
The Advantages of Radiofrequency Echographic MultiSpectrometry in the Evaluation of Bone Mineral Density in a Population with Osteoarthritis at the Lumbar Spine



Abstract
1. Introduction
Aim of the Study
2. Materials and Methods
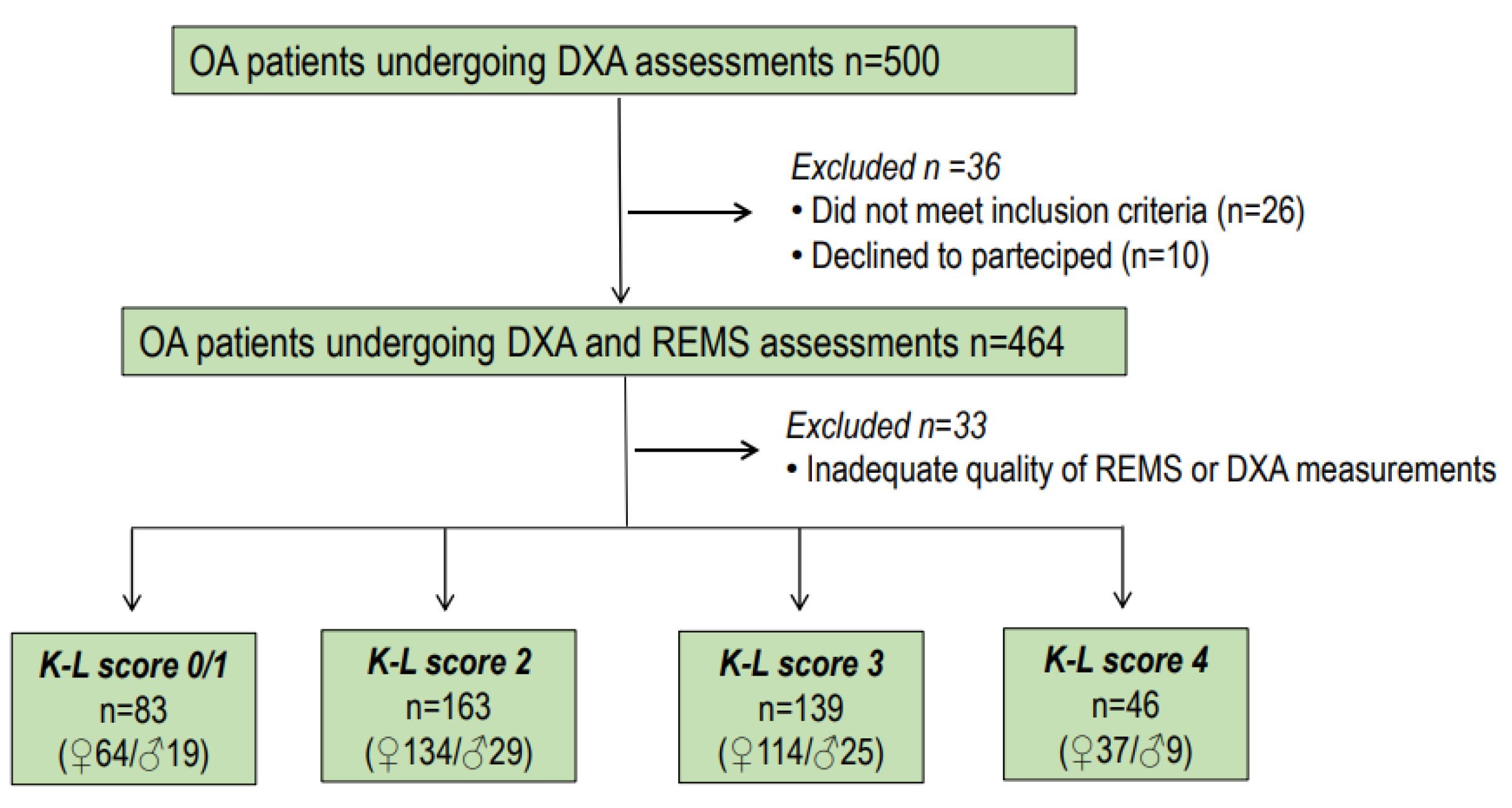
2.1. Study Design and Population
2.2. Digital X-ray Radiography
2.3. Dual-Energy X-ray Absorptiometry
2.4. Radiofrequency Echographic Multispectrometry (REMS)
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hart, D.; Mootoosamy, I.; Doyle, D.; Spector, T. The relationship between osteoarthritis and osteoporosis in the general population: The Chingford Study. Ann. Rheum. Dis. 1994, 53, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Im, G.I.; Kim, M.K. The relationship between osteoarthritis and osteoporosis. J. Bone Miner. Metab. 2014, 32, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Castaño-Betancourt, M.C.; Oei, L.; Rivadeneira, F.; de Schepper, E.I.; Hofman, A.; Bierma-Zeinstra, S.; Pols, H.A.; Uitterlinden, A.G.; Van Meurs, J.B. Association of lumbar disc degeneration with osteoporotic fractures: The Rotterdam Study and meta-analysis from systematic review. Bone 2013, 57, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Kasher, M.; Williams, F.M.K.; Freidin, M.B.; Cherny, S.; Livshits, G. An in-depth study of the associations between osteoarthritis- and osteoporosis-related phenotypes at different skeletal locations. Osteoporos. Int. 2020, 31, 2197–2208. [Google Scholar] [CrossRef]
- Kim, D.; Pirshahid, A.A.; Li, Y.; Varghese, T.; Pope, J.E. Prevalence of osteoporosis in osteoarthritis: A systematic review and meta-analysis. Osteoporos. Int. 2022, 33, 1687–1693. [Google Scholar] [CrossRef]
- Masud, T.; Langley, S.; Wiltshire, P.; Doyle, D.V.; Spector, T.D. Effect of spinal osteophytosis on bone mineral density measurements in vertebral osteoporosis. Br. Med. J. 1993, 307, 172–173. [Google Scholar] [CrossRef]
- Jones, G.; Nguyen, T.; Sambrook, P.N.; Kelly, P.J.; Eisman, J.A. A longitudinal study of the effect of spinal degenerative disease on bone density in the elderly. J. Rheumatol. 1995, 22, 932–936. [Google Scholar]
- Knight, S.M.; Ring, E.F.; Bhalla, A.K. Bone mineral density and osteoarthritis. Ann. Rheum. Dis. 1992, 51, 1025–1026. [Google Scholar] [CrossRef]
- Stewart, A.; Black, A.J. Bone mineral density in osteoarthritis. Curr. Opin. Rheumatol. 2000, 12, 464–477. [Google Scholar] [CrossRef]
