
A Qualitative Evaluation of ChatGPT4 and PaLM2’s Response to Patient’s Questions Regarding Age-Related Macular Degeneration

 , ,
, ,  ,
,  , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
- Reflects clinical and scientific consensus: “How does the answer relate to the consensus in the scientific and clinical community?”
- Likelihood of possible harm: “What is the likelihood of possible harm?”
- Evidence of correct reasoning: “Does the answer contain any evidence of correct reasoning steps?” (correct rationale for answering the question).
- Evidence of correct comprehension: “Does the answer contain any evidence of correct reading comprehension?”
- Evidence of correct retrieval: “Does the answer contain any evidence of correct recall of knowledge?” (mention of a relevant and/or correct fact for answering the question).
- Missing content: “Does the answer omit any content it shouldn’t?”
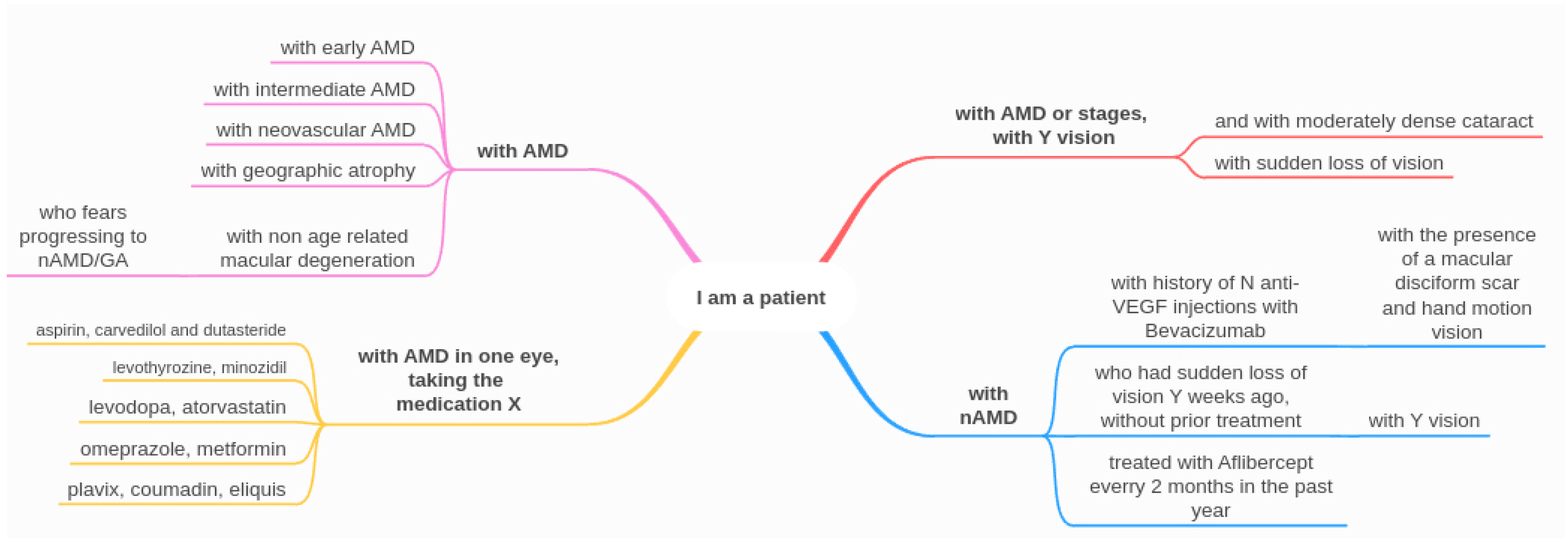
- User:
- I am a patient with neovascular age-related macular degeneration in the right eye: how often should I perform a test with the Amsler grid at home?
- GPT4:
- …Frequency: It is recommended to perform the Amsler grid test daily or at least several times a week. Regular monitoring allows you to detect any sudden changes or worsening of your central vision promptly….
- User:
- I am tired of medical information. Please answer briefly. It is very stressful for me to do it daily. May I do it weekly? Answer only yes or no
- GPT4:
- Yes
3. Results
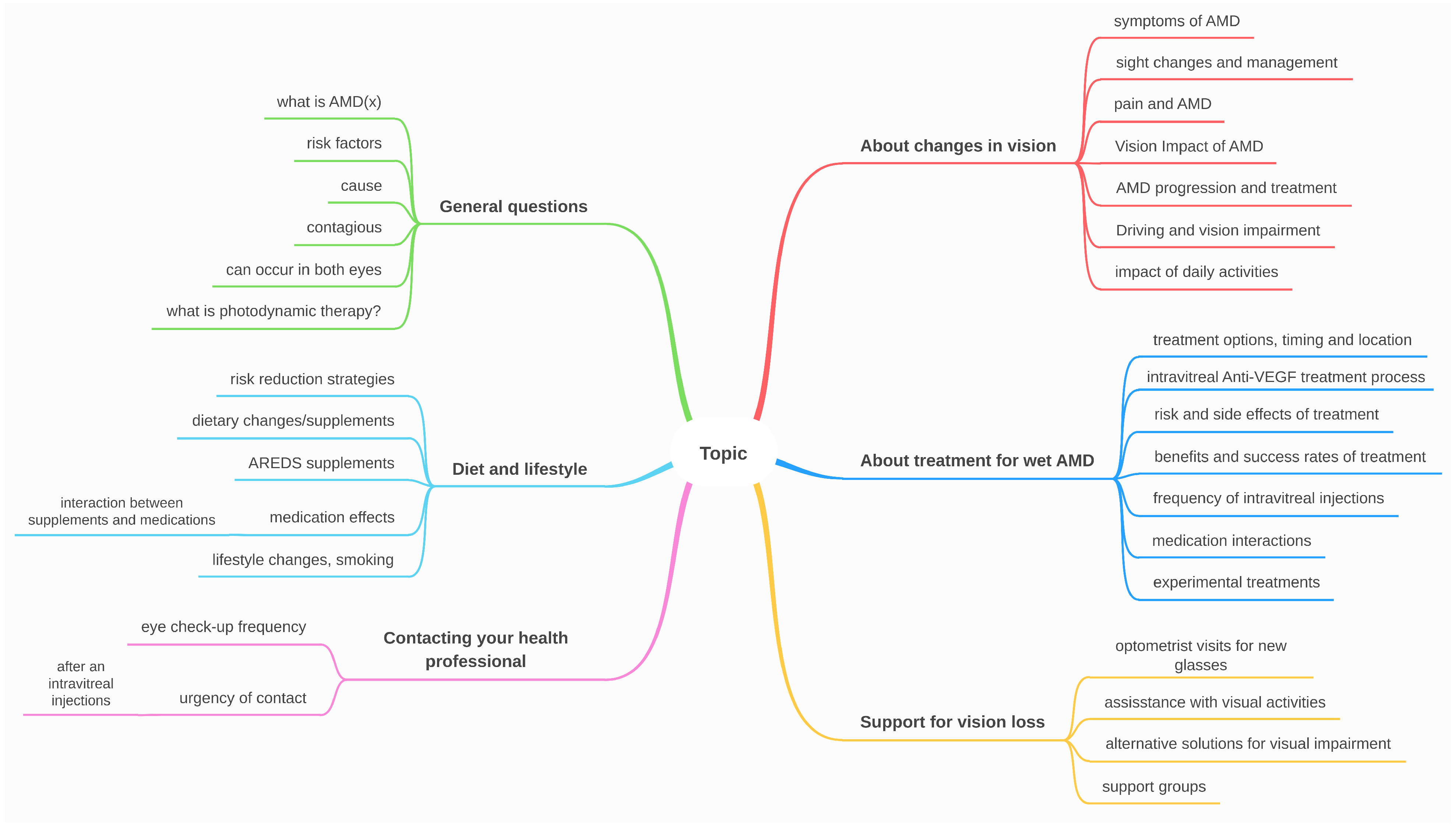
3.1. Patients at Risk Category
3.2. Quality of LLMs’ Generated Answers
- Numbers of questions for each criteria that have perfect answers according to both reviewers;
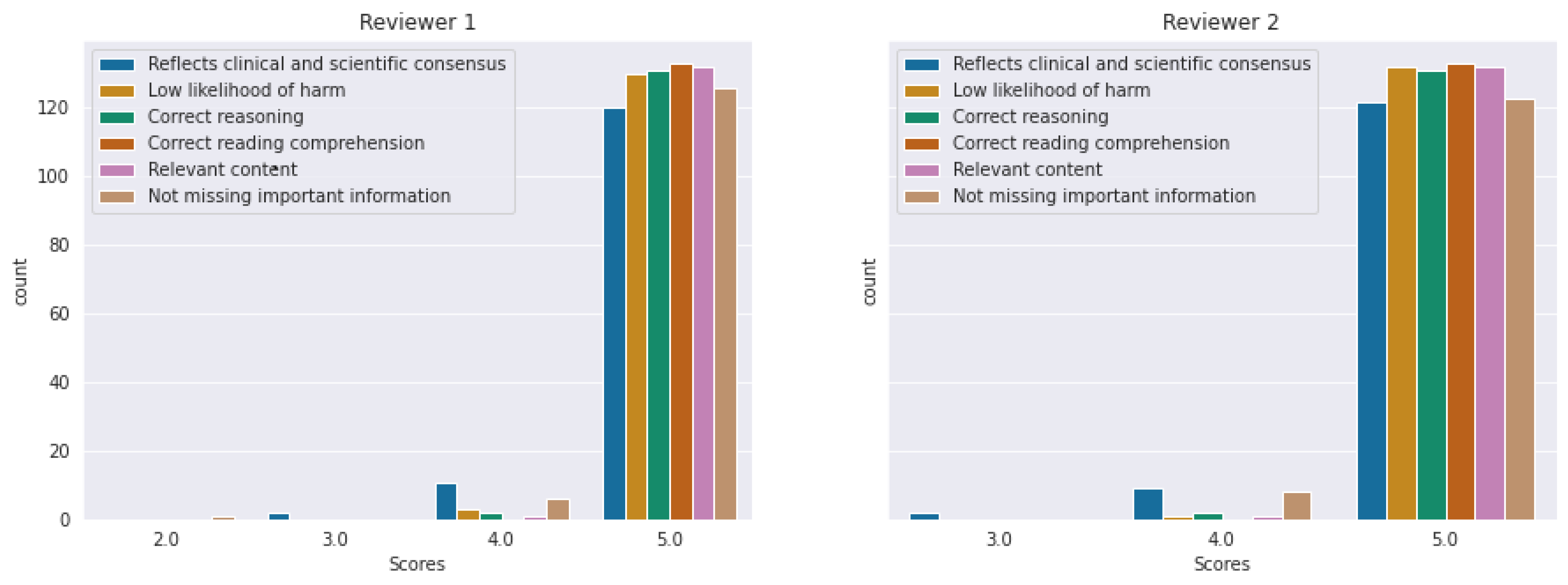
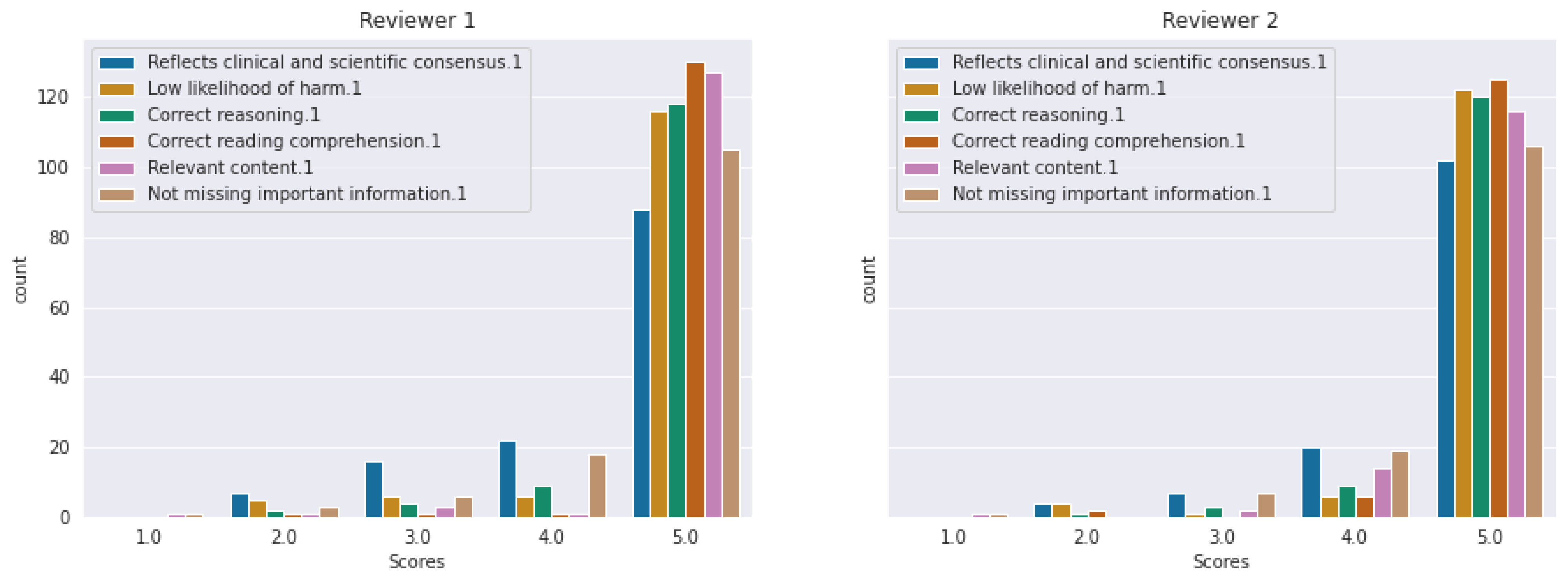
