
Machine Learning Predicts Decompression Levels for Lumbar Spinal Stenosis Using Canal Radiomic Features from Computed Tomography Myelography

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
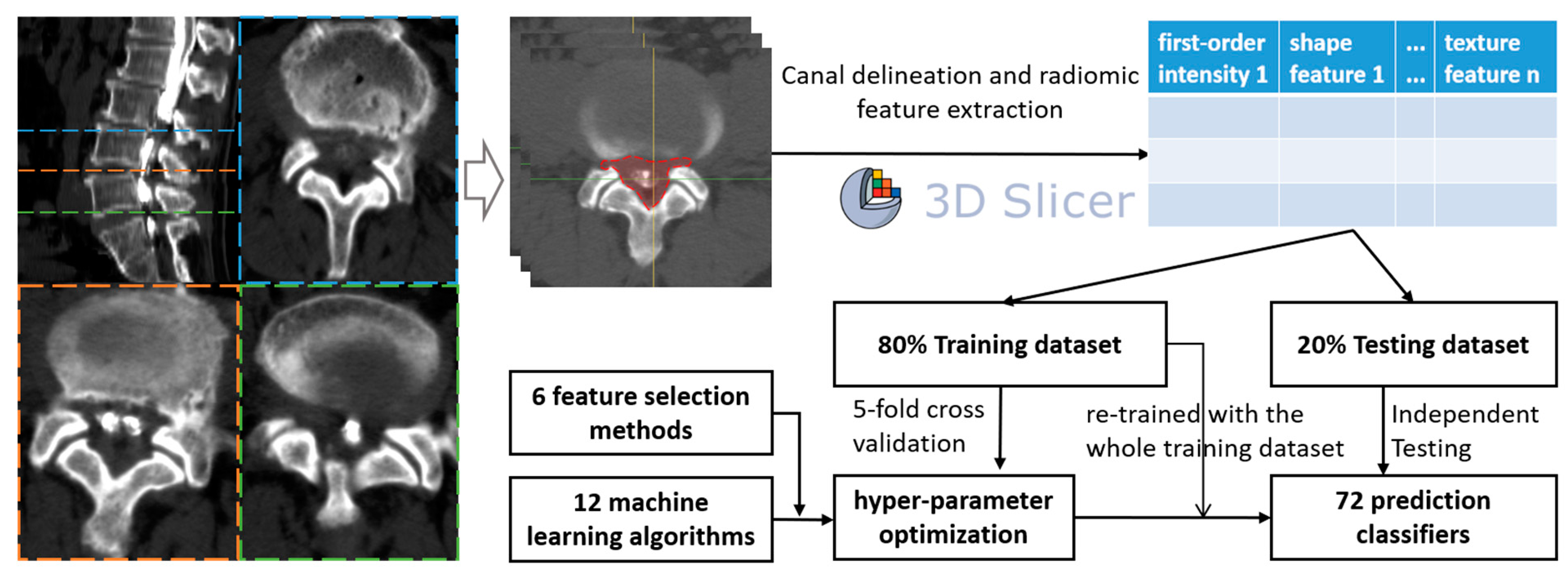
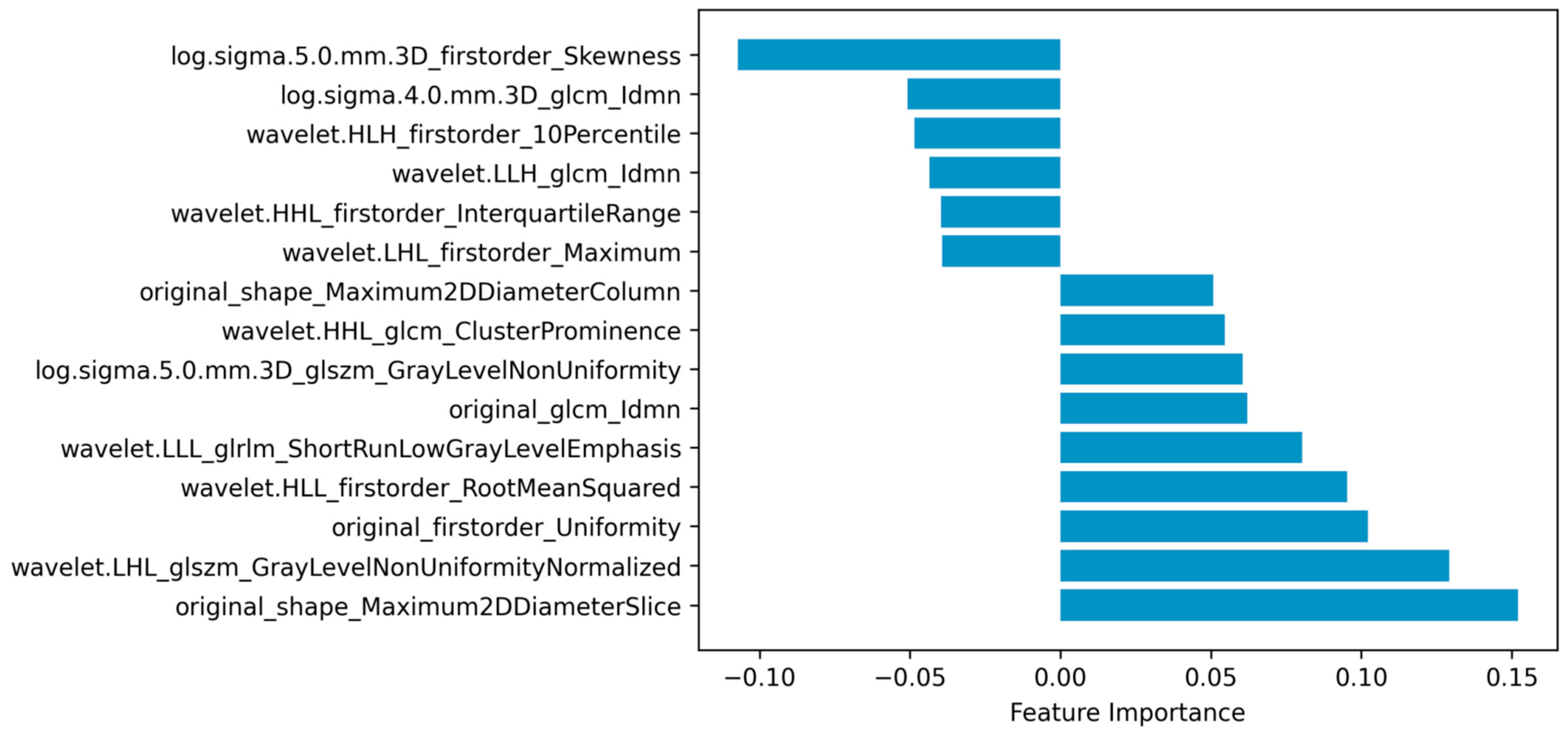
2.2. Radiomic Features
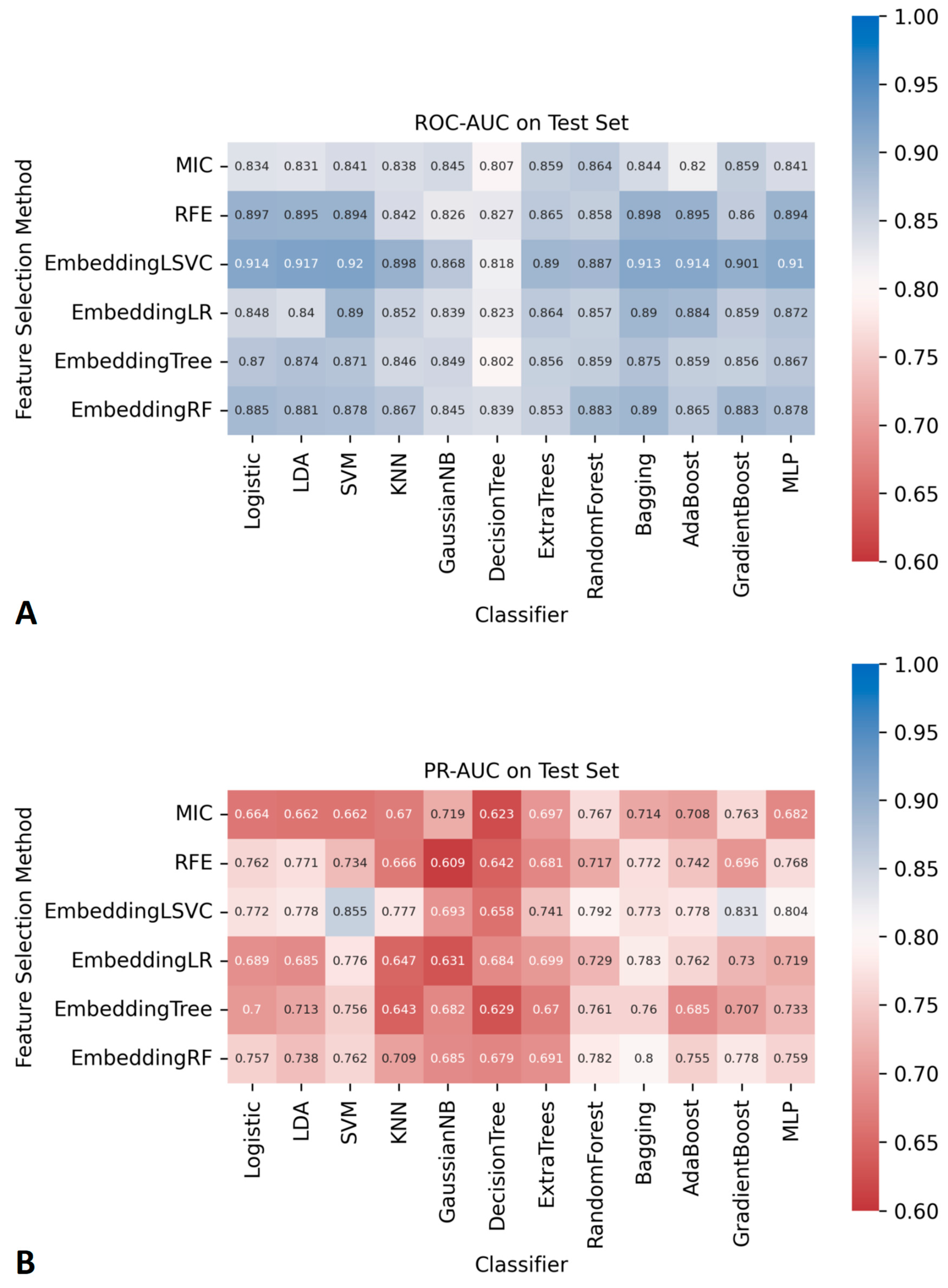
2.3. Model Development
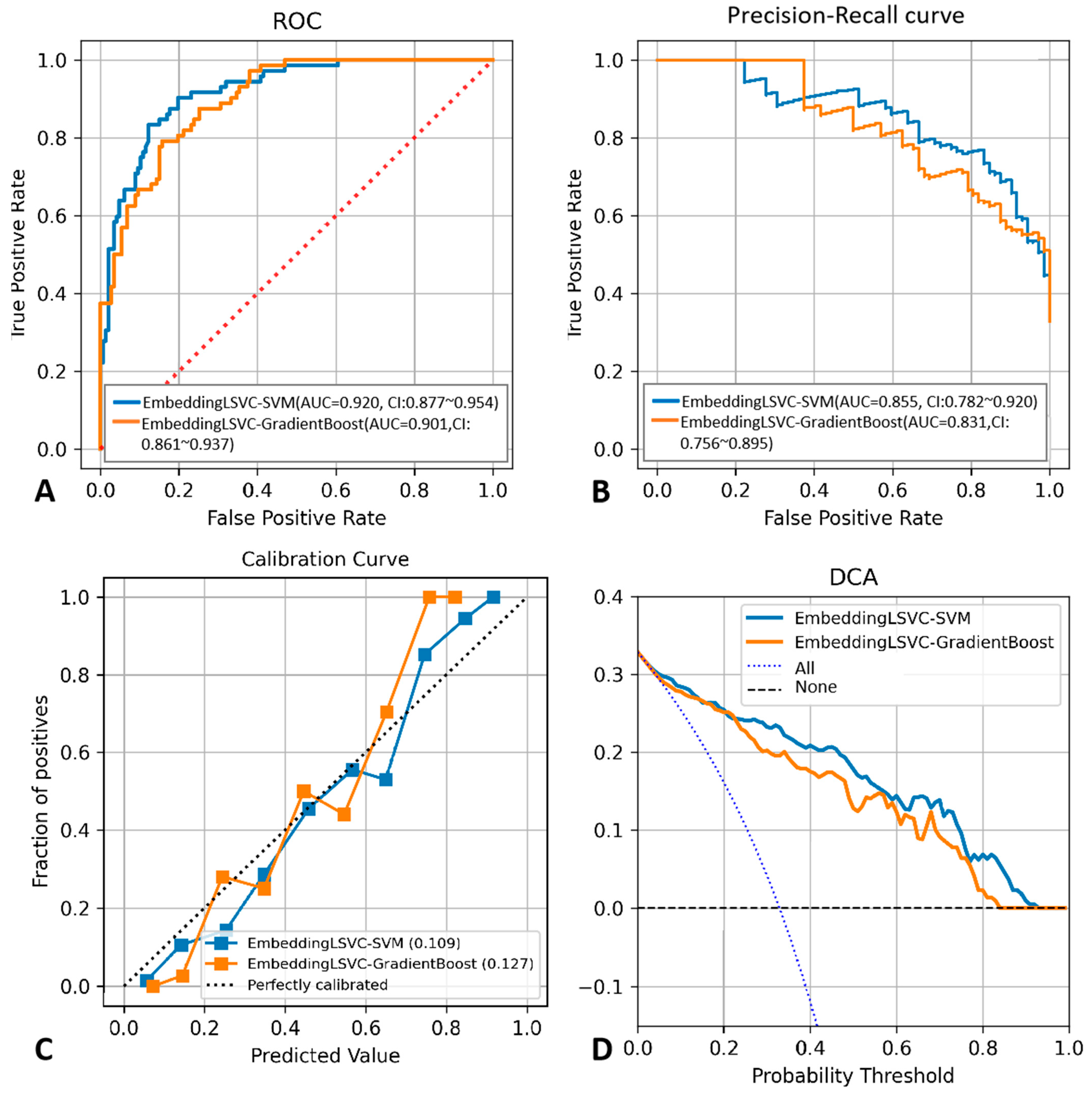
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katz, J.N.; Zimmerman, Z.E.; Mass, H.; Makhni, M.C. Diagnosis and Management of Lumbar Spinal Stenosis: A Review. JAMA 2022, 327, 1688–1699. [Google Scholar] [CrossRef] [PubMed]
- Siebert, E.; Prüss, H.; Klingebiel, R.; Failli, V.; Einhäupl, K.M.; Schwab, J.M. Lumbar spinal stenosis: Syndrome, diagnostics and treatment. Nat. Rev. Neurol. 2009, 5, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Gray, D.T.; Kreuter, W.; Mirza, S.; Martin, B.I. United States trends in lumbar fusion surgery for degenerative conditions. Spine 2005, 30, 1441–1445; discussion 1446–1447. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Mirza, S.K.; Martin, B.I.; Kreuter, W.; Goodman, D.C.; Jarvik, J.G. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 2010, 303, 1259–1265. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.; Li, Q.; Li, S.; Mao, H.; Meng, B.; Zhou, F.; Yang, H. Percutaneous Endoscopic Lumbar Discectomy: Indications and Complications. Pain Physician 2020, 23, 49–56. [Google Scholar] [PubMed]
- Smith, Z.A.; Fessler, R.G. Paradigm changes in spine surgery: Evolution of minimally invasive techniques. Nat. Rev. Neurol. 2012, 8, 443–450. [Google Scholar] [CrossRef]
- Wei, F.L.; Zhou, C.P.; Liu, R.; Zhu, K.L.; Du, M.R.; Gao, H.R.; Wu, S.D.; Sun, L.L.; Yan, X.D.; Liu, Y.; et al. Management for lumbar spinal stenosis: A network meta-analysis and systematic review. Int. J. Surg. 2021, 85, 19–28. [Google Scholar] [CrossRef]
- Ngiam, K.Y.; Khor, I.W. Big data and machine learning algorithms for health-care delivery. Lancet Oncol. 2019, 20, e262–e273. [Google Scholar] [CrossRef]
