

The Effects of Moxifloxacin and Gemifloxacin on the ECG Morphology in Healthy Volunteers: A Phase 1 Randomized Clinical Trial

 , ,
, ,  , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
- Whose ages were age <20 years or >40 years, due to increased risk with advancing age. Similarly, old females at twice the risk were excluded.
- Hypocalcemia, hypokalemic and participants suffering from ischemia and LV dysfunction.
- Participants having QTc ≥ 450 ms before starting the dose, QRS ≥ 120 ms, with a family history of cardiovascular disease (CVDs), heart beats <50 BPM or >100 BPM, or with a history of fluoroquinolones allergy were also excluded.
- Female participants who were lactating or pregnant were not selected.
2.3. Safety Monitoring and Trial Discontinuation
2.4. Sample Estimation and Randomization
2.5. Procedures
2.5.1. Drugs and Dosing
2.5.2. Instruments
Blood Pressure Measurements
ECG Recording
- (a)
- ECG Analysis and Interpretation
- (b)
- QRS-Complex Measurements
- (c)
- Blinding
2.6. Adverse Drug Effects Monitoring
2.7. Statistical Analysis
3. Results
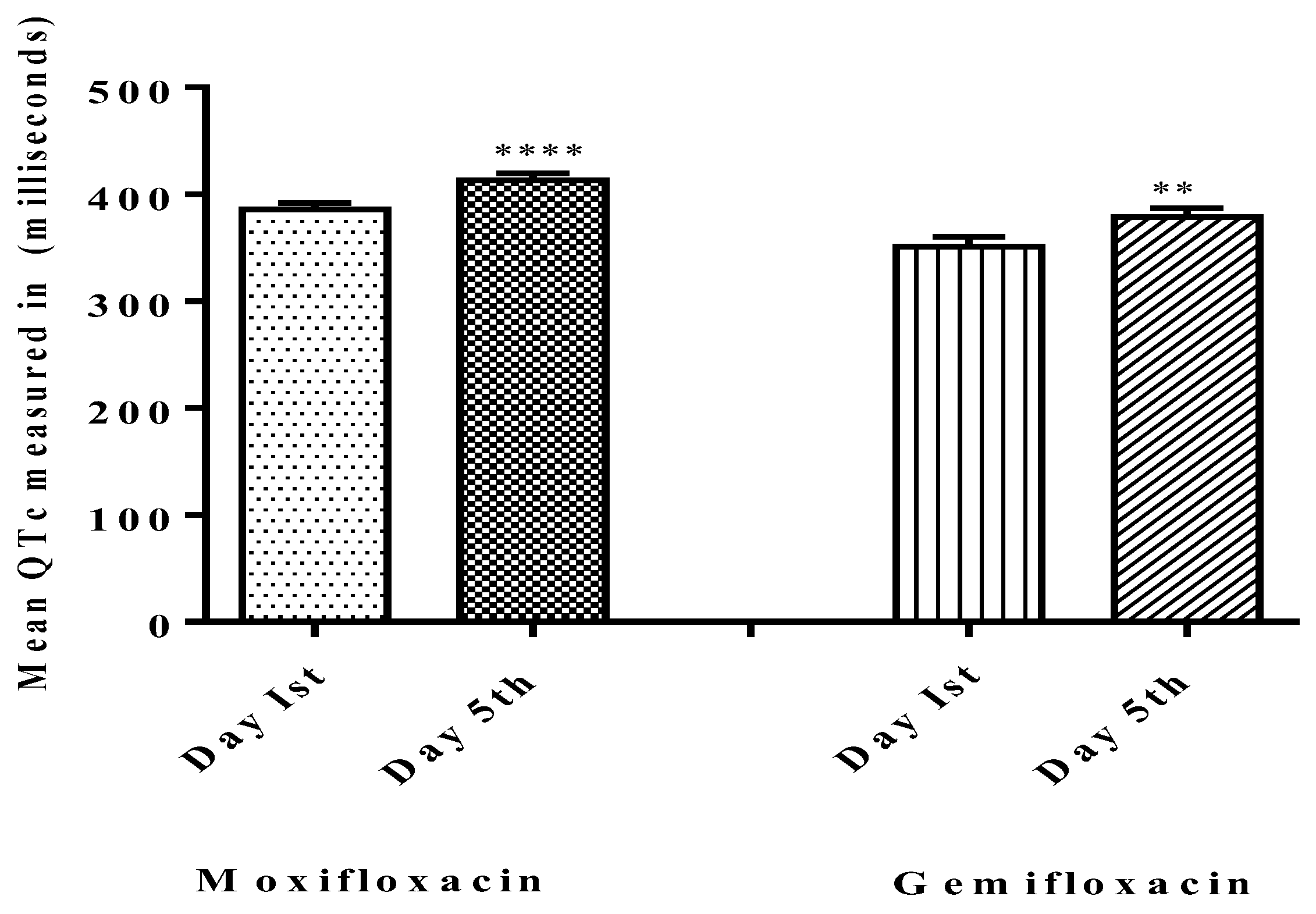
3.1. Effects on QT Interval
3.2. Adverse Effects
4. Discussions
5. Limitations
6. Conclusions
7. Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BP | Blood Pressure |
| BPM | Beats Per minutes |
| CVD | Cardiovascular disease |
| EMEA | European Medicines Evaluation Agency |
| ECG | Electrocardiogram |
| FDA | Food and Drug Administration |
| FQs | Fluoroquinolones |
| ms | milliseconds |
| Kir | Internal rectifying potassium unit |
| LV Dysfunction | Left Ventricular dysfunction |
| QTc | Corrected QT-interval |
| QTIP | QT interval prolongation |
| TdP | Torsade de points |
References
- Hori, S.; Kawamura, M.; Kizu, J. Effect of fluoroquinolones on plasma glucose levels in fasted and glucose-loaded mice. J. Infect. Chemother. 2006, 12, 109–111. [Google Scholar] [CrossRef] [PubMed]
- Emmerson, A.; Jones, A. The quinolones: Decades of development and use. J. Antimicrob. Chemother. 2003, 51, 13–20. [Google Scholar] [CrossRef]
- Appelbaum, P.; Hunter, P. The fluoroquinolone antibacterials: Past, present and future perspectives. Int. J. Antimicrob. Agents 2000, 16, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Speciale, A.; Musumeci, R.; Blandino, G.; Milazzo, I.; Caccamo, F.; Nicoletti, G. Minimal inhibitory concentrations and time-kill determination of moxifloxacin against aerobic and anaerobic isolates. Int. J. Antimicrob. Agents 2002, 19, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, I. The influence of new quinolones on blood glucose level. J. Chemother. 1996, 44, 798–803. [Google Scholar]
- Takehiro, M. Severe hypoglycemia induced by lomefloxacin hydrochloride in a hemodyilytic patient. J. Diabet Soc. 2002, 45, 293. [Google Scholar]
