
Three-Dimensional Assessment of Upper Airway Volume and Morphology in Patients with Different Sagittal Skeletal Patterns

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design, Participants, Measurements, and Variables
- Nasion (N): most anterior point on the frontonasal suture in the midsagittal plane.
- Sella (S): center of the pituitary fossa of the sphenoid bone.
- Point A (A): deepest point of the curve of the anterior border of the maxilla.
- Point B (B): most posterior point in the concavity along the anterior border of the symphysis.
- SNA: angle between the Sella, Nasion, and A point; this angle measures the position of the upper jaw relative to the base of the skull.
- SNB: angle between the Sella, Nasion, and B point; this angle measures the lower jaw’s position relative to the skull’s base.
- ANB: angle between point A, the Nasion, and point B, indicating the relationship between the upper and lower jaws.
- SN: plane between the Sella and Nasion.
- Anterior nasal spine (ANS): anterior tip of the sharp bony process of the maxilla at the lower margin of the anterior nasal aperture.
- Posterior nasal spine (PNS): posterior limit of the palatine bone.
2.2. Data Measurement
2.3. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zheng, Z.H.; Yamaguchi, T.; Kurihara, A.; Li, H.F.; Maki, K. Three-dimensional evaluation of upper airway in patients with different anteroposterior skeletal patterns. Orthod. Craniofacial Res. 2014, 17, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Brito, F.C.; Brunetto, D.P.; Nojima, M.C.G. Three-dimensional study of the upper airway in different skeletal Class II malocclusion patterns. Angle Orthod. 2019, 89, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Azevêdo, M.S.; Machado, A.W.; Barbosa, I.D.S.; Esteves, L.S.; Rocha, V.Á.C.; Bittencourt, M.A.V. Evaluation of upper airways after bimaxillary orthognathic surgery in patients with skeletal Class III pattern using cone-beam computed tomography. Dent. Press J. Orthod. 2016, 21, 34–41. [Google Scholar] [CrossRef]
- Golchini, E.; Rasoolijazi, H.; Momeni, F.; Shafaat, P.; Ahadi, R.; Jafarabadi, M.A.; Rahimian, S. Investigation of the relationship between mandibular morphology and upper airway dimensions. J. Craniofacial Surg. 2020, 31, 1353–1361. [Google Scholar] [CrossRef]
- Masoud, A.I.; Jackson, G.W.; Carley, D.W. Sleep and airway assessment: A review for dentists. Cranio 2017, 35, 206–222. [Google Scholar] [CrossRef]
- Georgiadis, T.; Angelopoulos, C.; Papadopoulos, M.A.; Kolokitha, O.E. Three-Dimensional Cone-Beam Computed Tomography Evaluation of Changes in Naso-Maxillary Complex Associated with Rapid Palatal Expansion. Diagnostics 2023, 13, 1322. [Google Scholar] [CrossRef] [PubMed]
- Kochar, G.D.; Chakranarayan, A.; Kohli, S.; Kohli, V.S.; Khanna, V.; Jayan, B.; Chopra, S.S.; Verma, M. Effect of surgical mandibular advancement on pharyngeal airway dimensions: A three-dimensional computed tomography study. Int. J. Oral Maxillofac. Surg. 2016, 45, 553–559. [Google Scholar] [CrossRef]
