
Use of Diode Laser in Hysteroscopy for the Management of Intrauterine Pathology: A Systematic Review

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  , , ,
, , ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
1.1. Background
1.2. Objectives
2. Methods
2.1. Eligibility Criteria
2.2. Information Sources
2.3. Search Strategy
2.4. Study Selection
2.5. Data Extraction
2.6. Assessment of Risk of Bias
2.7. Outcome Measures and Data Synthesis
- “Efficacy”: efficacy was measured by the success rate of the procedures, as determined by the absence of residual lesions at the end of the procedure and/or at the follow-up visit.
- “Feasibility”: feasibility was assessed as the rate of procedures completed in a single surgical step, without interruptions due to surgical problems or patient complaints.
- “Safety”: safety was determined by the rate of intraoperative and postoperative complications.
3. Results
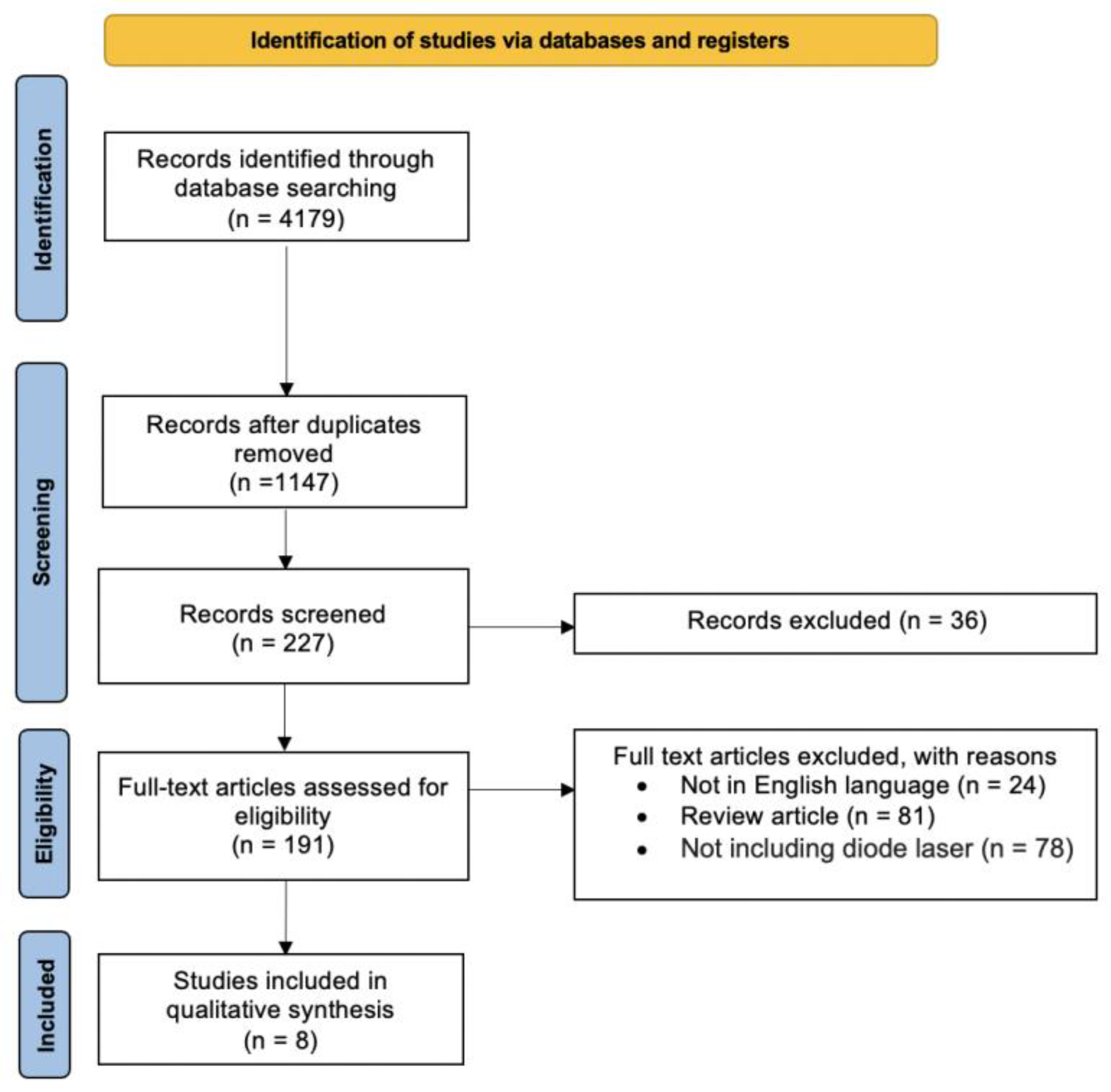
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias of Included Studies
3.4. Synthesis of the Results
3.4.1. Female Genital Tract Anomalies
3.4.2. Uterine Leiomyomas
3.4.3. Endometrial Polyps
3.4.4. Cesarean Scar Pregnancy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raz, N.; Feinmesser, L.; Moore, O.; Haimovich, S. Endometrial Polyps: Diagnosis and Treatment Options–a Review of Literature. Minim. Invasive Ther. Allied Technol. 2021, 30, 278–287. [Google Scholar] [CrossRef]
- Krispin, E.; Nassr, A.A.; Espinoza, J.; Donepudi, R.; Sun, R.C.; Sanz-Cortes, M.; Mostafaei, S.; Belfort, M.A.; Shamshirsaz, A.A. Outcomes of Laparoscopy-Assisted Fetoscopic Laser Photocoagulation for Twin-Twin Transfusion Syndrome: An Established Alternative for Inaccessible Anterior Placenta. Prenat. Diagn. 2021, 41, 1582–1588. [Google Scholar] [CrossRef]
- Adamyan, L.; Kasyan, V.; Pivazyan, L.; Isaeva, S.; Avetisyan, J. Laser Vaporization Compared with Other Surgical Techniques in Women with Ovarian Endometrioma: A Systematic Review and Meta-Analysis. Arch. Gynecol. Obstet. 2023, 308, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Mosseri, J.; Hocquemiller, R.; Mergui, J.-L.; Uzan, C.; Canlorbe, G. Laser Conization for Cervical Intraepithelial Neoplasia: Effectiveness and Obstetric Outcomes. J. Gynecol. Obstet. Hum. Reprod. 2022, 51, 102341. [Google Scholar] [CrossRef] [PubMed]
- ESGE Special Interest Group ‘Innovations’ Working Group. Lasers in Gynaecology–Are They Still Obsolete? Review of Past, Present and Future Applications. Facts Views Vis. Obgyn 2020, 12, 63–66. [Google Scholar]
- Law, K.S.K.; Abbott, J.A.; Lyons, S.D. Energy Sources for Gynecologic Laparoscopic Surgery: A Review of the Literature. Obstet. Gynecol. Surv. 2014, 69, 763–776. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.; Baik, G.H.; Ko, W.J.; Ko, B.M.; Kim, S.H.; Jang, J.S.; Jang, J.-Y.; Lee, W.-S.; Cho, Y.K.; Lim, S.G.; et al. Diode Laser-Can It Replace the Electrical Current Used in Endoscopic Submucosal Dissection? Clin. Endosc. 2021, 54, 555–562. [Google Scholar] [CrossRef]
- Nappi, L.; Sorrentino, F.; Angioni, S.; Pontis, A.; Greco, P. The Use of Laser in Hysteroscopic Surgery. Minerva Ginecol. 2016, 68, 722–726. [Google Scholar]
