
A Technique for Monitoring Mechanically Ventilated Patient Lung Conditions


Abstract
1. Introduction
- In ICU settings, an endotracheal tube (ETT) bypasses a significant portion of the respiratory system, neglecting part of the true respiratory resistance.
2. Materials
2.1. Automated Diagnostic Techniques in the Medical Domain
2.2. Time-Series Data Diagnostic Techniques in Medical Applications
2.3. Challenges in Applying Time-Series Diagnostic Techniques to MV Data
- Inappropriate Data Types: Many datasets focus on limited patient condition labels or data from non-ideal ventilation modes like BiPAP/CPAP.
- Irrelevance to Fully Sedated Patients: Data related to PVA are irrelevant here, as our focus is on fully sedated patients.
- Incompleteness and Low Sampling Frequency: Many datasets have infrequent data collection, reducing their utility for accurate diagnostics.
- Limited Data Volume and Variety: Available data lack diversity in patient parameters and are not representative of broader populations.
- Lack of Labeling: Many datasets lack essential information such as ventilator settings and patient characteristics.
2.4. Synthetic Data and Human Lung Modeling for MV Diagnostics
2.5. Current Mechanical Parameter Analysis Techniques
3. Methods
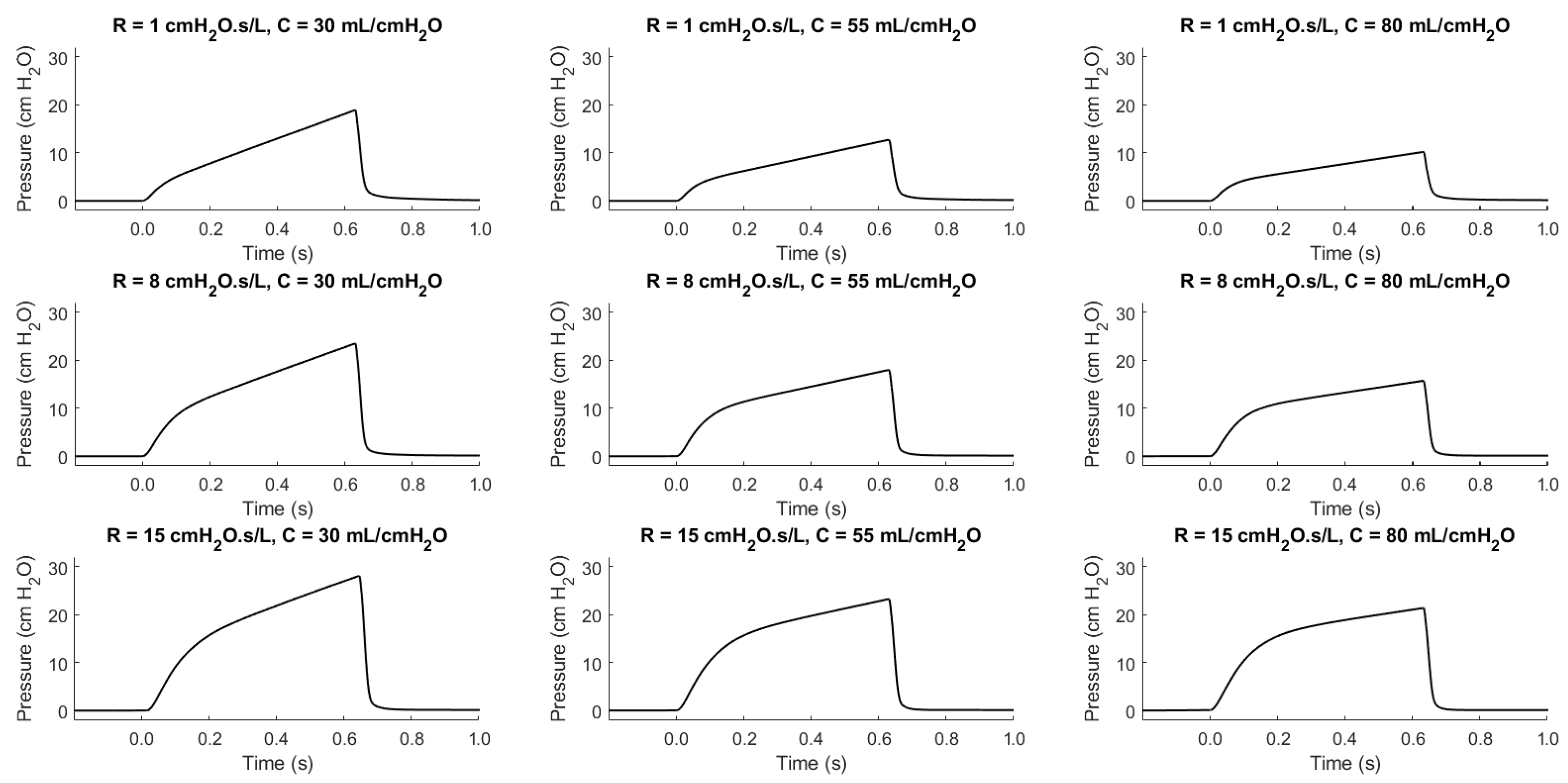
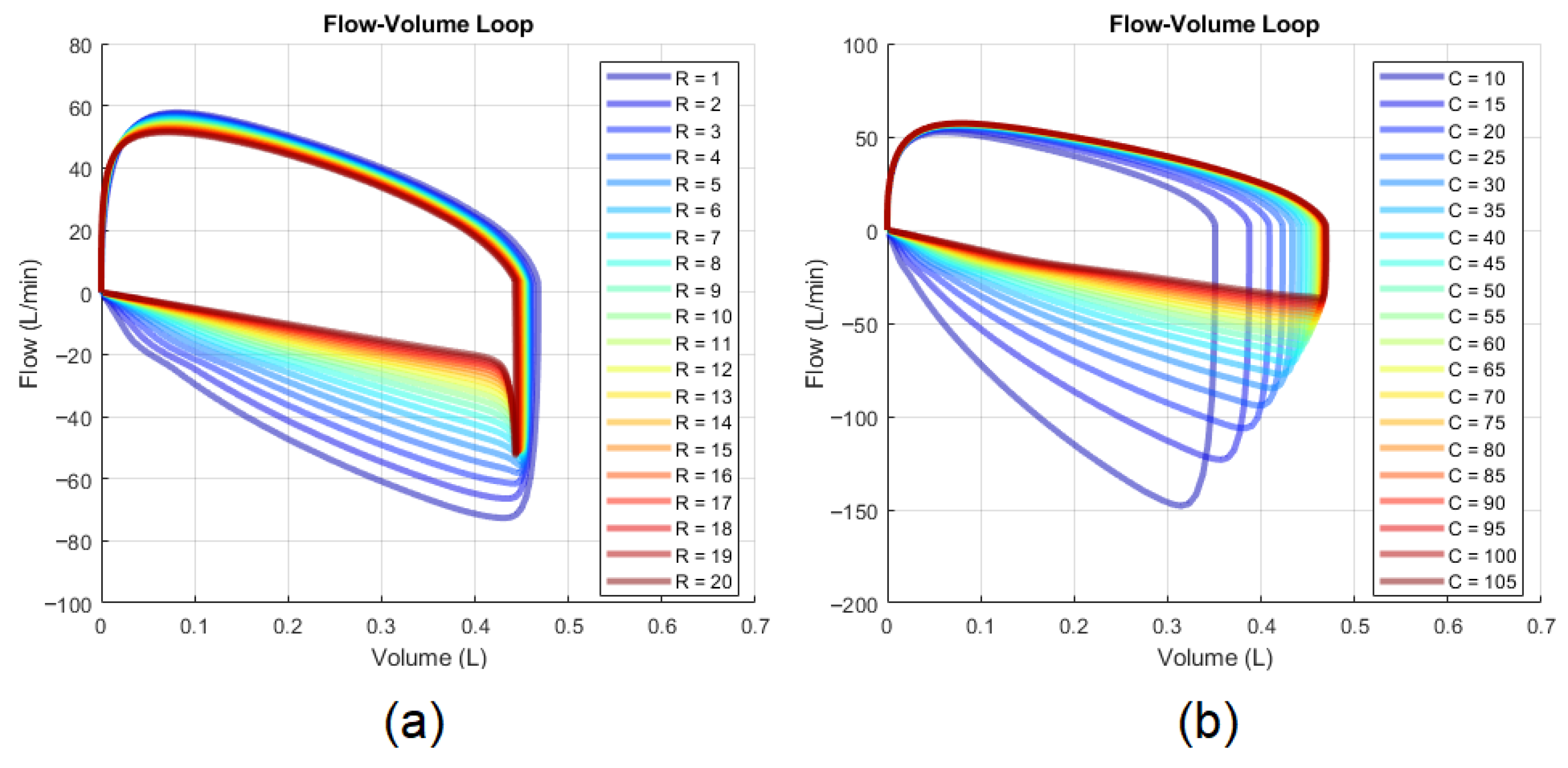
3.1. Synthetic Data Generation
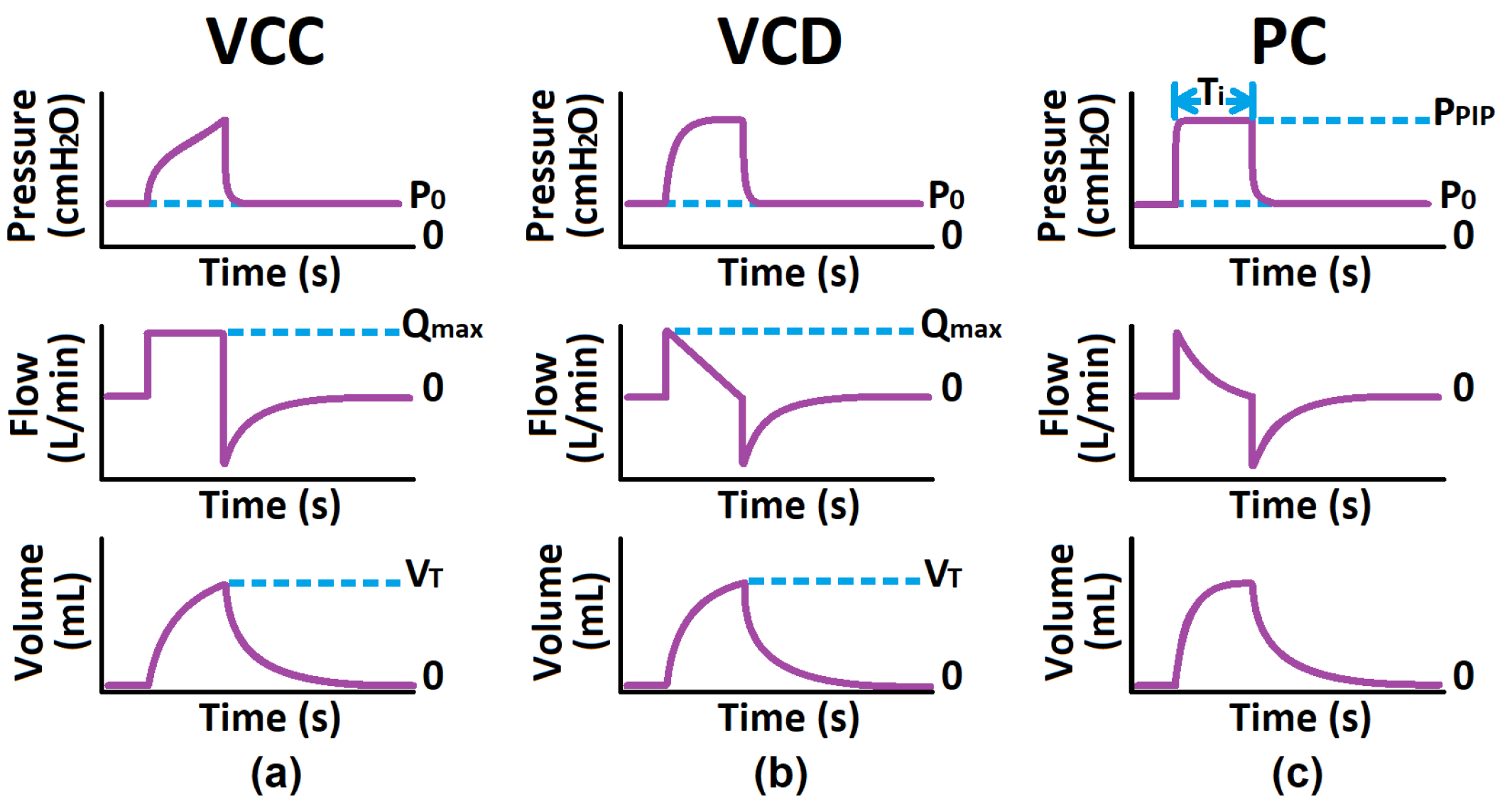
- VCC and VCD Modes: Positive End-Expiratory Pressure (), Maximum Flow (), Tidal Volume (), Respiratory Resistance (), Static Compliance ()
- PC Mode: , Peak Inspiratory Pressure (), Inspiratory Time (), ,
- : 0 to 15 (4 levels)
- : 10 to 105 (20 levels)
- : 180 to 750 (20 levels)
- : + 5 to 35 (20 levels)
- : 0.5 to 2.4 (20 levels)
- : 1 to 20 (20 levels)
- : 10 to 105 (20 levels)
3.2. Automated Diagnostic Approach
3.2.1. Automatic Mode Classifier
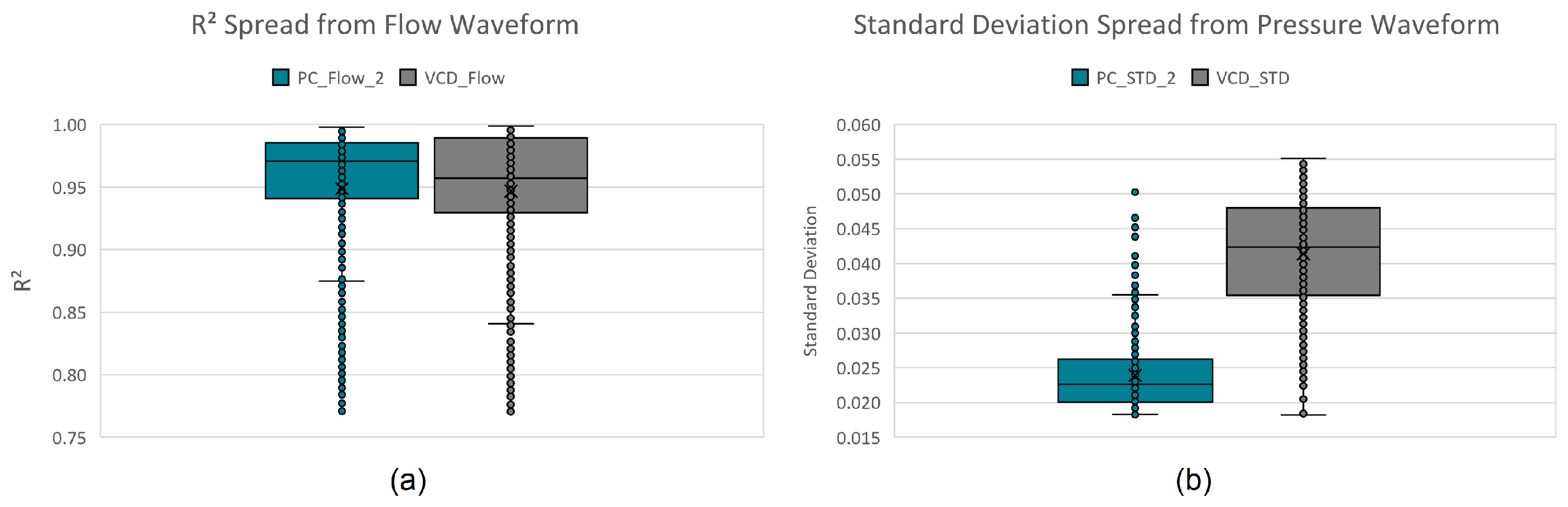
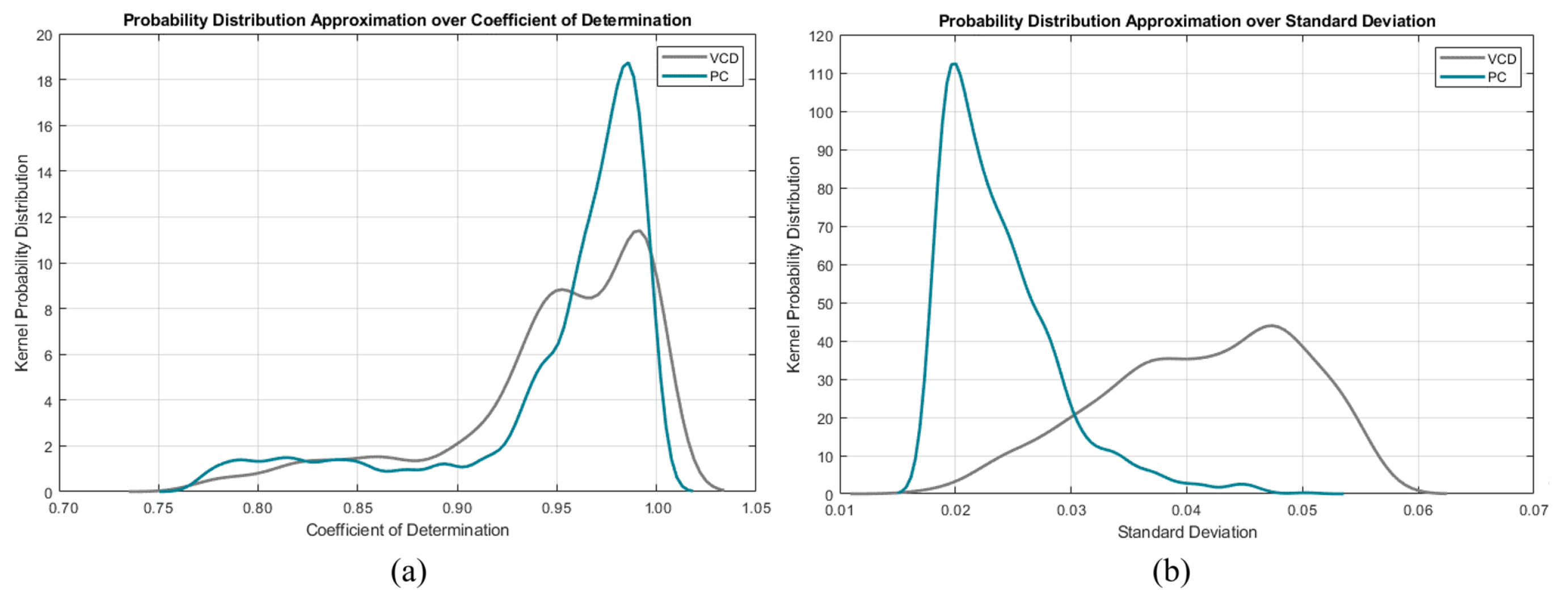
- Standard Deviation () from the Average Inspiratory Pressure: Represented by a horizontal line during the inspiratory phase of a normalized waveform. It is small for PC mode, slightly larger for VCD mode, and largest for VCC mode.