- Nath, M.; Ahmed, J.; Ongole, R.; Denny, C.; Shenoy, N. CBCT analysis of pharyngeal airway volume and comparison of airway volume among patients with skeletal Class I, Class II, and Class III malocclusion: A retrospective study. Cranio 2021, 39, 379–390. [Google Scholar] [CrossRef]
- Jacobs, R.; Salmon, B.; Codari, M.; Hassan, B.; Bornstein, M.M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 2018, 18, 88. [Google Scholar] [CrossRef]
- Zimmerman, J.N.; Vora, S.R.; Pliska, B.T. Reliability of upper airway assessment using CBCT. Eur. J. Orthod. 2019, 41, 101–108. [Google Scholar] [CrossRef]
- Yamashita, A.L.; Iwaki Filho, L.; Leite, P.C.C.; de Lima Navarro, R.; Ramos, A.L.; Previdelli, I.T.S.; Dal Molin Ribeiro, M.H.; Iwaki, L.C.V. Three-dimensional analysis of the pharyngeal airway space and hyoid bone position after orthognathic surgery. J. Cranio-Maxillofac. Surg. 2017, 45, 1408–1414. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, R. Cone-beam computed tomography and three-dimensional orthodontics. Where we are and future perspectives. J. Orthod. 2019, 46 (Suppl. 1), 45–48. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, D.C., III. Dentistry’s Great Awakening. Cranio 2018, 36, 139–140. [Google Scholar] [CrossRef] [PubMed]
- Gholinia, F.; Habibi, L.; Amrollahi Boyouki, M. Cephalometric evaluation of the upper airway in different skeletal classifications of jaws. J. Craniofacial Surg. 2019, 30, e469–e474. [Google Scholar] [CrossRef]
- D’Onofrio, L. Oral dysfunction as a cause of malocclusion. Orthod. Craniofacial Res. 2019, 22, 43–48. [Google Scholar] [CrossRef]
- Alhammadi, M.S.; Almashraqi, A.A.; Halboub, E.; Almahdi, S.; Jali, T.; Atafi, A.; Alomar, F. Pharyngeal airway spaces in different skeletal malocclusions: A CBCT 3D assessment. Cranio 2019, 39, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Sfondrini, M.F.; Gallo, S.; Pascadopoli, M.; Gandini, P.; Roncoroni, C.; Scribante, A. Upper Airway Dimensions among Different Skeletal Malocclusions: A Retrospective Observational Study by Cephalometric Analysis. Dent. J. 2024, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Rivlin, J.; Hoffstein, V.; Kalbfleisch, J.; McNichols, W.; Zamel, N.; Bryan, A.C. Upper Airway Morphology in Patients with Idiopathic Obstructive Sleep Apnea. Surv. Anesthesiol. 1985, 29, 42. [Google Scholar] [CrossRef]
- Di Carlo, G.; Polimeni, A.; Melsen, B.; Cattaneo, P.M. The relationship between upper airways and craniofacial morphology studied in 3D. A CBCT study. Orthod. Craniofac. Res. 2015, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Alswairki, H.J.; Alam, M.K.; Rahman, S.A.; Alsuwailem, R.; Alanazi, S.H. Upper airway changes in diverse orthodontic looms: A systematic review and meta-analysis. Appl. Sci. 2022, 12, 916. [Google Scholar] [CrossRef]
