
Imaging Characteristics of Diffuse Idiopathic Skeletal Hyperostosis: More Than Just Spinal Bony Bridges
Abstract
1. Introduction
2. Axial Skeleton
2.1. New Bone Formation in the Spine
2.2. Cervical Spine
2.3. Thoracic Spine
2.4. Lumbar Spine
2.5. Sacroiliac Joints
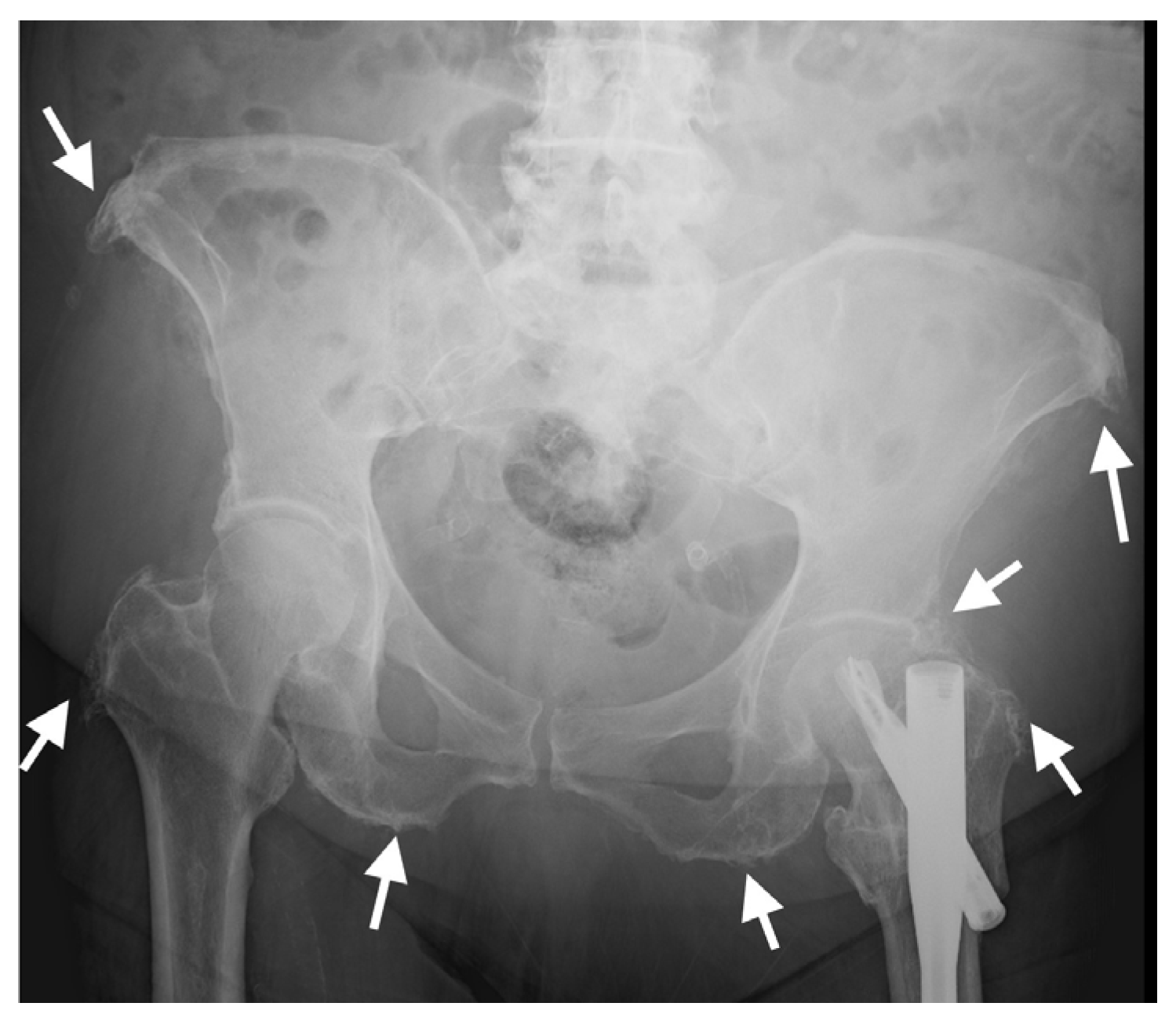
3. Pelvis and Appendicular Skeleton
4. DISH vs. SpA
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Resnick, D.; Niwayama, G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976, 119, 559–568. [Google Scholar] [CrossRef]
- Resnick, D.; Niwayama, G. Entheses and enthesopathy. Anatomical, pathological, and radiological correlation. Radiology 1983, 146, 1–9. [Google Scholar] [CrossRef]
- Slonimsky, E.; Leibushor, N.; Aharoni, D.; Lidar, M.; Eshed, I. Pelvic enthesopathy on CT is significantly more prevalent in patients with diffuse idiopathic skeletal hyperostosis (DISH) compared with matched control patients. Clin. Rheumatol. 2015, 35, 1823–1827. [Google Scholar] [CrossRef]
- Resnick, D.; Shaul, S.R.; Robins, J.M. Diffuse idiopathic skeletal hyperostosis (DISH): Forestier’s disease with extraspinal manifestations. Radiology 1975, 115, 513–524. [Google Scholar] [CrossRef]
- Mader, R.; Novofestovski, I.; Adawi, M.; Lavi, I. Metabolic syndrome and cardiovascular risk in patients with diffuse idiopathic skeletal hyperostosis. Semin. Arthritis Rheum. 2009, 38, 361–365. [Google Scholar] [CrossRef]
- Le, H.V.; Wick, J.B.; Van, B.W.; Klineberg, E.O. Diffuse Idiopathic Skeletal Hyperostosis of the Spine: Pathophysiology, Diagnosis, and Management. J. Am. Acad. Orthop. Surg. 2021, 29, 1044–1051. [Google Scholar] [CrossRef]
- Mader, R.; Verlaan, J.J.; Buskila, D. Diffuse idiopathic skeletal hyperostosis: Clinical features and pathogenic mechanisms. Nat. Rev. 2013, 9, 741–750. [Google Scholar] [CrossRef]
- Rustagi, T.; Drazin, D.; Oner, C.; York, J.; Schroeder, G.D.; Vaccaro, A.R.; Oskouian, R.J.; Chapman, J.R. Fractures in Spinal Ankylosing Disorders: A Narrative Review of Disease and Injury Types, Treatment Techniques, and Outcomes. J. Orthop. Trauma 2017, 31, S57–S74. [Google Scholar] [CrossRef]
- Dan Lantsman, C.; Barkay, G.; Friedlander, A.; Barbi, M.; Stern, M.; Eshed, I. Whole Spine CT Scan for the Detection of Acute Spinal Fractures in Diffuse Idiopathic Skeletal Hyperostosis Patients Who Sustained Low-energy Trauma. Spine 2020, 45, 1348–1353. [Google Scholar] [CrossRef]