- Gaonkar, B.; Villaroman, D.; Beckett, J.; Ahn, C.; Attiah, M.; Babayan, D.; Villablanca, J.P.; Salamon, N.; Bui, A.; Macyszyn, L. Quantitative Analysis of Spinal Canal Areas in the Lumbar Spine: An Imaging Informatics and Machine Learning Study. AJNR Am. J. Neuroradiol. 2019, 40, 1586–1591. [Google Scholar] [CrossRef] [PubMed]
- Huber, F.A.; Stutz, S.; Vittoria de Martini, I.; Mannil, M.; Becker, A.S.; Winklhofer, S.; Burgstaller, J.M.; Guggenberger, R. Qualitative versus quantitative lumbar spinal stenosis grading by machine learning supported texture analysis-Experience from the LSOS study cohort. Eur. J. Radiol. 2019, 114, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Hallinan, J.; Zhu, L.; Yang, K.; Makmur, A.; Algazwi, D.A.R.; Thian, Y.L.; Lau, S.; Choo, Y.S.; Eide, S.E.; Yap, Q.V.; et al. Deep Learning Model for Automated Detection and Classification of Central Canal, Lateral Recess, and Neural Foraminal Stenosis at Lumbar Spine MRI. Radiology 2021, 300, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Won, D.; Lee, H.J.; Lee, S.J.; Park, S.H. Spinal Stenosis Grading in Magnetic Resonance Imaging Using Deep Convolutional Neural Networks. Spine 2020, 45, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Bharadwaj, U.U.; Christine, M.; Li, S.; Chou, D.; Pedoia, V.; Link, T.M.; Chin, C.T.; Majumdar, S. Deep learning for automated, interpretable classification of lumbar spinal stenosis and facet arthropathy from axial MRI. Eur. Radiol. 2023, 33, 3435–3443. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Wei, B.; Leung, S.; Nachum, I.B.; Laidley, D.; Li, S. Automated Pathogenesis-Based Diagnosis of Lumbar Neural Foraminal Stenosis via Deep Multiscale Multitask Learning. Neuroinformatics 2018, 16, 325–337. [Google Scholar] [CrossRef] [PubMed]
- Altun, S.; Alkan, A.; Altun, İ. LSS-VGG16: Diagnosis of Lumbar Spinal Stenosis With Deep Learning. Clin. Spine Surg. 2023, 36, E180–E190. [Google Scholar] [CrossRef] [PubMed]