- Kwong, J.C.; Palomo, J.M.; Landers, M.A.; Figueroa, A.; Hans, M.G. Image quality produced by different cone-beam computed tomography settings. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Abdelkarim, A.Z.; Khalifa, A.R.; Hassan, M.G.; Abdou, A.; Duman, S.B.; Rezallah, N.N.; Abdraboh, A.E.; Ghoneima, A. Three-Dimensional Assessment of the Pharyngeal Airway in Growing versus Non-Growing Subjects with/without Cleft Lip and Palate. Anatomia 2023, 2, 192–205. [Google Scholar] [CrossRef]
- Fountoulaki, G.; Thurzo, A. Change in the Constricted Airway in Patients after Clear Aligner Treatment: A Retrospective Study. Diagnostics 2022, 12, 2201. [Google Scholar] [CrossRef] [PubMed]
- Osorio, F.; Perilla, M.; Doyle, D.J.; Palomo, J.M. Cone beam computed tomography: An innovative tool for airway assessment. Anesth. Analg. 2008, 106, 1803–1807. [Google Scholar] [CrossRef] [PubMed]
- Lanteri, V.; Farronato, M.; Ugolini, A.; Cossellu, G.; Gaffuri, F.; Parisi, F.M.R.; Cavagnetto, D.; Abate, A.; Maspero, C. Volumetric Changes in the Upper Airways after Rapid and Slow Maxillary Expansion in Growing Patients: A Case-Control Study. Materials 2020, 13, 2239. [Google Scholar] [CrossRef] [PubMed]
- Ortu, E.; Giannoni, M.; Ortu, M.; Gatto, R.; Monaco, A. Oropharyngeal airway changes after rapid maxillary expansion: The state of the art. Int. J. Clin. Exp. Med. 2014, 7, 1632–1638. [Google Scholar] [PubMed]
- Tsolakis, I.A.; Kolokitha, O.-E. Comparing Airway Analysis in Two-Time Points after Rapid Palatal Expansion: A CBCT Study. J. Clin. Med. 2023, 12, 4686. [Google Scholar] [CrossRef]
- Kirjavainen, M.; Kirjavainen, T. Upper airway dimensions in Class II malocclusion. Ef-fects of headgear treatment. Angle Orthod. 2007, 77, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Bokhari, F.; Yosaf, U.; Qayyum, F.; Jamil, A.; Jamil, M. CBCT Based Comparison of Pharyngeal Airway Area and Volume in patients with Angle’s Class I and Class II Malocclusion: A Retrospective Study. Pak. J. Med. Health Sci. 2022, 16, 21–23. [Google Scholar] [CrossRef]
- Kim, Y.I.; Schroeder, J.; Lynch, D.; Newell, J.; Make, B.; Friedlander, A.; Estépar, R.S.; Hanania, N.A.; Washko, G.; Murphy, J.R.; et al. Gender differences of airway dimensions in anatomically matched sites on CT in smokers. COPD 2011, 8, 285–292. [Google Scholar] [CrossRef]
- Dominelli, P.B.; Ripoll, J.G.; Cross, T.J.; Baker, S.E.; Wiggins, C.C.; Welch, B.T.; Joyner, M.J. Sex differences in large conducting airway anatomy. J. Appl. Physiol. 1985, 125, 960–965. [Google Scholar] [CrossRef] [PubMed]
- Gungor, A.Y.; Turkkahraman, H. Effects of Airway Problems on Maxillary Growth: A Review. Eur. J. Dent. 2009, 3, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, J.E.; Kim, Y.H.; Kang, B.C.; Heo, S.B.; Kim, C.K.; Park, W.K. An assessment of oropharyngeal airway position using a fibreoptic bronchoscope. Anaesthesia 2014, 69, 53–57. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zhang, J.; Honda, K.; Wei, J.; Kitamura, T. Morphological characteristics of male and female hypopharynx: A magnetic resonance imaging-based study. J. Acoust. Soc. Am. 2019, 145, 734. [Google Scholar] [CrossRef]
