
Spontaneous Headshake after a Kinematic Event (SHAAKE): Evaluating the Utility of a Potential New Sign in the Diagnosis of Concussion

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
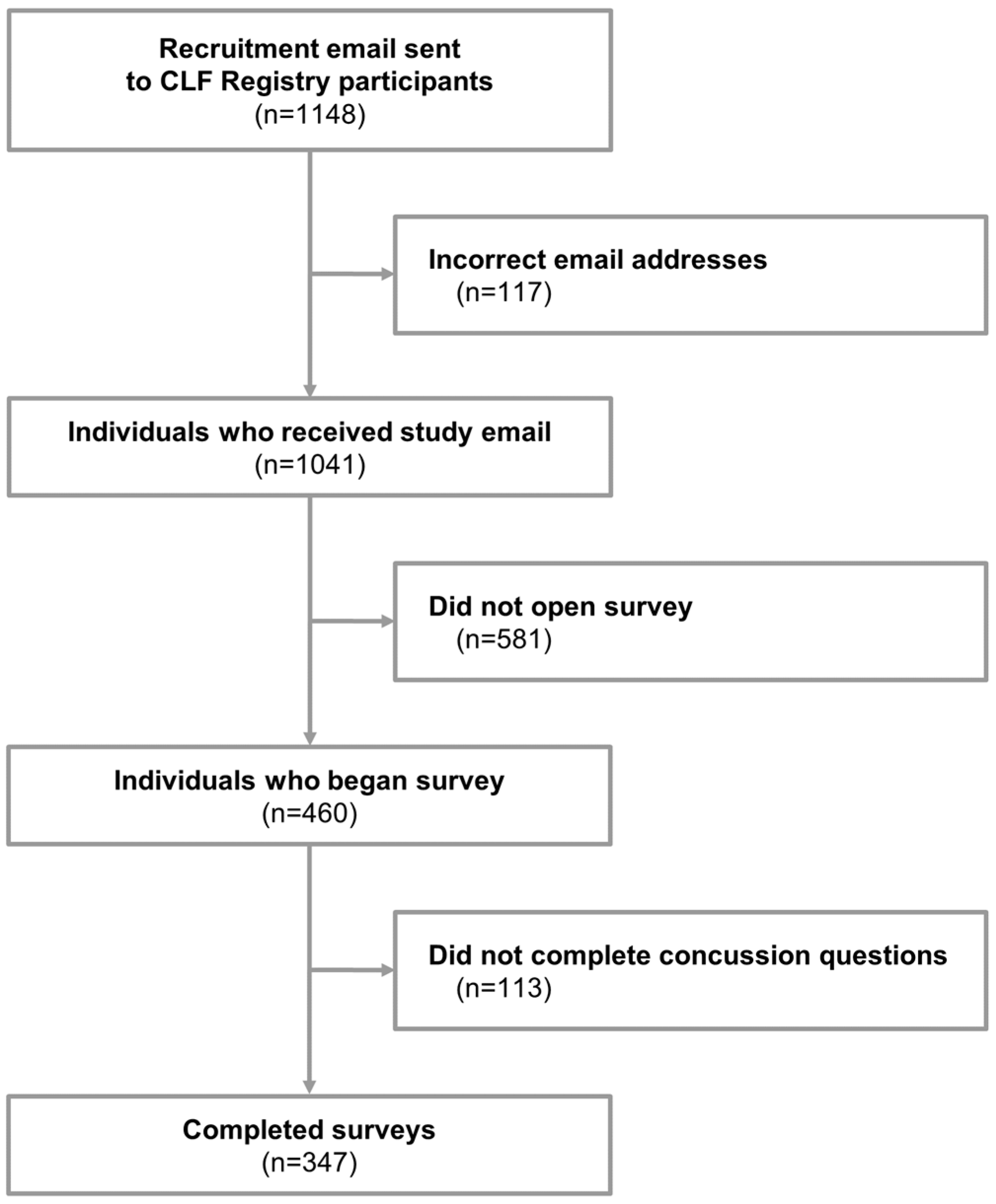
2.1. Sample
2.2. Procedure
2.3. Survey
2.4. Statistical Analysis
3. Results
3.1. Participants
3.2. Concussion Experience
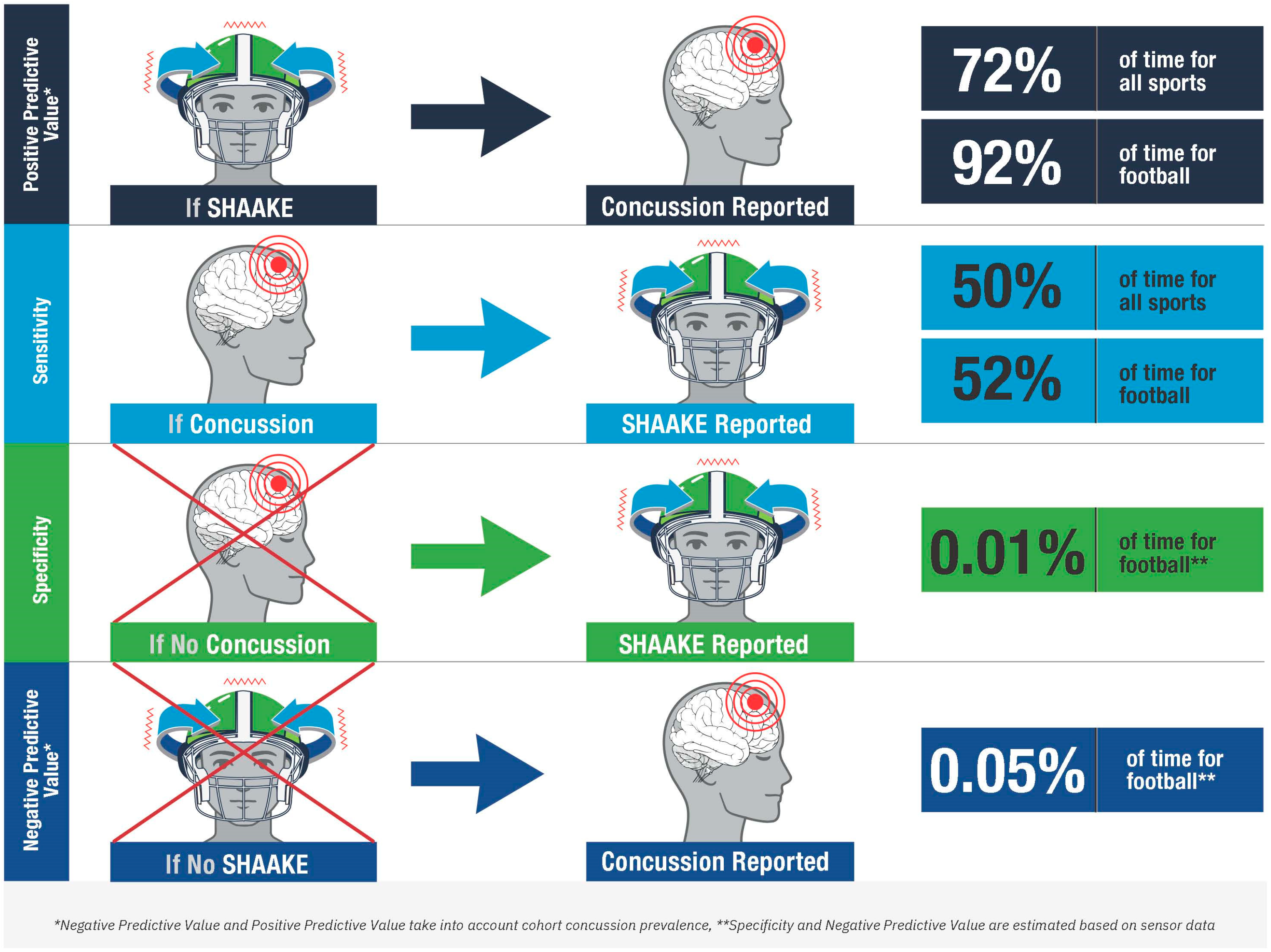
3.3. SHAAKE Experience and Association with Concussion
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Daneshvar, D.H.; Riley, D.O.; Nowinski, C.J.; McKee, A.C.; Stern, R.A.; Cantu, R.C. Long-term consequences: Effects on normal development profile after concussion. Phys. Med. Rehabil. Clin. N. Am. 2011, 22, 683–700. [Google Scholar] [CrossRef]
- McPherson, A.L.; Nagai, T.; Webster, K.E.; Hewett, T.E. Musculoskeletal Injury Risk After Sport-Related Concussion: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2019, 47, 1754–1762. [Google Scholar] [CrossRef]
- Loftin, M.C.; Zynda, A.J.; Tracey, A.J.; Klein, L.A.; Pollard-McGrandy, A.M.; Covassin, T. The association between continuing to play, clinical domains, and recovery outcomes in collegiate athletes following concussion. Neurosurg. Focus 2024, 57, E8. [Google Scholar] [CrossRef]
- McKee, A.C.; Stein, T.D.; Huber, B.R.; Crary, J.F.; Bieniek, K.; Dickson, D.; Alvarez, V.E.; Cherry, J.D.; Farrell, K.; Butler, M.; et al. Chronic traumatic encephalopathy (CTE): Criteria for neuropathological diagnosis and relationship to repetitive head impacts. Acta Neuropathol. 2023, 145, 371–394. [Google Scholar] [CrossRef]
- Stern, R.A.; Daneshvar, D.H.; Baugh, C.M.; Seichepine, D.R.; Montenigro, P.H.; Riley, D.O.; Fritts, N.G.; Stamm, J.M.; Robbins, C.A.; McHale, L.; et al. Clinical presentation of chronic traumatic encephalopathy. Neurology 2013, 81, 1122–1129. [Google Scholar] [CrossRef]