- Martineau, P.; Bazarjani, S.; Zuckier, L.S. Artifacts and incidental findings encountered on dual energy X-ray absortiometry: Atlas and analysis. Semin. Nucl. Med. 2015, 45, 458–469. [Google Scholar] [CrossRef]
- Lewiecki, E.M.; Kendler, D.L.; Kiebzak, G.M.; Schmeer, P.; Prince, R.L.; El-Hajj Fuleihan, G.; Hans, D. Special report on the official positions of the International Society for Clinical Densitometry. Osteoporos. Int. 2004, 15, 779–784. [Google Scholar] [CrossRef]
- Gazzotti, S.; Aparisi Gómez, M.P.; Schileo, E.; Taddei, F.; Sangiorgi, L.; Fusaro, M.; Miceli, M.; Guglielmi, G.; Bazzocchi, A. High-resolution peripheral quantitative computed tomography: Research or clinical practice? Br. J. Radiol. 2023, 24, 20221016. [Google Scholar] [CrossRef]
- Kolta, S.; Briot, K.; Fechtenbaum, J.; Paternotte, S.; Armbrecht, G.; Felsenberg, D.; Glüer, C.C.; Eastell, R.; Roux, C. TBS result is not affected by lumbar spine osteoarthritis. Osteoporos. Int. 2014, 25, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Shevroja, E.; Reginster, J.Y.; Lamy, O.; Al-Daghri, N.; Chandran, M.; Demoux-Baiada, A.L.; Kohlmeier, L.; Lecart, M.P.; Messina, D.; Camargos, B.M.; et al. Update on the clinical use of trabecular bone score (TBS) in the management of osteoporosis: Results of an expert group meeting organized by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO), and the International Osteoporosis Foundation (IOF) under the auspices of WHO Collaborating Center for Epidemiology of Musculoskeletal Health and Aging. Osteoporos. Int. 2023, 34, 1501–1529. [Google Scholar] [CrossRef] [PubMed]
- Conversano, F.; Franchini, R.; Greco, A.; Soloperto, G.; Chiriacò, F.; Casciaro, E.; Aventaggiato, M.; Renna, M.D.; Pisani, P.; Di Paola, M.; et al. Novel Ultrasound Methodology for Estimating Spine Mineral Density. Ultrasound Med. Biol. 2015, 41, 281–300. [Google Scholar] [CrossRef] [PubMed]
- Di Paola, M.; Gatti, D.; Viapiana, O.; Cianferotti, L.; Cavalli, L.; Caffarelli, C.; Conversano, F.; Quarta, E.; Pisani, P.; Girasole, G.; et al. Radiofrequency echographic multispectrometry compared with dual X-ray absorptiometry for osteoporosis diagnosis on lumbar spine and femoral neck. Osteoporos. Int. 2019, 30, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Messina, C.; Gitto, S.; Colombo, R.; Fusco, S.; Guagliardo, G.; Piazza, M.; Poli, J.C.; Albano, D.; Sconfienza, L.M. Short-Term Precision and Repeatability of Radiofrequency Echographic Multi Spectrometry (REMS) on Lumbar Spine and Proximal Femur: An In Vivo Study. J. Imaging 2023, 9, 118. [Google Scholar] [CrossRef] [PubMed]
