
Development of a Point-of-Care Cervico-Vaginal Sampling/Testing Device for the Colorimetric Detection of Cervical Cancer
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Characterization
2.3. Clinical Samples: Collection and Analysis
2.4. Analysis of Clinical Samples Using the C-ColAur Technique
2.5. Sensitivity and Specificity of C-ColAur Detection
2.6. Aggregation Coefficient and Particle Size Analysis
2.7. Estimation of the Concentration of Lipids and Protein in Clinical Samples
2.8. Analysis with Synthetic Proteins and Lipids
2.9. Design of the Self-Sampling Device: CerviSelf
2.9.1. Design Specifications
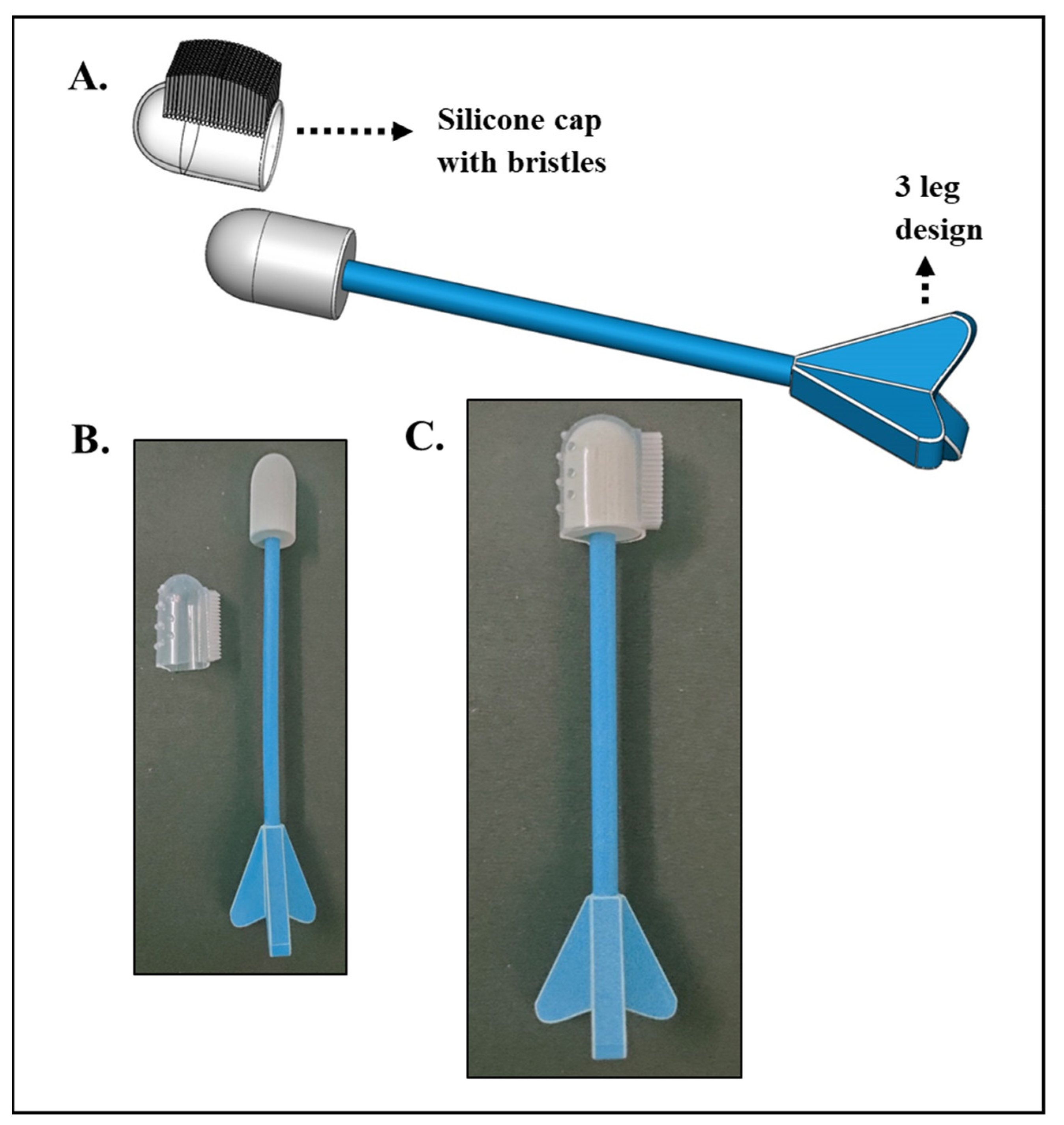
2.9.2. Physical Prototypes
2.10. Statistical Analysis
3. Results and Discussions
3.1. Clinical Samples and Their Analysis
3.2. Modeling, Design, and Prototyping of a Self-Sampling Device
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Buskwofie, A.; David-West, G.; Clare, C.A. A review of cervical cancer: Incidence and disparities. J. Natl. Med. Assoc. 2020, 112, 229–232. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.A.; Jhingran, A.; Oaknin, A.; Denny, L. Cervical cancer. Lancet 2019, 393, 169–182. [Google Scholar] [CrossRef]
- Singh, D.; Vignat, J.; Lorenzoni, V.; Eslahi, M.; Ginsburg, O.; Lauby-SECRETAN, B.; Arbyn, M.; Basu, P.; Bray, F.; Vaccarella, S. Global estimates of incidence and mortality of cervical cancer in 2020: A baseline analysis of the WHO Global Cervical Cancer Elimination Initiative. Lancet Glob. Health 2022, 11, e197–e206. [Google Scholar] [CrossRef]
- Zhang, S.; Xu, H.; Zhang, L.; Qiao, Y. Cervical cancer: Epidemiology, risk factors and screening. Chin. J. Cancer Res. 2020, 32, 720. [Google Scholar] [CrossRef] [PubMed]
- Ramamoorthy, T.; Sathishkumar, K.; Das, P.; Sudarshan, K.L.; Mathur, P. Epidemiology of Human Papillomavirus Related Cancers in India: Findings from the National Cancer Registry Programme; Indian Council of Medical Research—National Centre for Disease Informatics and Research: Karnataka, India, 2022. [Google Scholar]
