
Agreement between Fetal Brain Ultrasonography and Magnetic Resonance Imaging in the Measurements of the Corpus Callosum and Transverse Cerebellar Diameter


Abstract
1. Introduction
2. Materials and Methods
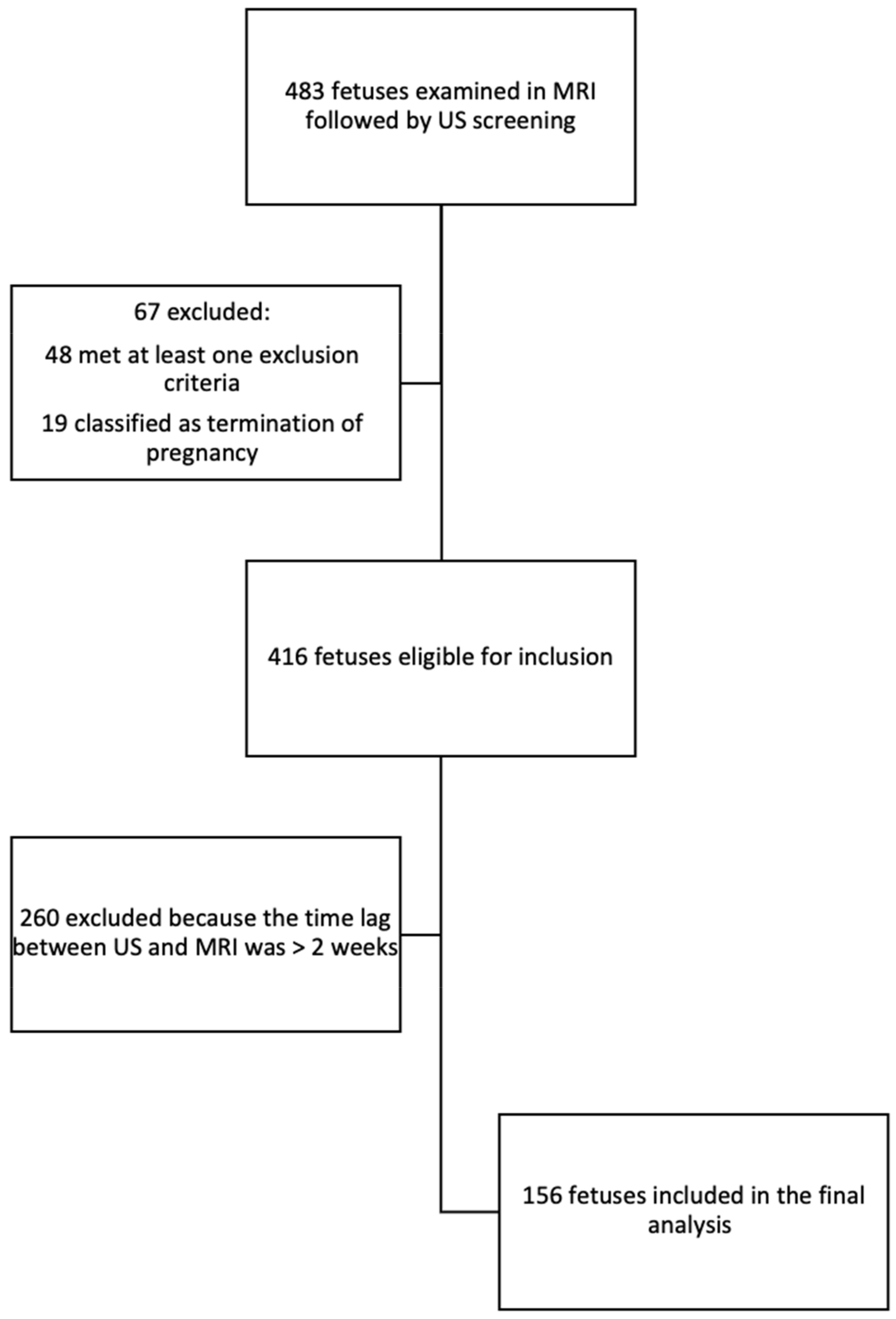
2.1. Study Design
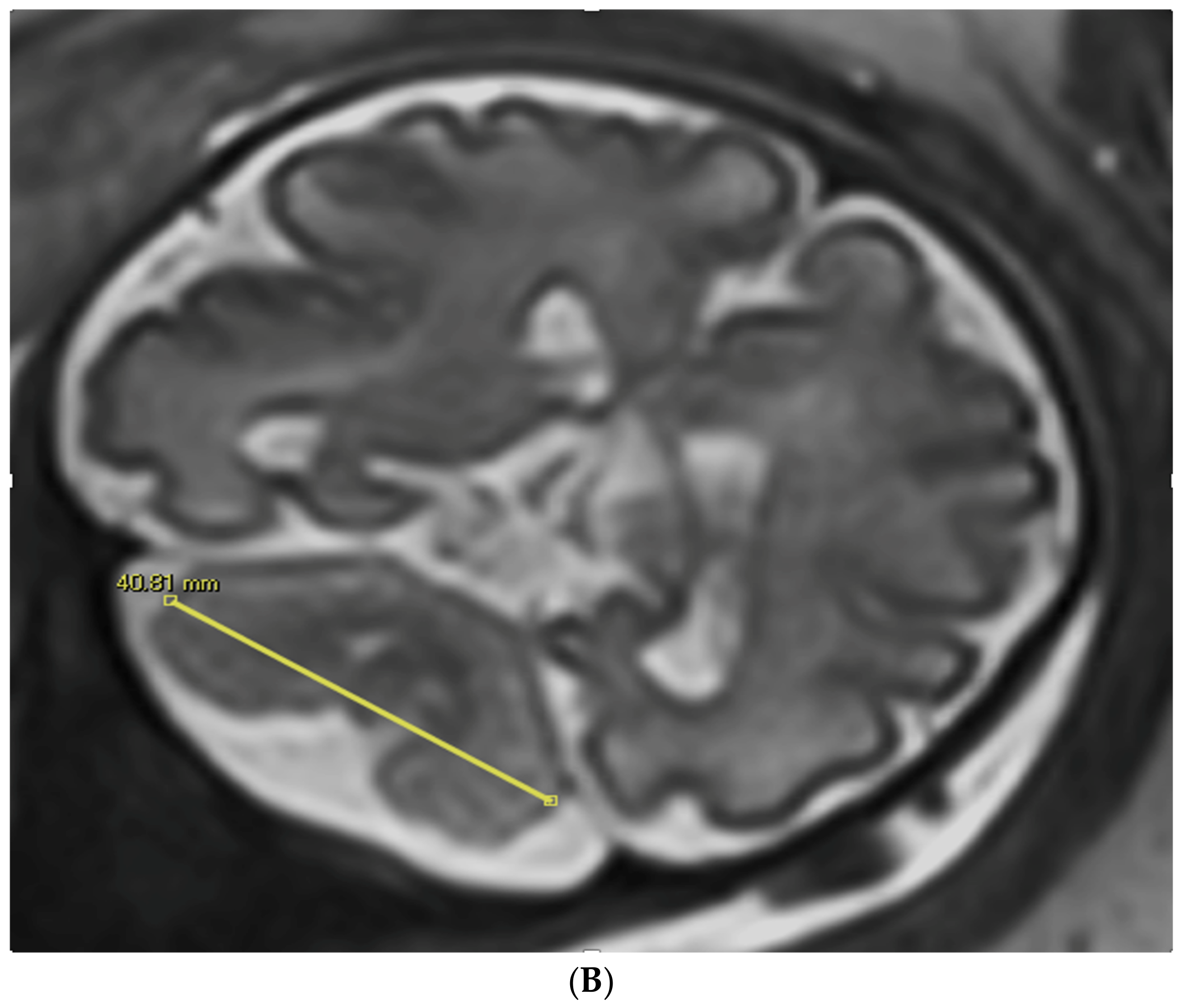
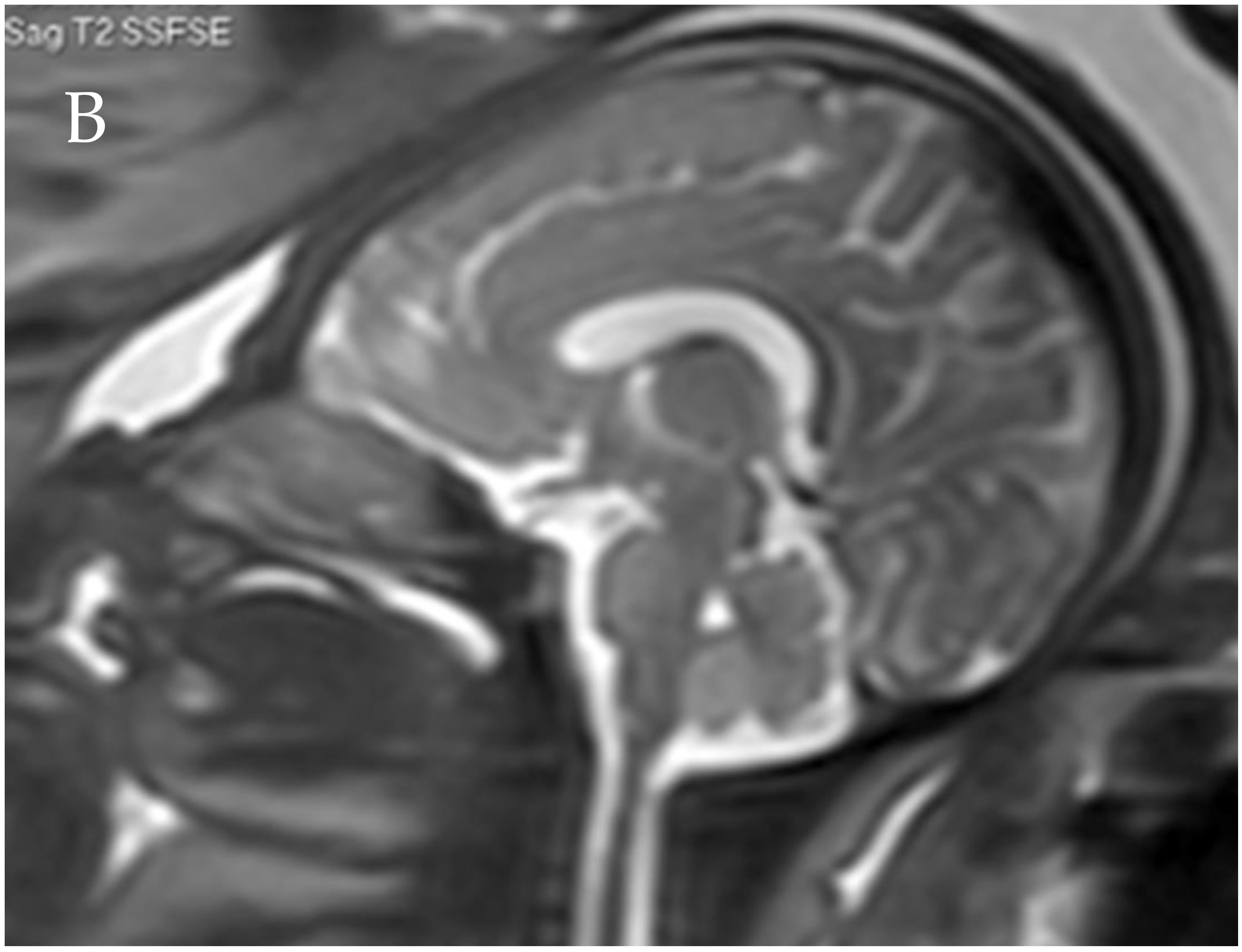
2.2. MR Imaging Scans
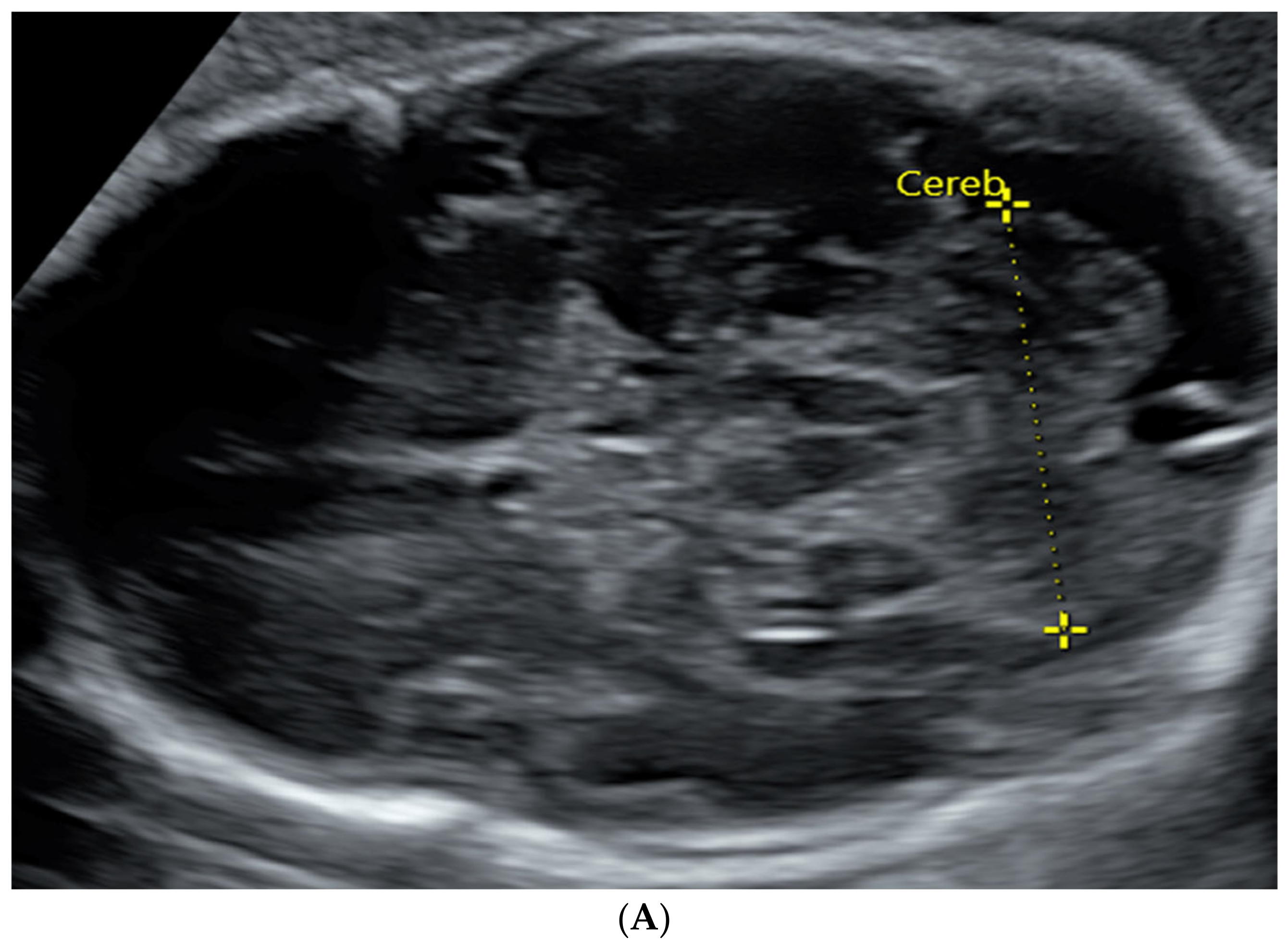
2.3. Ultrasound Scans
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Study Population
3.2. Correlation Assessment of MRI and US Measurements
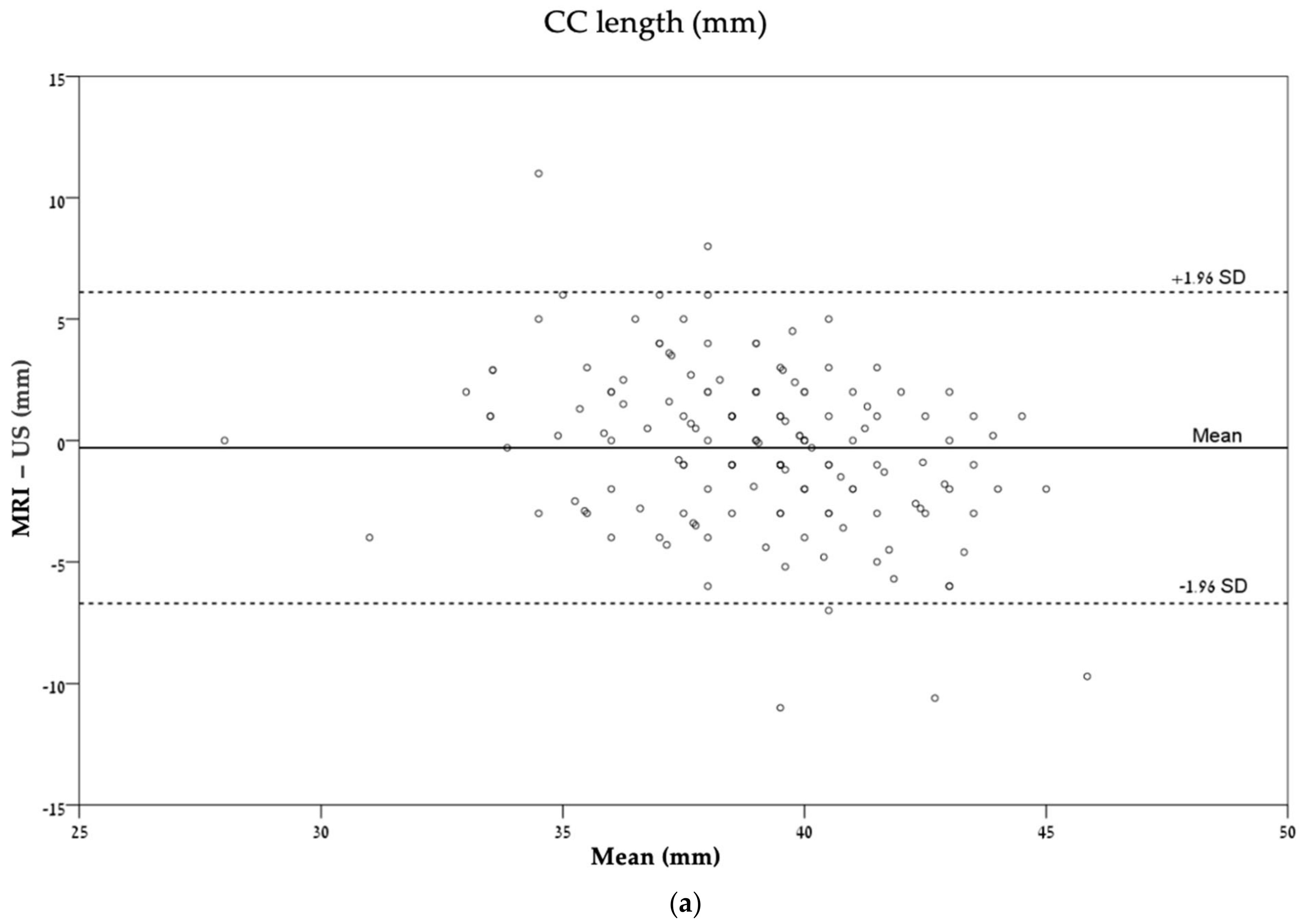
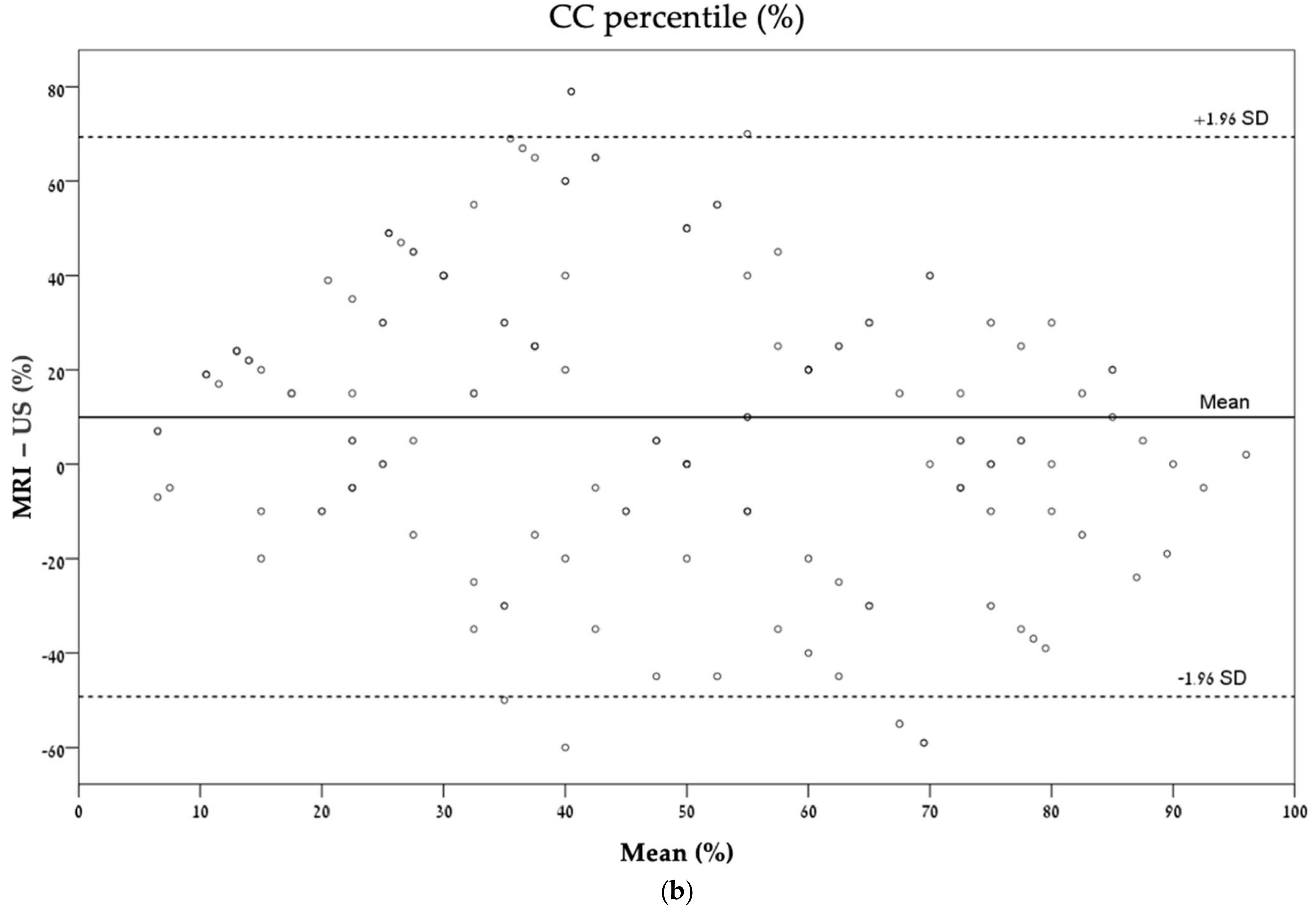
3.3. Agreement Estimation between MRI and Ultrasonography
4. Discussion
4.1. Key Results
4.2. Interpretation and Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salomon, L.J.; Garel, C. Magnetic resonance imaging examination of the fetal brain. Ultrasound Obstet. Gynecol. 2007, 30, 1019–1032. [Google Scholar] [CrossRef]