- Ramirez Zegarra, R.; Degennaro, V.; Brandi, M.L.; Cagninelli, G.; Casciaro, S.; Celora, G.; Conversano, F.; Lombardi, F.A.; Pisani, P.; Ghi, T. Longitudinal changes of the femoral bone mineral density from first to third trimester of pregnancy: Bone health assessment by means of non-ionizing REMS technology. Aging Clin. Exp. Res. 2024, 36, 31. [Google Scholar] [CrossRef]
- Adami, G.; Arioli, G.; Bianchi, G.; Brandi, M.L.; Caffarelli, C.; Cianferotti, L.; Gatti, D.; Girasole, G.; Gonnelli, S.; Manfredini, M.; et al. Radiofrequency echographic multi spectrometry for the prediction of incident fragility fractures: A 5-year follow-up study. Bone 2020, 134, 115297. [Google Scholar] [CrossRef]
- Cortet, B.; Dennison, E.; Diez-Perez, A.; Locquet, M.; Muratore, M.; Nogués, X.; OvejeroCrespo, D.; Quarta, E.; Brandi, M.L. Radiofrequency Echographic multi spectrometry (REMS) for the diagnosis of osteoporosis in a European multicenter clinical context. Bone 2021, 143, 115786. [Google Scholar] [CrossRef]
- Caffarelli, C.; Tomai Pitinca, M.D.; Al Refaie, A.; Ceccarelli, E.; Gonnelli, S. Ability of radiofrequency echographic multispectrometry to identify osteoporosis status in elderly women with type 2 diabetes. Aging Clin. Exp. Res. 2022, 34, 121–127. [Google Scholar] [CrossRef]
- Caffarelli, C.; Tomai Pitinca, M.D.; Al Refaie, A.; De Vita, M.; Catapano, S.; Gonnelli, S. Could radiofrequency echographic multispectrometry (REMS) overcome the overestimation in BMD by dual-energy X-ray absorptiometry (DXA) at the lumbar spine? BMC Musculoskelet. Disord. 2022, 23, 469. [Google Scholar] [CrossRef]
- Fassio, A.; Andreola, S.; Gatti, D.; Bianco, B.; Gatti, M.; Gambaro, G.; Rossini, M.; Viapiana, O.; Negrelli, R.; Adami, G. Radiofrequency echographic multi-spectrometry and DXA for the evaluation of bone mineral density in a peritoneal dialysis setting. Aging Clin. Exp. Res. 2023, 35, 185–192. [Google Scholar] [CrossRef]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef]
- International Society for Clinical Densitometry. Official Positions—Adult. 2019. Available online: http://www.iscd.org/official-positions/2019-iscd-official-positions-adult (accessed on 1 December 2021).
