Google Scholar] [CrossRef]
- Ashley, G.T. A Comparison of Human and Anthropoid Mesosterna. Am. J. Phys. Anthropol. 1956, 14, 449–465. [Google Scholar] [CrossRef] [PubMed]
- Ateşoğlu, S.; Deniz, M.; Uslu, A.İ. Evaluation of the Morphological Characteristic and Sex Differences of Sternum by Multi-Detector Computed Tomography. Folia Morphol (Warsz) 2018, 77, 489–497. [Google Scholar] [CrossRef]
- Bayarogullari, H.; Yengil, E.; Davran, R.; Aglagul, E.; Karazincir, S.; Balci, A. Evaluation of Postnatal Development and Variations of Sternum Using Multi-Detector Computed Tomography. Diagn. Interv. Radiol. 2013, 20, 82–89. [Google Scholar] [CrossRef]
- Chandrakanth, H.V.; Kanchan, T.; Krishan, K. Osteometric Analysis for Sexing of Modern Sternum—An Autopsy Study from South India. Leg. Med. 2014, 16, 350–356. [Google Scholar] [CrossRef]
- Dahiphale VP, B.B.K.S. Sexing the Human Sternum in Marathwada Region. J. Anat. Soc. India 2002, 51, 162–167. [Google Scholar]
- Donlon, D.A. The Value of Infracranial Nonmetric Variation in Studies of ModernHomo Sapiens: An Australian Focus. Am. J. Phys. Anthropol. 2000, 113, 349–368. [Google Scholar] [CrossRef]
- Dwight, T. The Sternum as an Index of Sex and Age. J. Anat. Physiol. 1881, 15, 327–330. [Google Scholar] [PubMed]
- Dwight, T. Sternum as an Index of Sex, Height, and Age. J. Anat. Physiol. 1890, 24, 527–535. [Google Scholar]
- García-Parra, P.; Pérez Fernández, Á.; Djorojevic, M.; Botella, M.; Alemán, I. Sexual Dimorphism of Human Sternum in a Contemporary Spanish Population. Forensic Sci. Int. 2014, 244, 313.e1–313.e9. [Google Scholar] [CrossRef] [PubMed]
- Hyrtl, J. Handbuch Der Topographischen Anatomic Percentage. Vienna Wilhelm. Braumuller 1893, 1, 348. [Google Scholar]
- Khartade, H.K.; Shrivastava, S.; Shedge, R.; Meshram, V.P.; Garg, S.P. Anthropometry of the Sternum: An Autopsy-Based Study for Sex Determination. Med.-Leg. J. 2024, 92, 27–33. [Google Scholar] [CrossRef]