- Siccoli, A.; de Wispelaere, M.P.; Schröder, M.L.; Staartjes, V.E. Machine learning-based preoperative predictive analytics for lumbar spinal stenosis. Neurosurg. Focus 2019, 46, E5. [Google Scholar] [CrossRef]
- Karhade, A.V.; Fogel, H.A.; Cha, T.D.; Hershman, S.H.; Doorly, T.P.; Kang, J.D.; Bono, C.M.; Harris, M.B.; Schwab, J.H.; Tobert, D.G. Development of prediction models for clinically meaningful improvement in PROMIS scores after lumbar decompression. Spine J. 2021, 21, 397–404. [Google Scholar] [CrossRef]
- Mannil, M.; Burgstaller, J.M.; Thanabalasingam, A.; Winklhofer, S.; Betz, M.; Held, U.; Guggenberger, R. Texture analysis of paraspinal musculature in MRI of the lumbar spine: Analysis of the lumbar stenosis outcome study (LSOS) data. Skelet. Radiol. 2018, 47, 947–954. [Google Scholar] [CrossRef]
- Mannil, M.; Burgstaller, J.M.; Held, U.; Farshad, M.; Guggenberger, R. Correlation of texture analysis of paraspinal musculature on MRI with different clinical endpoints: Lumbar Stenosis Outcome Study (LSOS). Eur. Radiol. 2019, 29, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Yagi, M.; Michikawa, T.; Yamamoto, T.; Iga, T.; Ogura, Y.; Tachibana, A.; Miyamoto, A.; Suzuki, S.; Nori, S.; Takahashi, Y.; et al. Development and validation of machine learning-based predictive model for clinical outcome of decompression surgery for lumbar spinal canal stenosis. Spine J. 2022, 22, 1768–1777. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Terai, H.; Yamada, K.; Kato, M.; Suzuki, A.; Takahashi, S.; Tamai, K.; Yabu, A.; Iwamae, M.; Sawada, Y.; et al. A decision tree analysis to predict clinical outcome of minimally invasive lumbar decompression surgery for lumbar spinal stenosis with and without coexisting spondylolisthesis and scoliosis. Spine J. 2023, 23, 973–981. [Google Scholar] [CrossRef] [PubMed]
