

Exploring Chromogranin A (CgA) as a Diagnostic Marker in Hypothermia-Related Deaths: Two Case Studies and a Literature Review


Abstract
1. Introduction
2. Case Presentation
2.1. Case 1
2.1.1. Autopsy
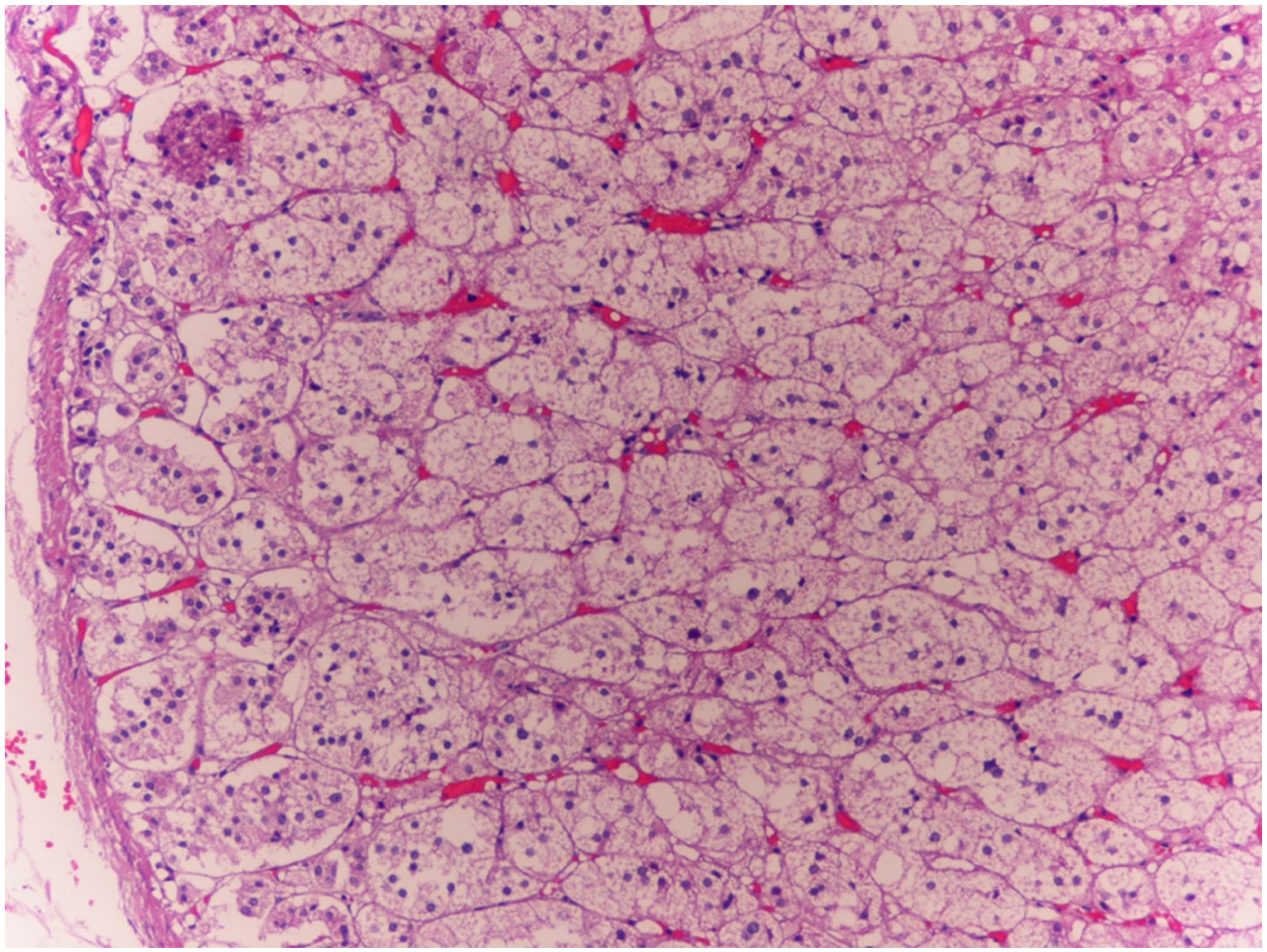
2.1.2. Histopathology
2.2. Case 2
2.2.1. Autopsy
2.2.2. Histopathology
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CgA | Chromogranin A |
| HPA | Hypothalamic–pituitary–adrenal |
| IHC | Immunohistochemistry |
| WSs | Wischnewsky spots |
References
- Turk, E.E. Hypothermia. Forensic Sci. Med. Pathol. 2010, 6, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Falat, C. Environmental Hypothermia. Emerg. Med. Clin. N. Am. 2024, 42, 493–511. [Google Scholar] [CrossRef] [PubMed]
- Duguid, H.; Simpson, R.G.; Stowers, J.M. Accidental hypothermia. Lancet 1961, 2, 1213–1219. [Google Scholar] [CrossRef] [PubMed]
- Mair, P.; Kornberger, E.; Furtwaengler, W.; Balogh, D.; Antretter, H. Prognostic markers in patients with severe accidental hypothermia and cardiocirculatory arrest. Resuscitation 1994, 27, 47–54. [Google Scholar] [CrossRef]
- Vretenar, D.F.; Urschel, J.D.; Parrott, J.C.; Unruh, H.W. Cardiopulmonary bypass resuscitation for accidental hypothermia. Ann. Thorac. Surg. 1994, 58, 895–898. [Google Scholar] [CrossRef]
- Paal, P.; Pasquier, M.; Darocha, T.; Lechner, R.; Kosinski, S.; Wallner, B.; Zafren, K.; Brugger, H. Accidental Hypothermia: 2021 Update. Int. J. Environ. Res. Public. Health 2022, 19, 501. [Google Scholar] [CrossRef]