- Macaluso, P.J. The Efficacy of Sternal Measurements for Sex Estimation in South African Blacks. Forensic Sci. Int. 2010, 202, 111.e1–111.e7. [Google Scholar] [CrossRef]
- McCormick, W.F.; Stewart, J.H.; Langford, L.A. Sex Determination from Chest Plate Roentgenograms. Am. J. Phys. Anthropol. 1985, 68, 173–195. [Google Scholar] [CrossRef]
- Osunwoke, E.A.; Gwunireama, I.U.; Orish, C.N.; Ordu, K.S.; Ebowe, I. A Study of Sexual Dimorphism of the Human Sternum in the Southern Nigerian Population. J. Appl. Biosci. 2010, 26, 1636–1639. [Google Scholar]
- Rojas, C.V.; Olivares, J.I.; Tutor, P.M.; García, A.M.; Sánchez, M.B. Sternal Human Variability and Population Affinity: Frequency of Discrete Traits and Their Relationship with Sex and Age. Anat. Rec. 2022, 305, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Selthofer, R.; Nikolić, V.; Mrcela, T.; Radić, R.; Leksan, I.; Rudez, I.; Selthofer, K. Morphometric Analysis of the Sternum. Coll. Antropol. 2006, 30, 43–47. [Google Scholar]
- Torwalt, C.R.M.M.; Hoppa, R.D. A Test of Sex Determination from Measurements of Chest Radiographs. J. Forensic Sci. 2005, 50, 785–790. [Google Scholar] [CrossRef]
- Verna, E.; Piercecchi-Marti, M.; Chaumoitre, K.; Bartoli, C.; Leonetti, G.; Adalian, P. Discrete Traits of the Sternum and Ribs: A Useful Contribution to Identification in Forensic Anthropology and Medicine. J. Forensic Sci. 2013, 58, 571–577. [Google Scholar] [CrossRef]
- Batool, S.N.; Yang, J.; Gilanie, G.; Latif, A.; Yasin, S.; Ikram, A.; Por, L.Y. Forensic Radiology: A Robust Approach to Biological Profile Estimation from Bone Image Analysis Using Deep Learning. Biomed. Signal Process. Control 2025, 105, 107661. [Google Scholar] [CrossRef]
- Elmansy, A.; Ammar, A.M.; Elhawary, A.E. Sex identification using sternal measurements by multi-slice computed tomography in a sample of the egyptian population. Egypt. J. Forensic Sci. Appl. Toxicol. 2024, 24, 1–15. [Google Scholar] [CrossRef]
- Galante, N.; Cotroneo, R.; Furci, D.; Lodetti, G.; Casali, M.B. Applications of Artificial Intelligence in Forensic Sciences: Current Potential Benefits, Limitations and Perspectives. Int. J. Leg. Med. 2023, 137, 445–458. [Google Scholar] [CrossRef]