- Chan, C.K.; Aimagambetova, G.; Ukybassova, T.; Kongrtay, K.; Azizan, A. Human papillomavirus infection and cervical cancer: Epidemiology, screening, and vaccination—Review of current perspectives. J. Oncol. 2019, 2019, 3257939. [Google Scholar] [CrossRef]
- Dhaher, E.A. Knowledge, attitudes and practices of women in the southern region of Saudi Arabia regarding cervical cancer and the pap smear test. Asian Pac. J. Cancer Prev. APJCP 2019, 20, 1177. [Google Scholar] [CrossRef] [PubMed]
- Sompawong, N.; Mopan, J.; Pooprasert, P.; Himakhun, W.; Suwannarurk, K.; Ngamvirojcharoen, J.; Vachiramon, T.; Tantibundhit, C. Automated pap smear cervical cancer screening using deep learning. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 7044–7048. [Google Scholar]
- Rezende, M.T.; Bianchi, A.G.; Carneiro, C.M. Cervical cancer: Automation of pap test screening. Diagn. Cytopathol. 2021, 49, 559–574. [Google Scholar] [CrossRef]
- Bedell, S.L.; Goldstein, L.S.; Goldstein, A.R.; Goldstein, A.T. Cervical cancer screening: Past, present, and future. Sex. Med. Rev. 2020, 8, 28–37. [Google Scholar] [CrossRef]
- Win, K.P.; Kitjaidure, Y.; Hamamoto, K. An implementation of medical image mosaicing system based on oriented FAST and rotated BRIEF approach. Appl. Sci. 2020, 10, 1800. [Google Scholar] [CrossRef]
- Parraga, F.T.; Rodriguez, C.; Pomachagua, Y.; Rodriguez, D. A review of image-based deep learning algorithms for cervical cancer screening. In Proceedings of the 2021 13th International Conference on Computational Intelligence and Communication Networks (CICN), Lima, Peru, 22–23 September 2023; pp. 155–160. [Google Scholar]
- Appidi, T.; Mudigunda, S.V.; Kodandapani, S.; Rengan, A.K. Development of label-free gold nanoparticle based rapid colorimetric assay for clinical/point-of-care screening of cervical cancer. Nanoscale Adv. 2020, 2, 5737–5745. [Google Scholar] [CrossRef] [PubMed]
- Saranath, D.; Khanna, A. Current status of cancer burden: Global and Indian scenario. Biomed. Res. J. 2014, 1, 1–5. [Google Scholar] [CrossRef]
- WHO. Cervical Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 15 January 2023).