- Nowinski, C.J.; Rhim, H.C.; McKee, A.C.; Zafonte, R.D.; Dodick, D.W.; Cantu, R.C.; Daneshvar, D.H. ‘Subconcussive’ is a dangerous misnomer: Hits of greater magnitude than concussive impacts may not cause symptoms. Br. J. Sports Med. 2024, 58, 754–756. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Goldstein, L.E.; Kiernan, P.T.; Stein, T.D.; McKee, A.C. Post-traumatic neurodegeneration and chronic traumatic encephalopathy. Mol. Cell Neurosci. 2015, 66, 81–90. [Google Scholar] [CrossRef]
- Kroshus, E.; Baugh, C.M.; Daneshvar, D.H. Content, Delivery, and Effectiveness of Concussion Education for US College Coaches. Clin. J. Sport Med. 2016, 26, 391–397. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Baugh, C.M.; Yutsis, M.; Pea, R.D.; Goldman, S.; Grant, G.A.; Cantu, R.C.; Sanders, L.M.; Chen, C.L.; Lama, R.D.; et al. Athlete Enjoyment of Prior Education Moderates change in Concussion-Reporting Intention after Interactive Education. Inquiry 2021, 58, 1–8. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Yutsis, M.; Baugh, C.M.; Pea, R.D.; Goldman, S.; Grant, G.A.; Ghajar, J.; Sanders, L.M.; Chen, C.L.; Tenekedjieva, L.T.; et al. Evaluating the Effect of Concussion-Education Programs on Intent to Report Concussion in High School Football. J. Athl. Train. 2021, 56, 1197–1208. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Baugh, C.M.; Lama, R.D.; Yutsis, M.; Pea, R.D.; Goldman, S.; Grant, G.A.; Cantu, R.C.; Sanders, L.M.; Zafonte, R.D.; et al. Participating in Two Video Concussion Education Programs Sequentially Improves Concussion-Reporting Intention. Neurotrauma Rep. 2021, 2, 581–591. [Google Scholar] [CrossRef]