- Zhang, M. The Application of Forensic Imaging to Sex Estimation: Focus on Skull and Pelvic Structures. Perspect. Leg. Forensic Sci. 2024, 1, 10005. [Google Scholar] [CrossRef]
- Wang, X.; Liu, G.; Wu, Q.; Zheng, Y.; Song, F.; Li, Y. Sex Estimation Techniques Based on Skulls in Forensic Anthropology: A Scoping Review. PLoS ONE 2024, 19, e0311762. [Google Scholar] [CrossRef]
- Braun, S.; Schwendener, N.; Kanz, F.; Lösch, S.; Milella, M. What We See Is What We Touch? Sex Estimation on the Pelvis in Virtual Anthropology. Int. J. Leg. Med. 2023, 137, 1839–1852. [Google Scholar] [CrossRef]
- Ghorbanlou, M.; Moradi, F.; Asgari, H.R. Morphometric Study of Sternum by Computed Tomography in an Iranian Population: A Method to Discriminate between Male and Female. Forensic Imaging 2022, 28, 200501. [Google Scholar] [CrossRef]
- Kalbouneh, H.; Mubarak, N.; Daradkeh, S.; Ashour, O.; Alkhatib, A.M.; Suboh, L.; Nofal, A.; Mahafzah, W.; Alsalem, M. Estimation of Sex Based on Metrics of the Sternum in a Contemporary Jordanian Population. Medicine 2021, 100, e28169. [Google Scholar] [CrossRef] [PubMed]
- Poodendaen, C.; Klaikran, S.; Maihong, A.; Choompoo, N.; Duangchit, S.; Boonthai, W.; Tangsrisakda, N.; Arun, S.; Chaimontri, C.; Iamsaard, S. Biological Sex and Stature Estimations from Dry Sternum: A Population-Specific Study in Northeastern Thais. Forensic Sci. Int. Rep. 2025, 11, 100419. [Google Scholar] [CrossRef]
- Boonthai, W.; Kwanyou, A.; Puntawangkoon, S.; Waehama, R.; Poodendaen, C.; Arun, S.; Chaiyamoon, A.; Iamsaard, S.; Duangchit, S. Sexual Dimorphism and Population-Specific Sex Estimation Equations Using Morphometric Analysis of Dry Lumbar Vertebrae in a Northeastern Thais. Int. J. Morphol. 2024, 42, 1611–1617. [Google Scholar] [CrossRef]
- Vaswani, V.; Caenazzo, L.; Congram, D. Corpse Identification in Mass Disasters and Other Violence: The Ethical Challenges of a Humanitarian Approach. Forensic Sci. Res. 2024, 9, owad048. [Google Scholar] [CrossRef]