- Docto, I. HumansofMaRS: Eve Medical Enables Women to Test for Cervical Cancer from the Comfort of Their Own Homes. Available online: https://www.marsdd.com/news/humansofmars-eve-medical-enables-women-test-cervical-cancer-comfort-homes/ (accessed on 19 February 2023).
- Cervical Screening—CervicalCheck. Available online: https://www2.hse.ie/conditions/cervical-screening/ (accessed on 19 February 2023).
- Ilangovan, K.; Kobetz, E.; Koru-Sengul, T.; Marcus, E.N.; Rodriguez, B.; Alonzo, Y.; Carrasquillo, O. Acceptability and feasibility of human papilloma virus self-sampling for cervical cancer screening. J. Womens Health 2016, 25, 944–951. [Google Scholar] [CrossRef]
- Malone, C.; Barnabas, R.V.; Buist, D.S.; Tiro, J.A.; Winer, R.L. Cost-effectiveness studies of HPV self-sampling: A systematic review. Prev. Med. 2020, 132, 105953. [Google Scholar] [CrossRef] [PubMed]
- Defo, V.F.; Domgue, J.F. Why consider self-sampling for cervical cancer screening in low-and middle-income countries? AMA J. Ethics 2020, 22, 116–125. [Google Scholar]
- Parikh, R.; Mathai, A.; Parikh, S.; Sekhar, G.C.; Thomas, R. Understanding and using sensitivity, specificity and predictive values. Indian J. Ophthalmol. 2008, 56, 45. [Google Scholar] [CrossRef] [PubMed]
- Trevethan, R. Sensitivity, specificity, and predictive values: Foundations, pliabilities, and pitfalls in research and practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef]
- Sina, A.A.I.; Carrascosa, L.G.; Liang, Z.; Grewal, Y.S.; Wardiana, A.; Shiddiky, M.J.; Gardiner, R.A.; Samaratunga, H.; Gandhi, M.K.; Scott, R.J. Epigenetically reprogrammed methylation landscape drives the DNA self-assembly and serves as a universal cancer biomarker. Nat. Commun. 2018, 9, 4915. [Google Scholar] [CrossRef]
- Mao, J.-Y.; Li, H.-W.; Wei, S.-C.; Harroun, S.G.; Lee, M.-Y.; Lin, H.-Y.; Chung, C.-Y.; Hsu, C.-H.; Chen, Y.-R.; Lin, H.-J. DNA Modulates the Interaction of Genetically Engineered DNA-Binding Proteins and Gold Nanoparticles: Diagnosis of High-Risk HPV Infection. ACS Appl. Mater. Interfaces 2017, 9, 44307–44315. [Google Scholar] [CrossRef]
- Anderson, D.M.G.; Peter, P.; Domanik Richard, A. Personal Cervical Cell Collector; US-6352513-B1. Available online: https://patents.google.com/patent/US6352513 (accessed on 1 October 2001).