- Coefficient of Determination () of the Flow Waveform: Measures the fit of the flow waveform to a straight line spanning from the point of maximum initial flow to zero flow at the end of the inspiratory phase. It indicates a good fit for VCD mode, a fair fit for PC mode, and a poor fit for VCC mode.
3.2.2. Feature Extraction Layer
- Vent Mode: VCC, VCD or PC
- Vent Parameters: , , , ,
- Expiratory Phase Volume Time Constant ( in )
- Expiratory Flow at One Time Constant ( in )
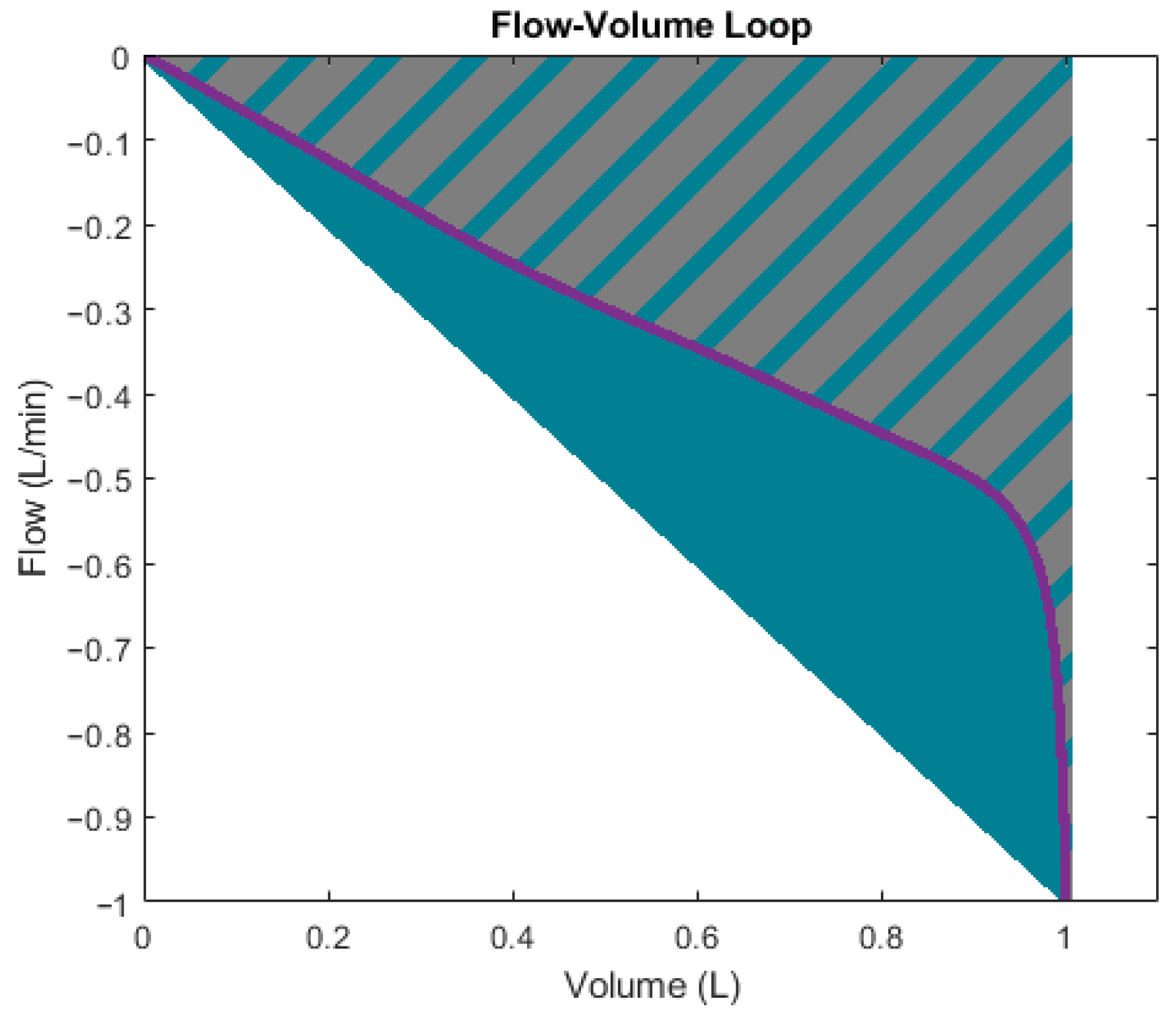
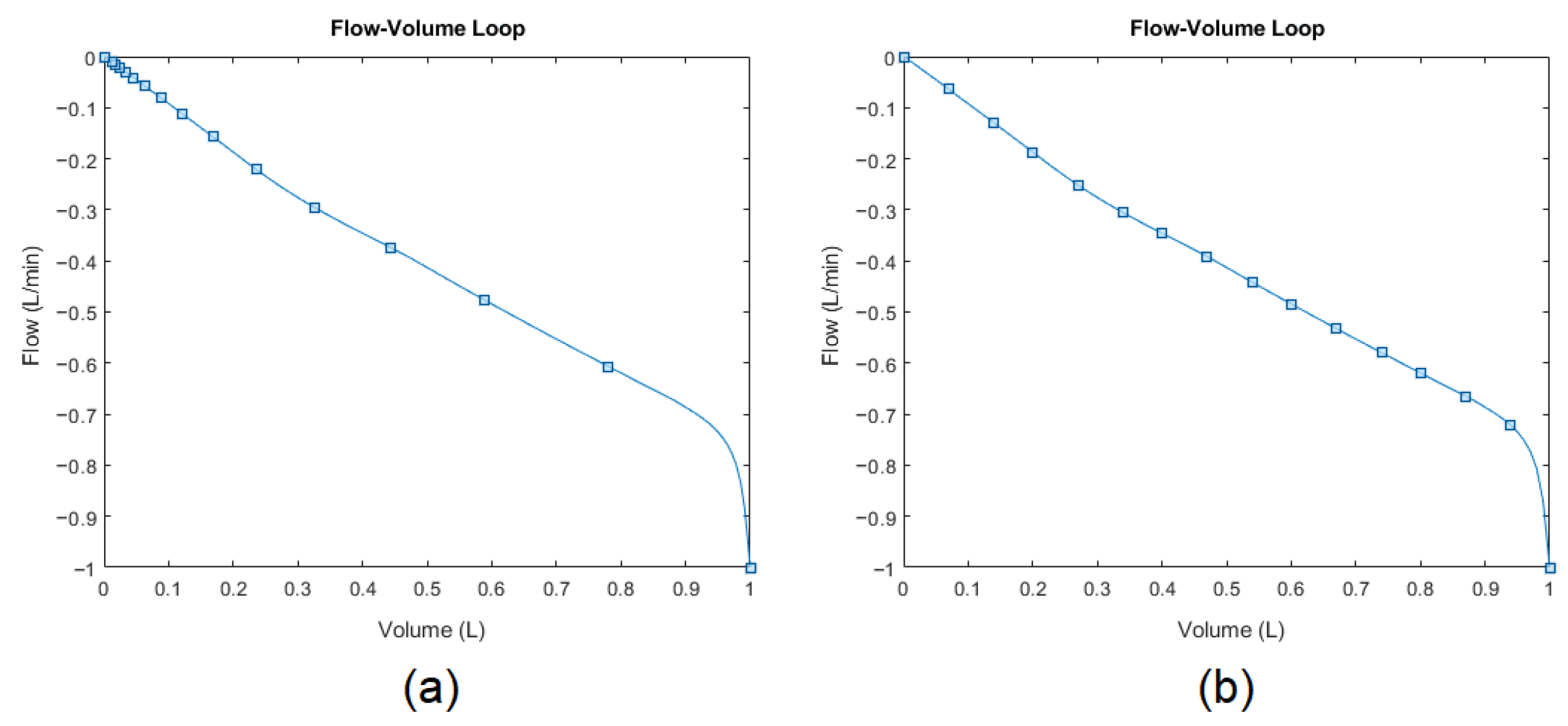
- Flow-Volume Loop Shape Descriptors: gradient, surface ratio, skewness, kurtosis
3.2.3. Supervised Regression Models for Lung Parameters
- Linear Regression Algorithms: Normal Linear Regression, Interactions Linear Regression, Robust Linear Regression, and Stepwise Linear Regression
- Decision Tree Algorithms: Fine Trees, Medium Trees, Coarse Trees
- Support Vector Machine (SVM) Algorithms: Linear SVM, Quadratic SVM, Cubic SVM, Fine Gaussian SVM, Medium Gaussian SVM, and Coarse Gaussian SVM
- Gaussian Process Regression (GPR) Algorithms: Exponential GPR, Squared Exponential GPR, Matern 5/2 GPR, Rational Quadratic GPR
- Ensemble Algorithms: Boosted Trees, and Bagged Trees
- Neural Networks (NN): Narrow Neural Network (NNN), Medium Neural Network (MNN), Wide Neural Network (WNN), Bi-Layered Neural Network (BLNN), and Tri-Layered Neural Network (TLNN).