- Natanti, A.; Mazzanti, R.; Palpacelli, M.; Turchi, C.; Tagliabracci, A.; Pesaresi, M. Death following extreme temperature exposure: Histological, biochemical and immunohistochemical markers. Med. Sci. Law. 2021, 61, 36–41. [Google Scholar] [CrossRef]
- Yoshida, C.; Ishikawa, T.; Michiue, T.; Quan, L.; Maeda, H. Postmortem biochemistry and immunohistochemistry of chromogranin A as a stress marker with special regard to fatal hypothermia and hyperthermia. Int. J. Leg. Med. 2011, 125, 11–20. [Google Scholar] [CrossRef]
- Yoshida, C.; Ishikawa, T.; Michiue, T.; Zhao, D.; Komatsu, A.; Quan, L.; Maeda, H. Immunohistochemical distribution of chromogranin A in medicolegal autopsy materials. Leg. Med. 2009, 11 (Suppl. S1), S231–S233. [Google Scholar] [CrossRef]
- Palmiere, C.; Mangin, P. Postmortem biochemical investigations in hypothermia fatalities. Int. J. Leg. Med. 2013, 127, 267–276. [Google Scholar] [CrossRef]
- Anti-Chromogranin A (LK2H10) Primary Antibody. Available online: https://elabdoc-prod.roche.com/eLD/web/global/en/products/RTD000662 (accessed on 25 June 2025).
- Hendy, G.N.; Bevan, S.; Mattei, M.G.; Mouland, A.J. Chromogranin A. Clin. Investig. Med. 1995, 18, 47–65. [Google Scholar]