- Lara-Domínguez, M.D.; Arjona-Berral, J.E.; Dios-Palomares, R.; Castelo-Branco, C. Outpatient Hysteroscopic Polypectomy: Bipolar Energy System (Versapoint®) versus Diode Laser–Randomized Clinical Trial. Gynecol. Endocrinol. 2016, 32, 196–200. [Google Scholar] [CrossRef]
- Esteban Manchado, B.; Lopez-Yarto, M.; Fernandez-Parra, J.; Rodriguez-Oliver, A.; Gonzalez-Paredes, A.; Laganà, A.S.; Garzon, S.; Haimovich, S. Office Hysteroscopic Metroplasty with Diode Laser for Septate Uterus: A Multicenter Cohort Study. Minim. Invasive Ther. Allied Technol. 2022, 31, 441–447. [Google Scholar] [CrossRef]
- Bilgory, A.; Shalom-Paz, E.; Atzmon, Y.; Aslih, N.; Shibli, Y.; Estrada, D.; Haimovich, S. Diode Laser Hysteroscopic Metroplasty for Dysmorphic Uterus: A Pilot Study. Reprod. Sci. 2022, 29, 506–512. [Google Scholar] [CrossRef]
- Żywicka, B.; Rybak, Z.; Janeczek, M.; Czerski, A.; Bujok, J.; Szymonowicz, M.; Dobrzyński, M.; Korczyński, M.; Świderski, J. Comparison of A 1940 Nm Thulium-Doped Fiber Laser and A 1470 Nm Diode Laser for Cutting Efficacy and Hemostasis in A Pig Model of Spleen Surgery. Materials 2020, 13, 1167. [Google Scholar] [CrossRef]
- Bakour, S.H.; Jones, S.E.; O’Donovan, P. Ambulatory Hysteroscopy: Evidence-Based Guide to Diagnosis and Therapy. Best Pract. Res. Clin. Obstet. Gynaecol. 2006, 20, 953–975. [Google Scholar] [CrossRef]
- Revel, A.; Shushan, A. Investigation of the Infertile Couple: Hysteroscopy with Endometrial Biopsy Is the Gold Standard Investigation for Abnormal Uterine Bleeding. Hum. Reprod. 2002, 17, 1947–1949. [Google Scholar] [CrossRef] [PubMed]
- Tanos, V.; Berry, K.E.; Seikkula, J.; Abi Raad, E.; Stavroulis, A.; Sleiman, Z.; Campo, R.; Gordts, S. The Management of Polyps in Female Reproductive Organs. Int. J. Surg. 2017, 43, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Loddo, A.; Djokovic, D.; Drizi, A.; De Vree, B.P.; Sedrati, A.; van Herendael, B.J. Hysteroscopic Myomectomy: The Guidelines of the International Society for Gynecologic Endoscopy (ISGE). Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 268, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Practice Committee of the American Society for Reproductive Medicine Uterine Septum: A Guideline. Fertil. Steril. 2016, 106, 530–540. [Google Scholar] [CrossRef]
- Capmas, P.; Pourcelot, A.-G.; Giral, E.; Fedida, D.; Fernandez, H. Office Hysteroscopy: A Report of 2402 Cases. J. Gynecol. Obstet. Biol. Reprod. 2016, 45, 445–450. [Google Scholar] [CrossRef]
- Salazar, C.A.; Isaacson, K.B. Office Operative Hysteroscopy: An Update. J. Minim. Invasive Gynecol. 2018, 25, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Di Spiezio Sardo, A.; Giampaolino, P.; Manzi, A.; De Angelis, M.C.; Zizolfi, B.; Alonso, L.; Carugno, J. The Invisible External Cervical Os. Tips and Tricks to Overcome This Challenge during In-Office Hysteroscopy. J. Minim. Invasive Gynecol. 2021, 28, 172–173. [Google Scholar] [CrossRef]
- Wortman, M. “See-and-Treat” Hysteroscopy in the Management of Endometrial Polyps. Surg. Technol. Int. 2016, 28, 177–184. [Google Scholar] [PubMed]
