
Obscure Bleeding from a Metastatic Small Bowel Tumor Diagnosed Using Motorized Spiral Enteroscopy: A Case Study and a Literature Review

 , , , and
, , , and 
Abstract
1. Introduction
2. Case Presentation
2.1. Motorized Power Spiral Enteroscopy
2.2. Thoracic Computed Tomography
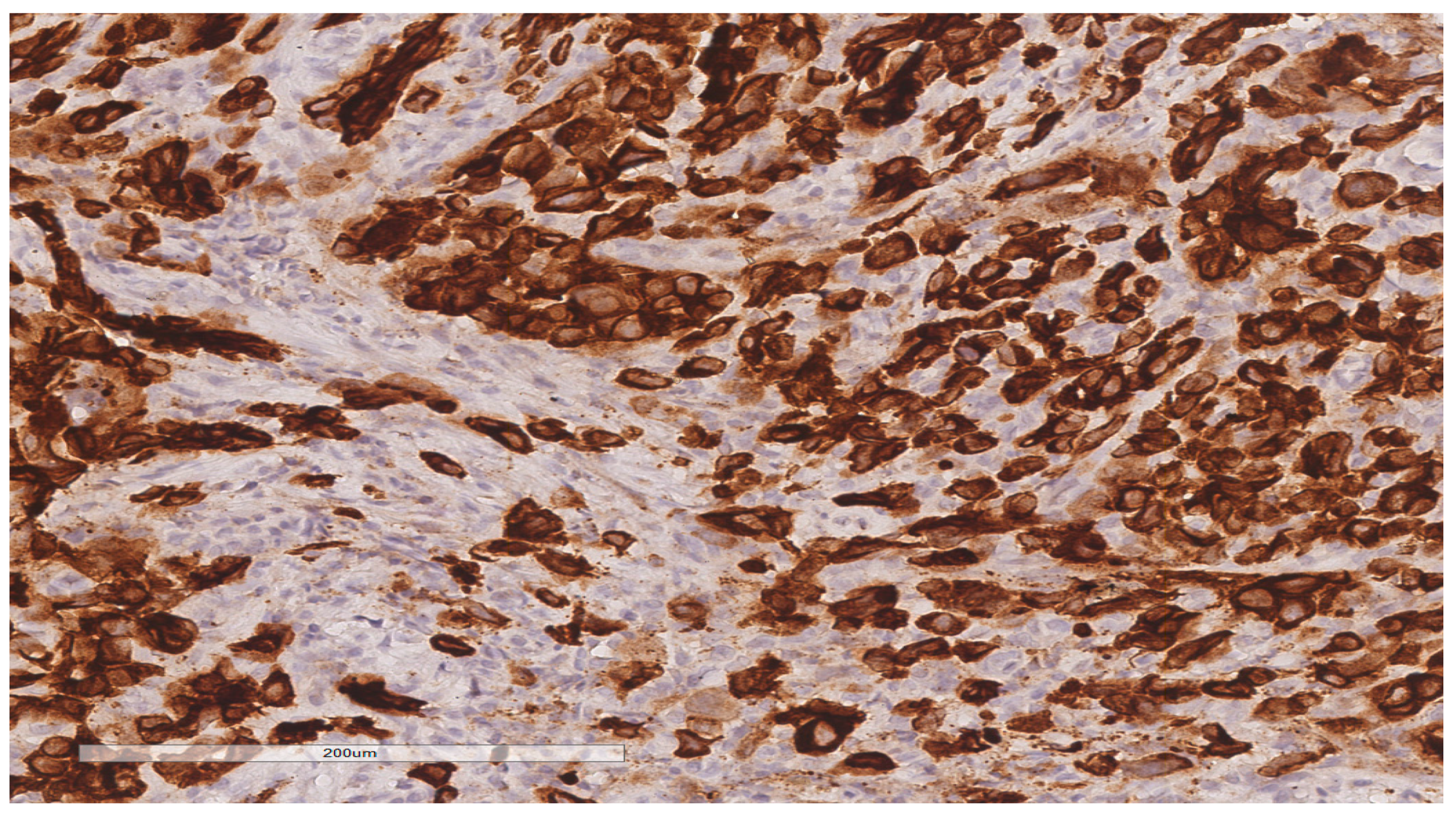
2.3. Surgical Procedure and Pathological Findings
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Khosla, D.; Dey, T.; Madan, R.; Gupta, R.; Goyal, S.; Kumar, N.; Kapoor, R. Small bowel adenocarcinoma: An overview. World J. Gastrointest. Oncol. 2022, 14, 413–422. Available online: https://www.wjgnet.com/1948-5204/full/v14/i2/413.htm (accessed on 3 February 2024). [CrossRef]
- Gore, R. Diagnosis and staging of small bowel tumours. Cancer Imaging 2006, 6, 209–212. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1766561/ (accessed on 3 February 2024). [CrossRef]
- Vlachou, E.; Koffas, A.; Toumpanakis, C.; Keuchel, M. Updates in the diagnosis and management of small-bowel tumors. Best Pract. Res. Clin. Gastroenterol. 2023, 64–65, 101860. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1521691823000409 (accessed on 3 February 2024). [CrossRef]
- Singh, P.; Singla, V.; Bopanna, S.; Shawl, M.R.; Garg, P.; Agrawal, J.; Arya, A.; Mittal, V.; Bhargava, R.; Madan, K. Safety and efficacy of the novel motorized power spiral enteroscopy: A single-center experience. DEN Open 2023, 3, e148. Available online: https://onlinelibrary.wiley.com/doi/10.1002/deo2.148 (accessed on 3 February 2024). [CrossRef]
- Kim, S.Y.; Ha, H.K.; Park, S.W.; Kang, J.; Kim, K.W.; Lee, S.S.; Park, S.H.; Kim, A.Y. Gastrointestinal Metastasis from Primary Lung Cancer: CT Findings and Clinicopathologic Features. Am. J. Roentgenol. 2009, 193, W197–W201. Available online: https://www.ajronline.org/doi/10.2214/AJR.08.1907 (accessed on 9 February 2024). [CrossRef]
- Song, J.Y.; Lee, B.J.; Yu, E.S.; Na, Y.J.; Park, J.-J.; Kim, J.S.; Bak, Y.-T. Small Bowel Metastatic Cancer Observed with Double Balloon Enteroscopy in a Patient with a Past History of Multiple Cancers. Intest. Res. 2015, 13, 350. Available online: http://irjournal.org/journal/view.php?doi=10.5217/ir.2015.13.4.350 (accessed on 9 February 2024). [CrossRef][Green Version]
- Li, J.; Wang, Z.; Liu, N.; Hao, J.; Xu, X. Small bowel adenocarcinoma of the jejunum: A case report and literature review. World J. Surg. Oncol. 2016, 14, 177. Available online: http://wjso.biomedcentral.com/articles/10.1186/s12957-016-0932-3 (accessed on 16 February 2024). [CrossRef]