- Girard, N.; Ozanne, A.; Chaumoitre, K.; Sigaudy, S.; Gire, C.; Dubuc, M.; Porcu, G.; D’Ercole, C.; Millet, V.; Potier, A.; et al. MRI and in utero ventriculomegaly. J. Radiol. 2003, 8, 1933–1944. [Google Scholar]
- Masselli, G.; Vaccaro Notte, M.R.; Zacharzewska-Gondek, A.; Laghi, F.; Manganaro, L.; Brunelli, R. Fetal MRI of CNS abnormalities. Clin. Radiol. 2020, 75, 640.e1–640.e11. [Google Scholar] [CrossRef] [PubMed]
- International Society of Ultrasound in Obstetrics and Gynecology Education Committee. Sonographic examination of the fetal central nervous system: Guidelines for performing the ‘basic examination’ and the ‘fetal neurosonogram’. Ultrasound Obstet. Gynecol. 2007, 29, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Cignini, P.; Padula, F.; Giorlandino, M.; Brutti, P.; Alfò, M.; Giannarelli, D.; Mastrandrea, M.L.; D’Emidio, L.; Vacca, L.; Aloisi, A.; et al. Reference Charts for Fetal Corpus Callosum Length. J. Ultrasound Med. 2014, 33, 1065–1078. [Google Scholar] [CrossRef] [PubMed]