- Baker, S.E.; Hangii, M.C. Possible gatifloxacin-induced hypoglycemia. Ann. Pharmacother. 2002, 36, 1722–1726. [Google Scholar] [CrossRef]
- Aspinall, S.L.; Good, C.B.; Jiang, R.; McCarren, M.; Dong, D.; Cunningham, F.E. Severe dysglycemia with the fluoroquinolones: A class effect? Clin. Infect. Dis. 2009, 49, 402–408. [Google Scholar] [CrossRef]
- Chou, H.-W.; Wang, J.-L.; Chang, C.-H.; Lee, J.-J.; Shau, W.-Y.; Lai, M.-S. Risk of severe dysglycemia among diabetic patients receiving levofloxacin, ciprofloxacin, or moxifloxacin in Taiwan. Clin. Infect. Dis. 2013, 57, 971–980. [Google Scholar] [CrossRef]
- Lawrence, K.R.; Adra, M.; Keir, C. Hypoglycemia-induced anoxic brain injury possibly associated with levofloxacin. J. Infect. 2006, 52, 177–180. [Google Scholar] [CrossRef]
- Kapoor, R.; Blum, D.; Batra, A.; Varma, N.; Lakshmi, K.; Basak, P.; Jesmajian, S. Life-threatening hypoglycemia with moxifloxacin in a dialysis patient. J. Clin. Pharmacol. 2012, 52, 269–271. [Google Scholar] [CrossRef]
- Gorelik, E.; Masarwa, R.; Perlman, A.; Rotshild, V.; Abbasi, M.; Muszkat, M.; Matok, I. Fluoroquinolones and cardiovascular risk: A systematic review, meta-analysis and network meta-analysis. Drug. Saf. 2019, 42, 529–538. [Google Scholar] [CrossRef]
- Van Noord, C.; Eijgelsheim, M.; Stricker, B.H.C. Drug-and non-drug-associated QT interval prolongation. Br. J. Clin. Pharmacol. 2010, 70, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Surges, R.; Taggart, P.; Sander, J.W.; Walker, M.C. Too long or too short? New insights into abnormal cardiac repolarization in people with chronic epilepsy and its potential role in sudden unexpected death. Epilepsia 2010, 51, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Haring, B.; Bauer, W. Ciprofl oxacin and the risk for cardiac arrhythmias: Culprit delicti or watching bystander? Acta Cardiol. 2012, 67, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Glassman, A.H.; Bigger, J.T. Antipsychotic drugs: Prolonged QTc interval, torsade de pointes, and sudden death. Am. J. Psychiatry 2001, 158, 1774–1782. [Google Scholar] [CrossRef] [PubMed]
- Briasoulis, A.; Agarwal, V.; Pierce, W.J. QT prolongation and torsade de pointes induced by fluoroquinolones: Infrequent side effects from commonly used medications. Cardiology 2011, 120, 103–110. [Google Scholar] [CrossRef]
- Liu, H.H. Safety profile of the fluoroquinolones. Drug. Saf. 2010, 33, 353–369. [Google Scholar] [CrossRef]
- Gill, J.; Johnson, P.; Clark, M. Research Methods for Managers; SAGE Publications: Thousand Oaks, CA, USA, 2010. [Google Scholar]
- Antoniou, C.-K.; Dilaveris, P.; Manolakou, P.; Galanakos, S.; Magkas, N.; Gatzoulis, K.; Tousoulis, D. QT Prolongation and Malignant Arrhythmia: How Serious a Problem? Eur. Cardiol. Rev. 2017, 12, 112–120. [Google Scholar] [CrossRef]