- Helle, K.B.; Metz-Boutigue, M.-H.; Cerra, M.C.; Angelone, T. Chromogranins: From discovery to current times. Pflug. Arch.-Eur. J. Physiol. 2018, 470, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Ottesen, A.H.; Christensen, G.; Omland, T.; Røsjø, H. Glycosylated Chromogranin A: Potential Role in the Pathogenesis of Heart Failure. Curr. Heart Fail. Rep. 2017, 14, 478–488. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Rozet, F.; Roubaud, G.; Stanbury, T.; Sargos, P.; Roupret, M. Chromogranin A: A useful biomarker in castration-resistant prostate cancer. World J. Urol. 2023, 41, 361–369. [Google Scholar] [CrossRef]
- Lawrence, B.; Gustafsson, B.I.; Kidd, M.; Pavel, M.; Svejda, B.; Modlin, I.M. The clinical relevance of chromogranin A as a biomarker for gastroenteropancreatic neuroendocrine tumors. Endocrinol. Metab. Clin. North. Am. 2011, 40, 111–134. [Google Scholar] [CrossRef]
- Konukiewitz, B.; Jesinghaus, M.; Kasajima, A.; Klöppel, G. Neuroendocrine neoplasms of the pancreas: Diagnosis and pitfalls. Virchows Arch. 2022, 480, 247–257. [Google Scholar] [CrossRef]
- Corti, A.; Marcucci, F.; Bachetti, T. Circulating chromogranin A and its fragments as diagnostic and prognostic disease markers. Pflug. Arch.-Eur. J. Physiol. 2018, 470, 199–210. [Google Scholar] [CrossRef]
- Ceconi, C.; Ferrari, R.; Bachetti, T.; Opasich, C.; Volterrani, M.; Colombo, B.; Parrinello, G.; Corti, A. Chromogranin A in heart failure; a novel neurohumoral factor and a predictor for mortality. Eur. Heart J. 2002, 23, 967–974. [Google Scholar] [CrossRef]