- Karnuta, J.M.; Golubovsky, J.L.; Haeberle, H.S.; Rajan, P.V.; Navarro, S.M.; Kamath, A.F.; Schaffer, J.L.; Krebs, V.E.; Pelle, D.W.; Ramkumar, P.N. Can a machine learning model accurately predict patient resource utilization following lumbar spinal fusion? Spine J. 2020, 20, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Ogink, P.T.; Karhade, A.V.; Thio, Q.; Gormley, W.B.; Oner, F.C.; Verlaan, J.J.; Schwab, J.H. Predicting discharge placement after elective surgery for lumbar spinal stenosis using machine learning methods. Eur. Spine J. 2019, 28, 1433–1440. [Google Scholar] [CrossRef]
- Karhade, A.V.; Cha, T.D.; Fogel, H.A.; Hershman, S.H.; Tobert, D.G.; Schoenfeld, A.J.; Bono, C.M.; Schwab, J.H. Predicting prolonged opioid prescriptions in opioid-naïve lumbar spine surgery patients. Spine J. 2020, 20, 888–895. [Google Scholar] [CrossRef]
- Saravi, B.; Zink, A.; Ülkümen, S.; Couillard-Despres, S.; Hassel, F.; Lang, G. Performance of Artificial Intelligence-Based Algorithms to Predict Prolonged Length of Stay after Lumbar Decompression Surgery. J. Clin. Med. 2022, 11, 4050. [Google Scholar] [CrossRef]
- Wilson, B.; Gaonkar, B.; Yoo, B.; Salehi, B.; Attiah, M.; Villaroman, D.; Ahn, C.; Edwards, M.; Laiwalla, A.; Ratnaparkhi, A.; et al. Predicting Spinal Surgery Candidacy From Imaging Data Using Machine Learning. Neurosurgery 2021, 89, 116–121. [Google Scholar] [CrossRef]
- De Barros, A.; Abel, F.; Kolisnyk, S.; Geraci, G.C.; Hill, F.; Engrav, M.; Samavedi, S.; Suldina, O.; Kim, J.; Rusakov, A.; et al. Determining Prior Authorization Approval for Lumbar Stenosis Surgery With Machine Learning. Glob. Spine J. 2023, 21925682231155844. [Google Scholar] [CrossRef]
- Fan, G.; Qin, J.; Liu, H.; Liao, X. Commentary: Radiomics in oncology: A 10-year bibliometric analysis. Front. Oncol. 2022, 12, 891056. [Google Scholar] [CrossRef]
- Avanzo, M.; Wei, L.; Stancanello, J.; Vallières, M.; Rao, A.; Morin, O.; Mattonen, S.A.; El Naqa, I. Machine and deep learning methods for radiomics. Med. Phys. 2020, 47, e185–e202. [Google Scholar] [CrossRef] [PubMed]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Jujjavarapu, C.; Suri, P.; Pejaver, V.; Friedly, J.; Gold, L.S.; Meier, E.; Cohen, T.; Mooney, S.D.; Heagerty, P.J.; Jarvik, J.G. Predicting decompression surgery by applying multimodal deep learning to patients’ structured and unstructured health data. BMC Med. Inf. Decis. Mak. 2023, 23, 2. [Google Scholar] [CrossRef] [PubMed]