- Kroshus, E.; Baugh, C.M.; Hawrilenko, M.; Daneshvar, D.H. Pilot randomized evaluation of publically available concussion education materials: Evidence of a possible negative effect. Health Educ. Behav. 2015, 42, 153–162. [Google Scholar] [CrossRef]
- Broglio, S.P.; Katz, B.P.; Zhao, S.; McCrea, M.; McAllister, T. Test-Retest Reliability and Interpretation of Common Concussion Assessment Tools: Findings from the NCAA-DoD CARE Consortium. Sports Med. 2018, 48, 1255–1268. [Google Scholar] [CrossRef]
- Davis, G.A.; Patricios, J.; Schneider, K.J.; Iverson, G.L.; Silverberg, N.D. Definition of sport-related concussion: The 6th International Conference on Concussion in Sport. Br. J. Sports Med. 2023, 57, 617–618. [Google Scholar] [CrossRef]
- Dharnipragada, R.; Naik, A.; Denduluri, L.S.; Bederson, M.; Akkad, A.; Cramer, S.W.; Koester, S.W.; Catapano, J.S.; Zuckerman, S.L.; Snyder, L.; et al. Diagnostic predictive values for sport-related concussions: A systematic review and diagnostic meta-analysis. J. Neurosurg. 2024, 140, 560–569. [Google Scholar] [CrossRef]
- Harmon, K.G.; Whelan, B.M.; Aukerman, D.F.; Hwang, C.E.; Poddar, S.K.; DeLeo, A.; Elkington, H.A.; Garruppo, G.; Holliday, M.; Bruce, J.M. Diagnosis of Sports-Related Concussion Using Symptom Report or Standardized Assessment of Concussion. JAMA Netw. Open 2024, 7, e2416223. [Google Scholar] [CrossRef]
- Silverberg, N.D.; Iverson, G.L.; Cogan, A.; Dams, O.C.K.; Delmonico, R.; Graf, M.J.P.; Iaccarino, M.A.; Kajankova, M.; Kamins, J.; McCulloch, K.L.; et al. The American Congress of Rehabilitation Medicine Diagnostic Criteria for Mild Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2023, 104, 1343–1355. [Google Scholar] [CrossRef]
- United States Centers for Disease Control and Prevention. Signs and Symptoms of Concussion. Available online: https://www.cdc.gov/heads-up/signs-symptoms/index.html (accessed on 26 August 2024).