- Gulumser, C.; Narvekar, N.; Pathak, M.; Palmer, E.; Parker, S.; Saridogan, E. See-and-Treat Outpatient Hysteroscopy: An Analysis of 1109 Examinations. Reprod. Biomed. Online 2010, 20, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Gambadauro, P.; Martínez-Maestre, M.A.; Torrejón, R. When Is See-and-Treat Hysteroscopic Polypectomy Successful? Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 178, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Saridogan, E.; Tilden, D.; Sykes, D.; Davis, N.; Subramanian, D. Cost-Analysis Comparison of Outpatient See-and-Treat Hysteroscopy Service with Other Hysteroscopy Service Models. J. Minim. Invasive Gynecol. 2010, 17, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Neveu, M.-E.; Debras, E.; Niro, J.; Fernandez, H.; Panel, P. Standardizing Hysteroscopy Teaching: Development of a Curriculum Using the Delphi Method. Surg. Endosc. 2017, 31, 5389–5398. [Google Scholar] [CrossRef]
- Vilà Famada, A.; Cos Plans, R.; Costa Canals, L.; Rojas Torrijos, M.; Rodríguez Vicente, A.; Bainac Albadalejo, A. Outcomes of Surgical Hysteroscopy: 25 Years of Observational Study. J. Obstet. Gynaecol. 2022, 42, 1365–1369. [Google Scholar] [CrossRef]
- Donnez, J.; Gillerot, S.; Bourgonjon, D.; Clerckx, F.; Nisolle, M. Neodymium: YAG Laser Hysteroscopy in Large Submucous Fibroids. Fertil. Steril. 1990, 54, 999–1003. [Google Scholar] [CrossRef]
- Choe, J.K.; Baggish, M.S. Hysteroscopic Treatment of Septate Uterus with Neodymium-YAG Laser. Fertil. Steril. 1992, 57, 81–84. [Google Scholar] [CrossRef]
- Jourdain, O.; Dabysing, F.; Harle, T.; Lajus, C.; Roux, D.; Dallay, D. Management of Septate Uterus by Flexible Hysteroscopy and Nd:YAG Laser. Int. J. Gynaecol. Obstet. 1998, 63, 159–162. [Google Scholar] [CrossRef]
- Köchli, O.R. Endometrial Ablation in the Year 2000–Do We Have More Methods than Indications? Contrib. Gynecol. Obstet. 2000, 20, 91–120. [Google Scholar] [CrossRef] [PubMed]
- Chapman, R. New Therapeutic Technique for Treatment of Uterine Leiomyomas Using Laser-Induced Interstitial Thermotherapy (LITT) by a Minimally Invasive Method. Lasers Surg. Med. 1998, 22, 171–178. [Google Scholar] [CrossRef]
- Fedele, L.; Arcaini, L.; Parazzini, F.; Vercellini, P.; Di Nola, G. Reproductive Prognosis after Hysteroscopic Metroplasty in 102 Women: Life-Table Analysis. Fertil. Steril. 1993, 59, 768–772. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; Mikuš, M.; De Angelis, M.C.; Carugno, J.; Riemma, G.; Franušić, L.; Cerovac, A.; D’alterio, M.N.; Nappi, L.; Angioni, S. Diode Laser Use in Hysteroscopic Surgery: Current Status and Future Perspectives. Minim. Invasive Ther. Allied Technol. 2023, 32, 275–284. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated Guidance for Trusted Systematic Reviews: A New Edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, ED000142. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical Evaluation of the Newcastle-Ottawa Scale for the Assessment of the Quality of Nonrandomized Studies in Meta-Analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Home–2020. Available online: https://www.cebm.net/ (accessed on 5 October 2023).