- Roller, B.L.; Boutin, R.D.; O’Gara, T.J.; Knio, Z.O.; Jamaludin, A.; Tan, J.; Lenchik, L. Accurate prediction of lumbar microdecompression level with an automated MRI grading system. Skelet. Radiol. 2021, 50, 69–78. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Fan, G.; Liu, H.; Wu, Z.; Li, Y.; Feng, C.; Wang, D.; Luo, J.; Wells, W.M., 3rd; He, S. Deep Learning-Based Automatic Segmentation of Lumbosacral Nerves on CT for Spinal Intervention: A Translational Study. AJNR. Am. J. Neuroradiol. 2019, 40, 1074–1081. [Google Scholar] [CrossRef]
- Covaro, A.; Vilà-Canet, G.; de Frutos, A.G.; Ubierna, M.T.; Ciccolo, F.; Caceres, E. Management of degenerative lumbar spinal stenosis: An evidence-based review. EFORT Open Rev. 2016, 1, 267–274. [Google Scholar] [CrossRef]
- Haddadi, K.; Ganjeh Qazvini, H.R. Outcome after Surgery of Lumbar Spinal Stenosis: A Randomized Comparison of Bilateral Laminotomy, Trumpet Laminectomy, and Conventional Laminectomy. Front. Surg. 2016, 3, 19. [Google Scholar] [CrossRef]
- Adilay, U.; Guclu, B. Comparison of Single-Level and Multilevel Decompressive Laminectomy for Multilevel Lumbar Spinal Stenosis. World Neurosurg. 2018, 111, e235–e240. [Google Scholar] [CrossRef]
- Yamamoto, T.; Yagi, M.; Suzuki, S.; Takahashi, Y.; Nori, S.; Tsuji, O.; Nagoshi, N.; Ogawa, J.; Matsumoto, M.; Nakamura, M.; et al. Multilevel Decompression Surgery for Degenerative Lumbar Spinal Canal Stenosis Is Similarly Effective With Single-level Decompression Surgery. Spine 2022, 47, 1728–1736. [Google Scholar] [CrossRef]
- Hamawandi, S.A.; Sulaiman, I.I.; Al-Humairi, A.K. Microdecompression versus Open Laminectomy and Posterior Stabilization for Multilevel Lumbar Spine Stenosis: A Randomized Controlled Trial. Pain Res. Manag. 2019, 2019, 7214129. [Google Scholar] [CrossRef] [PubMed]