- Echemendia, R.J.; Brett, B.L.; Broglio, S.; Davis, G.A.; Giza, C.C.; Guskiewicz, K.M.; Harmon, K.G.; Herring, S.; Howell, D.R.; Master, C.L.; et al. Introducing the Sport Concussion Assessment Tool 6 (SCAT6). Br. J. Sports Med. 2023, 57, 619–621. [Google Scholar] [CrossRef]
- NFL Head, Neck and Spine Committee’s Concussion Diagnosis and Management Protocol. Available online: https://www.nfl.com/playerhealthandsafety/resources/fact-sheets/nfl-head-neck-and-spine-committee-s-concussion-diagnosis-and-management-protocol (accessed on 26 August 2024).
- Elbin, R.J.; Zuckerman, S.L.; Sills, A.K.; Crandall, J.R.; Lessley, D.J.; Solomon, G.S. Sensitivity and Specificity of On-Field Visible Signs of Concussion in the National Football League. Neurosurgery 2020, 87, 530–537. [Google Scholar] [CrossRef]
- Baugh, C.M.; Kiernan, P.T.; Kroshus, E.; Daneshvar, D.H.; Montenigro, P.H.; McKee, A.C.; Stern, R.A. Frequency of head-impact-related outcomes by position in NCAA division I collegiate football players. J. Neurotrauma 2015, 32, 314–326. [Google Scholar] [CrossRef]
- Conway, F.N.; Domingues, M.; Monaco, R.; Lesnewich, L.M.; Ray, A.E.; Alderman, B.L.; Todaro, S.M.; Buckman, J.F. Concussion Symptom Underreporting Among Incoming National Collegiate Athletic Association Division I College Athletes. Clin. J. Sport Med. 2020, 30, 203–209. [Google Scholar] [CrossRef]
- Kroshus, E.; Daneshvar, D.H.; Baugh, C.M.; Nowinski, C.J.; Cantu, R.C. NCAA concussion education in ice hockey: An ineffective mandate. Br. J. Sports Med. 2014, 48, 135–140. [Google Scholar] [CrossRef]
- Kroshus, E.; Baugh, C.M.; Daneshvar, D.H.; Viswanath, K. Understanding concussion reporting using a model based on the theory of planned behavior. J. Adolesc. Health 2014, 54, 269–274.e2. [Google Scholar] [CrossRef]
- Kroshus, E.; Baugh, C.M.; Daneshvar, D.H.; Stamm, J.M.; Laursen, R.M.; Austin, S.B. Pressure on Sports Medicine Clinicians to Prematurely Return Collegiate Athletes to Play After Concussion. J. Athl. Train. 2015, 50, 944–951. [Google Scholar] [CrossRef]
- Makdissi, M.; Davis, G. The reliability and validity of video analysis for the assessment of the clinical signs of concussion in Australian football. J. Sci. Med. Sport 2016, 19, 859–863. [Google Scholar] [CrossRef]
- The Management of Sport-Related Concussion in Australian Football. Available online: https://play.afl/sites/default/files/2024-03/The-Management-of-Sport-Related-Concussion-in-Australian-Football-Mar-24.pdf (accessed on 10 August 2024).
- Gardner, A.J. Reliability of Using the Proposed International Consensus Video Signs of Potential Concussion for National Rugby League Head Impact Events. Neurosurgery 2021, 88, 538–543. [Google Scholar] [CrossRef]
- Concussion Guidance. Available online: https://resources.worldrugby-rims.pulselive.com/worldrugby/document/2024/08/26/ab286493-d1b4-4213-b476-ee6309a3f9c9/Concussion-Guidance-August-2024.pdf (accessed on 10 August 2024).
- Christmas Vacation Lights Scene HD SFW. Erik Abelar. 2016. Available online: https://www.youtube.com/watch?v=iXaw70X7wb4&t=157s (accessed on 10 August 2024).
- The Super Mario Bros. Movie—Mario vs. Donkey Kong Scene|Movieclips. Movieclips. 2023. Available online: https://www.youtube.com/watch?v=-EIXPOw_Wzs&t=264s (accessed on 10 August 2024).
- Tom and Jerry (Season 1) Dog Hits Spike with a Frying Pan and Spike Presses Tom’s Seatbelt to Stop. 2023. Available online: https://www.youtube.com/watch?v=OSOGGVbc8gg (accessed on 10 August 2024).