4. Results
4.1. Automatic Mode Classifier
4.2. Feature Extraction Layer
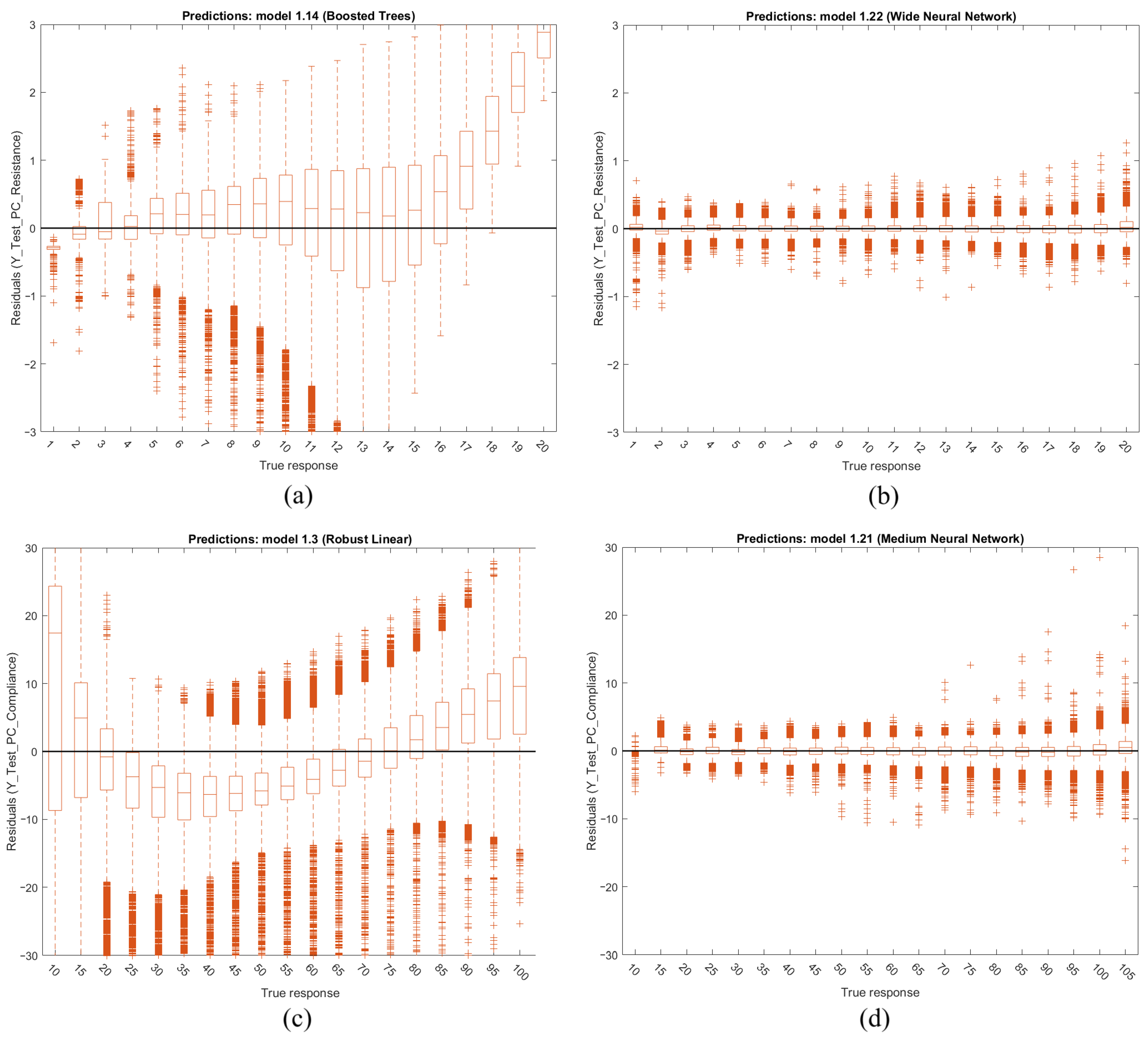
4.3. Supervised Regression Models for Lung Parameters
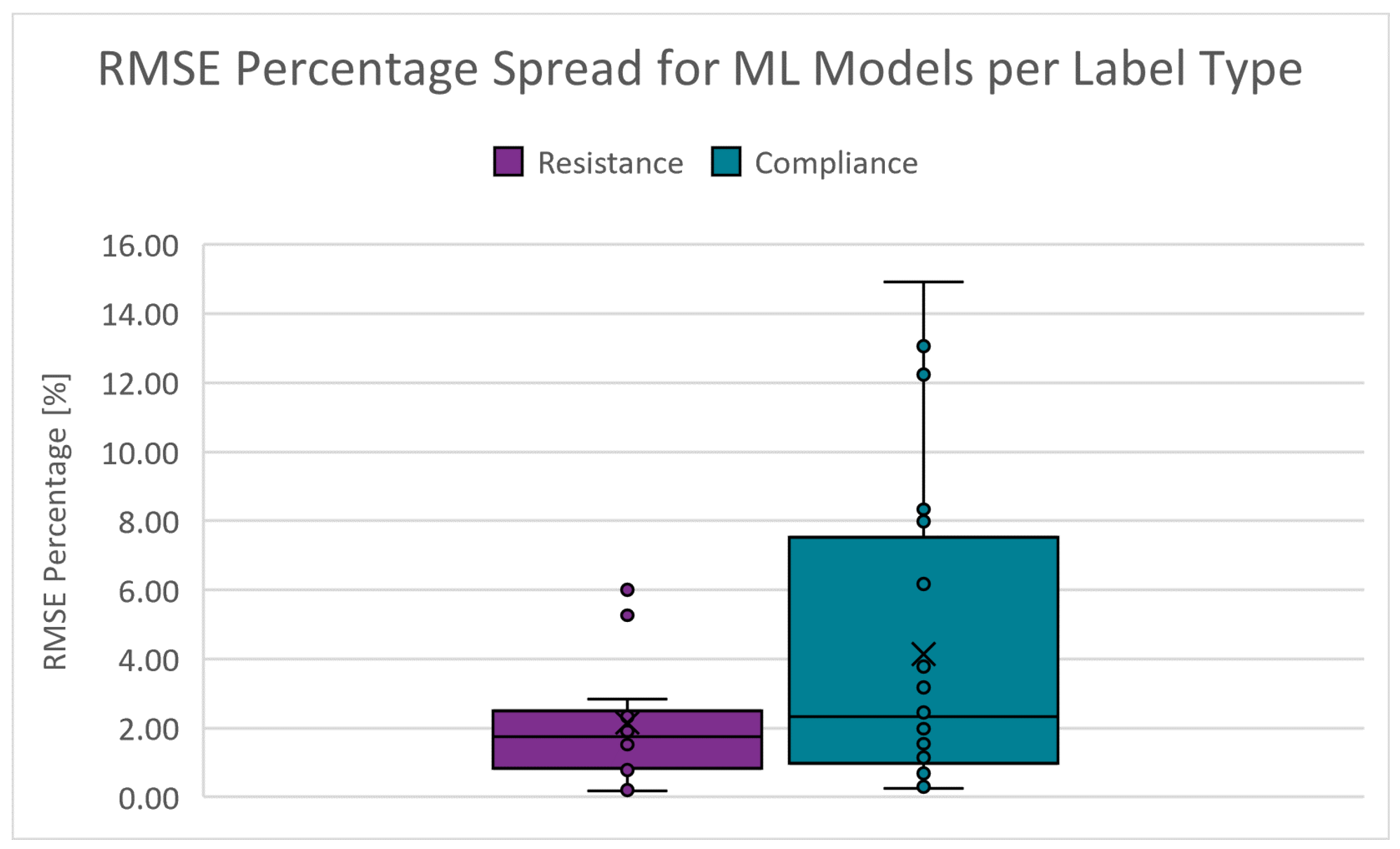
4.3.1. RMSE Percentage
4.3.2. Training Speed
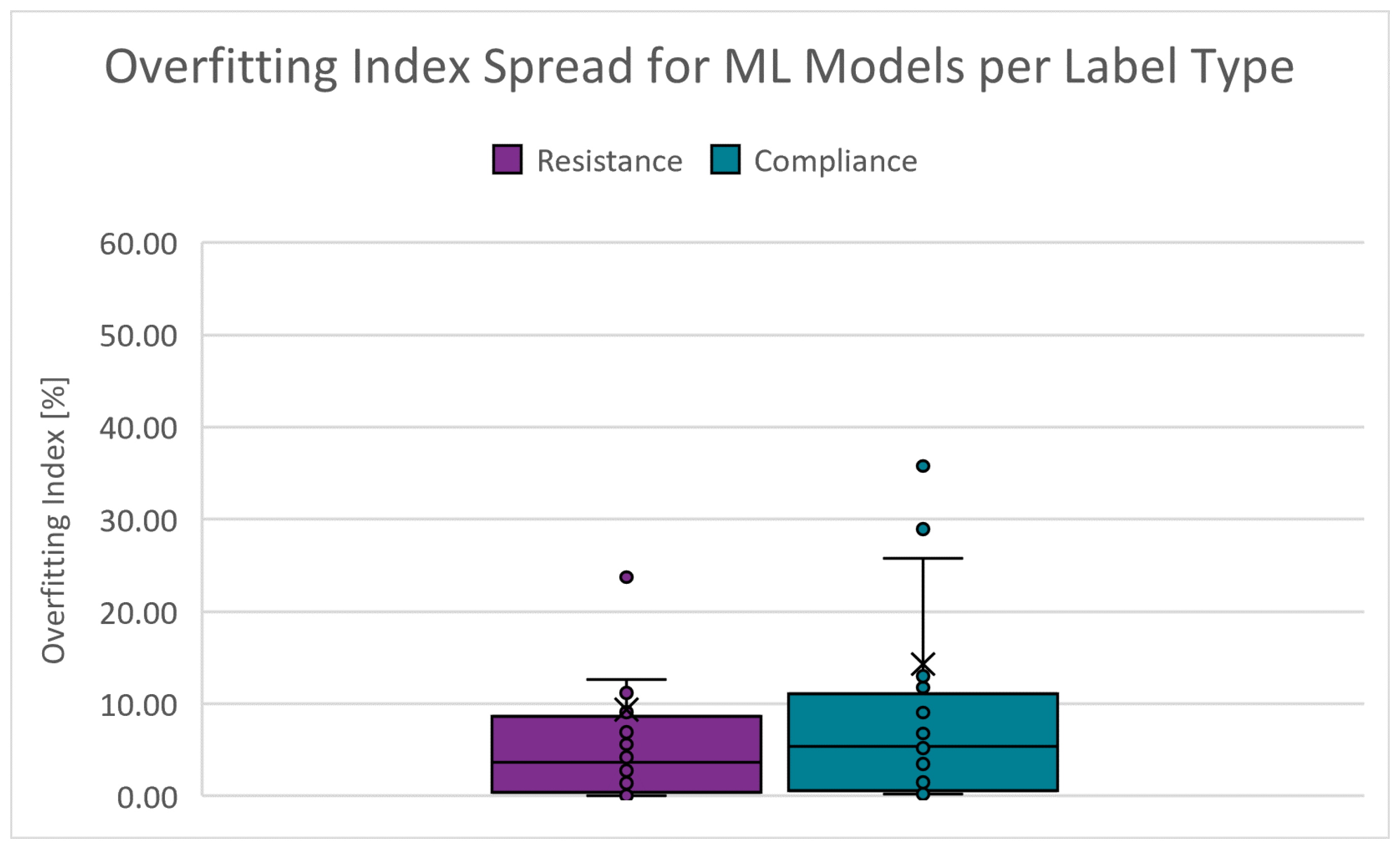
4.3.3. Overfitting Index
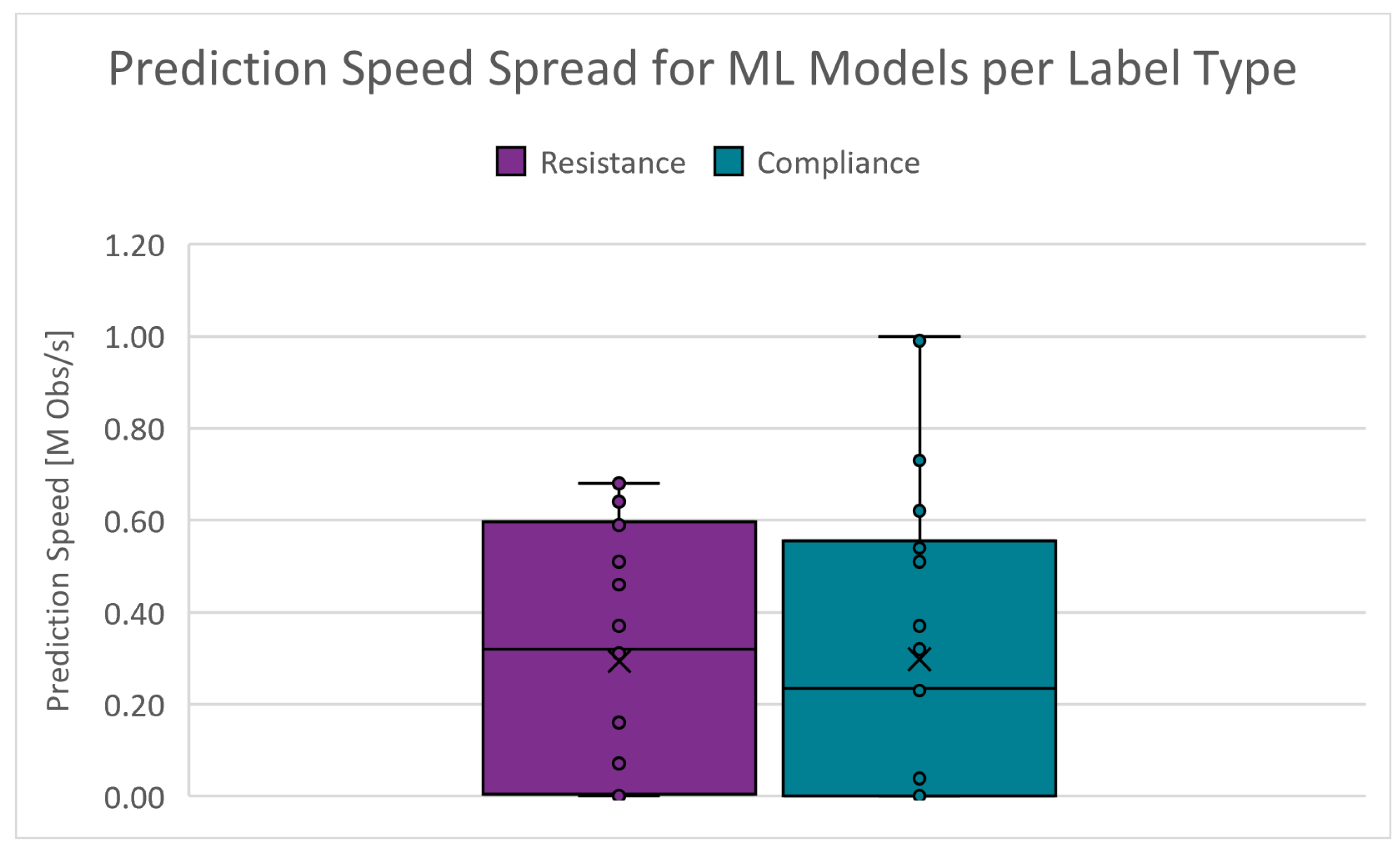
4.3.4. Prediction Speed
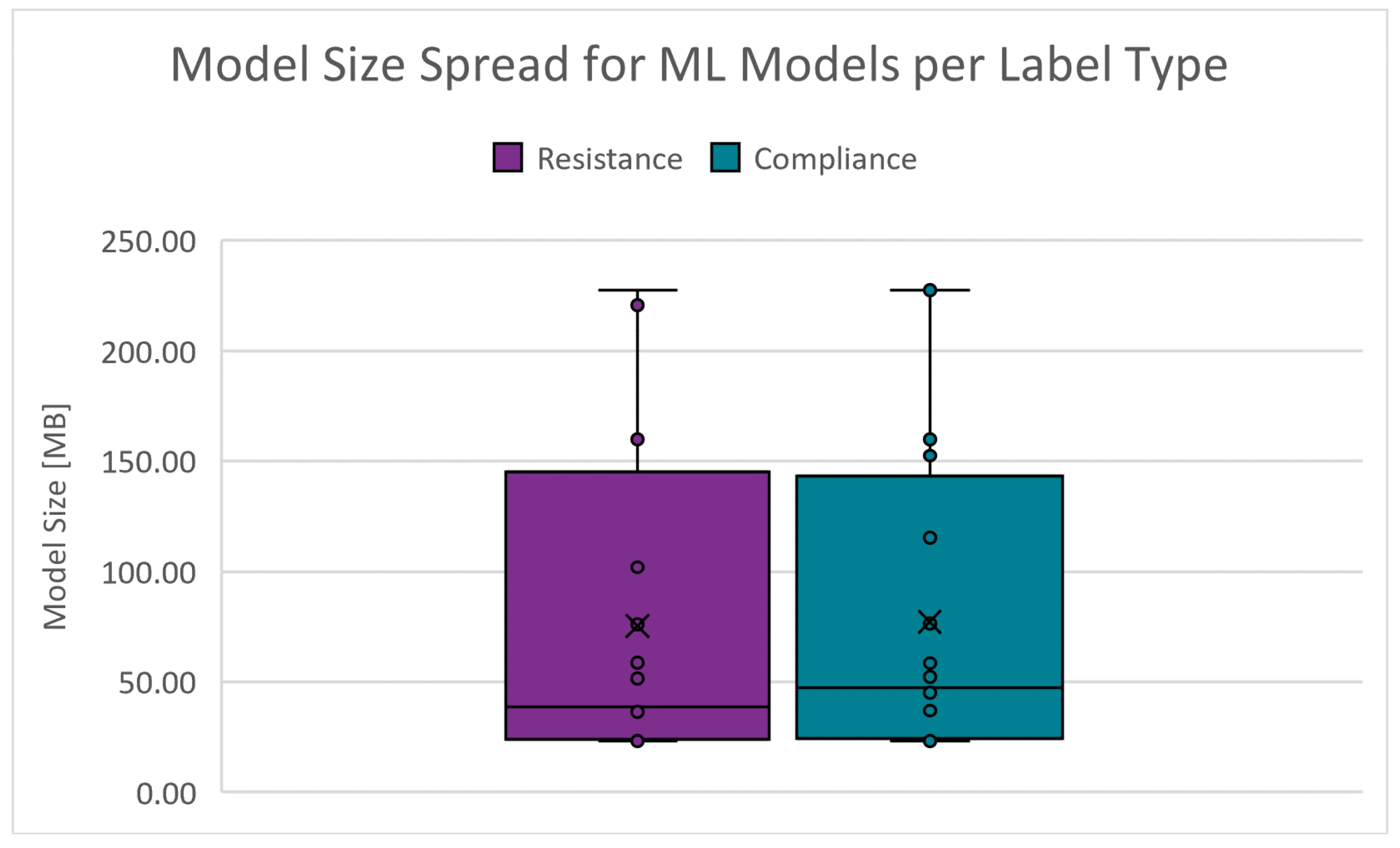
4.3.5. Model Size
4.4. Deployment of Regression Models
5. Discussion
6. Work Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BLNN | Bi-Layered Neural Network |
| COVID-19 | Coronavirus Disease 2019 |
| Static Compliance | |
| FDI | Fault Detection and Isolation |
| GPR | Gaussian Process Regression |
| ICU | Intensive Care Unit |
| KPDF | Kernel Probability Distribution Functions |
| MNN | Medium Neural Network |
| MV | Mechanical Ventilation |
| NNN | Narrow Neural Network |
| PC | Pressure-Controlled |
| PEEP | Positive End-Expiratory Pressure |
| Peak Inspiratory Pressure | |
| PVA | Patient-Ventilator Asynchrony |
| Maximum Flow | |
| Respiratory System Resistance | |
| RMSE | Root Mean Squared Error |
| STD | Standard Deviation |
| SVM | Support Vector Machine |
| TLNN | Tri-Layered Neural Network |
| TS | Time-Series |
| Inspiratory Time | |
| VCC | Volume-Controlled Constant Flow |
| VCD | Volume-Controlled Decreasing Flow |
| Tidal Volume | |
| WNN | Wide Neural Network |
References
- Poor, H. Basics of Mechanical Ventilation, 1st ed.; Springer International Publishing: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- West, J.B. Respiratory Physiology: The Essentials; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Wilcox, S.R.; Aydin, A.; Marcolini, E.G. Mechanical Ventilation in Emergency Medicine; Springer: Cham, Switzerland, 2021. [Google Scholar]
- World Health Organization. GHE: Leading Causes of Death. 2023. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death (accessed on 18 September 2024).
- Smith, J.; Doe, R. Acute respiratory distress syndrome in COVID-19: Possible mechanisms and therapeutic management. Pneumonia 2020, 12, 45–58. [Google Scholar] [CrossRef]
- Al-Rawas, N.; Banner, M.J.; Euliano, N.R.; Tams, C.G.; Brown, J.; Martin, A.D.; Gabrielli, A. Expiratory time constant for determinations of plateau pressure, respiratory system compliance, and total resistance. Crit. Care 2013, 17, R23. [Google Scholar] [CrossRef] [PubMed]
- Wald, A.; Jason, D.; Murphy, T.W.; Mazzia, V.D. A computer system for respiratory parameters. Comput. Biomed. Res. 1969, 2, 411–429. [Google Scholar] [CrossRef] [PubMed]
- Uhl, R.R.; Lewis, F. Digital computer calculation of human pulmonary mechanics using a least squares fit technique. Comput. Biomed. Res. 1974, 7, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Daoud, E.G.; Katigbak, R.; Ottochian, M. Accuracy of the Ventilator Automated Displayed Respiratory Mechanics in Passive and Active Breathing Conditions: A Bench Study. Respir. Care 2019, 64, 1555–1560. [Google Scholar] [CrossRef]
- Kannangara, D.O.; Newberry, F.; Howe, S.; Major, V.; Redmond, D.; Szlavecs, A.; Chiew, Y.S.; Pretty, C.; Benyó, B.; Shaw, G.M.; et al. Estimating the true respiratory mechanics during asynchronous pressure controlled ventilation. Biomed. Signal Process. Control 2016, 30, 70–78. [Google Scholar] [CrossRef]
- Howe, S.L.; Chase, J.G.; Redmond, D.P.; Morton, S.E.; Kim, K.T.; Pretty, C.; Shaw, G.M.; Tawhai, M.H.; Desaive, T. Inspiratory respiratory mechanics estimation by using expiratory data for reverse-triggered breathing cycles. Comput. Methods Programs Biomed. 2020, 186, 105184. [Google Scholar] [CrossRef]
- van Drunen, E.J.; Chiew, Y.S.; Chase, J.G.; Shaw, G.M.; Lambermont, B.; Janssen, N.; Damanhuri, N.S.; Desaive, T. Expiratory model-based method to monitor ARDS disease state. Biomed. Eng. Online 2013, 12, 1. [Google Scholar] [CrossRef]
- Peslin, R.; Da Silva, J.F.; Chabot, F.; Duvivier, C. Respiratory mechanics studied by multiple linear regression in unsedated ventilated patients. Eur. Respir. J. 1992, 5, 871–878. [Google Scholar] [CrossRef]