- Bazett, H. An analysis of the time relations of electrocardiograms. Ann. Noninvasive Electrocardiol. 1997, 2, 177–194. [Google Scholar] [CrossRef]
- Goldenberg, I.; Moss, A.J.; Zareba, W. QT interval: How to measure it and what is “normal”. J. Cardiovasc. Electrophysiol. 2006, 17, 333–336. [Google Scholar] [CrossRef]
- Satpathy, S.; Satpathy, S.; Nayak, P.K. Effect of age and gender on QT interval. Natl. J. Physiol. Pharm. Pharmacol. 2018, 8, 224–227. [Google Scholar] [CrossRef]
- Cubeddu, L.X. Drug-induced inhibition and trafficking disruption of ion channels: Pathogenesis of QT abnormalities and drug-induced fatal arrhythmias. Curr. Cardiol. Rev. 2016, 12, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Scherptong, R.W.; Henkens, I.R.; Man, S.C.; Le Cessie, S.; Vliegen, H.W.; Draisma, H.H.; Maan, A.C.; Schalij, M.J.; Swenne, C.A. Normal limits of the spatial QRS-T angle and ventricular gradient in 12-lead electrocardiograms of young adults: Dependence on sex and heart rate. J. Electrocardiol. 2008, 41, 648–655. [Google Scholar] [CrossRef]
- El Ghandour, S.; Azar, S.T. Dysglycemia associated with quinolones. Prim. Care Diabetes 2015, 9, 168–171. [Google Scholar] [CrossRef]
- Khan, F.; Ismail, M.; Khan, Q.; Ali, Z. Moxifloxacin-induced QT interval prolongation and torsades de pointes: A narrative review. Expert. Opin. Drug. Saf. 2018, 17, 1029–1039. [Google Scholar] [CrossRef] [PubMed]
- Graumlich, J.F.; Habis, S.; Avelino, R.R.; Salverson, S.M.; Gaddamanugu, M.; Jamma, K.; Aldag, J.C. Hypoglycemia in inpatients after gatifloxacin or levofloxacin therapy: Nested case control study. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2005, 25, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Crouch, M.A.; Limon, L.; Cassano, A.T. Clinical relevance and management of drug-related QT interval prolongation. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2003, 23, 881–908. [Google Scholar] [CrossRef]
- Démolis, J.; Kubitza, D.; Tennezé, L.; Funck-Brentano, C. Effect of a single oral dose of moxifloxacin (400 mg and 800 mg) on ventricular repolarization in healthy subjects. Clin. Pharm. Ther. 2000, 68, 658–666. [Google Scholar] [CrossRef]
- Yap, Y.G.; Camm, A.J. Drug induced QT prolongation and torsades de pointes. Heart 2003, 89, 1363–1372. [Google Scholar] [CrossRef]
- Drew, B.J.; Ackerman, M.J.; Funk, M.; Gibler, W.B.; Kligfield, P.; Menon, V.; Philippides, G.J.; Roden, D.M.; Zareba, W. Prevention of torsade de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation endorsed by the American Association of Critical-Care Nurses and the International Society for Computerized Electrocardiology. J. Am. Coll. Cardiol. 2010, 55, 934–947. [Google Scholar]