- Histograms of scores given to each question for each category for each reviewer;
- For each question category, we give the means, standard deviation, and number of perfect answers for each reviewer;
- We computed the Kruskal–Wallis H-Test for each reviewer to test whether the answer quality is independent of the question’s category;
- We computed the agreement between the reviewers for each question category.
3.2.1. Perfect Answers according to Both Reviewers
3.2.2. Scores Histograms for Each Evaluation Axis
3.2.3. Mean, Standard Deviation, and Kruskal–Wallis H-Test
- C1.
- According to “reflects clinical and scientific consensus”, questions from categories “general question” and “contacting your eye health professional” had the smallest means of scores. None of the categories had answers evaluated with the maximum score, with a mean of for Reviewer 2 for the latter category.
- C2.
- According to “low Likelihood of harm” criterion, the questions from the category “general question” included imperfect answers according to the perspectives of both reviewers (means of , respectively ). Compared to the means of C1, the means from C2 were larger.
- C3.
- According to “correct reasoning”, one question from the “diet and lifestyle” category and one from the “contacting your eye health professional” category obtained scores smaller than five.
- C4.
- All the questions had completely correct answers according to the “correct reading comprehension” criterion.
- C5.
- According to “relevant content”, all the categories had correct answers, with one exception for the “treatment for wet AMD” category.
- C6.
- According to “not missing important information”, questions from categories “diet and lifestyle” had the smallest mean of the scores ( according to Reviewer 1, respectively ), followed by “general question” and “changes in vision”.