- Vicario, F.; Buizza, R.; Truschel, W.A.; Chbat, N.W. Noninvasive estimation of alveolar pressure. In Proceedings of the 2016 IEEE Engineering in Medicine and Biology Society Annual Conference, Orlando, FL, USA, 16–20 August 2016; pp. 2721–2724. [Google Scholar] [CrossRef]
- Vicario, F.; Albanese, A.; Karamolegkos, N.; Wang, D.; Seiver, A.; Chbat, N.W. Noninvasive estimation of respiratory mechanics in spontaneously breathing ventilated patients: A constrained optimization approach. IEEE Trans. Biomed. Eng. 2016, 63, 775–787. [Google Scholar] [CrossRef]
- Tan, C.P.; Chiew, Y.S.; Chase, J.G.; Chiew, Y.W.; Pretty, C.; Desaive, T.; Md Ralib, A.; Mat, M.B. Model iterative airway pressure reconstruction during mechanical ventilation asynchrony: Shapes and sizes of reconstruction. In Proceedings of the IFMBE Proceedings, Penang, Malaysia, 10–13 December 2017; Volume 67, pp. 133–139. [Google Scholar]
- Newberry, F.; Kannangara, O.; Howe, S.; Major, V.; Redmond, D.; Szlavecz, A.; Chiew, Y.S.; Pretty, C.; Benyo, B.; Shaw, G.M.; et al. Iterative interpolative pressure reconstruction for improved respiratory mechanics estimation during asynchronous volume controlled ventilation. In Proceedings of the IFMBE Proceedings, Putrajaya, Malaysia, 6–8 December 2015; Volume 56, pp. 133–139. [Google Scholar]
- Redmond, D.P.; Docherty, P.D.; Chiew, Y.S.; Chase, J.G. A polynomial model of patient-specific breathing effort during controlled mechanical ventilation. In Proceedings of the 2015 IEEE Engineering in Medicine and Biology Society Annual Conference, Milan, Italy, 25–29 August 2015; pp. 4532–4535. [Google Scholar] [CrossRef]
- Chen, Y.; Yuan, Y.; Chang, Q.; Zhang, H.; Li, F.; Chen, Z. Continuous estimation of respiratory system compliance and airway resistance during pressure-controlled ventilation without end-inspiration occlusion. BMC Pulm. Med. 2024, 24, 249. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, G. A novel method to calculate compliance and airway resistance in ventilated patients. Intensive Care Med. Exp. 2022, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Redmond, D.P.; Major, V.; Corbett, S.; Glassenbury, D.; Beatson, A.; Szlávecz, A.; Chiew, Y.S.; Shaw, G.M.; Chase, J.G. Pressure reconstruction by eliminating the demand effect of spontaneous respiration (PREDATOR) method for assessing respiratory mechanics of reverse-triggered breathing cycles. In Proceedings of the 2014 IEEE Conference on Biomedical Engineering and Sciences, Kuala Lumpur, Malaysia, 8–10 December 2014; pp. 332–337. [Google Scholar] [CrossRef]
- Major, V.; Corbett, S.; Redmond, D.; Beatson, A.; Glassenbury, D.; Chiew, Y.S.; Pretty, C.; Desaive, T.; Szlávecz, A.; Benyó, B.; et al. Respiratory mechanics assessment for reverse-triggered breathing cycles using pressure reconstruction. Biomed. Signal Process. Control 2015, 22, 135–145. [Google Scholar] [CrossRef]
- Redmond, D.P.; Chiew, Y.S.; Major, V.; Chase, J.G. Evaluation of model-based methods in estimating respiratory mechanics in the presence of variable patient effort. Comput. Methods Programs Biomed. 2019, 171, 67–79. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Yuan, Y.; Chang, Q.; Zhang, H.; Li, F.; Chen, Z. Monitoring Lung Mechanics during Mechanical Ventilation using Machine Learning Algorithms. In Proceedings of the 2018 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Honolulu, HI, USA, 18–21 July 2018; pp. 2197–2201. [Google Scholar] [CrossRef]
- Lotti, P.; Braschi, A. Measurements of respiratory mechanics during mechanical ventilation. Minerva Anestesiol. 1999, 65, 301–307. [Google Scholar]
- Guérin, C.; Richard, J.C. Measurement of respiratory system resistance during mechanical ventilation. Intensive Care Med. 2007, 33, 1046–1049. [Google Scholar] [CrossRef]
- DuBois, A.B.; Brody, A.W.; Lewis, D.H.; Burgess, B.F.J. Oscillation mechanics of lungs and chest in man. J. Appl. Physiol. 1956, 8, 587–594. [Google Scholar] [CrossRef]