- Vaz Safatle-Ribeiro, A.; Ribeiro, U., Jr. Impact of enteroscopy on diagnosis and management of small bowel tumors. Chin. J. Cancer Res. 2020, 32, 319–333. Available online: http://article.cjcrcn.org/en/article/doi/10.21147/j.issn.1000-9604.2020.03.04?viewType=HTML (accessed on 2 March 2024). [CrossRef]
- Zuckerman, G.R.; Prakash, C.; Askin, M.P.; Lewis, B.S. AGA technical review on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology 2000, 118, 201–221. [Google Scholar] [CrossRef]
- Mitchell, S.H.; Schaefer, D.C.; Dubagunta, S. A new view of occult and obscure gastrointestinal bleeding. Am. Fam. Physician. 2004, 69, 875–881. [Google Scholar]
- Mans, L.; Arvanitakis, M.; Neuhaus, H.; Devière, J. Motorized Spiral Enteroscopy for Occult Bleeding. Dig. Dis. 2018, 36, 325–327. Available online: https://www.karger.com/Article/FullText/488479 (accessed on 30 January 2024). [CrossRef]
- Beyna, T.; Arvanitakis, M.; Schneider, M.; Gerges, C.; Hoellerich, J.; Devière, J.; Neuhaus, H. Total motorized spiral enteroscopy: First prospective clinical feasibility trial. Gastrointest. Endosc. 2021, 93, 1362–1370. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0016510720349348 (accessed on 2 March 2024). [CrossRef]
- Nabi, Z.; Samanta, J.M.; Chavan, R.M.; Dhar, J.M.; Hussain, S.M.; Singh, A.P.M.; Rughwani, H.M.; Reddy, D.M. Role of Novel Motorized Enteroscopy in the Evaluation of Small Bowel Diseases. J. Clin. Gastroenterol. 2024, 58, 349–359. Available online: https://journals.lww.com/10.1097/MCG.0000000000001862 (accessed on 28 January 2024). [CrossRef]
- Giordano, A.; Casanova, G.; Escapa, M.; Fernández-Esparrach, G.; Ginès, À.; Sendino, O.; Araujo, I.K.; Cárdenas, A.; Córdova, H.; Martínez-Ocon, J.; et al. Motorized Spiral Enteroscopy Is Effective in Patients with Prior Abdominal Surgery. Dig. Dis. Sci. 2023, 68, 1447–1454. Available online: https://link.springer.com/10.1007/s10620-022-07688-1 (accessed on 9 January 2024). [CrossRef] [PubMed]
- Prasad, M.; Prasad, V.M.; Sangameswaran, A.; Verghese, S.C.; Murthy, V.; Prasad, M.; Shanker, G.K.; Koppal, S. A spiraling journey into the small bowel: A case series of novel motorized power spiral enteroscopies. VideoGIE 2020, 5, 591–596. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2468448120302502 (accessed on 9 February 2024). [CrossRef]