- Helle, K.B. Biochemical studies of the chromaffin granule. III. Redistribution of lipid phosphate, dopamine-β-hydroxylase and chromogranin a after freezing and thawing of the isolated granule membranes. Biochim. Biophys. Acta (BBA)-Biomembr. 1973, 318, 167–180. [Google Scholar] [CrossRef]
- Tota, B.; Cerra, M.C.; Gattuso, A. Catecholamines, cardiac natriuretic peptides and chromogranin A: Evolution and physiopathology of a “whip-brake” system of the endocrine heart. J. Exp. Biol. 2010, 213 Pt 18, 3081–3103. [Google Scholar] [CrossRef]
- Mahata, S.K.; Corti, A. Chromogranin A and its fragments in cardiovascular, immunometabolic, and cancer regulation. Ann. N. Y. Acad. Sci. 2019, 1455, 34–58. [Google Scholar] [CrossRef]
- Bandyopadhyay, G.K.; Mahata, S.K. Chromogranin A Regulation of Obesity and Peripheral Insulin Sensitivity. Front. Endocrinol. 2017, 8, 20. [Google Scholar] [CrossRef] [PubMed]
- Lugardon, K.; Raffner, R.; Goumon, Y.; Corti, A.; Delmas, A.; Bulet, P.; Aunis, D.; Metz-Boutigue, M.H. Antibacterial and antifungal activities of vasostatin-1, the N-terminal fragment of chromogranin A. J. Biol. Chem. 2000, 275, 10745–10753. [Google Scholar] [CrossRef] [PubMed]
- Helle, K.B.; Corti, A.; Metz-Boutigue, M.H.; Tota, B. The endocrine role for chromogranin A: A prohormone for peptides with regulatory properties. Cell. Mol. Life Sci. 2007, 64, 2863–2886. [Google Scholar] [CrossRef] [PubMed]