- Saving Your Brain Is a Winning Move: Concussion Awareness Now. Concussion Awareness Now. 2023. Available online: https://www.youtube.com/watch?v=bUwh-MZm6tE&t=3s%202023 (accessed on 10 August 2024).
- Triple H Epic Oversell. terrence0258. 2014. Available online: https://www.youtube.com/watch?v=z8KbXThVBFI (accessed on 10 August 2024).
- Robbins, C.A.; Daneshvar, D.H.; Picano, J.D.; Gavett, B.E.; Baugh, C.M.; Riley, D.O.; Nowinski, C.J.; McKee, A.C.; Cantu, R.C.; Stern, R.A. Self-reported concussion history: Impact of providing a definition of concussion. Open Access J. Sports Med. 2014, 5, 99–103. [Google Scholar] [CrossRef]
- Laker, S.R.; Nicolosi, C. Sports Related Concussion. Phys. Med. Rehabil. Clin. N. Am. 2024, 35, 547–558. [Google Scholar] [CrossRef]
- Tomei, K.L.; Doe, C.; Prestigiacomo, C.J.; Gandhi, C.D. Comparative analysis of state-level concussion legislation and review of current practices in concussion. Neurosurg. Focus 2012, 33, E11. [Google Scholar] [CrossRef]
- Daneshvar, D.H.; Nair, E.S.; Baucom, Z.H.; Rasch, A.; Abdolmohammadi, B.; Uretsky, M.; Saltiel, N.; Shah, A.; Jarnagin, J.; Baugh, C.M.; et al. Leveraging football accelerometer data to quantify associations between repetitive head impacts and chronic traumatic encephalopathy in males. Nat. Commun. 2023, 14, 3470. [Google Scholar] [CrossRef]
- Louis, E.D.; Meyers, J.H.; Cristal, A.D.; Patel, A.; Tinaz, S.; Pullman, S.L.; Clark, L.N.; Ottman, R.; Factor-Litvak, P. Transient, Isolated Head Tremor in “Unaffected” Individuals: Is Essential Tremor an even more Prevalent Disease than We Suppose? Front. Neurol. 2018, 9, 570. [Google Scholar] [CrossRef]
- McCrea, M.A.; Shah, A.; Duma, S.; Rowson, S.; Harezlak, J.; McAllister, T.W.; Broglio, S.P.; Giza, C.C.; Goldman, J.; Cameron, K.L.; et al. Opportunities for Prevention of Concussion and Repetitive Head Impact Exposure in College Football Players: A Concussion Assessment, Research, and Education (CARE) Consortium Study. JAMA Neurol. 2021, 78, 346–350. [Google Scholar] [CrossRef]
- Sherman, R. Tua Tagovailoa and the NFL’s Horrible Handling of Head Injuries. The Ringer. 2022. Available online: https://www.theringer.com/nfl/2022/9/30/23379871/tua-tagovailoa-concussion-miami-dolphins (accessed on 10 August 2024).
- Belson, K.N.F.L. N.F.L.’s Concussion Protocol under Scrutiny after Tagovailoa Is Hit Hard again. The New York Times, 30 September 2022. [Google Scholar]

{kind=link}
{kind=link}
| United States Centers for Disease Control and Prevention [18] | American Congress of Rehabilitation Medicine [17] | Concussion in Sport Group [19] | National Football League [20] |
|---|---|---|---|
| The injury event causes an acute physiological disruption of brain function, as manifested by one or more of the clinical signs listed below.