- Sravan, J.S.; Arora, A.; Yadav, J.; Vidua, R.K.; Gayathri, B.H. Determination of Sex from Morphometry of Sternum Using Multidetector Computed Tomography in Central Indian Population. Int. J. Appl. Basic. Med. Res. 2025, 15, 32–37. [Google Scholar] [CrossRef]
- Banyeh, M.; Abdulai, A.-R.; Annan, E.K.; Mensah, E.K.; Nkansah, C.; Nathan, J.A.; Twum, M.B.; Achumboro, P.A. Assessing the Reliability and Accuracy of Sex Estimation Models Utilizing Sternal Morphometry Derived from Computed Tomography in the Ghanaian Population. Forensic Sci. Int. Rep. 2024, 9, 100368. [Google Scholar] [CrossRef]
- Pasieka, P.; Pasieka, P.M.; Komosa, A.; Barnowska, A.; Pękala, J.; Malinowski, K.; Tomaszewski, K. Prevalence and Morphometry of Sternal and Xiphoid Foramen: A Meta-Analysis on 16,666 Subjects. Surg. Radiol. Anat. 2023, 45, 623–635. [Google Scholar] [CrossRef]
- Karagulle, M.; Candan, B.; Torun, E.; Hizay, A.; Keles-Celik, N. In Vivo Morphology of the Sternum with Emphasis on the Frequency of Sternal Foramen. Bratisl. Med. J. 2025, 126, 872–880. [Google Scholar] [CrossRef]
- Toy, S.; Secgin, Y.; Oner, Z.; Turan, M.K.; Oner, S.; Senol, D. A Study on Sex Estimation by Using Machine Learning Algorithms with Parameters Obtained from Computerized Tomography Images of the Cranium. Sci. Rep. 2022, 12, 4278. [Google Scholar] [CrossRef]
- Palamenghi, L.; Gibelli, D.; Panzeri, M.; Zago, M.; Cattaneo, C. Skull variants in forensic anthropology: Assessing their frequency and forensic value in a modern identified skeletal collection. Int. J. Legal. Med. 2025, 139, 875–885. [Google Scholar] [CrossRef]
- Campobasso, C.P.; Dell’Erba, A.S.; Belviso, M.; Di Vella, G. Craniofacial identification by comparison of antemortem and postmortem radiographs: Two case reports dealing with burnt bodies. Am. J. Forensic Med. Pathol. 