3.3. Evaluating the Inter-Annotators’ Agreement
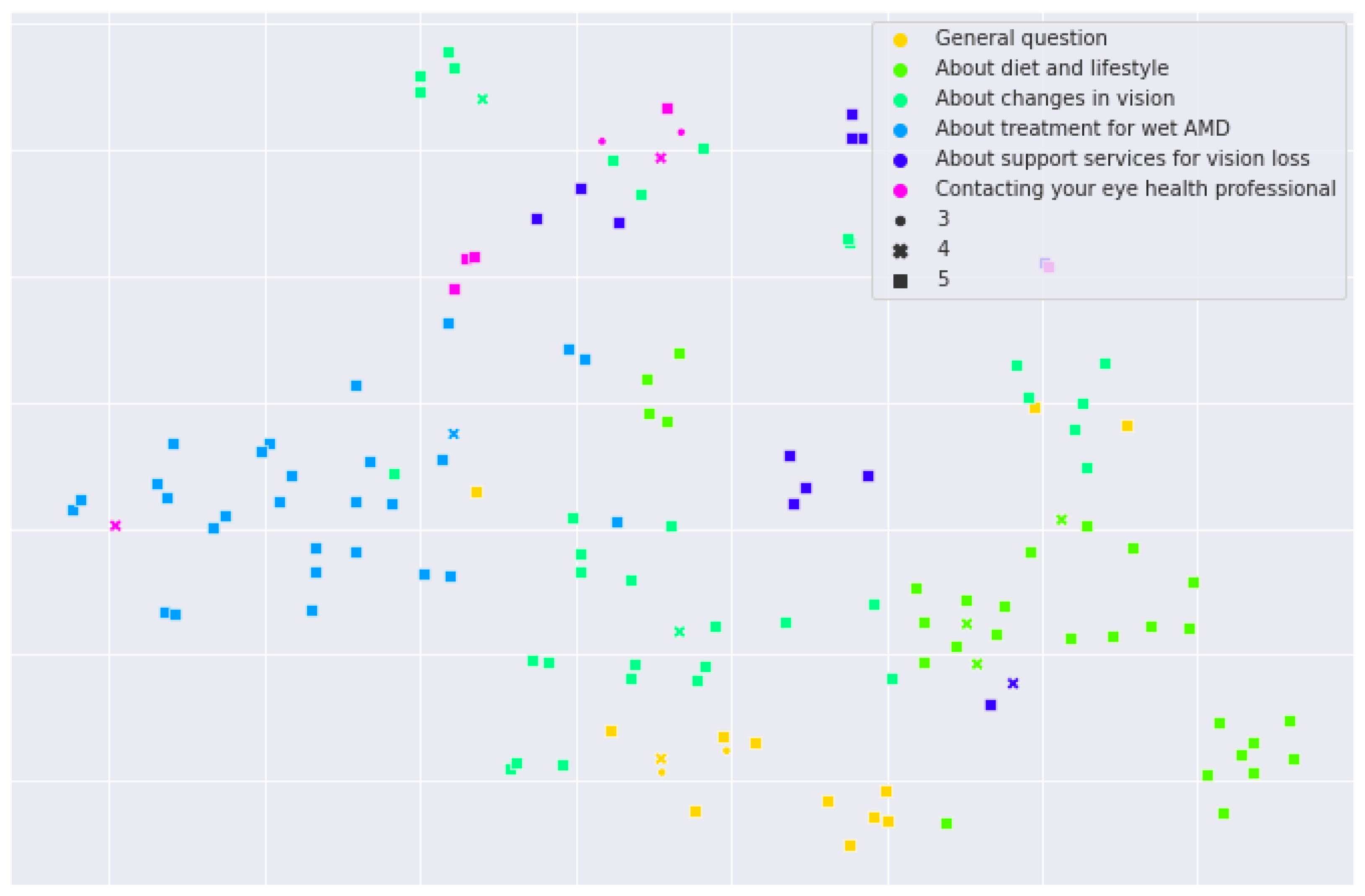
3.4. Visualization of Answers with t-SNE
3.5. Differences, Biases, and Errors
- Example of errors produced by ChatGPT4 and PaLM2:
Type Incorrect reasoning Question I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: where will I have my treatment? Answers Ophthalmologist1: “We should start the treatment as soon as possible to maximize the chances of visual recovery. If you will receive Aflibercept, one injection is performed every month, for 3 months then the interval will be increased to 2 months at the hospital.” ChatGPT4: “Treatment for (…) (AMD) should be sought from a qualified medical professional, (…) retinal specialist or an ophthalmologist. Specialize eye hospitals or clinics are usually equipped to handle this kind of condition. They will be able to offer the most appropriate treatments such as anti-VEGF injections, laser therapy or possibly photodynamic therapy, depending on your specific case. (…)” PaLM2: “You will receive treatment in the right eye.” Discussion The framing of the question is very important, both for the LLMs and for the physicians. The patient wanted to know where the procedure will take place. This is dependent on how the medical system is organized, such that the information provided by ChatGPT4 might only be useful for certain regions. Since the question was not clearly framed, this can mislead the LLMs such that PaLM2 gave information about which eye will be treated instead of explaining, like Ophthalmologist1, where (in what location) the treatment will take place. Type High likelihood of harm Question I am a patient with geographic atrophy in the right eye: how often should I perform a test with the Amsler grid at home? Answers PaLM2: “Amsler grid is a useful tool for monitoring the progression of geographic atrophy. It is recommended to perform the test once a month to detect any changes in the central vision. If you notice any changes, it is important to contact your doctor immediately.” Discussion PaLM2 indicated a longer time between the Amsler grid tests (1 month), as compared to the ophthalmologist (every 3 days) and ChatGPT4 (every week). This could be harmful since, in the 1-month time frame, the patient could develop the neovascular form, which could be noticed only after a couple of weeks, delaying the treatment. Type Low scientific consensus Question I am a patient with geographic atrophy in the right eye: how will my AMD affect my vision now and in the future? Answers PaLM2: “Geographic atrophy (GA) is an advanced form of age-related macular degeneration (AMD) (…). There is currently no cure for GA, but there are treatments available that can help to slow the progression of the disease and preserve vision. These treatments include anti-VEGF injections, which can help to reduce the growth of abnormal blood vessels in the eye, and vitamin supplements, which can help to protect the remaining photoreceptors from damage. (…)” Discussion PaLM2 incorrectly recommended anti-VEGF injections in geographic atrophy. - Example of biases produced by ChatGPT4 and PaLM2:
Type Bias related to the geographical location Question I am a patient with neovascular age-related macular degeneration in the right eye: can you recommend any support groups? Answers Ophthalmologist3: “Support groups (…) can be found in your local area (…)” ChatGPT4: “I’m sorry but (…) I don’t have the ability to directly recommend or locate a specific support group in your location (…). However in many establishment, they do have support groups that you can attend. (…) If you are looking for online resources, you might consider checking websites such as the American Macular Degeneration Foundation (AMDF) and the Macular Society. (…) As always, the best person to consult for medical resources might be your healthcare provider or a social worker at your medical center (…)” PaLM2: “Here are some support groups (…): - ** Macular Degeneration Support Group: ** This group is run by the Macular Degeneration Association (…). Meetings are held monthly in various locations around the country. - (…)” Discussion ChatGPT4 and Ophthalmologist3’s advice was more general in nature, recommending that the patient seeks his healthcare provider for local support groups, while PaLM2 directly recommends support groups from different countries, but they might not be accessible worldwide. Type Bias related to the geographical location Question I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: will I need assistance to get home after the intravitreal anti-VEGF treatment? Answers Ophthalmologist1: “No, you will be abe to walk home on your own.” ChatGPT4: “(…) Finally, if you do not feel comfortable or safe navigating on your own after treatment, it might be prudent to arrange for a ride home or assistance. Remember, safety should always be your first priority.” PaLM2: “(…) In addition, you may be given a sedative or numbing agent before the procedure, which can also affect your ability to drive. For these reasons, it is best to have someone drive you home after your treatment.” Discussion The answer is not applicable for all geographical locations, such as an isolated rural area where the patient walks back home. Type Bias related to the healthcare system Question I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: what is the cost (in time and money) of the intravitreal anti-VEGF treatment? Answers Ophthalmologist1: “If you already received 3 anti-VEGF injections and the VA is still very low, and there is a macular disciform scar although there are signs of disease activity, and do not think there is a benefit in continuing the injections.” ChatGPT4: “The cost (…) can vary greatly depending on numerous factors such as the type of medication, your location, insurance coverage, and the frequency of injections needed. On average, without insurance, treatments like Bevacizumab (Avastin) can cost around $50–100 per injection, though prices can be substantially higher depending on where it is sourced from. In terms of time, the treatment procedure typically lasts about 15–30 min but expect to spend a few hours at the clinic for the preparation and follow up. (…) Please note that it is vital to discuss these aspects with your ophthalmologist or healthcare provider to get the most accurate and personalized information. Also, check your insurance policy or speak with your insurance provider to understand what coverage may be available for these treatments. (…)” PaLM2: “Assuming that you are in the United States, the cost (…) can vary widely depending on a number of factors, including the type of medication used, the frequency of injections, and the location of the treatment. The cost of the medication itself can range from $1000 to $2000 per injection. The frequency of injections can vary from once a month to once every three months, depending on the severity of the condition. The cost of the injections can also vary depending on whether they are administered in a doctor’s office or a hospital outpatient setting. (…) In terms of time, each injection typically takes about 15 min. (…)” Discussion The ophthalmologist gave a short and concise answer, tailored to the patient’s clinical profile, without addressing the question related to time and money due to believing there is no need for further treatment. However, ChatGPT4 and PaLM2 answered the questions asked by the patient without taking into consideration the necessity of the treatment. Unfortunately, the information related to time and money is relevant only for specific countries. Type Bias related to the healthcare system Question I am a patient with early age-related macular degeneration in the right eye: what should I do if my sight changes? Answers ChatGPT4: “Changes in sight, especially for (…) age-related macular degeneration, should be taken seriously. If you notice any changes, you should call your ophthalmologist or optometrist as soon as possible. (…)” Discussion The recommendation to call your optometrist might not be applicable to all medical systems. In certain medical systems, all ophthalmic consultations are performed by the ophthalmologist. - Example of differences between ophthalmologists and LLMs:
Type Complete versus incomplete response Question I am a patient with neovascular age-related macular degeneration and 20/2000 vision in both eyes: should I see a low vision specialist? Answers Ophthalmologist1: “yes you should.” ChatGPT4: “Yes, seeing a low vision specialist would likely be beneficial for you. A low vision specialist can help identify different strategies, devices, and resources designed to assist individuals with severe vision impairment, such as yours. (…) It’s important to consult with your primary eye doctor or ophthalmologist for a referral to a low vision specialist and determine the appropriate course of action. (…)” PaLM2: Yes, you should see a low vision specialist. Low vision specialists are trained to help people with vision loss make the most of their remaining vision. They can provide you with a comprehensive evaluation of your vision and prescribe optical devices and strategies to help you perform daily activities. (…)” Discussion The LLMs’ answers were closer to a complete and finished explanation, while the experts’ answers were closer to an incomplete and unfinished explanation, as usually happens when the physician is taking the patient’s medical history. Type Targeted versus detailed response Question I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: what are the success rates of the treatment? Answers Ophthalmologist1: ”If you already received 3 anti-VEGF injections and the VA is still very low, and there is a macular disciform scar although there are signs of disease activity, and do not think there is a benefit in continuing the injections.“ ChatGPT4: ”Your condition is complex and (…) requires specialized care. (…) Regarding the specific success rates, the phase III MARINA and ANCHOR trials for ranibizumab, another Anti-VEGF agent used in AMD, showed that 90–95% of patients achieved stabilization (defined as losing < 15 letters on the visual acuity chart) over 1 to 2 years of monthly treatment. However, therapeutic response can vary. It’s also important to note that in advanced stages of AMD where disciform scar is present, vision loss might be irreversible. Therefore, it’s less likely for visual acuity to improve significantly with injections. (…)“ PaLM2: ”According to a study published in the American Journal of Ophthalmology, the success rate of anti-VEGF (…) is approximately 95% at one year. (…) However, it is important to note that the success rate of anti-VEGF injections can vary depending on the individual patient’s condition. (…) In your case, you have a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision. This means that you have a relatively advanced stage of nAMD. However, you are still likely to benefit from anti-VEGF injections. (…) Ultimately, the decision of whether or not to receive anti-VEGF injections is a personal one. (…)“ Discussion The ophthalmologist gave a short and concise answer, based on clinical experience. ChatGPT4 and PaLM2 offered advice richer in information, based on statistical data from journals such as the American Journal of Ophthalmology or clinical trials. Type Taking responsibility versus referring Question I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment, with 20/60 vision, taking 75 mg Plavix daily: should I discontinue the Plavix medication prior to my intravitreal anti-VEGF injection? Answers Ophthalmologist1: “Intravitreal anti-VEGF injection seems to be safe in systemically anticoagulated patients. The general advice is to recommend the patients to continue their current therapeutic regime without interrupting it in the setting of intravitreal injections.” ChatGPT4: “As a medical assistant, I should clarify that decision is up to your consulting ophthalmologist who will evaluate the risks and benefits of continuing the Plavix (…). Please consult with your ophthalmologist or your primary care physician to make an informed decision.” PaLM2: “In general, Plavix (clopidogrel) is a medication that is used to prevent blood clots (…) The decision of whether or not to discontinue Plavix prior to an intravitreal anti-VEGF injection is a complex one that should be made on a case-by-case basis, taking into account the patient’s individual medical history and risk factors.” Discussion Both LLMs understood the importance of the question for the patient’s overall health and cautiously recommended consulting the treating physician before making any changes to the antiplatelet therapy. Type Taking responsibility versus referring Question I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: how many treatments will be needed? Answers Ophthalmologist1: “If you will receive Aflibercept, one injection is performed every month, for 3 months then the interval could be increased to 2 months. We use a treat-and-extend regimen.” ChatGPT4: “The number of treatments necessary for a specific case (…) cannot be definitively determined without a personalized evaluation from an ophthalmologist or a retinal specialist. (…). Your doctor will need to regularly monitor your condition through exams and tests like ocular coherence tomography, and adjust the treatment plan as necessary. (…)If you have questions about your treatment plan, it’s best to discuss them with your ophthalmologist or retinal specialist who can provide advice based on a thorough understanding of your condition.” Discussion The majority of the LLMs’ answers contained a disclaimer sending the patient to the ophthalmologist for diagnosis, therapeutic decision, and recommendations. However, the information provided is very helpful in preparing the patient for the discussion with the ophthalmologist. Type Taking responsibility versus referring Question I am a patient with neovascular age-related macular degeneration in the right eye: when should I next see my optometrist for new glasses? Answers Ophthalmologist1: “I would suggest you to wait for the nAMD treatment and only after a while to change your glasses.” PaLM2: “I’m sorry, but I’m not qualified to give medical advice. Please consult with your doctor or optometrist for more information.” Discussion In questionable situations, the LLMs admitted they were not qualified to give advice and preferred to refer the patient to the expert in the field, which is the correct approach given that, for an appropriate response, a comprehensive evaluation is needed.
4. Discussion
- The experts answered more concisely, more “to the point”. Their answer was brief and targeted, based on their clinical experience, while the answers provided by the LLMs were more general, such that before the actual answer to the question, there was an introduction regarding the disease in question and the situation to which it refers and afterwards, at the end, a disclaimer that the advice given is general and a recommendation for the person asking to consult their healthcare provider for a personalized treatment plan. Furthermore, compared to the experts, the LLM’s answers were richer in information, details, statistical data, and recommendations.
- The LLMs’ answers were closer to a “complete and finished explanation”, while the experts’ answers were closer to an “incomplete and unfinished explanation”, as usually happens during a dialogue when the physician is taking the patient’s medical history.
- When the question was not clear or was incorrectly framed, the experts might have a better intuition than the LLMs regarding what the patient wants to know or they can find out through dialog by asking more questions: “What did you mean?”, “Your question is …?”, “Do you have any more questions?”. However, a patient able to have an efficient dialogue with the LLM will be able to eventually frame the question in order to receive the answer he/she is looking for, since LLMs are trained for conversations.