|
| National Football League no-go
Potential concussion signs (observable) may include
|
| All Sports (n = 347) | Soccer (n = 99) | Football (n = 109) | p-Value * | ||
|---|---|---|---|---|---|
| Age | 27 (IQR 25–29) | 26 (IQR 23–29) | 28 (IQR 26–29) | <.001 | |
| Gender | <.001 | ||||
| Male | 167 (48.1%) | 21 (21.2%) | 103 (94.5%) | ||
| Female | 165 (47.6%) | 72 (72.7%) | 4 (3.7%) | ||
| Non-binary | 12 (3.5%) | 5 (5.1%) | 0 (0%) | ||
| Transgender female | 3 (0.9%) | 1 (1.0%) | 2 (1.8%) | ||
| Race and Ethnicity | >.05 | ||||
| American Indian or Alaska Native | 13 (3.7%) | 3 (3.0%) | 5 (4.1%) | ||
| Asian | 19 (5.5%) | 5 (5.1%) | 3 (2.8%) | ||
| Black or African American | 13 (3.7%) | 3 (3.0%) | 8 (7.3%) | ||
| Hispanic or Latino or Spanish Origin | 14 (4.0%) | 8 (8.1%) | 3 (2.8%) | ||
| White or Caucasian | 320 (92.2%) | 91 (91.9%) | 100 (91.7%) | ||
| Highest Level of Sport Participation | .19 | ||||
| Youth | 1 (0.3%) | 1 (1.0%) | 0 (0%) | ||
| High school/secondary school | 143 (41.2%) | 43 (43.4%) | 47 (43.1%) | ||
| College | 160 (46.1%) | 44 (44.4%) | 56 (51.4%) | ||
| Semi-professional | 23 (6.6%) | 3 (3.0%) | 4 (3.7%) | ||
| Professional | 11 (3.2%) | 3 (3.0%) | 2 (1.8%) | ||
| Other | 9 (2.59%) | 5 (5.1%) | 0 (0%) | ||
| Number of Seasons | 8 (IQR 6–12) | 12 (IQR 6–16) | 8 (IQR 5–12) | <.001 | |
| Military | 12 (3.5%) | 2 (2.0%) | 6 (5.5%) | .28 | |
| Years of Military | 6.8 ± 3.0 | 10 ± 4.2 | 5.8 ± 3.1 | .17 | |
| Geographical Distribution | .72 | ||||
| North America (Canada) | 51 (14.7%) | 10 (10.1%) | 12 (11.0%) | ||
| North America (USA) | 224 (64.6%) | 69 (69.7%) | 73 (66.1%) | ||
| Central America | 67 (19.3%) | 18 (18.2%) | 23 (21.1%) | ||
| Europe (Northern) | 1 (0.3%) | 0 (0%) | 0 (0%) | ||
| Europe (Western) | 2 (0.29%) | 1 (1.0%) | 1 (0.9%) | ||
| Asia (Eastern) | 1 (0.3%) | 0 (0%) | 0 (0%) | ||
| Other | 1 (0.3%) | 1 (1.0%) | 0 (0%) | ||
| All Sports (n = 347) | Soccer (n = 99) | Football (n = 109) | p-Value * | ||
|---|---|---|---|---|---|
| Ever had a concussion | 342 (98.6%) | 99 (100%) | 107 (98.2%) | .50 | |
| Number of concussions | 6 (IQR 4–11) | 6 (IQR 4–12) | 8 (IQR 5–15) | .03 | |
| Number of diagnosed concussions | 3 (IQR 2–5) | 4 (IQR 2–6) | 2 (IQR 2–4) | .01 | |
| Most recent concussion timing | .003 | ||||
| Within the past week | 1 (0.3%) | 0 | 0 | ||
| Between one week and one month ago | 5 (1.5%) | 4 (4.1%) | 0 | ||
| Between one month and six months age | 22 (6.5%) | 6 (6.1%) | 9 (8.4%) | ||
| Between six months and one year ago | 32 (9.4%) | 15 (15.3%) | 3 (2.8%) | ||
| Between one and five years ago | 136 (40%) | 37 (37.8%) | 40 (37.4%) | ||
| Between five and ten years ago | 121 (35.6%) | 32 (32.7%) | 431 (40.2%) | ||
| Between ten and twenty years ago | 23 (6.8%) | 4 (4.1%) | 12 (11.2%) | ||
| Percent of concussions from sports | 90% (IQR 75–100) | 84% (IQR 65–100) | 100% (IQR 90–100) | <.001 | |
| All Sports (n = 347) | Soccer (n = 99) | Football (n = 109) | p-Value * | ||
|---|---|---|---|---|---|
| Ever had a SHAAKE | 239 (68.9%) | 71 (71.7%) | 85 (78.0%) | .30 | |
| Number of SHAAKEs | 5 (IQR 3–10) | 4 (IQR 3–6) | 10 (IQR 5–20) | <.001 | |
| Ever had a concussion | 342 (98.6%) | 99 (100%) | 107 (98.2%) | .50 | |
| Ever had a SHAAKE because of a concussion | 223 (64.3%) | 64 (64.6%) | 80 (73.4%) | .11 | |