2007, 28, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Mello-Gentil, T.; Souza-Mello, V. Contributions of Anatomy to Forensic Sex Estimation: Focus on Head and Neck Bones. Forensic Sci. Res. 2022, 7, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, G.D.; Asirdizer, M.; Kartal, E.; Keskin, S.; Mutlu, I.; Goya, C. Sex Estimation from the Hyoid Bone Measurements in an Adult Eastern Turkish Population Using 3D CT Images, Discriminant Function Analysis, Support Vector Machines, and Artificial Neural Networks☆. Leg. Med. 2024, 67, 102383. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Sex | N | Mean | Median | SD | Range | Min | Max | SE | t-Statistic | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | F | 50 | 58.10 | 63.00 | 17.70 | 61 | 24 | 85 | 2.50 | −1.03 | 0.304 |
| M | 50 | 61.38 | 60.50 | 13.78 | 60 | 27 | 87 | 1.95 | |||
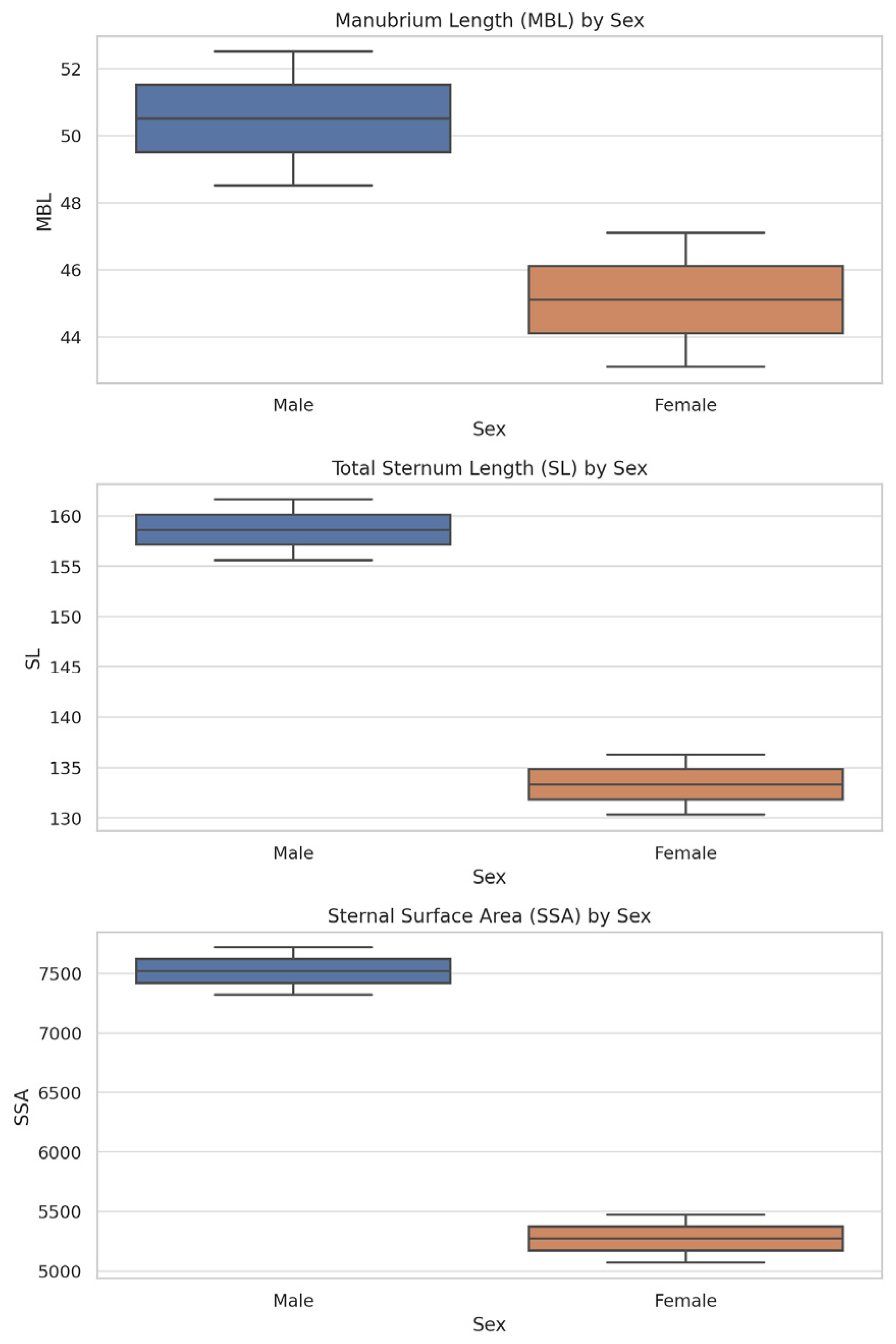
| MB length (ΜΒL) | F | 50 | 45.13 | 44.90 | 4.45 | 21.30 | 36.20 | 57.50 | 0.63 | −5.82 | <0.001 |
| M | 50 | 50.50 | 50.75 | 4.79 | 17.70 | 41.30 | 59.00 | 0.68 | |||
| MB width (MΒW) | F | 50 | 62.65 | 62.30 | 8.91 | 38.00 | 46.80 | 84.80 | 1.26 | −7.10 | <0.001 |
| M | 50 | 78.01 | 77.60 | 12.45 | 67.50 | 51.20 | 118.70 | 1.76 | |||
| SB Length (SBL) | F | 50 | 88.18 | 87.80 | 10.05 | 52.80 | 61.40 | 114.20 | 1.42 | −9.58 | <0.001 |
| M | 50 | 108.13 | 107.45 | 10.75 | 43.40 | 89.60 | 133.00 | 1.52 | |||
| SB width at the 2nd intercostal space (SBWa) | F | 50 | 25.10 | 24.90 | 3.14 | 16.30 | 16.70 | 33.00 | 0.44 | −5.01 | <0.001 |
| M | 50 | 28.27 | 27.35 | 3.20 | 15.40 | 20.50 | 35.90 | 0.45 | |||
| SB width at the 3rd intercostal space (SBWb) | F | 50 | 27.52 | 27.30 | 3.78 | 21.80 | 21.30 | 43.10 | 0.53 | −4.72 | <0.001 |
| M | 50 | 31.27 | 31.00 | 4.16 | 15.80 | 23.70 | 39.50 | 0.59 | |||
| SB width at the 4th intercostal space (SBWc) | F | 50 | 30.91 | 30.05 | 5.24 | 26.10 | 24.40 | 50.50 | 0.74 | −4.34 | <0.001 |
| M | 50 | 35.48 | 35.65 | 5.29 | 23.20 | 24.60 | 47.80 | 0.75 | |||
| MB minimum thickness (MΒTmin) | F | 50 | 8.62 | 8.55 | 1.11 | 5.40 | 6.30 | 11.70 | 0.16 | −4.19 | <0.001 |