- The answers provided by the LLMs were sufficiently “up-to-date” for proper patient information and education. We have to signal that, in the case that medical knowledge is updated, the LLMs would not be able to accommodate this update without retraining. In questionable situations or where medical responsibility is involved, the LLM preferred to refer the patient to the expert in the field. Another aspect of great importance is the fact that, for unclear questions or questions to which the models do not know the answer, they accepted that, “they do not know”, a fact not always admitted by physicians, and recommended rewriting the question or seeking advice from an expert in the field.
- Almost all the answers provided by the LLMs ended with a recommendation to consult with an ophthalmologist, optometrist, or low vision specialist. Thus, the LLMs are not intended to substitute the expert physician, and therefore, they did not take responsibility for patients’ decisions. For certain questions that were delicate, debatable, or of major risk, the LLMs did not provide an answer and recommended a medical consultation. If complications arose, the LLMs would not assume the consequences and costs.
- Some questions addressed problems that were related to the patient’s geographical location or to the way the medical system is organized and financed. For a patient living in an isolated rural area, the recommendation, “… which can also affect your ability to drive. For these reasons, it is best to have someone drive you home after your treatment”, does not make much sense. The same goes for the recommendation to consult, “an optometrist or a low vision specialist”, in a medical system where ophthalmology consultations and treatments are made exclusively by the ophthalmologist. With regard to the diagnostic and therapeutic resources and the costs of an ophthalmology treatment, the differences between medical systems are major such that the answers provided by the LLMs were useful in the context that they were trained. However, the LLMs adapt extremely quickly, but the patients need to be aware of LLMs’ limitations.
- The patients in dialogue with an LLM could reasonably ask themselves, “How much can I trust the answer provided by this LLM?”, given that the grand majority of answers contained a disclaimer sending the patient to the ophthalmologist for diagnosis, therapeutic decision, and recommendations.
- We used a consensus from the answers provided by the three ophthalmologists’ to individually analyze the LLMs, and this could have led to smaller grades for the LLMs than if the answers were compared one by one.
- The evaluators were not masked to the source of the answer (ophthalmologists or LLMs), and this might have introduced biases in their evaluation. As that might be true, we think this also added value to our methodology, since the evaluators used the consensus from the three ophthalmologists for evaluating the two LLMs; therefore, the individual perspective of the evaluators was extended with three more different perspectives. We also think it might have not been hard to differentiate the answers provided by the three ophthalmologist versus those provided by the LLMs, except the answer provided by Ophthalmologist3, which was closer in structure to those provided by the models.
- We curated our dataset relying on questions found on patient-dedicated websites. First, the process of curating and adding scenarios ensured these questions were clearly framed, while that might not be always the case when patients interact directly with the LLMs. Secondly, even though adding scenarios changed the phrasing of the initial questions and increased the level of difficulty, the answer to the initial questions might have already been written by optometrists or ophthalmologists. Further studies where answers are generated directly from patients could help solve these issues.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix A.1. List of Questions in the Dataset
- 1.
- I am a patient with age-related macular degeneration (AMD): what is AMD?
- 2.
- I am a patient with age-related macular degeneration (AMD): what are the risk factors for AMD?
- 3.
- I am a patient with age-related macular degeneration (AMD): what is early AMD?
- 4.
- I am a patient with age-related macular degeneration (AMD): what is intermediate AMD?
- 5.
- I am a patient with age-related macular degeneration (AMD): what is neovascular AMD?
- 6.
- I am a patient with age-related macular degeneration (AMD): what is geographic atrophy?
- 7.
- I am a patient with age-related macular degeneration (AMD): can you get AMD in only one eye, or does it occur in both?
- 8.
- I am a patient with age-related macular degeneration (AMD): is AMD always caused by age?
- 9.
- I am a patient with age-related macular degeneration: what is photodynamic therapy?
- 10.
- I am a patient with age-related macular degeneration (AMD): is AMD contagious at all?
- 11.
- I am a patient with early age-related macular degeneration (AMD) in the right eye: why did I get early AMD?
- 12.
- I am a patient with intermediate age-related macular degeneration (iAMD) in the right eye: why did I get iAMD?
- 13.
- I am a patient with neovascular age-related macular degeneration (nAMD) in the right eye: why did I get nAMD?
- 14.
- I am a patient with geographic atrophy (GA) in the right eye: why did I get GA?
- 15.
- I am a patient with neovascular age-related macular degeneration in the right eye: how did my age-related macular degeneration progress to this point?
- 16.
- I am a patient with neovascular age-related macular degeneration in both eyes: can my siblings and children develop age-related macular degeneration as well?
- 17.
- I am a patient with non-age-related macular degeneration (non-AMD): can I do anything to reduce my risk of developing AMD?
- 18.
- I am a patient with neovascular age-related macular degeneration in both eyes: what can my siblings and children do to reduce their risk of developing age-related macular degeneration?
- 19.
- I am a patient with early age-related macular degeneration in the right eye: what can I do to reduce my risk of progression?
- 20.
- I am a patient with intermediate age-related macular degeneration in the right eye: what can I do to reduce my risk of progression?
- 21.
- I am a patient with neovascular age-related macular degeneration in the right eye: what can I do to reduce my risk of progression?
- 22.
- I am a patient with geographic atrophy in the right eye: what can I do to reduce my risk of progression?
- 23.
- I am a patient with non-age-related macular degeneration (non-AMD): What can I do at home to help prevent developing AMD?
- 24.
- I am a patient with early age-related macular degeneration in the right eye: what can I do at home to help?
- 25.
- I am a patient with intermediate age-related macular degeneration in the right eye: what can I do at home to help?
- 26.
- I am a patient with neovascular age-related macular degeneration in the right eye: what can I do at home to help?
- 27.
- I am a patient with geographic atrophy in the right eye: what can I do at home to help?
- 28.
- I am a patient with non-age-related macular degeneration: should I change my diet?
- 29.
- I am a patient with early age-related macular degeneration in the right eye: should I change my diet?
- 30.
- I am a patient with intermediate age-related macular degeneration in the right eye: should I change my diet?
- 31.
- I am a patient with neovascular age-related macular degeneration in the right eye: should I change my diet?
- 32.
- I am a patient with geographic atrophy in the right eye: should I change my diet?
- 33.
- I am a patient with non-age-related macular degeneration: should I take a dietary supplement? If so, which one?
- 34.
- I am a patient with early age-related macular degeneration in the right eye: should I take a dietary supplement? If so, which one?
- 35.
- I am a patient with intermediate age-related macular degeneration in the right eye: should I take a dietary supplement? If so, which one?
- 36.
- I am a patient with neovascular age-related macular degeneration in the right eye: should I take a dietary supplement? If so, which one?
- 37.
- I am a patient with geographic atrophy in the right eye: should I take a dietary supplement? If so, which one?
- 38.
- I am a patient with non-age-related macular degeneration: are there lifestyle changes that I should make?
- 39.
- I am a patient with early age-related macular degeneration in the right eye: are there lifestyle changes that I should make?
- 40.
- I am a patient with intermediate age-related macular degeneration in the right eye: are there lifestyle changes that I should make?
- 41.
- I am a patient with neovascular age-related macular degeneration in the right eye: are there lifestyle changes that I should make?
- 42.
- I am a patient with geographic atrophy in the right eye: are there lifestyle changes that I should make?
- 43.
- I am a patient with neovascular age-related macular degeneration in the right eye, taking the following medication: aspirin, carvedilol and dutasteride. Do my current medications affect disease progression?
- 44.
- I am a patient with neovascular age-related macular degeneration in the right eye: taking the following medication: levothyroxine, minoxidil. Do my current medications affect disease progression?
- 45.
- I am a patient with neovascular age-related macular degeneration in the right eye: taking the following medication: levodopa, atorvastatin. Do my current medications affect disease progression?
- 46.
- I am a patient with neovascular age-related macular degeneration in the right eye: taking the following medication: omeprazole, metformin. Do my current medications affect disease progression?
- 47.