- Rantavuori, K.; Silvola, A.-S.; Suominen, A.; Masood, M.; Suominen, A.L.; Lahti, S. Gender differences in the association between malocclusion traits and oral health-related quality of life in Finnish adults. Eur. J. Oral Sci. 2023, 131, e12927. [Google Scholar] [CrossRef]
- Yu, M.; Hao, Z.L.; Xu, L.Y.; Wen, Y.F.; Han, F.; Gao, X.M. Craniofacial anatomical Characteristics of patients with catathrenia. Zhonghua Kou Qiang Yi Xue Za Zhi 2023, 58, 659–669. (In Chinese) [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H. Study on Airway Size in Class III Malocclusion by the Gender. Korean J. Phys. Anthropol. 2017, 30, 145. [Google Scholar] [CrossRef]
- Meehan, M.; Teschner, M.; Girod, S. Three-dimensional simulation and prediction of craniofacial surgery. Orthod. Craniofacial. Res. 2003, 6 (Suppl. 1), 102–107. [Google Scholar] [CrossRef]
- Savoldi, F.; Dagassan-Berndt, D.; Patcas, R.; Mak, W.S.; Kanavakis, G.; Verna, C.; Gu, M.; Bornstein, M.M. The use of CBCT in orthodontics with special focus on upper airway analysis in patients with sleep-disordered breathing. Dentomaxillofacial Radiol. 2024, 53, 178–188. [Google Scholar] [CrossRef]
- Christovam, I.O.; Lisboa, C.O.; Ferreira, D.M.; Cury-Saramago, A.A.; Mattos, C.T. Upper airway dimensions in patients undergoing orthognathic surgery: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Surg. 2016, 45, 460–471. [Google Scholar] [CrossRef]
- Hsu, W.C.; Kang, K.T.; Yao, C.J.; Chou, C.H.; Weng, W.C.; Lee, P.L.; Chen, Y.J. Evaluation of Upper Airway in Children with Obstructive Sleep Apnea Using Cone-Beam Computed Tomography. Laryngoscope 2021, 131, 680–685. [Google Scholar] [CrossRef] [PubMed]
- Masoud, A.I.; Alwadei, F.H. Two-dimensional upper airway normative values in children aged 7 to 17 years. Cranio 2022, 40, 536–543. [Google Scholar] [CrossRef]
- Gurani, S.F.; Cattaneo, P.M.; Rafaelsen, S.R.; Pedersen, M.R.; Thorn, J.J.; Pinholt, E.M. The effect of altered head and tongue posture on upper airway volume based on a validated upper airway analysis-An MRI pilot study. Orthod. Craniofac. Res. 2020, 23, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Masoud, A.I.; Alwadei, A.H.; Gowharji, L.F.; Park, C.G.; Carley, D.W. Relating three-dimensional airway measurements to the apnea-hypopnea index in pediatric sleep apnea patients. Orthod. Craniofac. Res. 2021, 24, 137–146. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Superior Limit | Inferior Limit | |
|---|---|---|
| Oropharynx | Line extending from the PNS to the tip of the odontoid process. | Line extending from the antero-inferior border of the C2 vertebra. |
| Hypopharynx | Line extending from the antero-inferior border of the C2 vertebra. | Line extending from the horizontal line coming into contact with the most superior margin of the body of the hyoid bone. |
| Variables | Class I | Class II | Class III | Intergroup Comparison * | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
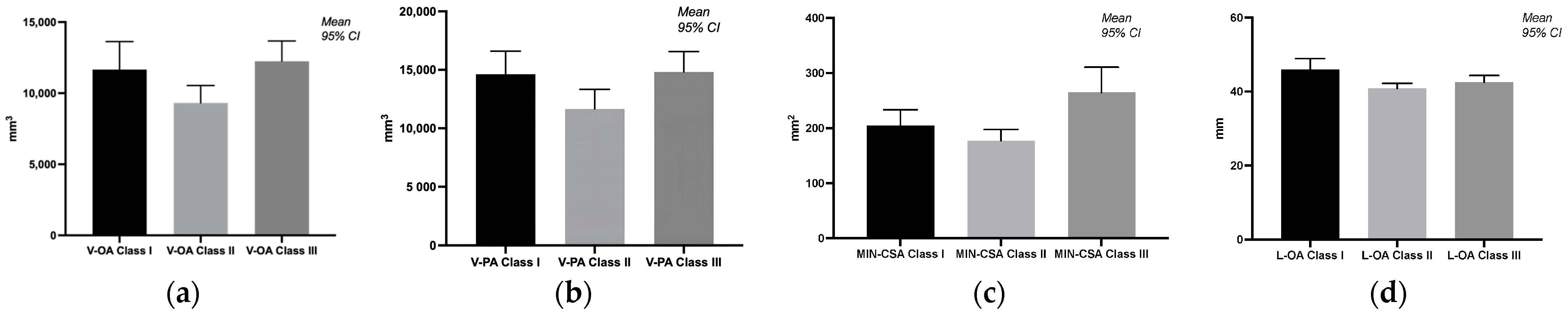