| M | 50 | 9.61 | 9.90 | 1.26 | 6.20 | 5.90 | 12.10 | 0.18 | |||
| MB maximum thickness (MΒTmax) | F | 50 | 13.49 | 13.45 | 1.58 | 8.40 | 10.70 | 19.10 | 0.22 | −4.78 | <0.001 |
| M | 50 | 15.07 | 14.90 | 1.70 | 7.20 | 11.40 | 18.60 | 0.24 | |||
| SB thickness (SBT) at the SBr 2–3 | F | 50 | 9.38 | 9.40 | 1.12 | 5.60 | 6.90 | 12.50 | 0.16 | −4.28 | <0.001 |
| M | 50 | 10.33 | 10.50 | 1.11 | 4.40 | 8.20 | 12.60 | 0.16 | |||
| Sternum body thickness (SBT) at the SBr 4–5 | F | 50 | 8.93 | 8.90 | 1.15 | 5.20 | 6.10 | 11.30 | 0.16 | −3.07 | 0.003 |
| M | 50 | 9.68 | 9.70 | 1.27 | 5.70 | 7.10 | 12.80 | 0.18 | |||
| SL (MBL + SBL) | F | 50 | 133.31 | 132.80 | 9.85 | 47.70 | 112.70 | 160.40 | 1.39 | −12.23 | <0.001 |
| M | 50 | 158.63 | 158.55 | 10.84 | 44.30 | 139.50 | 183.80 | 1.53 | |||
| XP length (XPL) | F | 50 | 35.98 | 34.95 | 13.53 | 51.80 | 12.20 | 64.00 | 1.91 | −3.61 | <0.001 |
| M | 50 | 45.50 | 46.90 | 12.89 | 51.60 | 15.40 | 67.00 | 1.82 | |||
| XP thickness (XPT) | F | 50 | 7.02 | 7.15 | 1.65 | 7.10 | 3.70 | 10.80 | 0.23 | −3.00 | 0.003 |
| M | 50 | 8.15 | 8.05 | 2.09 | 10.10 | 4.00 | 14.10 | 0.30 | |||
| Sternal Angle (SA) | F | 50 | 164.04 | 164.50 | 7.36 | 40.00 | 140.00 | 180.00 | 1.04 | 0.81 | 0.420 |
| M | 50 | 162.83 | 162.45 | 7.60 | 28.30 | 149.20 | 177.50 | 1.08 | |||
| Sternal Index (SI) (MBL/SBL) × 100 | F | 50 | 52.02 | 51.35 | 9.28 | 47.40 | 36.20 | 83.60 | 1.31 | 2.88 | 0.005 |
| M | 50 | 47.25 | 47.00 | 7.11 | 28.60 | 33.90 | 62.50 | 1.01 | |||
| MB Index (MBI) (MBW/MBL) × 100 | F | 50 | 139.78 | 138.75 | 21.82 | 114.60 | 96.30 | 210.90 | 3.09 | −3.07 | 0.003 |
| M | 50 | 156.17 | 154.45 | 30.80 | 153.80 | 99.20 | 253.00 | 4.36 | |||
| SB index (SBI) (SBWa/SBWc) × 100 | F | 50 | 82.59 | 82.55 | 12.94 | 52.10 | 56.20 | 108.30 | 1.83 | 0.83 | 0.411 |
| M | 50 | 80.68 | 79.70 | 10.09 | 44.50 | 64.00 | 108.50 | 1.43 | |||
| SSA (MB + SB) × (MBW + SBWa + SBWc)/3 | F | 50 | 5271.52 | 5194.10 | 657.65 | 3050.50 | 4082.00 | 7132.50 | 93.01 | −12.12 | <0.001 |