- Nerland, U.S.; Jakola, A.S.; Solheim, O.; Weber, C.; Rao, V.; Lønne, G.; Solberg, T.K.; Salvesen, Ø.; Carlsen, S.M.; Nygaard, Ø.P.; et al. Minimally invasive decompression versus open laminectomy for central stenosis of the lumbar spine: Pragmatic comparative effectiveness study. BMJ 2015, 350, h1603. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Liu, T.F.; Shan, H.; Wan, Z.Y.; Wang, Z.; Viswanath, O.; Paladini, A.; Varrassi, G.; Wang, H.Q. Decompression Using Minimally Invasive Surgery for Lumbar Spinal Stenosis Associated with Degenerative Spondylolisthesis: A Review. Pain Ther. 2021, 10, 941–959. [Google Scholar] [CrossRef] [PubMed]
- Murata, S.; Nagata, K.; Iwasaki, H.; Hashizume, H.; Yukawa, Y.; Minamide, A.; Nakagawa, Y.; Tsutsui, S.; Takami, M.; Taiji, R.; et al. Long-Term Outcomes after Selective Microendoscopic Laminotomy for Multilevel Lumbar Spinal Stenosis with and without Remaining Radiographic Stenosis: A 10-Year Follow-Up Study. Spine Surg. Relat. Res. 2022, 6, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Kent, D.L.; Haynor, D.R.; Larson, E.B.; Deyo, R.A. Diagnosis of lumbar spinal stenosis in adults: A metaanalysis of the accuracy of CT, MR, and myelography. AJR Am. J. Roentgenol. 1992, 158, 1135–1144. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Morita, M.; Miyauchi, A.; Okuda, S.; Oda, T.; Iwasaki, M. Comparison between MRI and myelography in lumbar spinal canal stenosis for the decision of levels of decompression surgery. J. Spinal Disord. Tech. 2011, 24, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Hasegawa, K.; Shimoda, H.; Keiji, I.; Homma, T. Can recumbent magnetic resonance imaging replace myelography or computed tomography myelography for detecting lumbar spinal stenosis? Eur. J. Orthop. Surg. Traumatol. 2013, 23 (Suppl. 1), S77–S83. [Google Scholar] [CrossRef]
- Zileli, M.; Crostelli, M.; Grimaldi, M.; Mazza, O.; Anania, C.; Fornari, M.; Costa, F. Natural Course and Diagnosis of Lumbar Spinal Stenosis: WFNS Spine Committee Recommendations. World Neurosurg. X 2020, 7, 100073. [Google Scholar] [CrossRef]