- Haimovich, S.; Mancebo, G.; Alameda, F.; Agramunt, S.; Solé-Sedeno, J.M.; Hernández, J.L.; Carreras, R. Feasibility of a New Two-Step Procedure for Office Hysteroscopic Resection of Submucous Myomas: Results of a Pilot Study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 168, 191–194. [Google Scholar] [CrossRef]
- Nappi, L.; Pontis, A.; Sorrentino, F.; Greco, P.; Angioni, S. Hysteroscopic Metroplasty for the Septate Uterus with Diode Laser: A Pilot Study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 206, 32–35. [Google Scholar] [CrossRef]
- Nappi, L.; Sorrentino, F.; Angioni, S.; Pontis, A.; Litta, P.; Greco, P. Feasibility of Hysteroscopic Endometrial Polypectomy Using a New Dual Wavelengths Laser System (DWLS): Preliminary Results of a Pilot Study. Arch. Gynecol. Obstet. 2017, 295, 3–7. [Google Scholar] [CrossRef]
- Sorrentino, F.; De Feo, V.; Stabile, G.; Tinelli, R.; D’Alterio, M.N.; Ricci, G.; Angioni, S.; Nappi, L. Cesarean Scar Pregnancy Treated by Artery Embolization Combined with Diode Laser: A Novel Approach for a Rare Disease. Medicina 2021, 57, 411. [Google Scholar] [CrossRef]
- Vitale, S.G.; Moore, O.; Riemma, G.; Carugno, J.; Yarto, M.L.; Haimovich, S. Hysteroscopic Laser Ablation of Symptomatic Uterine Fibroids: Insights from a Prospective Study. Climacteric 2023, 26, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.Y.; Jayaprakasan, K.; Zamora, J.; Thornton, J.G.; Raine-Fenning, N.; Coomarasamy, A. The Prevalence of Congenital Uterine Anomalies in Unselected and High-Risk Populations: A Systematic Review. Hum. Reprod. Update 2011, 17, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Abrao, M.S.; Muzii, L.; Marana, R. Anatomical Causes of Female Infertility and Their Management. Int. J. Gynaecol. Obstet. 2013, 123 (Suppl. S2), S18–S24. [Google Scholar] [CrossRef]
- Brucker, S.Y.; Rall, K.; Campo, R.; Oppelt, P.; Isaacson, K. Treatment of Congenital Malformations. Semin. Reprod. Med. 2011, 29, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Adhesions, A.D. The American Fertility Society Classifications of Adnexal Adhesions, Distal Tubal Occlusion, Tubal Occlusion Secondary to Tubal Ligation, Tubal Pregnancies, Müllerian Anomalies and Intrauterine Adhesions. Fertil. Steril. 1988, 49, 944–955. [Google Scholar] [CrossRef]
- Grimbizis, G.F.; Gordts, S.; Di Spiezio Sardo, A.; Brucker, S.; De Angelis, C.; Gergolet, M.; Li, T.-C.; Tanos, V.; Brölmann, H.; Gianaroli, L.; et al. The ESHRE/ESGE Consensus on the Classification of Female Genital Tract Congenital Anomalies. Hum. Reprod. 2013, 28, 2032–2044. [Google Scholar] [CrossRef] [PubMed]
- Alonso Pacheco, L.; Laganà, A.S.; Ghezzi, F.; Haimovich, S.; Azumendi Gómez, P.; Carugno, J. Subtypes of T-Shaped Uterus. Fertil. Steril. 2019, 112, 399–400. [Google Scholar] [CrossRef]
- Stewart, E.A. Uterine Fibroids. Lancet 2001, 357, 293–298. [Google Scholar] [CrossRef]
- Parker, W.H. Etiology, Symptomatology, and Diagnosis of Uterine Myomas. Fertil. Steril. 2007, 87, 725–736. [Google Scholar] [CrossRef]
- Lethaby, A.; Vollenhoven, B. Fibroids (Uterine Myomatosis, Leiomyomas). BMJ Clin. Evid. 2015, 2015, 0814. [Google Scholar]
- Bachmann, G.A.; Bahouth, L.A.; Amalraj, P.; Mhamunkar, V.; Hoes, K.; Ananth, C.V. Uterine Fibroids: Correlations of Anemia and Pain to Fibroid Location and Uterine Weight. J. Reprod. Med. 2011, 56, 463–466. [Google Scholar]
- Lasmar, R.B.; Barrozo, P.R.M.; Dias, R.; Oliveira, M.A.P. de Submucous Myomas: A New Presurgical Classification to Evaluate the Viability of Hysteroscopic Surgical Treatment--Preliminary Report. J. Minim. Invasive Gynecol. 2005, 12, 308–311. [Google Scholar] [CrossRef]
- Cicinelli, E.; Mitsopoulos, V.; Fascilla, F.D.; Sioutis, D.; Bettocchi, S. The OPPIuM Technique: Office Hysteroscopic Technique for the Preparation of Partially Intramural Leiomyomas. Minerva Ginecol. 2016, 68, 328–333. [Google Scholar] [PubMed]
- Munro, M.G.; Critchley, H.O.D.; Broder, M.S.; Fraser, I.S. FIGO Working Group on Menstrual Disorders FIGO Classification System (PALM-COEIN) for Causes of Abnormal Uterine Bleeding in Nongravid Women of Reproductive Age. Int. J. Gynaecol. Obstet. 2011, 113, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J. Endometrial Polyps. Am. J. Obstet. Gynecol. 2022, 226, 734–735. [Google Scholar] [CrossRef] [PubMed]