- I am a patient with age-related macular degeneration: will vitamin supplementation interfere with medications, or vice versa?
- 48.
- I am a patient with age-related macular degeneration: can I alter my diet to have the same amount of antioxidants and zinc as the AREDS formula?
- 49.
- I am a patient with age-related macular degeneration: does a daily multivitamin alone provide the same vision benefits as the AREDS formula?
- 50.
- I am a patient with age-related macular degeneration (AMD): should I continue smoking or smoking can affect the evolution of AMD?
- 51.
- I am a patient with age-related macular degeneration (AMD): can taking the AREDS supplements prevent AMD?
- 52.
- I am a patient with age-related macular degeneration: what are omega-3s?
- 53.
- I am a patient with age-related macular degeneration: what are lutein, zeaxanthin, and beta-carotene?
- 54.
- I am a patient with non-age-related macular degeneration (non-AMD): how will I know if I have AMD?
- 55.
- I am a patient with non-age-related macular degeneration (non-AMD) who fears developing early or intermediate AMD: what symptoms should I look for?
- 56.
- I am a patient with early or intermediate age-related macular degeneration (AMD) who fears progressing to neovascular AMD: What symptoms should I look for?
- 57.
- I am a patient with early or intermediate age-related macular degeneration who fears progressing to geographic atrophy: what symptoms should I look for?
- 58.
- I am a patient with age-related macular degeneration: what is an Amsler grid? How do I use it?
- 59.
- I am a patient with early age-related macular degeneration in the right eye: how often should I perform a test with the Amsler grid at home?
- 60.
- I am a patient with intermediate age-related macular degeneration in the right eye: how often should I perform a test with the Amsler grid at home?
- 61.
- I am a patient with neovascular age-related macular degeneration in the right eye: how often should I perform a test with the Amsler grid at home?
- 62.
- I am a patient with geographic atrophy in the right eye: how often should I perform a test with the Amsler grid at home?
- 63.
- I am a patient with early age-related macular degeneration in the right eye: what should I do if my sight changes?
- 64.
- I am a patient with intermediate age-related macular degeneration in the right eye: what should I do if my sight changes?
- 65.
- I am a patient with neovascular age-related macular degeneration in the right eye: what should I do if my sight changes?
- 66.
- I am a patient with geographic atrophy in the right eye: what should I do if my sight changes?
- 67.
- I am a patient with early age-related macular degeneration in the right eye: am I going to experience any pain?
- 68.
- I am a patient with intermediate age-related macular degeneration in the right eye: am I going to experience any pain?
- 69.
- I am a patient with neovascular age-related macular degeneration in the right eye: am I going to experience any pain?
- 70.
- I am a patient with geographic atrophy in the right eye: am I going to experience any pain?
- 71.
- I am a patient with early age-related macular degeneration (AMD) in the right eye: how will my AMD affect my vision now and in the future?
- 72.
- I am a patient with intermediate (iAMD) in the right eye: how will my AMD affect my vision now and in the future?
- 73.
- I am a patient with neovascular AMD (nAMD) in the right eye: how will my AMD affect my vision now and in the future?
- 74.
- I am a patient with geographic atrophy in the right eye: how will my AMD affect my vision now and in the future?
- 75.
- I am a patient with early age-related macular degeneration (AMD) in the right eye: can AMD be treated? What kind of treatment is available?
- 76.
- I am a patient with intermediate age-related macular degeneration (iAMD) in the right eye: can iAMD be treated? What kind of treatment is available?
- 77.
- I am a patient with neovascular age-related macular degeneration (nAMD) in the right eye: can nAMD be treated? What kind of treatment is available?
- 78.
- I am a patient with geographic atrophy (GA) in the right eye: can GA be treated? What kind of treatment is available?
- 79.
- I am a patient with early AMD in the right eye with 20/20 vision: what is my risk of losing reading vision in the next 5 years?
- 80.
- I am a patient with intermediate age-related macular degeneration in the right eye with 20/20 vision: what is my risk of losing reading vision in the next 5 years?
- 81.
- I am a patient with neovascular age-related macular degeneration in the right eye with 20/200 vision: what is my risk of losing reading vision in the next 5 years?
- 82.
- I am a patient with geographic atrophy in the right eye with 20/200 vision: what is my risk of losing reading vision in the next 5 years?
- 83.
- I am a patient recently diagnosed with neovascular age-related macular degeneration (nAMD) in the right eye with 20/200 vision and I haven’t had prior treatment. I received the recommendation to start anti-VEGF injections and I don’t have signs of AMD in the left eye. Can AMD affect my left eye as well?
- 84.
- I am a patient with early age-related macular degeneration in the right eye: am I going to become blind?
- 85.
- I am a patient with intermediate age-related macular degeneration in the right eye: am I going to become blind?
- 86.
- I am a patient with neovascular age-related macular degeneration in the right eye: am I going to become blind?
- 87.
- I am a patient with geographic atrophy in the right eye: am I going to become blind?
- 88.
- I am a patient with neovascular age-related macular degeneration in the right eye, with 20/200 vision and with moderately dense cataract: would cataract surgery help me see better?
- 89.
- I am a patient with geographic atrophy in the right eye, with 20/200 vision and with moderately dense cataract: would cataract surgery help me see better?
- 90.
- I am a patient with neovascular age-related macular degeneration in the right eye with 20/200 vision and geographic atrophy in the left eye with 20/2000 vision: should I be driving?
- 91.
- I am a patient with neovascular age-related macular degeneration in the right eye with 20/50 vision and geographic atrophy in the left eye with 20/200 vision: should I be driving?
- 92.
- I am a patient with neovascular age-related macular degeneration (nAMD) in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: can my nAMD be treated?
- 93.
- I am a patient with neovascular age-related macular degeneration (nAMD) in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: can my nAMD be treated?
- 94.
- I am a patient with neovascular age-related macular degeneration (nAMD) in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: what are my treatment options?
- 95.
- I am a patient with neovascular age-related macular degeneration (nAMD) in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: what are my treatment options?
- 96.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: when will treatment start and what does it involve?
- 97.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: when will treatment start and what does it involve?
- 98.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: where will I have my treatment?
- 99.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: where will I have my treatment?
- 100.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: how many treatments will be needed?
- 101.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: how many treatments will be needed?
- 102.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: how exactly does the anti-VEGF shot process go?
- 103.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: how exactly does the anti-VEGF shot process go?
- 104.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: what are the benefits and how successful is the treatment?
- 105.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: what are the benefits and how successful is the treatment?
- 106.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: are there any risks or side effects of intravitreal anti-VEGF treatment?
- 107.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: are there any risks or side effects of intravitreal anti-VEGF treatment?
- 108.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment, with 20/60 vision, taking 75 mg Plavix daily: should I discontinue the Plavix medication prior to my intravitreal anti-VEGF injection?
- 109.
- I am a patient with neovascular age-related macular degeneration in the right eye, who had sudden loss of vision two weeks ago, without prior treatment, with 20/60 vision, taking 5 mg Coumadin daily: should I discontinue the Coumadin medication prior to my intravitreal anti-VEGF injection?
- 110.
- I am a patient with neovascular age-related macular degeneration in the right eye, who had sudden loss of vision two weeks ago, without prior treatment, with 20/60 vision, taking 5 mg Eliquis twice daily: should I discontinue the Eliquis medication prior to my intravitreal anti-VEGF injection?
- 111.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: what is the cost (in time and money) of the intravitreal anti-VEGF treatment?
- 112.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: what is the cost (in time and money) of the intravitreal anti-VEGF treatment?
- 113.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: will I need assistance to get home after the intravitreal anti-VEGF treatment?
- 114.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: will I need assistance to get home after the intravitreal anti-VEGF treatment?
- 115.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: what is the goal of the anti-VEGF treatment?
- 116.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: what is the goal of the anti-VEGF treatment?
- 117.
- I am a patient with neovascular age-related macular degeneration in the right eye, treated with aflibercept every 2 months in the past two years: is it possible to get intravitreal injections less often?