- Akbari, K.K.; Badikillaya, V.; Venkatesan, M.; Ramanan, R.V.; Hegde, S.K. Resurgence of the Role of Computed-Tomography Myelogram in the Era of MRI for Surgical Decision-Making of Lumbar Degenerative Disc Disorder. Int. J. Spine Surg. 2021, 15, 788–794. [Google Scholar] [CrossRef]
- Weisenthal, B.W.; Glassman, S.D.; Mkorombindo, T.; Nelson, L.; Carreon, L.Y. When does CT-Myelography add value beyond MRI for lumbar degenerative disease? Spine J. 2021, 22, 787–792. [Google Scholar] [CrossRef]
- Rocos, B.; Evans, D.R.S.; Rajayogeswaran, B.; Hutchinson, M.J. The normal appearance of CT myelograms. Eur. Spine J. 2020, 29, 1087–1091. [Google Scholar] [CrossRef] [PubMed]
- Aerts, H.J.; Velazquez, E.R.; Leijenaar, R.T.; Parmar, C.; Grossmann, P.; Carvalho, S.; Bussink, J.; Monshouwer, R.; Haibe-Kains, B.; Rietveld, D.; et al. Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat. Commun. 2014, 5, 4006. [Google Scholar] [CrossRef] [PubMed]
- Dieckmeyer, M.; Sollmann, N.; El Husseini, M.; Sekuboyina, A.; Löffler, M.T.; Zimmer, C.; Kirschke, J.S.; Subburaj, K.; Baum, T. Gender-, Age- and Region-Specific Characterization of Vertebral Bone Microstructure Through Automated Segmentation and 3D Texture Analysis of Routine Abdominal CT. Front. Endocrinol. 2021, 12, 792760. [Google Scholar] [CrossRef] [PubMed]
- Wirries, A.; Geiger, F.; Hammad, A.; Oberkircher, L.; Blümcke, I.; Jabari, S. Artificial intelligence facilitates decision-making in the treatment of lumbar disc herniations. Eur. Spine J. 2021, 30, 2176–2184. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects | Training Dataset (n = 176) | Testing Dataset (n = 43) | p-Value |
|---|---|---|---|
| Age (years) | 61.59 ± 13.43 | 57.47 ± 14.95 | 0.126 |
| Gender | 0.978 | ||
| Male | 83 | 21 | |
| Female | 93 | 22 | |
| Decompression level | 0.233 | ||
| L1/L2 | 4 | 0 | |
| L2/L3 | 18 | 5 | |
| L3/L4 | 47 | 14 | |
| L4/L5 | 116 | 41 | |
| L5/S1 | 90 | 48 |
| Ranking | ROC-AUC | p-Values | SVM | LDA | AdaBoost | LR | Bagging | MLP | GradientBoost |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 0.920 | SVM | 1 | - | - | - | - | - | - |