- Martin-Hirsch, P.P.; Jarvis, G.G.; Kitchener, H.C.; Lilford, R.; Cochrane Gynaecological, N.o.; Group, O.C. Collection devices for obtaining cervical cytology samples. Cochrane Database Syst. Rev. 1996. [Google Scholar] [CrossRef]
- Elahi, N.; Kamali, M.; Baghersad, M.H. Recent biomedical applications of gold nanoparticles: A review. Talanta 2018, 184, 537–556. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Chen, C.-P.; Wu, T.-H.; Yang, C.-H.; Lin, C.-W.; Chen, C.-Y. Gold Nanoparticle-Based Colorimetric Strategies for Chemical and Biological Sensing Applications. Nanomaterials 2019, 9, 861. [Google Scholar] [CrossRef] [PubMed]
- Dadmehr, M.; Mortezaei, M.; Korouzhdehi, B. Dual mode fluorometric and colorimetric detection of matrix metalloproteinase MMP-9 as a cancer biomarker based on AuNPs@ gelatin/AuNCs nanocomposite. Biosens. Bioelectron. 2023, 220, 114889. [Google Scholar] [CrossRef] [PubMed]
- Shi, R.; Yang, J.; Cheng, S.; Qin, S.; Huang, L.; Wang, Y.; Xu, Y. Colorimetric determination of biothiols with AuNPs@ MoS 2 NSs as a peroxidase mimetic enzyme. New J. Chem. 2022, 46, 18718–18723. [Google Scholar] [CrossRef]
- Haguenoer, K.; Sengchanh, S.; Gaudy-Graffin, C.; Boyard, J.; Fontenay, R.; Marret, H.; Goudeau, A.; Pigneaux de Laroche, N.; Rusch, E.; Giraudeau, B. Vaginal self-sampling is a cost-effective way to increase participation in a cervical cancer screening programme: A randomised trial. Br. J. Cancer 2014, 111, 2187–2196. [Google Scholar] [CrossRef]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Appidi, T.; Vakada, M.; Buddhiraju, H.S.; Chinchulkar, S.A.; Kota, A.; Yadav, D.N.; Kodandapani, S.; Simhabhatla, S.K.; Rengan, A.K. Development of a Point-of-Care Cervico-Vaginal Sampling/Testing Device for the Colorimetric Detection of Cervical Cancer. Diagnostics 2023, 13, 1382. https://doi.org/10.3390/diagnostics13081382
Appidi T, Vakada M, Buddhiraju HS, Chinchulkar SA, Kota A, Yadav DN, Kodandapani S, Simhabhatla SK, Rengan AK. Development of a Point-of-Care Cervico-Vaginal Sampling/Testing Device for the Colorimetric Detection of Cervical Cancer. Diagnostics. 2023; 13(8):1382. https://doi.org/10.3390/diagnostics13081382
Chicago/Turabian StyleAppidi, Tejaswini, Murali Vakada, Hima Sree Buddhiraju, Shubham A. Chinchulkar, Akshar Kota, Dokkari Nagalaxmi Yadav, Suseela Kodandapani, Surya Kumar Simhabhatla, and Aravind Kumar Rengan. 2023. "Development of a Point-of-Care Cervico-Vaginal Sampling/Testing Device for the Colorimetric Detection of Cervical Cancer" Diagnostics 13, no. 8: 1382. https://doi.org/10.3390/diagnostics13081382
APA StyleAppidi, T., Vakada, M., Buddhiraju, H. S., Chinchulkar, S. A., Kota, A., Yadav, D. N., Kodandapani, S., Simhabhatla, S. K., & Rengan, A. K. (2023). Development of a Point-of-Care Cervico-Vaginal Sampling/Testing Device for the Colorimetric Detection of Cervical Cancer. Diagnostics, 13(8), 1382. https://doi.org/10.3390/diagnostics13081382