- Hiersch, L.; Melamed, N. Fetal growth velocity and body proportion in the assessment of growth. Am. J. Obstet. Gynecol. 2018, 218, S700–S711. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.M.; Marchese, S.; Peterson, C.; Fries, J. The effect of trisomy 18 on transverse cerebellar diameter. Am. J. Obstet. Gynecol. 1991, 165, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Cotes, C.; Bonfante, E.; Lazor, J.; Jadhav, S.; Caldas, M.; Swischuk, L.; Riascos, R. Congenital basis of posterior fossa anomalies. Neuroradiol. J. 2015, 28, 238–253. [Google Scholar] [CrossRef]
- Manganaro, L.; Bernardo, S.; Antonelli, A.; Vinci, V.; Saldari, M.; Catalano, C. Fetal MRI of the central nervous system: State-of-the-art. Eur. J. Radiol. 2017, 93, 273–283. [Google Scholar] [CrossRef]
- Ruland, A.M.; Berg, C.; Gembruch, U. Prenatal diagnosis of anomalies of the corpus callosum over a 13-year period. Ultraschall Med. 2015, 37, 598–603. [Google Scholar] [CrossRef]
- Blondiaux, E.; Garel, C. Fetal cerebral imaging—Ultrasound vs. MRI: An update. Acta Radiol. 2013, 54, 1046–1054. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.D.; Bradburn, M.; Campbell, M.J.; Cooper, C.L.; Embleton, N.; Graham, R.; Hart, A.R.; Jarvis, D.; Kilby, M.D.; Lie, M.; et al. MRI in the diagnosis of fetal developmental brain abnormalities: The MERIDIAN diagnostic accuracy study. Health Technol. Assess. 2019, 23, 1–144. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S.; Shashar, D.; Hoffmann, C.; Yosef, O.B.; Achiron, R.; Katorza, E. Prenatal diagnosis of fetal ventriculomegaly: Agreement between fetal brain ultrasonography and MR imaging. Am. J. Neuroradiol. 2014, 35, 1214–1218. [Google Scholar] [CrossRef] [PubMed]
- Corroenne, R.; Grevent, D.; Kasprian, G.; Stirnemann, J.; Ville, Y.; Mahallati, H.; Salomon, L.J. Corpus callosal reference ranges: Systemic review of methodology of biometric chart construction and measurements obtained. Ultrasound Obstet. Gynecol. 2023, 62, 175–184. [Google Scholar] [CrossRef]