- Noel, G.J.; Abels, R.; Minton, N.; Natarajan, J.; Chien, S. Effect of three fluoroquinolones on QTc intervals in healthy volunteers. In Proceedings of the 41st Interscience Conference on Antimicrobial Agents and Chemotherapy, Chicago, IL, USA, 16–19 December 2001. [Google Scholar]
- Wynn, G.H.; Oesterheld, J.R.; Cozza, K.L.; Armstrong, S.C. Clinical Manual of Drug Interaction Principles for Medical Practice; American Psychiatric Pub: Washington, DC, USA, 2009. [Google Scholar]
- Ponte, M.L.; Keller, G.A.; Girolamo, G.D. Mechanisms of drug induced QT interval prolongation. Curr. Drug Saf. 2010, 5, 44–53. [Google Scholar] [CrossRef]
- Rook, M.B.; Evers, M.M.; Vos, M.A.; Bierhuizen, M.F. Biology of cardiac sodium channel Nav1. 5 expression. Cardiovasc. Res. 2012, 93, 12–23. [Google Scholar] [CrossRef]
- Darpo, B.; Nebout, T.; Sager, P.T. Clinical evaluation of QT/QTc prolongation and proarrhythmic potential for nonantiarrhythmic drugs: The International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use E14 guideline. J. Clin. Pharmacol. 2006, 46, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Nau, C.; Seaver, M.; Wang, S.-Y.; Wang, G.K. Block of human heart hH1 sodium channels by amitriptyline. J. Pharmacol. Exp. Ther. 2000, 292, 1015–1023. [Google Scholar]
- Kang, J.; Wang, L.; Chen, X.-L.; Triggle, D.J.; Rampe, D. Interactions of a series of fluoroquinolone antibacterial drugs with the human cardiac K+ channel HERG. Mol. Pharmacol. 2001, 59, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Adil, M.I.; AttaUllah, M.; Gul, M.; Khan, S. Prolonged QTc interval and torsades de pointes induced by moxifloxacin. J. Bacha Khan Med. Coll. Editor. Board 2020, 300, 55. [Google Scholar]
- Ullah, A.; Ahmad, S.; Ali, N.; Rahman, S.U.; Hussain, H.; Alghamdi, S.; Almehmadi, M.; Dablool, A.S.; Bannunah, A.M.; Bukhari, S.H.; et al. Insulinotropic potential of Moxifloxacin and Gemifloxacin: An in vivo rabbits model study followed by randomized phase I clinical trial. Antibiotics 2022, 11, 148. [Google Scholar] [CrossRef]
- Panicker, G.K.; Karnad, D.R.; Kadam, P.; Badilini, F.; Damle, A.; Kothari, S. Detecting moxifloxacin-induced QTc prolongation in thorough QT and early clinical phase studies using a highly automated ECG analysis approach. Br. J. Pharmacol. 2016, 173, 1373–1380. [Google Scholar] [CrossRef]
- Altin, T.; Ozcan, O.; Turhan, S.; Ozdemir, A.O.; Akyurek, O.; Karaoguz, R.; Guldal, M. Torsade de pointes associated with moxifloxacin: A rare but potentially fatal adverse event. Can. J. Cardiol. 2007, 23, 907–908. [Google Scholar] [CrossRef]
- Morganroth, J.; Wang, Y.; Thorn, M.; Kumagai, Y.; Harris, S.; Stockbridge, N.; Kleiman, R.; Shah, R. Moxifloxacin-induced QTc interval prolongations in healthy male Japanese and Caucasian volunteers: A direct comparison in a thorough QT study. Br. J. Clin. Pharmacol. 2015, 80, 446–459. [Google Scholar] [CrossRef]