- Mensink, P.B.F. Complications of Double Balloon Enteroscopy. Tech. Gastrointest. Endosc. 2008, 10, 66–69. Available online: https://linkinghub.elsevier.com/retrieve/pii/S1096288307001088 (accessed on 28 January 2024). [CrossRef]
- Akerman, P.A.; Cantero, D. Severe Complications of Spiral Enteroscopy in the First 1750 Patients. Gastrointest. Endosc. 2009, 69, AB127. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0016510709006415 (accessed on 9 February 2024). [CrossRef]
- Rughwani, H.; Singh, A.P.; Ramchandani, M.; Jagtap, N.; Pal, P.; Inavolu, P.; Reddy, P.M.; Januszewicz, W.; Sekaran, A.; Nabi, Z.; et al. A Randomized, Controlled Trial Comparing the Total Enteroscopy Rate and Diagnostic Efficacy of Novel Motorized Spiral Enteroscopy and Single-Balloon Enteroscopy in Patients with Small-Bowel Disorders: The Motor Trial (NCT 05548140). Am. J. Gastroenterol. 2023, 118, 1855–1863. Available online: https://journals.lww.com/10.14309/ajg.0000000000002409 (accessed on 30 January 2024). [CrossRef]
- Falt, P.; Urban, O. Motorized spiral enteroscopy—A prospective analysis of 82 procedures at a single tertiary center. Scand. J. Gastroenterol. 2023, 58, 1207–1212. Available online: https://www.tandfonline.com/doi/full/10.1080/00365521.2023.2212311 (accessed on 3 February 2024). [CrossRef]
- Wang, Y.; Ma, B.; Li, W.; Li, P. Effectiveness and safety of novel motorized spiral enteroscopy: A systematic review and meta-analysis. Surg. Endosc. 2023, 37, 6998–7011. Available online: https://link.springer.com/10.1007/s00464-023-10179-7 (accessed on 30 January 2024). [CrossRef]
- Wang, J.; Chen, Y.; Zhang, S.; Chen, Q. Perforation of small intestine secondary to metastatic lung adenocarcinoma. Medicine 2018, 97, e13469. Available online: https://journals.lww.com/00005792-201812070-00069 (accessed on 22 February 2024). [CrossRef] [PubMed]
- Barsouk, A.; Rawla, P.; Barsouk, A.; Thandra, K.C. Epidemiology of Cancers of the Small Intestine: Trends, Risk Factors, and Prevention. Med. Sci. 2019, 7, 46. Available online: https://www.mdpi.com/2076-3271/7/3/46 (accessed on 22 February 2024). [CrossRef] [PubMed]
- Hu, Y.; Feit, N.; Huang, Y.; Xu, W.; Zheng, S.; Li, X. Gastrointestinal metastasis of primary lung cancer: An analysis of 366 cases. Oncol. Lett. 2018, 15, 9766–9776. Available online: http://www.spandidos-publications.com/10.3892/ol.2018.8575 (accessed on 3 March 2024). [CrossRef] [PubMed]