| M | 50 | 7517.09 | 7354.35 | 1133.62 | 5221.30 | 5721.60 | 10,942.90 | 160.32 |
| Predictor | Estimate | SE | Z | p | Odds Ratio |
|---|---|---|---|---|---|
| Intercept | −43.06 | 9.49 | −4.45 | <0.001 | 2 × 10−19 |
| MB length (mm) | 0.39 | 0.11 | 3.67 | <0.001 | 1.48 |
| SB length (mm) | 0.25 | 0.06 | 4.39 | <0.001 | 1.29 |
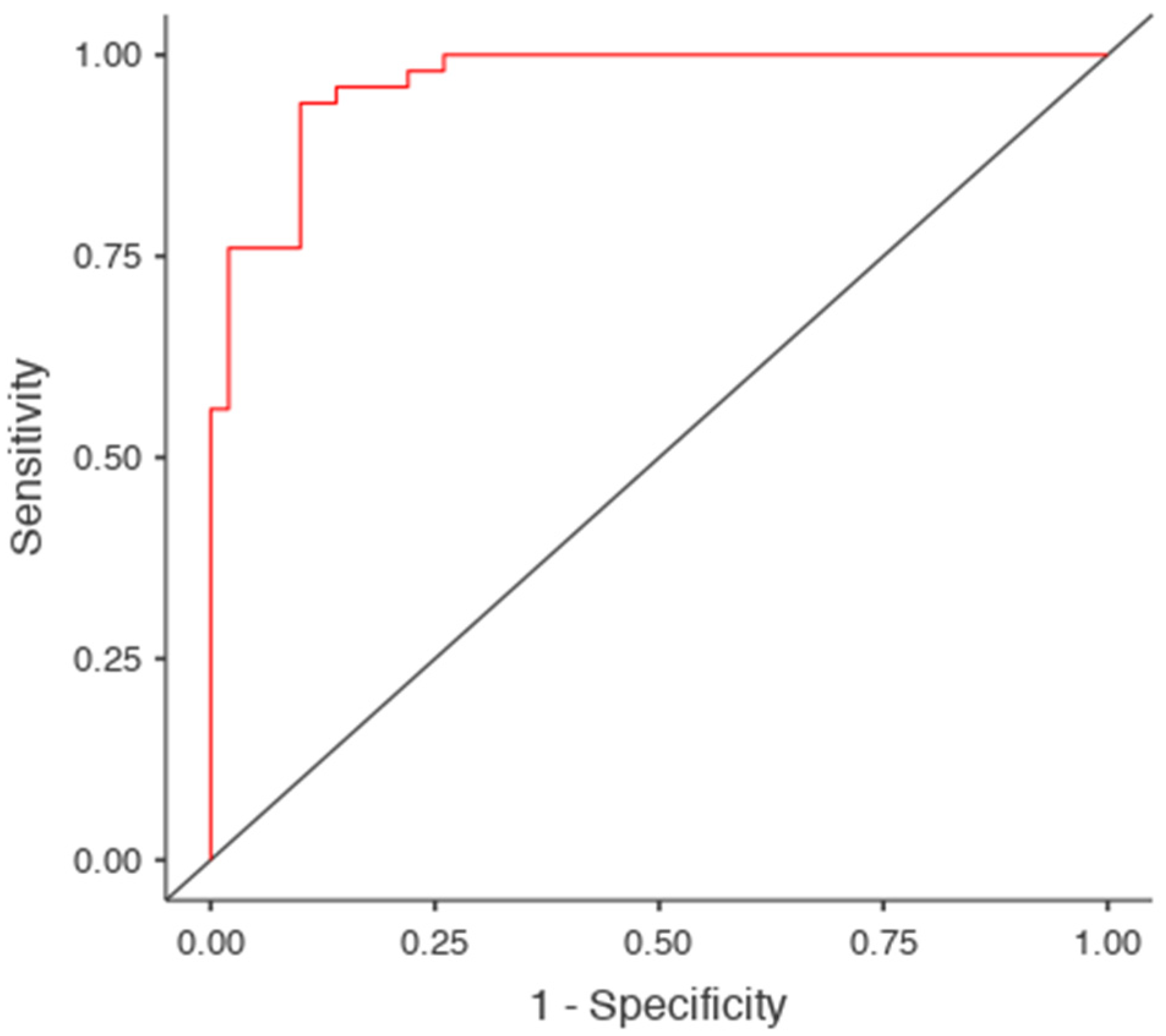
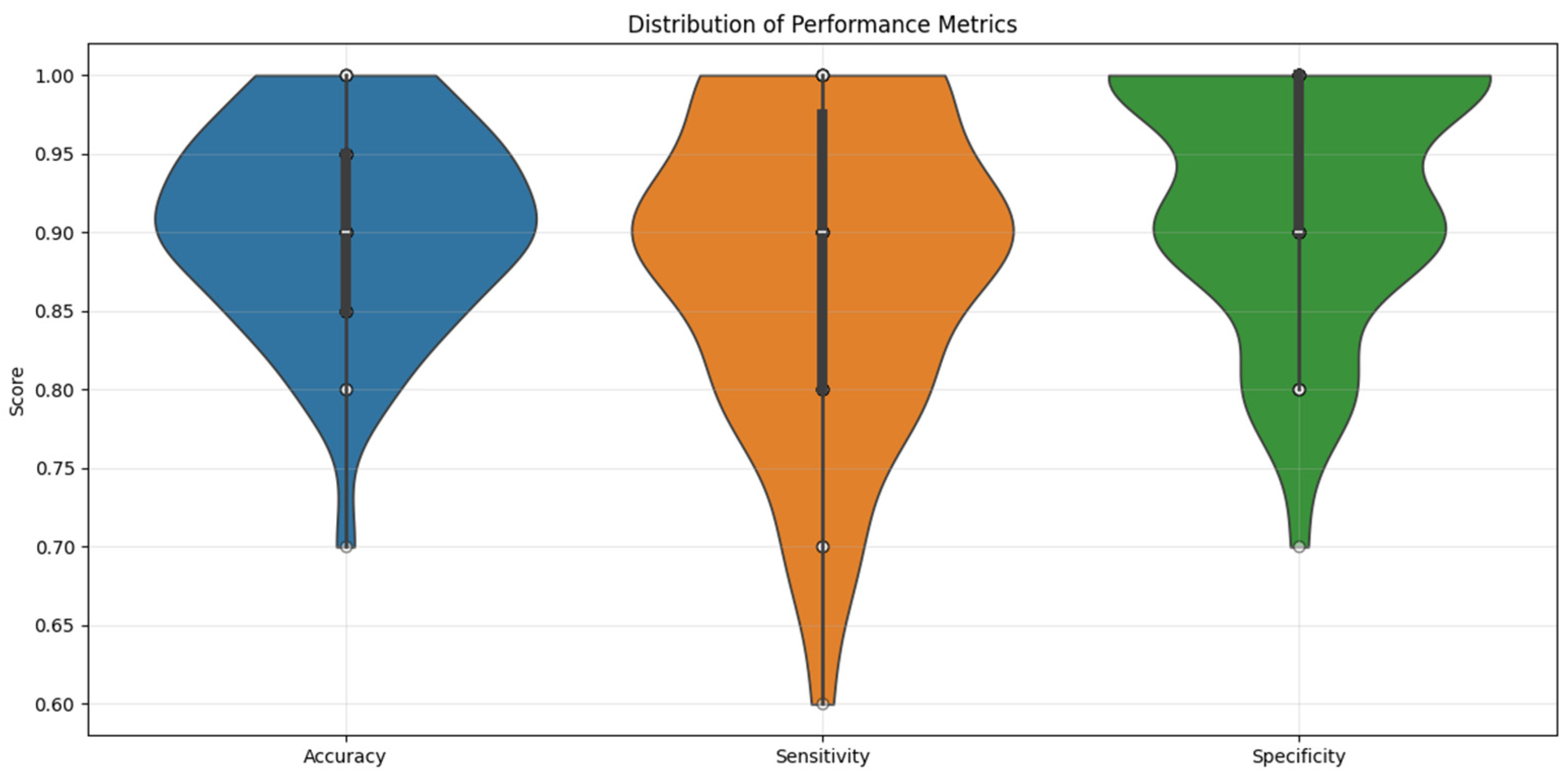
| Predictive measures | Accuracy: 0.91 | Specificity: 0.90 | Sensitivity: 0.92 | AUC: 0.97 |
| Metric | Threshold (mm) | Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Youden’s Index | AUC |
|---|---|---|---|---|---|---|---|
| MB length (MBL) | 47.3 | 76 | 74 | 75 | 76 | 0.5 | 0.795 |
| MB width (MBW) | 70.9 | 78 | 86 | 85 | 80 | 0.64 | 0.847 |
| SB length (SBL) | 94.4 | 92 | 78 | 81 | 91 | 0.7 | 0.918 |
| SB width at the 2nd intercostal space (SBWa) | 25.6 | 86 | 64 | 70 | 82 | 0.5 | 0.772 |
| SB width at the 3rd intercostal space (SBWb) | 29.8 | 62 | 78 | 74 | 67 | 0.4 | 0.761 |
| SB width at the 4th intercostal space (SBWc) | 31.5 | 78 | 70 | 72 | 76 | 0.48 | 0.764 |
| MB minimum thickness (MBTmin) | 9.6 | 64 | 82 | 78 | 69 | 0.46 | 0.737 |
| MB maximum thickness (MBTmax) | 13.9 | 80 | 66 | 70 | 77 | 0.46 | 0.771 |
| SB thickness of sternebrae 2–3 | 10.1 | 64 | 76 | 73 | 68 | 0.4 | 0.792 |
| SB thickness of sternebrae 4–5 | 9.1 | 70 | 58 | 63 | 66 | 0.28 | 0.662 |
| SL (MBL + SBL) | 143.2 | 96 | 86 | 87 | 96 | 0.82 | 0.965 |
| XP length (XPL) | 33.1 | 84 | 50 | 63 | 76 | 0.34 | 0.687 |
| XP thickness (XPT) | 7.7 | 58 | 70 | 66 | 63 | 0.28 | 0.662 |
| MB Index (MBI) (MBW/MBL) × 100 | 150.9 | 60 | 72 | 68 | 64 | 0.32 | 0.674 |
| SSA (mm2) (MB + SB) × (MBW + SBWa + SBWc)/3 | 6039.5 | 96 | 88 | 89 | 96 | 0.84 | 0.978 |
| Morphological Variant | Number of Cases | Frequency (%) | Male Cases (n = 50) | Female Cases (n = 50) | p-Value |
|---|---|---|---|---|---|
| Double-ended XP | 44 | 44% | 22 | 22 | 1.000 |
| Ligament Calcification | 36 | 36% | 20 | 16 | 0.532 |
| Sternal Foramen (SF) | 30 | 30% | 15 | 15 | 1.000 |