- Munro, M.G. Uterine Polyps, Adenomyosis, Leiomyomas, and Endometrial Receptivity. Fertil. Steril. 2019, 111, 629–640. [Google Scholar] [CrossRef]
- Rackow, B.W.; Jorgensen, E.; Taylor, H.S. Endometrial Polyps Affect Uterine Receptivity. Fertil. Steril. 2011, 95, 2690–2692. [Google Scholar] [CrossRef] [PubMed]
- Bowman, Z.S.; Smith, K.R.; Silver, R.M. Cesarean Delivery and Risk for Subsequent Ectopic Pregnancy. Am. J. Perinatol. 2015, 32, 815–820. [Google Scholar] [CrossRef]
- Po, L.; Thomas, J.; Mills, K.; Zakhari, A.; Tulandi, T.; Shuman, M.; Page, A. Guideline No. 414: Management of Pregnancy of Unknown Location and Tubal and Nontubal Ectopic Pregnancies. J. Obstet. Gynaecol. Can. 2021, 43, 614–630.e1. [Google Scholar] [CrossRef]
- Wortman, M. Endometrial Ablation: Past, Present, and Future Part II. Surg. Technol. Int. 2018, 33, 161–177. [Google Scholar]
- Abi Antoun, M.; Etrusco, A.; Chiantera, V.; Laganà, A.S.; Feghali, E.; Khazzaka, A.; Stabile, G.; Della Corte, L.; Dellino, M.; Sleiman, Z. Outcomes of Conventional and Advanced Energy Devices in Laparoscopic Surgery: A Systematic Review. Minim. Invasive Ther. Allied Technol. 2024, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chene, G.; Chauvy, L.; Buenerd, A.; Moret, S.; Nadaud, B.; Beaufils, E.; Le Bail-Carval, K.; Chabert, P.; Mellier, G.; Lamblin, G. In Vivo Confocal Laser Endomicroscopy during Laparoscopy for Gynecological Surgery: A Promising Tool. J. Gynecol. Obstet. Hum. Reprod. 2017, 46, 565–569. [Google Scholar] [CrossRef]
- Donnez, J.; Squifflet, J.; Polet, R.; Nisolle, M. Laparoscopic Myolysis. Hum. Reprod. Update 2000, 6, 609–613. [Google Scholar] [CrossRef] [PubMed]
- Mairos, J.; Di Martino, P. Office Hysteroscopy. An Operative Gold Standard Technique and an Important Contribution to Patient Safety. Gynecol. Surg. 2016, 13, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.F.; Carugno, J. Hysteroscopy. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Ahmad, G.; Saluja, S.; O’Flynn, H.; Sorrentino, A.; Leach, D.; Watson, A. Pain Relief for Outpatient Hysteroscopy. Cochrane Database Syst. Rev. 2017, CD007710. [Google Scholar] [CrossRef]
- Hadisaputra, W.; Hani, C.A.S.; Putri, N.A. Patient Safety in Hysteroscopic Procedure. Gynecol. Minim. Invasive Ther. 2022, 11, 145–149. [Google Scholar] [CrossRef]
- Garuti, G.; Cellani, F.; Colonnelli, M.; Grossi, F.; Luerti, M. Outpatient Hysteroscopic Polypectomy in 237 Patients: Feasibility of a One-Stop “See-and-Treat” Procedure. J. Am. Assoc. Gynecol. Laparosc. 2004, 11, 500–504. [Google Scholar] [CrossRef]
- Gambadauro, P.; Milenkovic, M.; Hadlaczky, G. Simulation for Training and Assessment in Hysteroscopy: A Systematic Review. J. Minim. Invasive Gynecol. 2018, 25, 963–973. [Google Scholar] [CrossRef]
- Chatzipapas, I.; Kathopoulis, N.; Protopapas, A.; Loutradis, D. Hysteroscopy for Training Residents Using Uterine Post-Hysterectomy Specimens with a Mobile Hysteroscope. Facts Views Vis. Obgyn 2020, 12, 43–46. [Google Scholar]
- Michel, L.; Chudnoff, S. Gynecology Resident Experience with Office Hysteroscopy Training. JSLS 2023, 27, e2023.00009. [Google Scholar] [CrossRef]
- Mazzon, I.; Etrusco, A.; Laganà, A.S.; Chiantera, V.; Di Angelo Antonio, S.; Tosto, V.; Gerli, S.; Favilli, A. Training in Diagnostic Hysteroscopy: The “Arbor Vitae” Method. Medicina 2023, 59, 1019. [Google Scholar] [CrossRef]
- Munro, M.G.; Critchley, H.O.D.; Fraser, I.S. FIGO Menstrual Disorders Committee The Two FIGO Systems for Normal and Abnormal Uterine Bleeding Symptoms and Classification of Causes of Abnormal Uterine Bleeding in the Reproductive Years: 2018 Revisions. Int. J. Gynaecol. Obstet. 2018, 143, 393–408. [Google Scholar] [CrossRef]
- Etrusco, A.; Laganà, A.S.; Chiantera, V.; Vitagliano, A.; Cicinelli, E.; Mikuš, M.; Šprem Goldštajn, M.; Ferrari, F.; Uccella, S.; Garzon, S.; et al. Feasibility and Surgical Outcomes of Hysteroscopic Myomectomy of FIGO Type 3 Myoma: A Systematic Review. J. Clin. Med. 2023, 12, 4953. [Google Scholar] [CrossRef]
- Favilli, A.; Etrusco, A.; Chiantera, V.; Laganà, A.S.; Cicinelli, E.; Gerli, S.; Vitagliano, A. Impact of FIGO Type 3 Uterine Fibroids on in Vitro Fertilization Outcomes: A Systematic Review and Meta-Analysis. Int. J. Gynaecol. Obstet. 2023, 163, 528–539. [Google Scholar] [CrossRef]