- Mahata, S.K.; Mahata, M.; Wakade, A.R.; O’Connor, D.T. Primary Structure and Function of the Catecholamine Release Inhibitory Peptide Catestatin (Chromogranin A344−364): Identification of Amino Acid Residues Crucial for Activity. Mol. Endocrinol. 2000, 14, 1525–1535. [Google Scholar] [CrossRef]
- Rousseau, G.; Reynier, P.; Jousset, N.; Rougé-Maillart, C.; Palmiere, C. Updated review of postmortem biochemical exploration of hypothermia with a presentation of standard strategy of sampling and analyses. Clin. Chem. Lab. Med. (CCLM) 2018, 56, 1819–1827. [Google Scholar] [CrossRef]
- Tomassini, L.; Lancia, M.; Gambelunghe, C.; Ricchezze, G.; Fedeli, P.; Cingolani, M.; De Micco, F.; Fiorucci, E.; Scendoni, R. Immunohistochemical insights into hypothermia-related deaths: A systematic review. Forensic Sci. Med. Pathol. 2025, 1–12. [Google Scholar] [CrossRef]
- Palmiere, C.; Teresiński, G.; Hejna, P. Postmortem diagnosis of hypothermia. Int. J. Leg. Med. 2014, 128, 607–614. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Available Data of the Cases | ||
|---|---|---|
| Parameter | Case 1 | Case 2 |
| Age | 67 years | 49 years |
| Location found | Snowy country road | Secluded wooded area |
| Ambient temperature (°C) | −1 to 2 °C | 1 to 3 °C |
| Time to autopsy | 12 h refrigerated | 18 h refrigerated |
| Key autopsy findings | WSs, cerebral/pulmonary edema, petechiae | WSs, cerebral/pulmonary edema, dermal vessel dilation |