- Moon, S.J.; Lee, J.; An, H.; Yim, D.S.; Chung, J.Y.; Yu, K.S.; Cho, J.Y.; Lim, K.S. The effects of moxifloxacin on QTc interval in healthy Korean male subjects. Drugs R&D 2014, 14, 63–71. [Google Scholar]
- Amankwa, K.; Krishnan, S.C.; Tisdale, J.E. Torsades de pointes associated with fluoroquinolones: Importance of concomitant risk factors. Clin. Pharmacol. Ther. 2004, 75, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Seop Kim, D.; Kim, K.S.; Hwan Choi, K.; Na, H.; Kim, J.I.; Shin, W.H.; Kim, E.J. Electrophysiological safety of novel fluoroquinolone antibiotic agents gemifloxacin and balofloxacin. Drug. Chem. Toxicol. 2006, 29, 303–312. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Moxifloxacin | Gemifloxacin |
|---|---|---|
| Age in Years | 27.4 ± 2.9 | 31.4 ± 5.4 |
| Male/Female Ratio | 25/5 | 25/5 |
| Height in Cm | 164 ± 5.1 | 165.3 ± 5.8 |
| Weight in Kg | 68.16 ± 5.1 | 67.4 ± 4.1 |
| Basal Mass Index (BMI) (Kg/m2) | 23.9 ± 1.7 | 24.0 ± 1.9 |
| Body Temperature (°C) | 37.1 ± 0.3 | 37 ± 0.3 |
| BP Systolic/Diastolic (mm Hg) | 120.8 ± 10/79.6 ± 4.5 | 116.8 ± 7/78.8 ± 3.3 |
| Pulse (BPM) | 77.4 ± 5.7 | 78.4 ± 6.7 |
| Drug Group | QTc Mean (ms) in Male Treated Group (Mean ± SD) | Mean QTc (ms) in Female Treated Group (Mean ± SD) | ||
|---|---|---|---|---|
| Pre Dosing Day 1st | Post Dosing Day 5th | Pre Dosing Day 1st | Post Dosing Day 5th | |
| Moxifloxacin | 404.7 ± 7.1 (n = 3) | 450 ± 0.57 (n = 3) | 449.4 (n = 1) | 473.7 (n = 1) |
| Gemifloxacin | 323.5 ± 33.2 (n = 2) | 393.5 ± 48.9 (n = 2) | (n = 0) | (n = 0) |
| Fluoroquinolone Used | Baseline ECG on Day 1 | ECG on Day 5 |
|---|---|---|
| QTc in ms | QTc in ms | |
| Moxifloxacin (n = 25) | 351 | 384 |
| 415 | 418 | |
| 421 | 433 | |
| 366 | 409 | |
| 372 | 413 | |
| 380 | 415 | |
| 371 | 373 | |
| 378 | 382 | |
| 416 | 444 | |
| 370 | 410 | |
| 377 | 400 | |
| 388 | 450.57 | |
| 436 | 450 | |
| 390 | 449.43 | |
| 416 | 444.4 | |
| 398 | 418 | |
| 401 | 400 | |
| 380 | 424 | |
| 370 | 410 | |
| 351 | 384 | |
| 348 | 413 | |
| 359 | 386 | |
| 393 | 418 | |
| 415 | 444 | |
| 449 | 473.68 |
| Fluoroquinolone Used | Baseline ECG on Day 1 | ECG on Day 5 |
|---|---|---|
| QTc in ms | QTc in ms | |
| Gemifloxacin (n = 25) | 385 | 400 |
| 386 | 388 | |
| 272 | 300 | |
| 324 | 385 | |
| 416 | 423 | |
| 300 | 359 | |
| 387 | 400 | |
| 300 | 342 | |
| 336 | 359 | |
| 363 | 368 | |
| 360 | 381 | |
| 433 | 463 | |
| 347 | 428 | |
| 405 | 404 | |
| 342 | 379 | |
| 300 | 340 | |
| 380 | 413 | |
| 282 | 320 | |
| 424 | 424 | |
| 346 | 388 | |
| 369 | 375 | |
| 360 | 377 | |
| 351 | 379 | |
| 386 | 388 | |
| 324 | 385 |
| Fluoroquinolones | Mean QTc on Day 1 | Mean QTc on Day 5 | p Value |
|---|---|---|---|
| Moxifloxacin (n = 25) | 385.8 ± 29.2 | 413.3 ± 31.4 | p < 0.0001 ** |
| Gemifloxacin (n = 25) | 351 ± 48.2 | 379 ± 41.9 | p < 0.05 |