- Drinka, P.J.; DeSmet, A.A.; Bauwens, S.F.; Rogot, A. The effect of overlying calcification on lumbar bone densitometry. Calcif. Tissue. Int. 1992, 50, 507–510. [Google Scholar] [CrossRef]
- Arden, N.K.; Nevitt, M.C.; Lane, N.E.; Gore, L.R.; Hochberg, M.C.; Scott, J.C.; Pressman, A.R.; Cummings, S.R. Osteoarthritis and risk of falls, rates of bone loss, and osteoporotic fractures. Study of Osteoporotic Fractures Research Group. Arthritis Rheum. 1999, 42, 1378–1385. [Google Scholar] [CrossRef] [PubMed]
- Wright, N.C.; Lisse, J.R.; Walitt, B.T.; Eaton, C.B.; Chen, Z.; Women’s Health Initiative Investigators. Arthritis increases the risk for fractures--results from the Women’s Health Initiative. J. Rheumatol. 2011, 38, 1680–1688. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.Y.; Center, J.R.; Eisman, J.A.; Nguyen, T.V. Bone mineral density and association of osteoarthritis with fracture risk. Osteoarthr. Cartil. 2014, 22, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Diez-Perez, A.; Brandi, M.L.; Al-Daghri, N.; Branco, J.C.; Bruyère, O.; Cavalli, L.; Cooper, C.; Cortet, B.; Dawson-Hughes, B.; Dimai, H.P.; et al. Radiofrequency echographic multi-spectrometry for the in-vivo assessment of bone strength: State of the art-outcomes of an expert consensus meeting organized by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO). Aging Clin. Exp. Res. 2019, 31, 1375–1389. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | K-L Score 0/1 | K-L Score 2 | K-L Score 3 | K-L Score 4 | p | |
|---|---|---|---|---|---|---|
| Age (yrs) | 63.9 ± 11.2 | 59.2 ± 11.4 | 62.8 ± 11.0 | 65.9 ± 10.5 | 70.5 ± 9.4 | 0.0001 |
| Weight (Kg) | 70.3 ± 14.9 | 73.3 ± 17.4 | 68.8 ± 14.3 | 69.5 ± 14.1 | 72.3 ± 14.2 | 0.086 |
| Height (cm) | 163.6 ± 8.6 | 166.1 ± 9.4 | 163.0 ± 8.2 | 162.7 ± 8.1 | 163.6 ± 9.7 | 0.025 |
| BMI (Kg/m2) | 26.1 ± 4.6 | 26.3 ± 4.9 | 25.8 ± 4.4 | 26.1 ± 4.6 | 27.0 ± 4.3 | 0.379 |
| DXA LS-BMD (g/cm2) | 1.048 ± 0.198 | 0.956 ± 0.169 | 1.002 ± 0.153 | 1.078 ± 0.166 | 1.269 ± 0.269 | 0.0001 |
| DXA FN-BMD (g/cm2) | 0.782 ± 0.157 | 0.770 ± 0.155 | 0.761 ± 0.145 | 0.793 ± 0.158 | 0.841 ± 0.182 | 0.015 |
| DXA TH-BMD (g/cm2) | 0.900 ± 0.157 | 0.870 ± 0.146 | 0.888 ± 0.151 | 0.913 ± 0.159 | 0.952 ± 0.176 | 0.018 |
| REMS LS-BMD (g/cm2) | 0.854 ± 0.108 | 0.892 ± 0.127 | 0.858 ± 0.103 | 0.832 ± 0.095 | 0.835 ± 0.100 | 0.0001 |
| REMS FN-BMD (g/cm2) | 0.673 ± 0.126 | 0.717 ± 0.147 | 0.677 ± 0.122 | 0.647 ± 0.116 | 0.660 ± 0.113 | 0.001 |
| REMS TH-BMD (g/cm2) | 0.809 ± 0.145 | 0.858 ± 0.163 | 0.812 ± 0.138 | 0.781 ± 0.138 | 0.794 ± 0.132 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caffarelli, C.; Al Refaie, A.; Mondillo, C.; Manasse, G.; Versienti, A.; Tomai Pitinca, M.D.; Conticini, E.; Frediani, B.; Gonnelli, S. The Advantages of Radiofrequency Echographic MultiSpectrometry in the Evaluation of Bone Mineral Density in a Population with Osteoarthritis at the Lumbar Spine. Diagnostics 2024, 14, 523. https://doi.org/10.3390/diagnostics14050523
Caffarelli C, Al Refaie A, Mondillo C, Manasse G, Versienti A, Tomai Pitinca MD, Conticini E, Frediani B, Gonnelli S. The Advantages of Radiofrequency Echographic MultiSpectrometry in the Evaluation of Bone Mineral Density in a Population with Osteoarthritis at the Lumbar Spine. Diagnostics. 2024; 14(5):523. https://doi.org/10.3390/diagnostics14050523
Chicago/Turabian StyleCaffarelli, Carla, Antonella Al Refaie, Caterina Mondillo, Giuditta Manasse, Alessandro Versienti, Maria Dea Tomai Pitinca, Edoardo Conticini, Bruno Frediani, and Stefano Gonnelli. 2024. "The Advantages of Radiofrequency Echographic MultiSpectrometry in the Evaluation of Bone Mineral Density in a Population with Osteoarthritis at the Lumbar Spine" Diagnostics 14, no. 5: 523. https://doi.org/10.3390/diagnostics14050523
APA StyleCaffarelli, C., Al Refaie, A., Mondillo, C., Manasse, G., Versienti, A., Tomai Pitinca, M. D., Conticini, E., Frediani, B., & Gonnelli, S. (2024). The Advantages of Radiofrequency Echographic MultiSpectrometry in the Evaluation of Bone Mineral Density in a Population with Osteoarthritis at the Lumbar Spine. Diagnostics, 14(5), 523. https://doi.org/10.3390/diagnostics14050523