- Farré, R.; Ferrer, M.; Rotger, M.; Torres, A.; Navajas, D. Respiratory mechanics in ventilated COPD patients: Forced oscillation versus occlusion techniques. Eur. Respir. J. 1998, 12, 170–176. [Google Scholar] [CrossRef]
- Farré, R.; Gavela, E.; Rotger, M.; Ferrer, M.; Roca, J.; Navajas, D. Noninvasive assessment of respiratory resistance in severe chronic respiratory patients with nasal CPAP. Eur. Respir. J. 2000, 15, 314–319. [Google Scholar] [CrossRef]
- Warner, M.A.; Patel, B. Mechanical Ventilation. In Benumof and Hagberg’s Airway Management, 3rd ed.; W.B. Saunders: Philadelphia, PA, USA, 2013; pp. 981–997. [Google Scholar]
- Yu, L.; Halalau, A.; Dalal, B.; Abbas, A.E.; Ivascu, F.; Amin, M.; Nair, G.B. Machine Learning Methods to Predict Mechanical Ventilation and Mortality in Patients with COVID-19. PLoS ONE 2021, 16, e0249285. [Google Scholar] [CrossRef]
- Landry, J. Respiratory Formulas, Calculations, and Equations. 2024. Available online: https://www.respiratorytherapyzone.com/respiratory-therapy-formulas-calculations/ (accessed on 30 April 2024).
- Arnal, J.M. Monitoring Mechanical Ventilation Using Ventilator Waveforms; Springer: Cham, Switzerland, 2018. [Google Scholar]
- Szmuk, P.; Ezri, T.; Evron, S.; Roth, Y.; Katz, J. A brief history of tracheostomy and tracheal intubation, from the Bronze Age to the Space Age. Intensive Care Med. 2008, 34, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Chatburn, R.L. Understanding mechanical ventilators. Expert Rev. Respir. Med. 2010, 4, 809–819. [Google Scholar] [CrossRef] [PubMed]
- Chatburn, R.L.; El-Khatib, M.; Mireles-Cabodevila, E. A taxonomy for mechanical ventilation: 10 fundamental maxims. Respir. Care 2014, 59, 1747–1763. [Google Scholar] [CrossRef] [PubMed]
- Pasteka, R.; da Costa, J.P.S.; Barros, N.; Kolar, R.; Forjan, M. Patient–Ventilator Interaction Testing Using the Electromechanical Lung Simulator xPulmTM During V/AC and PSV Ventilation Mode. Appl. Sci. 2021, 11, 3745. [Google Scholar] [CrossRef]
- Nagarjuna, M.V. Ventilator Waveform Analysis [Presented at the DM Seminars, Department of Pulmonary Medicine, PGIMER, Chandigarh, India]. 2016. Available online: https://www.indiachest.org/wp-content/uploads/2016/07/Ventilator-waveform-analysis-nagarjuna-2012.pdf (accessed on 30 April 2024).
- Campbell, R.S.; Davis, B.R. Pressure-Controlled Versus Volume-Controlled Ventilation: Does it Matter? Respir. Care 2002, 47, 416–426. [Google Scholar]
- Esteban, A.; Frutos, F.; Tobin, M.J.; Alía, I.; Solsona, J.F.; Valverdú, I.; Fernández, R.; de la Cal, M.A.; Benito, S.; Tomás, R.; et al. A Comparison of Four Methods of Weaning Patients from Mechanical Ventilation. Spanish Lung Failure Collaborative Group. N. Engl. J. Med. 1995, 332, 345–350. [Google Scholar] [CrossRef]
- Mathews, C.E.; Unnikrishnan, R. Comparison of Synchronised Intermittent Mandatory Ventilation with Pressure Support versus Assist Control Mode of Ventilation on Time to Extubation. Indian J. Respir. Care 2017, 6, 781. [Google Scholar]
- Shuttleworth, D.; Dodds, N. Ventilators and Breathing Systems. In Maths Physics for Clinical Measurement in Anaesthesia and Intensive Care; Cambridge University Press: Cambridge, UK, 2019; p. 130. [Google Scholar]
- Cairo, J.M. Pilbeam’s Mechanical Ventilation: Physiological and Clinical Applications; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Wright, G.T.; Ashworth, L.; Pettey, S. Optimizing Mechanical Ventilation During General Anesthesia. AANA J. 2020, 88, 149–157. [Google Scholar]
- Morton, S.E.; Knopp, J.L.; Tawhai, M.H.; Docherty, P.; Moeller, K.; Heines, S.J.; Bergmans, D.C.; Chase, J.G. Virtual Patient Modeling and Prediction Validation for Pressure Controlled Mechanical Ventilation. IFAC-PapersOnLine 2020, 53, 16221–16226. [Google Scholar] [CrossRef]
- Kock, K.D.S.; da Rosa, B.C.; Martignago, N.; Reis, C.; Maurici, R. Comparison of respiratory mechanics measurements in the volume cycled ventilation (VCV) and pressure controlled ventilation (PCV). Fisioter. Mov. 2016, 29, 229–236. [Google Scholar]