| Event/ADEs | Moxifloxacin (n = 25) | Gemifloxacin (n = 25) | ||
|---|---|---|---|---|
| Frequency | Percentage | Frequency | Percentage | |
| Hypotension | 4/25 | 16 | 0/25 | 0 |
| Nausea and Vomiting | 4/25 | 16 | 0/25 | 0 |
| Skin flushing | 0/25 | 0 | 04/25 | 16 |
| Lightheadedness and Dizziness | 11/25 | 44 | 0/25 | 0 |
| Diarrhea | 4/25 | 16 | 0/25 | 0 |
| Fluoroquinolone Used | Baseline ECG on Day 1st | ECG on Day 5th |
|---|---|---|
| QRS in ms | QRS in ms | |
| Moxifloxacin (n = 25) | 60 | 60 |
| 60 | 60 | |
| 40 | 40 | |
| 80 | 80 | |
| 60 | 120 | |
| 60 | 60 | |
| 80 | 100 | |
| 80 | 100 | |
| 100 | 120 | |
| 120 | 140 | |
| 120 | 120 | |
| 100 | 120 | |
| 80 | 120 | |
| 80 | 140 | |
| 100 | 100 | |
| 100 | 100 | |
| 60 | 60 | |
| 60 | 60 | |
| 80 | 120 | |
| 80 | 120 | |
| 80 | 90 | |
| 60 | 60 | |
| 60 | 60 | |
| 80 | 120 | |
| 80 | 80 |
| Fluoroquinolone Used | Baseline ECG on Day 1st | ECG on Day 5th |
|---|---|---|
| QRS in ms | QRS in ms | |
| Gemifloxacin (n = 25) | 60 | 60 |
| 60 | 80 | |
| 60 | 60 | |
| 60 | 60 | |
| 80 | 80 | |
| 60 | 60 | |
| 60 | 80 | |
| 60 | 40 | |
| 80 | 60 | |
| 60 | 60 | |
| 60 | 80 | |
| 60 | 80 | |
| 60 | 60 | |
| 60 | 80 | |
| 80 | 60 | |
| 60 | 80 | |
| 80 | 60 | |
| 60 | 60 | |
| 60 | 60 | |
| 60 | 60 | |
| 60 | 60 | |
| 60 | 60 | |
| 60 | 60 | |
| 60 | 80 | |
| 60 | 60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ullah, A.; Ahmad, S.; Ali, N.; Hussain, H.; Allahyani, M.; Almehmadi, M.; Alsaiari, A.A.; Abdulaziz, O.; Almarshad, F.; Bukhari, S.H. The Effects of Moxifloxacin and Gemifloxacin on the ECG Morphology in Healthy Volunteers: A Phase 1 Randomized Clinical Trial. Diagnostics 2023, 13, 1234. https://doi.org/10.3390/diagnostics13071234
Ullah A, Ahmad S, Ali N, Hussain H, Allahyani M, Almehmadi M, Alsaiari AA, Abdulaziz O, Almarshad F, Bukhari SH. The Effects of Moxifloxacin and Gemifloxacin on the ECG Morphology in Healthy Volunteers: A Phase 1 Randomized Clinical Trial. Diagnostics. 2023; 13(7):1234. https://doi.org/10.3390/diagnostics13071234
Chicago/Turabian StyleUllah, Abid, Shujaat Ahmad, Niaz Ali, Haya Hussain, Mamdouh Allahyani, Mazen Almehmadi, Ahad Amer Alsaiari, Osama Abdulaziz, Feras Almarshad, and Syeda Hajira Bukhari. 2023. "The Effects of Moxifloxacin and Gemifloxacin on the ECG Morphology in Healthy Volunteers: A Phase 1 Randomized Clinical Trial" Diagnostics 13, no. 7: 1234. https://doi.org/10.3390/diagnostics13071234
APA StyleUllah, A., Ahmad, S., Ali, N., Hussain, H., Allahyani, M., Almehmadi, M., Alsaiari, A. A., Abdulaziz, O., Almarshad, F., & Bukhari, S. H. (2023). The Effects of Moxifloxacin and Gemifloxacin on the ECG Morphology in Healthy Volunteers: A Phase 1 Randomized Clinical Trial. Diagnostics, 13(7), 1234. https://doi.org/10.3390/diagnostics13071234