- Resta, M.; Greco, P.; D’Addario, V.; Florio, C.; Dardes, N.; Caruso, G.; Spagnolo, P.; Clemente, R.; Vimercati, A.; Selvaggi, L. Magnetic resonance imaging in pregnancy: Study of fetal cerebral malformations. Ultrasound Obstet. Gynecol. 1994, 4, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Garel, C. Fetal cerebral biometry: Normal parenchymal findings and ventricular size. Eur. Radiol. 2005, 15, 809–813. [Google Scholar] [CrossRef] [PubMed]
- Tilea, B.; Alberti, C.; Adamsbaum, C.; Armoogum, P.; Oury, J.F.; Cabrol, D.; Sebag, G.; Kalifa, G.; Garel, C. Cerebral biometry in fetal magnetic resonance imaging: New reference data. Ultrasound Obstet. Gynecol. 2009, 33, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.M.; Guzick, D.; Fries, J.; Hixson, J.; Rivello, D. The transverse cerebellar diameter in estimating gestational age in the large- for-gestational-age fetus. Obstet. Gynecol. 1990, 75, 981–985. [Google Scholar]
- Gafner, M.; Kedar Sade, E.; Barzilay, E.; Katorza, E. Sexual dimorphism of the fetal brain biometry: An MRI-based study. Arch. Gynecol. Obstet. 2023, 308, 1257–1262. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Glenn, O.A. MR imaging of the fetal brain. Pediatr. Radiol. 2009, 40, 68–81. [Google Scholar] [CrossRef]
- Levine, D.; Barnes, P.D.; Robertson, R.R.; Wong, G.; Mehta, T.S. Fast MR imaging of fetal central nervous system abnormalities. Radiology 2003, 229, 51–61. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Percent (%) | |
|---|---|---|
| Gender | ||
| Female | 58 | 37.2 |
| Male | 98 | 62.8 |
| Presentation | ||
| Head | 140 | 89.7 |
| Breech | 13 | 8.1 |
| Transverse | 3 | 1.9 |
| Indication | ||
| Ventricular asymmetry | 94 | 60.3 |
| Cystic lesions | 12 | 7.7 |
| Genetic findings | 8 | 5.1 |
| CMV seroconversion | 8 | 5.1 |
| History of CNS illness | 9 | 5.8 |
| Other CNS findings | 19 | 12.2 |