- Capmas, P.; Voulgaropoulos, A.; Legendre, G.; Pourcelot, A.-G.; Fernandez, H. Hysteroscopic Resection of Type 3 Myoma: A New Challenge? Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 205, 165–169. [Google Scholar] [CrossRef]
- Favilli, A.; Mazzon, I.; Etrusco, A.; Dellino, M.; Laganà, A.S.; Tinelli, A.; Chiantera, V.; Cicinelli, E.; Gerli, S.; Vitagliano, A. The Challenge of FIGO Type 3 Leiomyomas and Infertility: Exploring Therapeutic Alternatives amidst Limited Scientific Certainties. Int. J. Gynaecol. Obstet. 2023. ahead of print. [Google Scholar] [CrossRef]
- Ahmadzade, M.; Rouientan, H.; Golzarian, J.; Akhlaghpoor, S. An Evaluation of Ultrasound-Guided Percutaneous Microwave Ablation for the Treatment of Symptomatic Uterine Fibroids. J. Vasc. Interv. Radiol. 2023, 35, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Fasciani, A.; Turtulici, G.; Pedullà, A.; Sirito, R. Uterine Myoma Position-Based Radiofrequency Ablation (UMP-b RFA): 36 Months Follow-up Clinical Outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2023, 281, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, M.Z.; Alkhorayef, M.; Alzimami, K.S.; Aljuhani, M.S.; Sulieman, A. High-Intensity Focused Ultrasound (HIFU) in Uterine Fibroid Treatment: Review Study. Pol. J. Radiol. 2014, 79, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Slotman, D.J.; Bartels, L.W.; Zijlstra, A.; Verpalen, I.M.; van Osch, J.A.C.; Nijholt, I.M.; Heijman, E.; van ’t Veer-Ten Kate, M.; de Boer, E.; van den Hoed, R.D.; et al. Diffusion-Weighted MRI with Deep Learning for Visualizing Treatment Results of MR-Guided HIFU Ablation of Uterine Fibroids. Eur. Radiol. 2023, 33, 4178–4188. [Google Scholar] [CrossRef] [PubMed]
- Casadio, P.; Gubbini, G.; Franchini, M.; Morra, C.; Talamo, M.R.; Magnarelli, G.; Paradisi, R.; Florio, P.; Seracchioli, R. Comparison of Hysteroscopic Cesarean Scar Defect Repair with 26 Fr Resectoscope and 16 Fr Mini-Resectoscope: A Prospective Pilot Study. J. Minim. Invasive Gynecol. 2021, 28, 314–319. [Google Scholar] [CrossRef]
- Papalampros, P.; Gambadauro, P.; Papadopoulos, N.; Polyzos, D.; Chapman, L.; Magos, A. The Mini-Resectoscope: A New Instrument for Office Hysteroscopic Surgery. Acta Obstet. Gynecol. Scand. 2009, 88, 227–230. [Google Scholar] [CrossRef]
- Ricciardi, R.; Lanzone, A.; Tagliaferri, V.; Di Florio, C.; Ricciardi, L.; Selvaggi, L.; Guido, M. Using a 16-French Resectoscope as an Alternative Device in the Treatment of Uterine Lesions: A Randomized Controlled Trial. Obstet. Gynecol. 2012, 120, 160–165. [Google Scholar] [CrossRef]
- Roy, K.K.; Lingampally, A.; Kansal, Y.; Bharti, J.; Kumar, S.; Vanamail, P.; Singhal, S.; Meena, J. A Pilot Study Comparing Hysteroscopic Adhesiolysis by Conventional Resectoscope Versus Mini-Resectoscope. Oman Med. J. 2017, 32, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Roy, K.K.; Anusha, S.M.; Rai, R.; Das, A.; Zangmo, R.; Singhal, S. A Prospective Randomized Comparative Clinical Trial of Hysteroscopic Septal Resection Using Conventional Resectoscope Versus Mini-Resectoscope. J. Hum. Reprod. Sci. 2021, 14, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Dealberti, D.; Riboni, F.; Prigione, S.; Pisani, C.; Rovetta, E.; Montella, F.; Garuti, G. New Mini-Resectoscope: Analysis of Preliminary Quality Results in Outpatient Hysteroscopic Polypectomy. Arch. Gynecol. Obstet. 2013, 288, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Dealberti, D.; Riboni, F.; Cosma, S.; Pisani, C.; Montella, F.; Saitta, S.; Calagna, G.; Di Spiezio Sardo, A. Feasibility and Acceptability of Office-Based Polypectomy With a 16F Mini-Resectoscope: A Multicenter Clinical Study. J. Minim. Invasive Gynecol. 2016, 23, 418–424. [Google Scholar] [CrossRef]


{kind=link}
| Author | Year | Type | Main Outcome | Country | Patient (n) | Age (Mean) | Control Group | Participant Characteristics | Intervention | Registration |
|---|---|---|---|---|---|---|---|---|---|---|