- Ambrozin, A.R.P.; Cataneo, A.J.M. Pulmonary function aspects after myocardial revascularization related to preoperative risk. Braz. J. Cardiovasc. Surg. 2005, 20, 408–415. [Google Scholar] [CrossRef]
- Dai, J.; Wang, H.; Xu, Y.; Chen, X.; Tian, R. Clinical application of AI-based PET images in oncological patients. Semin. Cancer Biol. 2023, 85, 161–175. [Google Scholar] [CrossRef]
- Bakr, M.; Reis, A. The role of machine learning in clinical chemistry: Current trends and future perspectives. Clin. Chem. Lab. Med. (CCLM) 2021, 59, 2027–2035. [Google Scholar]
- Gupta, A.; Sharma, S. Time-series analysis in healthcare: A systematic review. J. Biomed. Inform. 2021, 119, 103846. [Google Scholar] [CrossRef]
- Blanch, L.; Villagra, A.; Sales, B.; Montanya, J.; Lucangelo, U.; Luján, M.; García-Esquirol, O.; Chacón, E.; Estruga, A.; Oliva, J.C.; et al. Asynchronies during mechanical ventilation are associated with mortality. Intensive Care Med. 2015, 41, 633–641. [Google Scholar] [CrossRef]
- Vignaux, L.; Tassaux, D.; Jolliet, P.; Piquilloud, L. Automated detection of patient-ventilator asynchrony: New tools for improving ventilator settings. Respir. Care 2019, 64, 890–901. [Google Scholar] [CrossRef]
- Isermann, R. Fault-Diagnosis Systems: An Introduction from Fault Detection to Fault Tolerance; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2005. [Google Scholar]
- Heo, G.Y. Condition Monitoring Using Empirical Models: Technical Review and Prospects for Nuclear Applications. Nucl. Eng. Technol. 2008, 40, 49–68. [Google Scholar] [CrossRef]
- Shumway, R.H.; Stoffer, D.S. Time Series Analysis and Its Applications: With R Examples, 4th ed.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Durbin, R.; Eddy, S.R.; Krogh, A.; Mitchison, G. Biological Sequence Analysis: Probabilistic Models of Proteins and Nucleic Acids; Cambridge University Press: Cambridge, UK, 1998. [Google Scholar] [CrossRef]
- Brigham, E.O. The Fast Fourier Transform and Its Applications; Prentice Hall: Upper Saddle River, NJ, USA, 1988. [Google Scholar]
- Mallat, S. A Wavelet Tour of Signal Processing: The Sparse Way, 3rd ed.; Academic Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Hochreiter, S.; Schmidhuber, J. Long Short-Term Memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Bai, S.; Kolter, J.Z.; Koltun, V. An Empirical Evaluation of Generic Convolutional and Recurrent Networks for Sequence Modeling. arXiv 2018, arXiv:1803.01271. [Google Scholar]
- Müller, M. Dynamic Time Warping. In Information Retrieval for Music and Motion; Springer: Berlin/Heidelberg, Germany, 2007; pp. 69–84. [Google Scholar] [CrossRef]
- Jolliffe, I.T. Principal Component Analysis, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2002. [Google Scholar] [CrossRef]
- Granger, C.W.J. Investigating Causal Relations by Econometric Models and Cross-spectral Methods. Econometrica 1969, 37, 424–438. [Google Scholar] [CrossRef]
- Bengio, Y.; Courville, A.; Vincent, P. Representation Learning: A Review and New Perspectives. IEEE Trans. Pattern Anal. Mach. Intell. 2013, 35, 1798–1828. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.R.; Zin, W.A. Respiratory System Dynamical Mechanical Properties: Modeling in Time and Frequency Domain. Biophys. Rev. 2011, 3, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Ghafarian, P.; Jamaati, H.; Hashemian, S.M. A Review on Human Respiratory Modeling. Tanaffos 2016, 15, 61. [Google Scholar] [PubMed]
- Pillow, J.; Hall, G.L.; Willet, K.E.; Jobe, A.H.; Hantos, Z.; Sly, P. Effects of Gestation and Antenatal Steroid on Airway and Tissue Mechanics in Newborn Lambs. Am. J. Respir. Crit. Care Med. 2001, 163, 1158–1163. [Google Scholar] [CrossRef] [PubMed]
- Emrath, E. The basics of ventilator waveforms. Curr. Pediatr. Rep. 2021, 9, 11–19. [Google Scholar] [CrossRef]
- Russian, C.J.; Gonzales, J.F.; Henry, N.R. Suction catheter size: An assessment and comparison of 3 different calculation methods. Respir. Care 2014, 59, 32–38. [Google Scholar] [CrossRef]
- Tilakaratna, P. Tracheal Tubes Explained Simply. 2024. Available online: https://www.howequipmentworks.com/tracheal_tubes/ (accessed on 30 April 2024).