| Sternal Notch | 30 | 30% | 17 | 13 | 0.513 |
| Suprasternal Tubercle | 19 | 19% | 10 | 9 | 1.000 |
| Elongated XP | 14 | 14% | 9 | 5 | 0.388 |
| Sternal Sclerotic Band | 12 | 12% | 7 | 5 | 0.758 |
| Suprasternal Bone | 8 | 8% | 5 | 3 | 0.715 |
| MB Foramen | 6 | 6% | 2 | 4 | 0.678 |
| Sternal Foramen | 5 | 5% | 2 | 3 | 1.000 |
| Pseudoforamen | 5 | 5% | 3 | 2 | 1.000 |
| Triple-ended XP | 3 | 3% | 2 | 1 | 1.000 |
| Manubriosternal Fusion (MBSF) | 3 | 3% | 1 | 2 | 1.000 |
| Sternal Cleft | 1 | 1% | 1 | 0 | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vatzia, K.; Fanariotis, M.; Bugajski, M.; Fezoulidis, I.V.; Piagkou, M.; Vlychou, M.; Triantafyllou, G.; Vezakis, I.; Botis, G.; Papadodima, S.; et al. Assessing Sternal Dimensions for Sex Classification: Insights from a Greek Computed Tomography-Based Study. Diagnostics 2025, 15, 1649. https://doi.org/10.3390/diagnostics15131649
Vatzia K, Fanariotis M, Bugajski M, Fezoulidis IV, Piagkou M, Vlychou M, Triantafyllou G, Vezakis I, Botis G, Papadodima S, et al. Assessing Sternal Dimensions for Sex Classification: Insights from a Greek Computed Tomography-Based Study. Diagnostics. 2025; 15(13):1649. https://doi.org/10.3390/diagnostics15131649
Chicago/Turabian StyleVatzia, Konstantina, Michail Fanariotis, Maciej Bugajski, Ioannis V. Fezoulidis, Maria Piagkou, Marianna Vlychou, George Triantafyllou, Ioannis Vezakis, George Botis, Stavroula Papadodima, and et al. 2025. "Assessing Sternal Dimensions for Sex Classification: Insights from a Greek Computed Tomography-Based Study" Diagnostics 15, no. 13: 1649. https://doi.org/10.3390/diagnostics15131649
APA StyleVatzia, K., Fanariotis, M., Bugajski, M., Fezoulidis, I. V., Piagkou, M., Vlychou, M., Triantafyllou, G., Vezakis, I., Botis, G., Papadodima, S., Matsopoulos, G., & Vassiou, K. (2025). Assessing Sternal Dimensions for Sex Classification: Insights from a Greek Computed Tomography-Based Study. Diagnostics, 15(13), 1649. https://doi.org/10.3390/diagnostics15131649