| Haimovic et al. [38] | 2013 | Pilot | To evaluate the feasibility of a new two-step technique for office hysteroscopic resection of submucous myoma | Spain | 43 | 36.7 | none | Reproductive-age patients with symptomatic lesions diagnosed sonographically as single G1 or G2 myoma ≤ 4.0 cm | Two-step hysteroscopic procedure: preparation of partially intramural myomas by incision of the endometrial mucosa and pseudocapsule covering the myoma in the first step, and excision of the myoma by diode laser 4 weeks later. | None |
| Lara-Domínguez et al. [9] | 2015 | Randomized Controlled Trial | To compare the resection of endometrial polyps using Versapoint bipolar electrode versus diode laser | Spain | 102 | 51.5 | yes | Patients with endometrial polyps, single or multiple | Hysteroscopic diode laser polypectomy | Clinical Trial ID: NCT02126397 |
| Nappi et al. [39] | 2016 | Pilot | To evaluate the feasibility and safety of office hysteroscopic metroplasty using a 980 nm diode laser | Italy | 18 | 32.7 | none | Patients with sonographically diagnosed endometrial polyps ≤ 2.5 cm | Hysteroscopic diode laser polypectomy | None |
| Nappi et al. [40] | 2016 | Pilot | To evaluate the feasibility and effectiveness of hysteroscopic endometrial polypectomy using a new dual wavelength laser system | Italy | 300 | 54 | none | Patients with V-b or Class U2a septate uterus, in according with ASRM guidelines and the ESHRE-ESGE classification | Hysteroscopic diode laser metroplasty after 14-day endometrial preparation with 5 mg per day of nomegestrol acetate | None |
| Esteban Manchado et al. [10] | 2020 | Multicenter Prospective Cohort Study | To investigate the effectiveness and safety of office hysteroscopic metroplasty by diode laser for the treatment of septate uteri | Spain | 41 | 34.2 | none | Women diagnosed with V-b or Class U2a septate uterus, in accordance with ASRM guidelines and the ESHRE-ESGE classification, and a history of primary infertility or recurrent miscarriage | Hysteroscopic diode laser metroplasty | None |
| Sorrentino et al. [41] | 2021 | Case Report | To report a case of cesarean scar pregnancy treated by combined uterine artery embolization and hysteroscopic laser surgery | Italy | 1 | 40 | none | 40-year-old woman with cesarean scar pregnancy | Angiographic uterine artery embolization followed by hysteroscopic diode laser resection | None |
| Bilgory et al. [11] | 2021 | Retrospective Cohort Study | To study the efficacy and safety of diode laser hysteroscopic metroplasty for dysmorphic uterus and the impact on reproductive outcomes | Israel | 25 | 35.4 | none | Nulliparous woman with T- or Y-shape uterus and infertility | Hysteroscopic diode laser metroplasty | None |
| Vitale et al. [42] | 2023 | Prospective Cohort Study | To evaluate the feasibility and efficacy of in-office hysteroscopic ablation of submucous uterine fibroids using diode laser | Italy | 20 | 39.1 | none | Patients with at least one symptomatic, class 0–2 FIGO classification, uterine fibroids ≤ 7 cm in size. | Laser vaporization of the fibroid core | Clinical Trial ID: NCT05604001 |
| Nappi et al. [39] | Manchado et al. [10] | Bilgory et al. [11] | |
|---|---|---|---|
| Patients (n) | 18 | 40 | 25 |
| Mean age (years) | 32.66 ± 2.74 | 34.2 ± 5.278 | 35.4 ± 5.4 |
| BMI (kg/m2) | 21.58 ± 1.63 | n.d. | 25.4 ± 5.4 |
| Symptoms | |||
| Infertility (%) | 38.9 | 37.5 | n.d. |
| RPL (%) | 61.1 | 62.5 | n.d. |
| RIF (%) | n.d. | n.d. | n.d. |
| Female genital tract anomaly | |||
| Type of uterine anomaly | Septate uterus | Septate uterus | Dysmorphic uterus (T-shape and Y-shape) |
| ASRM/ESHRE Class | Vb–U2a | Va–U2b | U1a |
| Preoperative assessment | |||
| Preoperative 3D-US (%) | 100 | 100 | 100 |
| Surgery | |||
| Mean operative time (min) | 13.16 ± 1.33 |
| 25 ± 7 |
| Surgeon (n) | 2 | n.d. | 1 |
| Mean VAS | 3.05 ± 0.72 | 2.225 ± 0.5768 (1 to 5) | n.d. |
| Intraoperative complications (n) | 0 | 0 | 0 |
| Postoperative complications (n) | 0 | 1 | 0 |
| Adhesions (n) | 0 | 1 | 0 |
| Need for a surgical second step (n) | 0 | 7 | 0 |
| Follow-up | 1 | 0 | |
| Mean follow-up time (months) | 6–30 | 24 | 11.5 ± 9.2 |
| Postoperative follow-up hysteroscopy (%) | 100 | 100 | 100 |
| Reproductive outcomes | |||
| Clinical pregnancy rate before surgery (%) | n.d. | n.d. | 33.3 |
| Clinical pregnancy rate after surgery (%) |
| 78.9 | 60 |
| Miscarriage rate before surgery (%) | n.d. | n.d. | 40 |
| Miscarriage rate after surgery (%) |