- Marx, P. Masters_2022. 2022. Available online: https://github.com/TheRealPieterMarx/Masters_2022.git (accessed on 28 April 2024).
- MathWorks, I. Medical Ventilator with Lung Model. 2022. Available online: https://www.mathworks.com/help/simscape/ug/medical-ventilator-with-lung-model.html (accessed on 30 April 2024).
- Miller, S. Simscape-Medical-Ventilator. 2021. Available online: https://github.com/mathworks/Simscape-Medical-Ventilator (accessed on 14 April 2020).
- Kamthamraju, R. Neonatal-Ventilator. 2020. Available online: https://github.com/ravalik28/Neonatal-ventilator (accessed on 8 April 2020).
- Tamburrano, P.; Sciatti, F.; Distaso, E.; Lorenzo, L.D.; Amirante, R. Validation of a Simulink Model for Simulating the Two Typical Controlled Ventilation Modes of Intensive Care Units Mechanical Ventilators. Appl. Sci. 2022, 12, 2057. [Google Scholar] [CrossRef]
- Yeshurun, T.; David, Y.B.; Herman, A.; Bar-Sheshet, S.; Zilberman, R.; Bachar, G.; Liberzon, A.; Segev, G. A simulation of a medical ventilator with a realistic lungs model. F1000Research 2020, 9, ISF-1302. [Google Scholar] [CrossRef]
- Al-Naggar, N.Q. Modelling and Simulation of Pressure Controlled Mechanical Ventilation System. J. Biomed. Sci. Eng. 2015, 8, 707–716. [Google Scholar] [CrossRef]
- Yalcinkaya, F.; Yildirim, M.E.; Ünsal, H. Pressure-Volume Controlled Mechanical Ventilator: Modeling and Simulation. In Proceedings of the 2015 9th International Conference on Electrical and Electronics Engineering, Bursa, Turkey, 26–28 November 2015. [Google Scholar]
- Solís-Lemus, J.A.; Costar, E.; Doorly, D.; Kerrigan, E.C.; Kennedy, C.H.; Tait, F.; Niederer, S.; Vincent, P.E.; Williams, S.E. A simulated single ventilator/dual patient ventilation strategy for acute respiratory distress syndrome during the COVID-19 pandemic. R. Soc. Open Sci. 2020, 7, 200585. [Google Scholar] [CrossRef]
- Guler, H.; Ata, F. Design of a Fuzzy-LabVIEW-Based Mechanical Ventilator. Comput. Syst. Sci. Eng. 2014, 29, 219–229. [Google Scholar]
- Alessandro. Lung Ventilation in Simulink. 2022. Available online: https://alessandromastrofini.it/2022/04/05/ventilation/ (accessed on 30 April 2024).
- Tran, A.S.; Ngo, H.Q.T.; Dong, V.K.; Vo, A.H. Design, Control, Modeling, and Simulation of Mechanical Ventilator for Respiratory Support. Math. Probl. Eng. 2021, 2021, e2499804. [Google Scholar] [CrossRef]
- Das, A. Modelling and Optimisation of Mechanical Ventilation for Critically Ill Patients. Ph.D. Thesis, University of Exeter (United Kingdom), Exeter, UK, 2012. [Google Scholar]
- MathWorks. Pdf—Probability Density Function. MathWorks, 2023. Statistics and Machine Learning Toolbox Documentation. Available online: https://www.mathworks.com/help/stats/prob.normaldistribution.pdf.html (accessed on 30 April 2024).
- MathWorks. Skewness—Measure of Asymmetry of Data. MathWorks, 2023. Statistics and Machine Learning Toolbox Documentation. Available online: https://www.mathworks.com/help/stats/skewness.html (accessed on 30 April 2024).
- MathWorks. Kurtosis—Measure of the “Tailedness” of Data Distribution. MathWorks, 2023. Statistics and Machine Learning Toolbox Documentation. Available online: https://www.mathworks.com/help/stats/kurtosis.html (accessed on 30 April 2024).
- MathWorks. Regression Learner App. 2023. Available online: https://www.mathworks.com/help/stats/regression-learner-app.html (accessed on 18 September 2024).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Residual Mean [%] | Residual STD [%] |
|---|---|---|
| 1.298 | 1.115 | |
| −8.694 | 9.834 | |
| −5.406 | 3.941 | |
| −0.179 | 1.710 | |
| 0.868 | 0.970 |
| Case | Alg. | RMSE [%] | Training Speed [d] | Overfit Index [%] | Pred. Spd. [M Obs/s] | Size [MB] |
|---|---|---|---|---|---|---|
| R VCC | BLNN | 1.610 | 2.421 | 3.742 | 0.61 | 25.042 |
| R VCD | BLNN | 1.390 | 3.386 | 0.781 | 0.94 | 25.043 |
| R PC | WNN | 0.431 | 0.632 | 1.176 | 0.33 | 23.127 |
| C VCC | MNN | 1.963 | 2.373 | 1.791 | 0.79 | 25.142 |
| C VCD | NNN | 2.297 | 2.331 | 0.323 | 1.10 | 25.142 |
| C PC | MNN | 0.924 | 0.028 | 5.967 | 0.54 | 23.208 |
| Use Case | Mean Local RMSE Percentage [%] | Mean Total RMSE Percentage [%] |
|---|---|---|
| R VCC | 3.10 | 1.05 |
| R VCD | 3.44 | 1.24 |
| R PC | 0.72 | 0.26 |
| C VCC | 2.47 | 1.01 |
| C VCD | 6.04 | 1.78 |
| C PC | 1.34 | 0.77 |
| Cluster | Training Time | Testing RMSE (Accuracy) | Model Size | Prediction Speed | Best For |
|---|---|---|---|---|---|
| Linear Models | Very Low | Moderate | Moderate to Large | Very High | Fast deployment with low computational cost |
| Tree-Based Models | Very Low | Moderate to High | Small to Moderate | High | Balanced performance, interpretability |
| Support Vector Machines | Moderate to High | Good to Very Good | Moderate | Low to Moderate | High accuracy with manageable training cost |
| Gaussian Process Regression | Very High | Very High (Excellent) | Large | Very Low | High-accuracy tasks where real-time prediction isn’t needed |
| Neural Networks | Moderate | Good | Compact | Very High | Real-time applications needing both accuracy and speed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marx, P.; Marais, H. A Technique for Monitoring Mechanically Ventilated Patient Lung Conditions. Diagnostics 2024, 14, 2616. https://doi.org/10.3390/diagnostics14232616
Marx P, Marais H. A Technique for Monitoring Mechanically Ventilated Patient Lung Conditions. Diagnostics. 2024; 14(23):2616. https://doi.org/10.3390/diagnostics14232616
Chicago/Turabian StyleMarx, Pieter, and Henri Marais. 2024. "A Technique for Monitoring Mechanically Ventilated Patient Lung Conditions" Diagnostics 14, no. 23: 2616. https://doi.org/10.3390/diagnostics14232616
APA StyleMarx, P., & Marais, H. (2024). A Technique for Monitoring Mechanically Ventilated Patient Lung Conditions. Diagnostics, 14(23), 2616. https://doi.org/10.3390/diagnostics14232616