| V-OA | 11,660 | 5076 | 9313 | 3156 | 12,256 | 3647 | - |
| V-HA | 2966 | 1979 | 2354 | 1655 | 2567 | 1151 | class III > class I > class II |
| V-PA | 14,626 | 5094 | 11,667 | 4280 | 14,823 | 4479 | - |
| MIN-CSA | 204.9 | 74.56 | 177.2 | 52.39 | 264.8 | 117.9 | class III > class I > class II |
| L-OA | 45.99 | 7.603 | 40.92 | 3.468 | 42.60 | 4.589 | class III > class I > class II |
| L-HA | 13.23 | 5.911 | 14.62 | 4.318 | 14.39 | 4.480 | class I > class III > class II |
| L-PA | 59.22 | 7.628 | 55.60 | 2.746 | 56.99 | 4.718 | - |
| Variables | Class I | Class II | Class III | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Male | Female | p-Value | Male | Female | p-Value | Male | Female | p-Value | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||||
| V-OA | 12,484 (4256) | 11,671 (5907) | 0.5397 | 10,245 (2532) | 8673 (3717) | 0.1152 | 12,491 (3222) | 12,443 (3374) | 0.9746 |
| V-HA | 4857 (1823) | 1711 (684.5) | 0.0003 *** | 3127 (2121) | 2049 (1171) | 0.0559 | 3095 (1145) | 2278 (972.3) | 0.4506 |
| V-PA | 17,341 (2546) | 13,383 (5856) | 0.0069 ** | 13372 (3995) | 10,722 (4557) | 0.2135 | 15,587 (4234) | 14,721 (3930) | 0.5248 |
| MIN-CSA | 198.4 (41.62) | 213.2 (89.79) | 0.8605 | 206 (59.8) | 153.9 (29.94) | 0.0091 ** | 329.4 (140.3) | 225.5 (51.65) | 0.0184 * |
| L-OA | 49.74 (6.171) | 44.24 (7.915) | 0.0834 | 39.1 (3.207) | 42.3 (3.303) | 0.0559 | 40.19 (4.595) | 43.88 (4.202) | 0.0118 * |
| L-HA | 17.07 (7.392) | 10.58 (2.844) | 0.0316 * | 15.2 (4.115) | 14.55 (4.599) | >0.9999 | 16.98 (4.179) | 12.28 (3.404) | 0.0043 ** |
| L-PA | 66.81 (1.679) | 54.82 (5.839) | <0.0001 **** | 54.42 (2.416) | 56.85 (2.496) | 0.0221 * | 57.17 (6.653) | 56.15 (1.548) | 0.7547 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pop, S.I.; Procopciuc, A.; Arsintescu, B.; Mițariu, M.; Mițariu, L.; Pop, R.V.; Cerghizan, D.; Jánosi, K.M. Three-Dimensional Assessment of Upper Airway Volume and Morphology in Patients with Different Sagittal Skeletal Patterns. Diagnostics 2024, 14, 903. https://doi.org/10.3390/diagnostics14090903
Pop SI, Procopciuc A, Arsintescu B, Mițariu M, Mițariu L, Pop RV, Cerghizan D, Jánosi KM. Three-Dimensional Assessment of Upper Airway Volume and Morphology in Patients with Different Sagittal Skeletal Patterns. Diagnostics. 2024; 14(9):903. https://doi.org/10.3390/diagnostics14090903
Chicago/Turabian StylePop, Silvia Izabella, Ana Procopciuc, Bianca Arsintescu, Mihai Mițariu, Loredana Mițariu, Radu Vasile Pop, Diana Cerghizan, and Kinga Mária Jánosi. 2024. "Three-Dimensional Assessment of Upper Airway Volume and Morphology in Patients with Different Sagittal Skeletal Patterns" Diagnostics 14, no. 9: 903. https://doi.org/10.3390/diagnostics14090903
APA StylePop, S. I., Procopciuc, A., Arsintescu, B., Mițariu, M., Mițariu, L., Pop, R. V., Cerghizan, D., & Jánosi, K. M. (2024). Three-Dimensional Assessment of Upper Airway Volume and Morphology in Patients with Different Sagittal Skeletal Patterns. Diagnostics, 14(9), 903. https://doi.org/10.3390/diagnostics14090903