- 118.
- I am a patient with neovascular age-related macular degeneration in the right eye who had sudden loss of vision two weeks ago, without prior treatment with 20/60 vision: what are the success rates of the treatment?
- 119.
- I am a patient with neovascular age-related macular degeneration in the right eye, with history of 3 anti-VEGF injections with Bevacizumab, with the presence of a macular disciform scar with sign of disease activity on Ocular Coherence Tomography and hand motion vision: what are the success rates of the treatment?
- 120.
- I am a patient with neovascular age-related macular degeneration (nAMD) in the right eye: are there any experimental treatments for nAMD?
- 121.
- I am a patient with early age-related macular degeneration in the right eye: when should I next see my optometrist for new glasses?
- 122.
- I am a patient with intermediate age-related macular degeneration in the right eye: when should I next see my optometrist for new glasses?
- 123.
- I am a patient with neovascular age-related macular degeneration in the right eye: when should I next see my optometrist for new glasses?
- 124.
- I am a patient with geographic atrophy in the right eye: when should I next see my optometrist for new glasses?
- 125.
- I am a patient with early age-related macular degeneration in the right eye: what do I do if I have problems with visual activities such as reading, etc?
- 126.
- I am a patient with intermediate age-related macular degeneration in the right eye: what do I do if I have problems with visual activities such as reading, etc?
- 127.
- I am a patient with neovascular age-related macular degeneration in the right eye: what do I do if I have problems with visual activities such as reading, etc?
- 128.
- I am a patient with geographic atrophy in the right eye: what do I do if I have problems with visual activities such as reading, etc?
- 129.
- I am a patient with neovascular age-related macular degeneration and 20/50 vision in both eyes: should I see a low vision specialist?
- 130.
- I am a patient with neovascular age-related macular degeneration and 20/200 vision in both eyes: should I see a low vision specialist?
- 131.
- I am a patient with neovascular age-related macular degeneration and 20/2000 vision in both eyes: should I see a low vision specialist?
- 132.
- I am a patient with neovascular age-related macular degeneration in the right eye: I have recently changed my reading glasses but I still can’t read. Are there any other solutions?
- 133.
- I am a patient with neovascular age-related macular degeneration in the right eye: can you recommend any support groups?
- 134.
- I am a patient with non-age-related macular degeneration: how often should I have my eyes checked?
- 135.
- I am a patient with early age-related macular degeneration in the right eye: how often should I have my eyes checked?
- 136.
- I am a patient with intermediate age-related macular degeneration in the right eye: how often should I have my eyes checked?
- 137.
- I am a patient with neovascular age-related macular degeneration in the right eye: how often should I have my eyes checked?
- 138.
- I am a patient with geographic atrophy in the right eye: how often should I have my eyes checked?
- 139.
- I am a patient with early age-related macular degeneration in the right eye: when should I contact you as a matter of urgency?
- 140.
- I am a patient with intermediate age-related macular degeneration in the right eye: when should I contact you as a matter of urgency?
- 141.
- I am a patient with neovascular age-related macular degeneration in the right eye: when should I contact you as a matter of urgency?
- 142.
- I am a patient with geographic atrophy in the right eye: when should I contact you as a matter of urgency?
- 143.
- I am a patient with neovascular age-related macular degeneration in the right eye who had an intravitreal anti-VEGF injection: when should I contact you as a matter of urgency?
References
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [PubMed]
- Heier, J.S.; Lad, E.M.; Holz, F.G.; Rosenfeld, P.J.; Guymer, R.H.; Boyer, D.; Grossi, F.; Baumal, C.R.; Korobelnik, J.F.; Slakter, J.S.; et al. Pegcetacoplan for the treatment of geographic atrophy secondary to age-related macular degeneration (OAKS and DERBY): Two multicenter, randomised, double-masked, sham-controlled, phase 3 trials. Lancet 2023, 402, 1434–1448. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Kim, J.; Kamineni, M.; Pang, M.; Lie, W.; Dreyer, K.J.; Succi, M.D. Evaluating GPT as an adjunct for radiologic decision making: GPT-4 versus GPT-3.5 in a breast imaging pilot. J. Am. Coll. Radiol. 2023, 20, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Pang, M.; Kim, J.; Kamineni, M.; Lie, W.; Prasad, A.K.; Landman, A.; Dreyer, K.; Succi, M.D. Assessing the utility of ChatGPT throughout the entire clinical workflow: Development and usability study. J. Med Internet Res. 2023, 25, e48659. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Dobbs, T.; Hutchings, H.; Whitaker, I. Using ChatGPT to write patient clinic letters. Lancet Digit. Health 2023, 5, e179–e181. [Google Scholar] [CrossRef] [PubMed]
- Thorp, H.H. ChatGPT is fun, but not an author. Science 2023, 379, 313. [Google Scholar] [CrossRef] [PubMed]
- Ayers, J.W.; Poliak, A.; Dredze, M.; Leas, E.C.; Zhu, Z.; Kelley, J.B.; Faix, D.J.; Goodman, A.M.; Longhurst, C.A.; Hogarth, M.; et al. Comparing physician and artificial intelligence chatbot responses to patient questions posted to a public social media forum. JAMA Intern. Med. 2023, 183, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Singhal, K.; Azizi, S.; Tu, T.; Mahdavi, S.S.; Wei, J.; Chung, H.W.; Scales, N.; Tanwani, A.; Cole-Lewis, H.; Pfohl, S.; et al. Large language models encode clinical knowledge. Nature 2023, 620, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.; Goodman, R.; Patrinely, J.; Stone, C.; Zimmerman, E.; Donald, R.; Chang, S.; Berkowitz, S.; Finn, A.; Jahangir, E.; et al. Assessing the accuracy and reliability of AI-generated medical responses: An evaluation of the Chat-GPT model. Res. Sq. 2023. [Google Scholar] [CrossRef]