| Miscellaneous | 6 | 3.8 |
| Ultrasound Mean ± SD | MRI Mean ± SD | Absolute Differences in Measurements Mean ± SD | Significance | Correlation (r) | p-Value | |
|---|---|---|---|---|---|---|
| CC length (mm) | 39.15 ± 3.67 | 38.85 ± 2.76 | −0.29 ± 3.28 | 0.27 | 0.51 | <0.001 |
| CC percentile (%) | 42.35 ± 30.22 | 52.31 ± 24.31 | 9.96 ± 30.35 | <0.001 | 0.39 | <0.001 |
| TCD (mm) | 41.70 ± 4.56 | 41.68 ± 3.53 | −0.02 ± 2.85 | 0.92 | 0.78 | <0.001 |
| TCD percentile (%) | 58.76 ± 23.74 | 55.30 ± 21.82 | −3.46 ± 24.03 | 0.07 | 0.45 | <0.001 |
| ICC | 95% CI | Significance | |
|---|---|---|---|
| CC length (mm) | 0.49 | 0.36–0.60 | <0.001 |
| CC percentile (%) | 0.36 | 0.21–0.49 | <0.001 |
| TCD (mm) | 0.76 | 0.68–0.82 | <0.001 |
| TCD percentile (%) | 0.44 | 0.31–0.56 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bookstein, S.; Nachmias, N.; Katorza, E. Agreement between Fetal Brain Ultrasonography and Magnetic Resonance Imaging in the Measurements of the Corpus Callosum and Transverse Cerebellar Diameter. Diagnostics 2024, 14, 366. https://doi.org/10.3390/diagnostics14040366
Bookstein S, Nachmias N, Katorza E. Agreement between Fetal Brain Ultrasonography and Magnetic Resonance Imaging in the Measurements of the Corpus Callosum and Transverse Cerebellar Diameter. Diagnostics. 2024; 14(4):366. https://doi.org/10.3390/diagnostics14040366
Chicago/Turabian StyleBookstein, Shai, Noy Nachmias, and Eldad Katorza. 2024. "Agreement between Fetal Brain Ultrasonography and Magnetic Resonance Imaging in the Measurements of the Corpus Callosum and Transverse Cerebellar Diameter" Diagnostics 14, no. 4: 366. https://doi.org/10.3390/diagnostics14040366
APA StyleBookstein, S., Nachmias, N., & Katorza, E. (2024). Agreement between Fetal Brain Ultrasonography and Magnetic Resonance Imaging in the Measurements of the Corpus Callosum and Transverse Cerebellar Diameter. Diagnostics, 14(4), 366. https://doi.org/10.3390/diagnostics14040366