- Hillenbrand, A.; Sträter, J.; Henne-Bruns, D. Frequency, symptoms and outcome of intestinal metastases of bronchopulmonary cancer. Case report and review of the literature. Int. Semin. Surg. Oncol. 2005, 2, 13. Available online: https://issoonline.biomedcentral.com/articles/10.1186/1477-7800-2-13 (accessed on 25 February 2024). [CrossRef] [PubMed][Green Version]
- Ogasawara, N.; Ono, S.; Sugiyama, T.; Adachi, K.; Yamaguchi, Y.; Izawa, S.; Ebi, M.; Funaki, Y.; Sasaki, M.; Kasugai, K. Small-Intestinal Metastasis from Lung Carcinoma. Case Rep. Gastroenterol. 2022, 16, 195–200. Available online: https://www.karger.com/Article/FullText/523663 (accessed on 29 January 2024). [CrossRef] [PubMed]
- Misiakos, E.P.; Gouloumi, A.; Schizas, D.; Damaskou, V.; Tsapralis, D.; Farrugia, F.; Machairas, N.; Papaconstantinou, D.; Tzaneti, A.; Machairas, A. Small bowel perforation with multiple intestinal metastases from lung carcinoma: A case report. Oncol. Lett. 2019, 17, 3862–3866. Available online: http://www.spandidos-publications.com/10.3892/ol.2019.10031 (accessed on 29 January 2024). [CrossRef] [PubMed]
- Pleština, S.; Librenjak, N.; Marušić, A.; Batelja Vuletić, L.; Janevski, Z.; Jakopović, M. An extremely rare primary sarcoma of the lung with peritoneal and small bowel metastases: A case report. World J. Surg. Oncol. 2019, 17, 147. Available online: https://wjso.biomedcentral.com/articles/10.1186/s12957-019-1691-8 (accessed on 15 February 2024). [CrossRef] [PubMed]
- Zhong, Y.; Tang, X.; Deng, B. Capsule Endoscopy-Based Diagnosis of Lung Squamous Cell Carcinoma Associated with Abdominal Pain and Metastasis to Small Intestine: A Case Report. Case Rep. Oncol. 2023, 16, 108–114. Available online: https://karger.com/doi/10.1159/000529060 (accessed on 15 February 2024). [CrossRef] [PubMed]
- Ying, X.; Wang, M.; Verma, V.; Wang, M.; Ye, S.; Bi, J.; Zhou, X.; Han, G.; Zhen, W. Metastatic spread of solid subtype lung adenocarcinoma to the small intestine with anemia and melena. Medicine 2017, 96, e7768. Available online: https://journals.lww.com/00005792-201708250-00017 (accessed on 15 February 2024). [CrossRef]
- Li, J.; Zhao, Y.; Yu, Y. Metastatic spread of primary lung adenocarcinoma to the small intestine: A case report. Int. J. Surg. Case Rep. 2024, 114, 109111. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2210261223012403 (accessed on 15 February 2024). [CrossRef]
- Li, X.; Li, S.; Ma, Z.; Zhao, S.; Wang, X.; Wen, D. Multiple gastrointestinal metastases of squamous-cell lung cancer. Medicine 2018, 97, e11027. Available online: https://journals.lww.com/00005792-201806150-00024 (accessed on 29 January 2024). [CrossRef] [PubMed]