| 20 | 13.3 |
| Live birth rate before surgery (%) | n.d. | n.d. | 0 |
| Live birth rate after surgery (%) |
| 63.2 | 46.7 |
| Haimovic et al. [38] | Vitale et al. [42] | |
|---|---|---|
| Patients (n) | 43 | 20 |
| Mean age (years) | 36.7 ± 4.6 | 39.1 ± 4.7 |
| BMI (kg/m2) | n.d. | 21.4 ± 1.6 |
| Fertile age | 100 | 100 |
| Mean parity | 0.79 ± 0.94 | n.d. |
| Symptoms | ||
| Abnormal menstrual bleeding (%) | 44.2 | 90 |
| Pelvic pain (%) | 11.6 | 60 |
| Infertility (%) | 44.2 | n.d. |
| Increased urinary frequency (%) | n.d. | 30 |
| Bulking symptoms (%) | n.d. | 70 |
| Preoperative assessment | ||
| Preoperative 3D-US (%) | 100 | 100 |
| Characteristics of myomas | ||
| ESGE/FIGO class G1 (%) | 48.8 | 70 |
| ESGE/FIGO class G2 (%) | 51.2 | 30 |
| Mean size | 21.7 ± 7.3 | |
| Localization of myomas | ||
| Anterior wall | 46.5 | n.d. |
| Posterior wall | 30.2 | n.d. |
| Fundus | 16.3 | n.d. |
| Lateral walls | 7.0 | n.d. |
| Surgery | ||
| Technique used | Two-step hysteroscopic resection | Hysteroscopic laser ablation |
| Mean operative time (min) |
| n.d. |
| Surgeon (n) | 1 | 1 |
| Mean VAS |
| 2.9 ± 2.0 |
| Intraoperative complications (n) | 0 | 0 |
| Postoperative complications (n) | 0 | 0 |
| Need for a surgical second step (n) | 0 | 0 |
| Follow-up | ||
| Postoperative follow-up | n.d. | 3D-US |
| Reproductive outcomes | n.d. | n.d. |
| Lara-Domínguez et al. [9] | Nappi et al. [40] | |
|---|---|---|
| Patients (n) | 102 | 225 |
| Mean age (years) |
| 54 ± 12.6 |
| BMI (kg/m2) |
| 26.55 ± 4.23 |
| Fertile age (%) | 41.2 | 38.7 |
| Menopausal (%) | 58.8 | 61.3 |
| Mean parity |
| 2.11 ± 1.71 |
| Symptoms | ||
| Asymptomatic (%) |
| n.d. |
| Hypermenorrhea (%) |
| n.d. |
| Metrorrhagia (%) |
| n.d. |
| Preoperative assessment | ||
| Preoperative US (%) | 100 | 100 |
| Characteristics of polyps | ||
| Mean size (mm) | 21.7 ± 7.3 | n.d. |
| Size 0–1 cm (n) | n.d. | 94 |
| Size 1–2.5 cm (n) | n.d. | 131 |
| Localization of polyps (n) | 27 | |
| Anterior wall | n.d. | 63 |
| Posterior wall | n.d. | 28 |
| Fundus | n.d. | 87 |
| Lateral walls | n.d. | 3 |
| Isthmus | n.d. | 17 |
| Peri-ostial | n.d. | 27 |
| Surgery | ||
| Mean operative time (min) |
|
|
| Surgeon (n) | 2 | n.d. |
| Mean VAS |
| Women in reproductive age:
|
| Intraoperative complications (n) | 3 | 6 |
| Vagal syndrome/intolerance (n) | 3 | 6 |
| Incomplete resection of polyp |
| 0 |
| Postoperative complications (n) | 1 | 0 |
| Pelvic inflammatory disease (n) | 1 | 0 |
| Follow-up | ||
| Postoperative follow-up (%) | Hysteroscopy: 89.2% | Ultrasound: 100% |
| Polyp relapse (%) |
| 0 |
| Very satisfied with the procedure (%) |
| n.d. |
| Highly recommendable procedure (%) |
| n.d. |
| Reproductive outcomes | n.d. | n.d. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Etrusco, A.; Buzzaccarini, G.; Laganà, A.S.; Chiantera, V.; Vitale, S.G.; Angioni, S.; D’Alterio, M.N.; Nappi, L.; Sorrentino, F.; Vitagliano, A.; et al. Use of Diode Laser in Hysteroscopy for the Management of Intrauterine Pathology: A Systematic Review. Diagnostics 2024, 14, 327. https://doi.org/10.3390/diagnostics14030327
Etrusco A, Buzzaccarini G, Laganà AS, Chiantera V, Vitale SG, Angioni S, D’Alterio MN, Nappi L, Sorrentino F, Vitagliano A, et al. Use of Diode Laser in Hysteroscopy for the Management of Intrauterine Pathology: A Systematic Review. Diagnostics. 2024; 14(3):327. https://doi.org/10.3390/diagnostics14030327
Chicago/Turabian StyleEtrusco, Andrea, Giovanni Buzzaccarini, Antonio Simone Laganà, Vito Chiantera, Salvatore Giovanni Vitale, Stefano Angioni, Maurizio Nicola D’Alterio, Luigi Nappi, Felice Sorrentino, Amerigo Vitagliano, and et al. 2024. "Use of Diode Laser in Hysteroscopy for the Management of Intrauterine Pathology: A Systematic Review" Diagnostics 14, no. 3: 327. https://doi.org/10.3390/diagnostics14030327
APA StyleEtrusco, A., Buzzaccarini, G., Laganà, A. S., Chiantera, V., Vitale, S. G., Angioni, S., D’Alterio, M. N., Nappi, L., Sorrentino, F., Vitagliano, A., Difonzo, T., Riemma, G., Mereu, L., Favilli, A., Peitsidis, P., & D’Amato, A. (2024). Use of Diode Laser in Hysteroscopy for the Management of Intrauterine Pathology: A Systematic Review. Diagnostics, 14(3), 327. https://doi.org/10.3390/diagnostics14030327