| Number of SHAAKEs because of a concussion | 4 (IQR 2–7) | 3 (IQR 2–6) | 5 (IQR 3–10) | .01 | |
| Number of SHAAKEs with a undiagnosed concussions | 1 (IQR 0–4) | 1 (IQR 0–2) | 3 (IQR 1–6.25) | .25 | |
| All Sports (n = 239) | Soccer (n = 71) | Football (n = 85) | p-Value * | ||||
|---|---|---|---|---|---|---|---|
| Reasons for SHAAKE (select all) | .81 | ||||||
| Neck Pain | 48 (20.1%) | 15 (21.1%) | 15 (17.6%) | ||||
| A feeling of a change in temperature or chills | 26 (10.9%) | 7 (9.9%) | 11 (12.9%) | ||||
| Emotional reaction to preceding event | 95 (39.7%) | 27 (38.0%) | 25 (29.4%) | ||||
| Pain to your face, scalp, or other part of your head that was not a headache | 46 (19.2%) | 18 (25.4%) | 14 (16.5%) | ||||
| Changes in your vision | 109 (45.6%) | 36 (50.7%) | 42 (49.4%) | .97 | |||
| Double vision | 10 (14.1%) | 14 (16.5%) | 14 (16.5%) | ||||
| Blurred vision | 25 (35.2%) | 31 (36.5%) | 31 (36.5%) | ||||
| Trouble focusing | 22 (31.0%) | 26 (30.6%) | 26 (30.6%) | ||||
| Changes in colors perceived | 6 (8.5%) | 6 (7.1%) | 6 (7.1%) | ||||
| Other | 3 (4.2%) | 4 (4.7%) | 4 (4.7%) | ||||
| Double vision | 1 (1.4%) | 3 (3.5%) | 3 (3.5%) | ||||
| Auditory changes | 49 (20.5%) | 15 (21.1%) | 19 (22.4%) | .95 | |||
| Ringing in your ears | 13 (18.3%) | 17 (20.0%) | 17 (20.0%) | ||||
| Deafness or impaired ability to hear sounds | 3 (4.2%) | 3 (3.5%) | 3 (3.5%) | ||||
| Trouble recognizing sounds | 7 (9.9%) | 8 (9.4%) | 8 (9.4%) | ||||
| Dizziness | 129 (54.0%) | 30 (42.3%) | 55 (64.7%) | ||||
| Impaired ability to balance | 71 (29.7%) | 22 (31.0%) | 30 (35.3%) | ||||
| Changes to your perception of your body’s positioning or location in space (proprioception) | 101 (42.3%) | 28 (39.4%) | 40 (47.1%) | ||||
| Headache | 71 (29.7%) | 18 (25.4%) | 28 (32.9%) | ||||
| Disorientation or confusion | 170 (71.1%) | 47 (66.2%) | 61 (71.8%) | ||||
| Unable to keep your train of thought/inability to think clearly | 73 (30.5%) | 23 (32.4%) | 32 (37.6%) | ||||
| A feeling like you needed to jumpstart your brain | 125 (52.3%) | 40 (56.3%) | 41 (48.2%) | ||||
| Other | 8 (3.3%) | 2 (2.8%) | 3 (3.5%) | ||||
| Reasons for SHAAKE (most common) | .62 | ||||||
| Neck pain | 6 (2.5%) | 2 (2.8%) | 4 (4.7%) | ||||
| A feeling of a change in temperature or chills | 1 (0.4%) | 0 (0%) | 0 (0%) | ||||
| Emotional reaction to preceding event | 18 (7.5%) | 6 (8.5%) | 2 (2.4%) | ||||
| Pain to your face, scalp, or other part of your head that was not a headache | 9 (3.8%) | 3 (4.2%) | 3 (3.5%) | ||||
| Changes in your vision | 15 (6.3%) | 7 (5.6%) | 4 (4.7%) | .64 | |||
| Double vision | 3 (20%) | 1 (14.3%) | 2 (50%) | ||||
| Blurred vision | 6 (40%) | 3 (42.9%) | 1 (25%) | ||||
| Trouble focusing | 2 (13.3%) | 0 | 0 | ||||
| Changes in colors perceived | 2 (13.3%) | 1 (14.3%) | 1 (25%) | ||||
| Other | 2 (13.3%) | 2 (28.6%) | 0 | ||||
| Auditory changes | 4 (1.7%) | 0 (0%) | 3 (3.5%) | ||||
| Trouble recognizing sounds | 4 (100%) | 0 | 3 (100%) | ||||
| Dizziness | 19 (8.0%) | 4 (5.6%) | 7 (8.2%) | ||||
| Impaired ability to balance | 4 (1.7%) | 1 (1.4%) | 2 (2.4%) | ||||
| Changes to your perception of space or perception of your body in space | 33 (13.8%) | 8 (11.3%) | 13 (15.3%) | ||||
| Headache | 6 (2.5%) | 2 (2.8%) | 2 (2.4%) | ||||
| Disorientation or confusion | 59 (24.7%) | 20 (28.2%) | 24 (28.2%) | ||||
| Unable to keep your train of thought/inability to think clearly | 7 (2.9%) | 1 (1.4%) | 3 (3.5%) | ||||