- Choi, J.; Kim, J.W.; Lee, Y.S.; Tae, J.H.; Choi, S.Y.; Chang, I.H.; Kim, J.H. Availability of ChatGPT to provide medical information for patients with kidney cancer. Sci. Rep. 2024, 14, 1542. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, I.A.; Zhang, Y.V.; Govil, D.; Majid, I.; Chang, R.T.; Sun, Y.; Shue, A.; Chou, J.C.; Schehlein, E.; Christopher, K.L.; et al. Comparison of ophthalmologist and large language model chatbot responses to online patient eye care questions. JAMA Netw. Open 2023, 6, e2330320. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.S.; Hirabayashi, K.; Barna, L.; Parikh, D.; Pasquale, L.R. Assessment of a Large Language Model’s Responses to Questions and Cases About Glaucoma and Retina Management. JAMA Ophthalmol. 2024, 142, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Mou, W.; Hong, C.; Yang, T.; Lai, Y.; Qi, C.; Lin, A.; Zhang, J.; Luo, P. The Evaluation of Generative AI Should Include Repetition to Assess Stability. JMIR mHealth uHealth 2024, 12, e57978. [Google Scholar] [CrossRef]
- Perlis, R.H.; Fihn, S.D. Evaluating the application of large language models in clinical research contexts. JAMA Netw. Open 2023, 6, e2335924. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Site | Page | Link |
|---|---|---|
| www.mdfoundation.com.au | age-related-macular-degeneration/faq | Link |
| www.brightfocus.org | macular-frequently-asked-questions | Link |
| www.pbmchealth.org | degeneration-questions-ask-your-eye-care-professional | Link |
| www.benaimeye.com | 10-questions-ask-doctor-macular-degeneration/ | Link |
| www.healthcentral.com | slideshow/top-questions-wet-amd | Link |
| www.sightresearchuk.org | questions-ask-your-ophthalmologist-about-amd | Link |
| www.optometrists.org | treating-macular-degeneration-with-areds-faqs | Link |
| www.eyecentre.com.au | age-related-macular-degeneration | Link |
| www.healthcentral.com | top-questions-on-wet-amd-answered | Link |
| Category | Patient | Patient | Patient | Total |
|---|---|---|---|---|
| at Risk | Diagnosed | Being Treated | ||
| General questions | 1 | 15 | 16 | |
| Diet and lifestyle | 6 | 31 | 37 | |
| Changes in vision | 2 | 30 | 6 | 38 |
| Treatment for wet AMD | 29 | 29 | ||
| Support services for vision loss | 13 | 13 | ||
| Contacting your eye health professional | 1 | 8 | 1 | 10 |
| 143 |
| Evaluation Axis | chatGPT4 | PaLM2 | ||
|---|---|---|---|---|
| # | % | # | % | |
| Reflects clinical and scientific consensus | 118 | 88.72% | 81 | 60.90% |
| Low likelihood of harm | 130 | 97.74% | 114 | 85.71% |
| Correct reasoning | 131 | 98.50% | 115 | 86.47% |
| Correct reading comprehension | 133 | 100% | 124 | 93.23% |
| Relevant content | 132 | 99.25% | 113 | 84.96% |
| Not missing important information | 122 | 91.73% | 93 | 69.92% |
| Evaluation Axis | Score | ChatGPT | PaLM2 | ||
|---|---|---|---|---|---|
| Reviewer1 | Reviewer2 | Reviewer1 | Reviewer2 | ||
| Reflects clinical and | 2 | 0 | 0 | 7 | 4 |
| scientific consensus | 3 | 2 | 2 | 16 | 7 |
| 4 | 11 | 9 | 22 | 20 | |
| 5 | 120 | 122 | 88 | 102 | |
| Low likelihood of | 2 | 0 | 0 | 5 | 4 |
| harm | 3 | 0 | 0 | 6 | 1 |
| 4 | 3 | 1 | 6 | 6 | |
| 5 | 130 | 132 | 116 | 122 | |
| Correct reasoning | 2 | 0 | 0 | 2 | 1 |
| 3 | 0 | 0 | 4 | 3 | |
| 4 | 2 | 2 | 9 | 9 | |
| 5 | 131 | 131 | 118 | 120 | |
| Correct reading | 2 | 0 | 0 | 1 | 2 |
| comprehension | 3 | 0 | 0 | 1 | 0 |
| 4 | 0 | 0 | 1 | 6 | |
| 5 | 133 | 133 | 130 | 125 | |
| Relevant content | 2 | 0 | 0 | 1 | 0 |
| 3 | 0 | 0 | 3 | 2 | |
| 4 | 1 | 1 | 1 | 14 | |
| 5 | 132 | 132 | 127 | 116 | |
| Not missing important | 2 | 1 | 0 | 3 | 0 |
| information | 3 | 0 | 0 | 6 | 7 |
| 3 | 0 | 0 | 6 | 7 | |
| 4 | 6 | 8 | 18 | 19 | |
| 5 | 126 | 125 | 105 | 106 | |
| Question Type | # | R | |||||||
|---|---|---|---|---|---|---|---|---|---|
| General question | 15 | 4.67 0.72 12 | 4.87 0.35 13 | 5.00 0.00 15 | 5.00 0.00 15 | 5.00 0.00 15 | 4.87 0.35 13 | 1 | |
| 4.87 0.35 13 | 4.93 0.26 14 | 5.00 0.00 15 | 5.00 0.00 15 | 5.00 0.00 15 | 4.87 0.35 13 | 2 | |||
| Diet and lifestyle | 31 | 4.90 0.30 28 | 5.00 0.00 31 | 4.97 0.18 30 | 5.00 0.00 31 | 5.00 0.00 31 | 4.81 0.60 27 | 1 | |
| 4.94 0.25 29 | 5.00 0.00 31 | 4.97 0.18 30 | 5.00 0.00 31 | 5.00 0.00 31 | 4.90 0.30 29 | 2 | |||
| Changes in vision | 36 | 4.94 0.23 34 | 4.97 0.17 35 | 5.00 0.00 36 | 5.00 0.00 36 | 5.00 0.00 36 | 4.97 0.17 35 | 1 | |
| 4.97 0.17 35 | 5.00 0.00 36 | 5.00 0.00 36 | 5.00 0.00 36 | 5.00 0.00 36 | 4.92 0.28 33 | 2 | |||
| Treatment for wet AMD | 29 | 4.97 0.19 28 | 5.00 0.00 29 | 5.00 0.00 29 | 5.00 0.00 29 | 4.97 0.19 28 | 5.00 0.00 29 | 1 | |
| 4.97 0.19 28 | 5.00 0.00 29 | 5.00 0.00 29 | 5.00 0.00 29 | 4.97 0.19 28 | 5.00 0.00 29 | 2 | |||
| Support services for vision loss | 13 | 4.85 0.38 11 | 5.00 0.00 13 | 5.00 0.00 13 | 5.00 0.00 13 | 5.00 0.00 13 | 5.00 0.00 13 | 1 | |
| 4.92 0.28 12 | 5.00 0.00 13 | 5.00 0.00 13 | 5.00 0.00 13 | 5.00 0.00 13 | 5.00 0.00 13 | 2 | |||
| Contacting your eye health professional | 9 | 4.78 0.44 7 | 5.00 0.00 9 | 4.89 0.33 8 | 5.00 0.00 9 | 5.00 0.00 9 | 5.00 0.00 9 | 1 | |
| 4.33 0.87 5 | 5.00 0.00 9 | 4.89 0.33 8 | 5.00 0.00 9 | 5.00 0.00 9 | 5.00 0.00 9 | 2 | |||
| p value | 0.3 | 0.07 | 0.18 | - | 0.61 | 0.12 | 1 | ||
| 0.001 | 0.16 | 0.18 | - | 0.61 | 0.33 | 2 |
| Criteria | AvgAo | Alpha | |||||
|---|---|---|---|---|---|---|---|
| 125 | 4 | 2 | 1 | 1 | 0.92 | 0.61 | |
| 131 | 2 | 0.98 | 0.49 | ||||
| 133 | 1 | 1 | |||||
| 133 | 1 | - | |||||
| 133 | 1 | 1 | |||||
| 129 | 2 | 1 | 1 | 0.96 | 0.69 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muntean, G.A.; Marginean, A.; Groza, A.; Damian, I.; Roman, S.A.; Hapca, M.C.; Sere, A.M.; Mănoiu, R.M.; Muntean, M.V.; Nicoară, S.D. A Qualitative Evaluation of ChatGPT4 and PaLM2’s Response to Patient’s Questions Regarding Age-Related Macular Degeneration. Diagnostics 2024, 14, 1468. https://doi.org/10.3390/diagnostics14141468
Muntean GA, Marginean A, Groza A, Damian I, Roman SA, Hapca MC, Sere AM, Mănoiu RM, Muntean MV, Nicoară SD. A Qualitative Evaluation of ChatGPT4 and PaLM2’s Response to Patient’s Questions Regarding Age-Related Macular Degeneration. Diagnostics. 2024; 14(14):1468. https://doi.org/10.3390/diagnostics14141468
Chicago/Turabian StyleMuntean, George Adrian, Anca Marginean, Adrian Groza, Ioana Damian, Sara Alexia Roman, Mădălina Claudia Hapca, Anca Mădălina Sere, Roxana Mihaela Mănoiu, Maximilian Vlad Muntean, and Simona Delia Nicoară. 2024. "A Qualitative Evaluation of ChatGPT4 and PaLM2’s Response to Patient’s Questions Regarding Age-Related Macular Degeneration" Diagnostics 14, no. 14: 1468. https://doi.org/10.3390/diagnostics14141468
APA StyleMuntean, G. A., Marginean, A., Groza, A., Damian, I., Roman, S. A., Hapca, M. C., Sere, A. M., Mănoiu, R. M., Muntean, M. V., & Nicoară, S. D. (2024). A Qualitative Evaluation of ChatGPT4 and PaLM2’s Response to Patient’s Questions Regarding Age-Related Macular Degeneration. Diagnostics, 14(14), 1468. https://doi.org/10.3390/diagnostics14141468