- Janež, J. Acute intestinal obstruction due to metastatic lung cancer—Case report. J. Surg. Case Rep. 2017, 2017, rjx031. Available online: http://academic.oup.com/jscr/article/doi/10.1093/jscr/rjx031/3001995 (accessed on 3 March 2024). [CrossRef][Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Values | Reference Values | |
|---|---|---|
| Erythrocytes (RBC) | 3.69 × 106/μL | 4.5∙106–5.9 × 106/μL |
| Hemoglobin (HGB) | 9.6 g/dL | 13.5–17.5 g/dL |
| Hematocrit (HCT) | 30.60% | 37–53% |
| Mean corpuscular hemoglobin concentration (MCHC) | 31.4 g/dL | 32–36.5 g/dL |
| Leukocytes | 7.6 × 103/μL | 4.5 × 103–10 × 103/μL |
| Lymphocytes | 22% | 24–44% |
| Thrombocytes (PLT) | 494 × 103/μL | 150 × 103–450 × 103/μL |
| Erythrocyte Sedimentation Rate (ESR) | 57 mm/h | 1–15 mm/h |
| INR | 1.11 INR ISI | 0.9–1.10 INR ISI |
| Serum iron | 27 μg/dL | 50–175 μg/dL |
| GOT | 9.00 UI/L | 10–37 UI/L |
| GPT | 6.5 UI/L | 12–63 UI/L |
| Creatinine | 0.55 mg/dL | 0.6–1.30 mg/dL |
| Alkaline phosphatase | 49.00 U/L | 50–136 U/L |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Banciu, C.; Munteanu, A.; Aprotosoaie, A.; Fabian, R.; Dobrescu, A.; Vaduva, A.; Fabian, A.; Soica, I.; Ivan, V.; Sima, L. Obscure Bleeding from a Metastatic Small Bowel Tumor Diagnosed Using Motorized Spiral Enteroscopy: A Case Study and a Literature Review. Diagnostics 2024, 14, 904. https://doi.org/10.3390/diagnostics14090904
Banciu C, Munteanu A, Aprotosoaie A, Fabian R, Dobrescu A, Vaduva A, Fabian A, Soica I, Ivan V, Sima L. Obscure Bleeding from a Metastatic Small Bowel Tumor Diagnosed Using Motorized Spiral Enteroscopy: A Case Study and a Literature Review. Diagnostics. 2024; 14(9):904. https://doi.org/10.3390/diagnostics14090904
Chicago/Turabian StyleBanciu, Christian, Andreea Munteanu, Adrian Aprotosoaie, Ramona Fabian, Amadeus Dobrescu, Adrian Vaduva, Antonio Fabian, Irina Soica, Viviana Ivan, and Laurentiu Sima. 2024. "Obscure Bleeding from a Metastatic Small Bowel Tumor Diagnosed Using Motorized Spiral Enteroscopy: A Case Study and a Literature Review" Diagnostics 14, no. 9: 904. https://doi.org/10.3390/diagnostics14090904
APA StyleBanciu, C., Munteanu, A., Aprotosoaie, A., Fabian, R., Dobrescu, A., Vaduva, A., Fabian, A., Soica, I., Ivan, V., & Sima, L. (2024). Obscure Bleeding from a Metastatic Small Bowel Tumor Diagnosed Using Motorized Spiral Enteroscopy: A Case Study and a Literature Review. Diagnostics, 14(9), 904. https://doi.org/10.3390/diagnostics14090904