| 2 | 0.917 | LDA | 0.820 | 1 | - | - | - | - | - |
| 3 | 0.914 | AdaBoost | 0.632 | 0.316 | 1 | - | - | - | - |
| 4 | 0.914 | LR | 0.602 | 0.268 | 0.900 | 1 | - | - | - |
| 5 | 0.913 | Bagging | 0.665 | 0.521 | 0.867 | 0.698 | 1 | - | - |
| 6 | 0.910 | MLP | 0.328 | 0.177 | 0.452 | 0.504 | 0.439 | 1 | - |
| 7 | 0.901 | GradientBoost | 0.139 | 0.230 | 0.332 | 0.365 | 0.339 | 0.510 | 1 |
| Ranking | PR-AUC | p-Values | SVM | GradientBoost |
|---|---|---|---|---|
| 1 | 0.855 | SVM | 1 | <0.001 |
| 2 | 0.831 | GradientBoost | <0.001 | 1 |
| EmbeddingLSVC_ML | Sensitivity | Specificity | Accuracy | PPV | NPV |
|---|---|---|---|---|---|
| SVM | 0.833 | 0.864 | 0.854 | 0.750 | 0.864 |
| GradientBoost | 0.694 | 0.850 | 0.799 | 0.694 | 0.850 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fan, G.; Wang, D.; Li, Y.; Xu, Z.; Wang, H.; Liu, H.; Liao, X. Machine Learning Predicts Decompression Levels for Lumbar Spinal Stenosis Using Canal Radiomic Features from Computed Tomography Myelography. Diagnostics 2024, 14, 53. https://doi.org/10.3390/diagnostics14010053
Fan G, Wang D, Li Y, Xu Z, Wang H, Liu H, Liao X. Machine Learning Predicts Decompression Levels for Lumbar Spinal Stenosis Using Canal Radiomic Features from Computed Tomography Myelography. Diagnostics. 2024; 14(1):53. https://doi.org/10.3390/diagnostics14010053
Chicago/Turabian StyleFan, Guoxin, Dongdong Wang, Yufeng Li, Zhipeng Xu, Hong Wang, Huaqing Liu, and Xiang Liao. 2024. "Machine Learning Predicts Decompression Levels for Lumbar Spinal Stenosis Using Canal Radiomic Features from Computed Tomography Myelography" Diagnostics 14, no. 1: 53. https://doi.org/10.3390/diagnostics14010053
APA StyleFan, G., Wang, D., Li, Y., Xu, Z., Wang, H., Liu, H., & Liao, X. (2024). Machine Learning Predicts Decompression Levels for Lumbar Spinal Stenosis Using Canal Radiomic Features from Computed Tomography Myelography. Diagnostics, 14(1), 53. https://doi.org/10.3390/diagnostics14010053