| A feeling like you needed to jumpstart your brain | 56 (23.4%) | 17 (23.9%) | 17 (20.0%) | ||||
| Other | 2 (0.8%) | 0 (0%) | 1 (1.2%) | ||||
| Reasons for SHAAKEs because of a concussion (select all) | .62 | ||||||
| Neck pain | 34 (14.2%) | 8 (11.3%) | 13 (15.3%) | ||||
| A feeling of a change in temperature or chills | 13 (5.4%) | 2 (2.8%) | 6 (7.1%) | ||||
| Emotional reaction to preceding event | 76 (31.8%) | 23 (32.4%) | 17 (20.0%) | ||||
| Pain to your face, scalp, or other part of your head that was not a headache | 39 (16.3%) | 14 (19.7%) | 12 (14.1%) | ||||
| Changes in your vision | 101 (42.3%) | 34 (47.9%) | 40 (47.1%) | .96 | |||
| Double vision | 27 (11.3%) | 11 (15.5%) | 12 (14.1%) | ||||
| Blurred vision | 72 (30.1%) | 24 (33.8%) | 27 (31.8%) | ||||
| Trouble focusing | 70 (29.3%) | 25 (35.2%) | 27 (31.8%) | ||||
| Changes in colors perceived | 13 (5.4%) | 5 (7.0%) | 6 (7.1%) | ||||
| Slanted vision | 10 (4.2%) | 4 (5.6%) | 3 (3.5%) | ||||
| Other | 11 (4.6%) | 2 (2.8%) | 3 (3.5%) | ||||
| Auditory changes | 47 (19.7%) | 11 (15.5%) | 25 (29.4%) | .95 | |||
| Ringing in your ears | 41 (17.2%) | 10 (14.1%) | 22 (25.9%) | ||||
| Deafness or impaired ability to hear sounds | 15 (6.3%) | 4 (5.6%) | 9 (10.6%) | ||||
| Trouble recognizing sounds | 17 (7.1%) | 5 (7.0%) | 9 (10.6%) | ||||
| Other | 1 (0.4%) | 0 (0.0%) | 0 (0.0%) | ||||
| Dizziness | 105 (43.9%) | 31 (43.7%) | 44 (51.8%) | ||||
| Impaired ability to balance | 59 (24.7%) | 19 (26.8%) | 24 (28.2%) | ||||
| Changes to your perception of space or perception of your body in space/proprioception | 97 (40.6%) | 24 (33.8%) | 38 (44.7%) | ||||
| Headache | 68 (28.5%) | 21 (29.6%) | 27 (31.8%) | ||||
| Disorientation or confusion | 136 (56.9%) | 42 (59.2%) | 47 (55.3%) | ||||
| Unable to keep your train of thought/inability to think clearly | 68 (28.5%) | 23 (32.4%) | 26 (30.6%) | ||||
| A feeling like you needed to jumpstart your brain | 100 (41.8%) | 30 (42.3%) | 32 (37.6%) | ||||
| Other | 1 (0.4%) | 0 (0.0%) | 1 (1.2%) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowinski, C.J.; Bureau, S.C.; Rhim, H.C.; Zafonte, R.D.; Cantu, R.C.; Daneshvar, D.H. Spontaneous Headshake after a Kinematic Event (SHAAKE): Evaluating the Utility of a Potential New Sign in the Diagnosis of Concussion. Diagnostics 2024, 14, 2314. https://doi.org/10.3390/diagnostics14202314
Nowinski CJ, Bureau SC, Rhim HC, Zafonte RD, Cantu RC, Daneshvar DH. Spontaneous Headshake after a Kinematic Event (SHAAKE): Evaluating the Utility of a Potential New Sign in the Diagnosis of Concussion. Diagnostics. 2024; 14(20):2314. https://doi.org/10.3390/diagnostics14202314
Chicago/Turabian StyleNowinski, Christopher J., Samantha C. Bureau, Hye Chang Rhim, Ross D. Zafonte, Robert C. Cantu, and Daniel H. Daneshvar. 2024. "Spontaneous Headshake after a Kinematic Event (SHAAKE): Evaluating the Utility of a Potential New Sign in the Diagnosis of Concussion" Diagnostics 14, no. 20: 2314. https://doi.org/10.3390/diagnostics14202314
APA StyleNowinski, C. J., Bureau, S. C., Rhim, H. C., Zafonte, R. D., Cantu, R. C., & Daneshvar, D. H. (2024). Spontaneous Headshake after a Kinematic Event (SHAAKE): Evaluating the Utility of a Potential New Sign in the Diagnosis of Concussion. Diagnostics, 14(20), 2314. https://doi.org/10.3390/diagnostics14202314