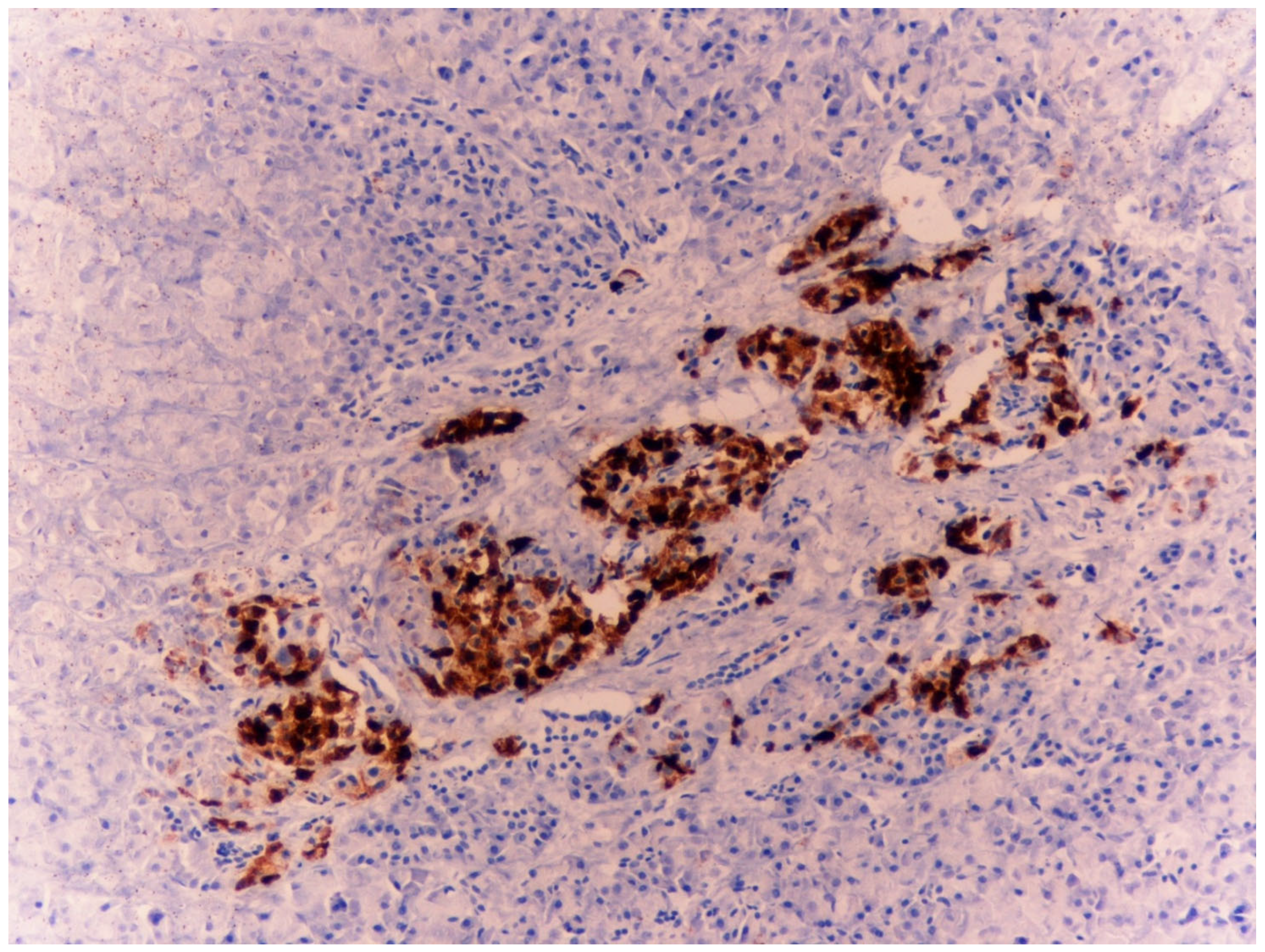
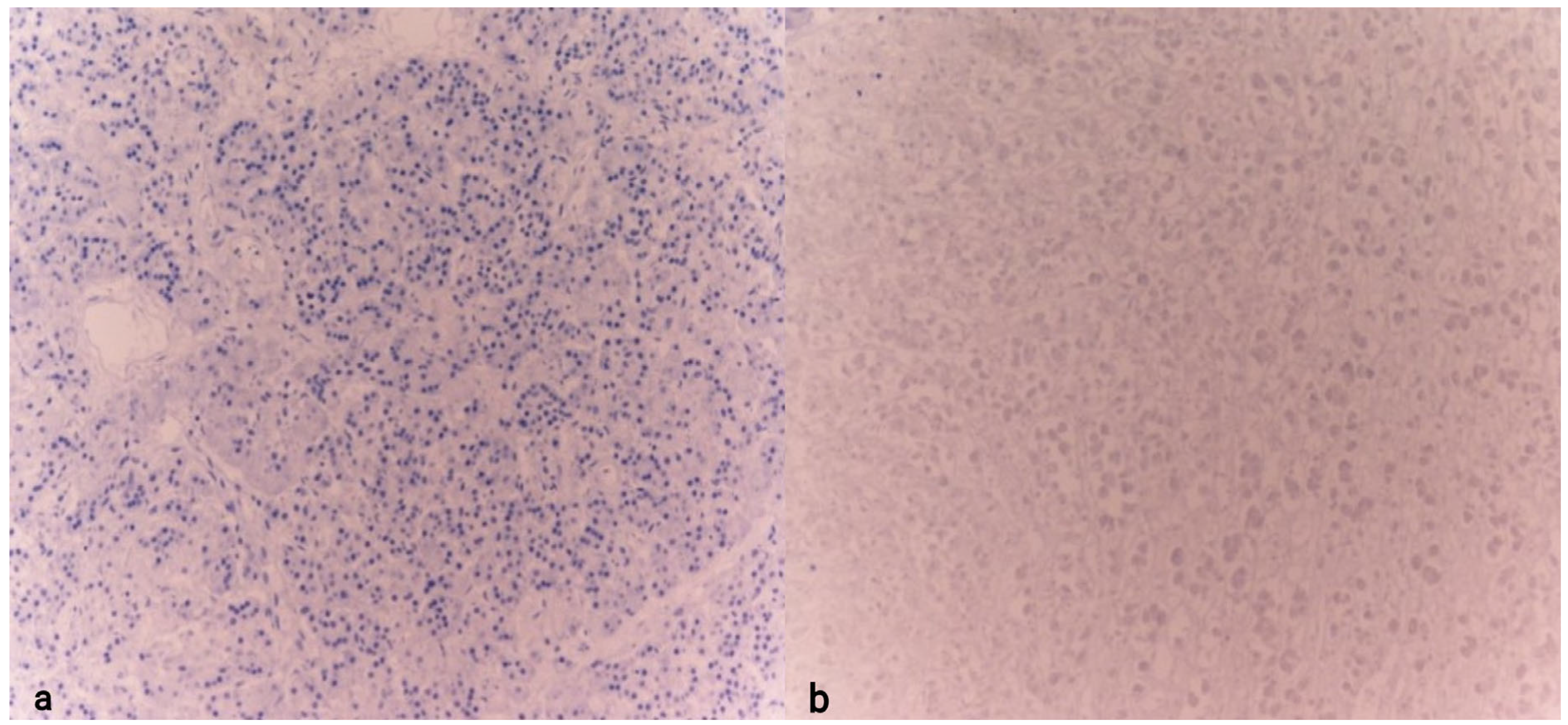
| CgA adrenal medulla | Strong positivity | Strong positivity |
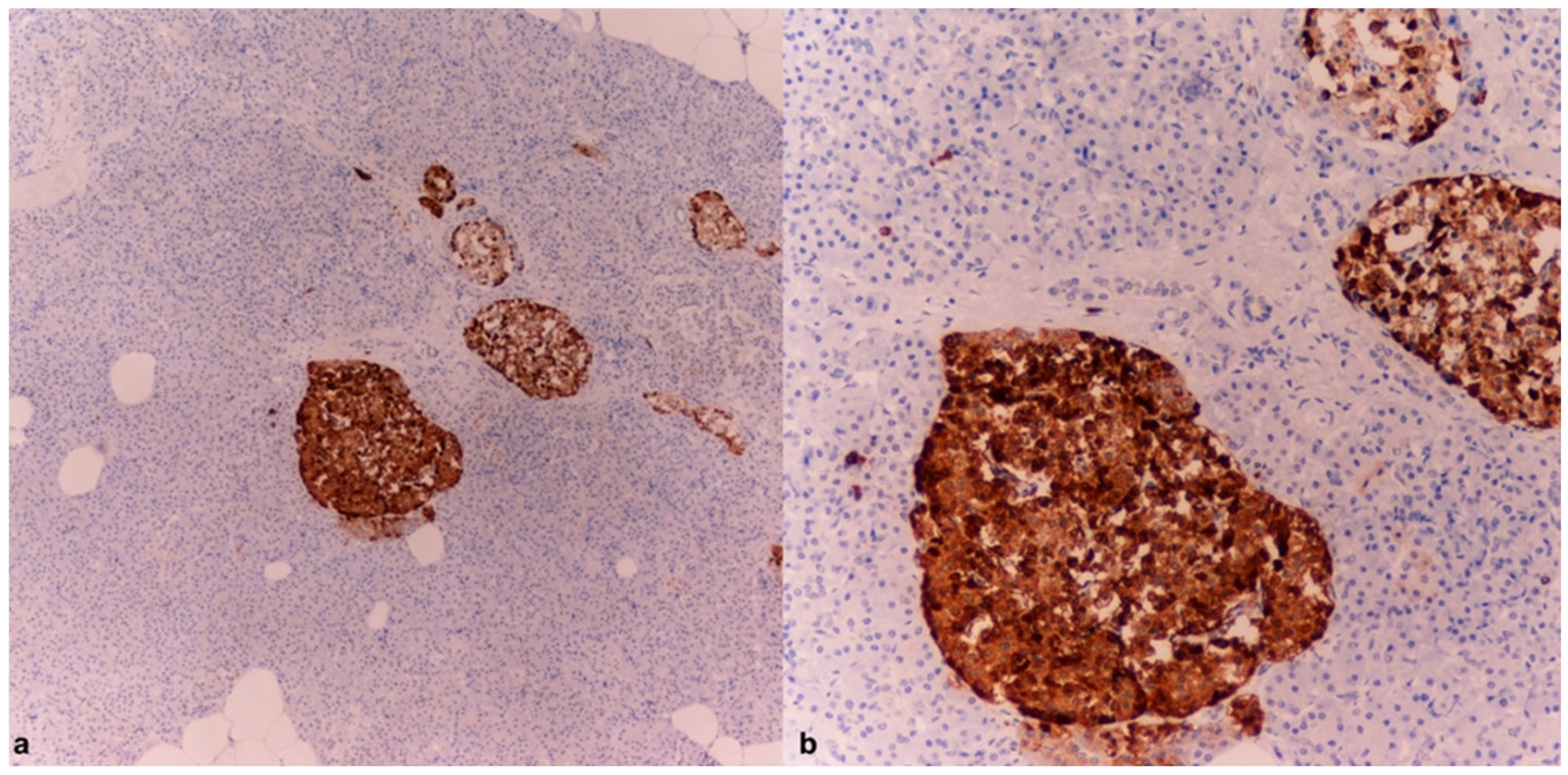
| CgA pancreatic islets | Strong positivity | Strong positivity |
| CgA hypothalamus | Not assessed | Not assessed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomassini, L.; Buratti, E.; Ricchezze, G.; Scendoni, R. Exploring Chromogranin A (CgA) as a Diagnostic Marker in Hypothermia-Related Deaths: Two Case Studies and a Literature Review. Diagnostics 2025, 15, 1673. https://doi.org/10.3390/diagnostics15131673
Tomassini L, Buratti E, Ricchezze G, Scendoni R. Exploring Chromogranin A (CgA) as a Diagnostic Marker in Hypothermia-Related Deaths: Two Case Studies and a Literature Review. Diagnostics. 2025; 15(13):1673. https://doi.org/10.3390/diagnostics15131673
Chicago/Turabian StyleTomassini, Luca, Erika Buratti, Giulia Ricchezze, and Roberto Scendoni. 2025. "Exploring Chromogranin A (CgA) as a Diagnostic Marker in Hypothermia-Related Deaths: Two Case Studies and a Literature Review" Diagnostics 15, no. 13: 1673. https://doi.org/10.3390/diagnostics15131673
APA StyleTomassini, L., Buratti, E., Ricchezze, G., & Scendoni, R. (2025). Exploring Chromogranin A (CgA) as a Diagnostic Marker in Hypothermia-Related Deaths: Two Case Studies and a Literature Review. Diagnostics, 15(13), 1673. https://doi.org/10.3390/diagnostics15131673