- Yaniv, G.; Bader, S.; Lidar, M.; Herman, A.; Shazar, N.; Aharoni, D.; Eshed, I. The natural course of bridging osteophyte formation in diffuse idiopathic skeletal hyperostosis: Retrospective analysis of consecutive CT examinations over 10 years. Rheumatology 2014, 53, 1951–1957. [Google Scholar] [CrossRef]
- Utsinger, P.D. Diffuse idiopathic skeletal hyperostosis. Clin. Rheum. Dis. 1985, 11, 325–351. [Google Scholar] [CrossRef]
- Kuperus, J.S.; Mohamed Hoesein, F.A.; de Jong, P.A.; Verlaan, J.J. Diffuse idiopathic skeletal hyperostosis: Etiology and clinical relevance. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101527. [Google Scholar] [CrossRef]
- Clavaguera, T.; Reyner, P.; Buxó, M.; Valls, M.; Armengol, E.; Juanola, X. Identifying Clinicoradiological Phenotypes in Diffuse Idiopathic Skeletal Hyperostosis: A Cross-Sectional Study. Medicina 2021, 57, 1005. [Google Scholar] [CrossRef]
- Mader, R.; Verlaan, J.-J.; Eshed, I.; Jacome, B.-A.; Puttini, P.S.; Atzeni, F.; Buskila, D.; Reinshtein, E.; Novofastovski, I.; Fawaz, A.; et al. Diffuse idiopathic skeletal hyperostosis (DISH): Where we are now and where to go next. RMD Open 2017, 3, e000472. [Google Scholar] [CrossRef]
- Pariente-Rodrigo, E.; Sgaramella, G.A.; Olmos-Martínez, J.M.; Pini-Valdivieso, S.F.; Landeras-Alvaro, R.; Hernández-Hernández, J.L. Relationship between diffuse idiopathic skeletal hyperostosis, abdominal aortic calcification and associated metabolic disorders: Data from the Camargo Cohort. Med. Clín. 2017, 149, 196–202. [Google Scholar] [CrossRef]
- Mader, R.; Pappone, N.; Baraliakos, X.; Eshed, I.; Sarzi-Puttini, P.; Atzeni, F.; Bieber, A.; Novofastovski, I.; Kiefer, D.; Verlaan, J.-J.; et al. Diffuse Idiopathic Skeletal Hyperostosis (DISH) and a Possible Inflammatory Component. Curr. Rheumatol. Rep. 2021, 23, 6. [Google Scholar] [CrossRef]
- McGonagle, D.; Marzo-Ortega, H.; O’Connor, P.; Gibbon, W.; Pease, C.; Reece, R.; Emery, P. The role of biomechanical factors and HLA-B27 in magnetic resonance imaging-determined bone changes in plantar fascia enthesopathy. Arthritis Rheum. 2002, 46, 489–493. [Google Scholar] [CrossRef]
- Benjamin, M.; McGonagle, D. Histopathologic changes at “synovio–entheseal complexes” suggesting a novel mechanism for synovitis in osteoarthritis and spondylarthritis. Arthritis Rheum. 2007, 56, 3601–3609. [Google Scholar] [CrossRef]
- Aouad, K.; Ziade, N.; Baraliakos, X. Structural progression in axial spondyloarthritis. Jt. Bone Spine 2020, 87, 131–136. [Google Scholar] [CrossRef]
- van der Heijde, D.; Østergaard, M.; Reveille, J.D.; Baraliakos, X.; Kronbergs, A.; Sandoval, D.M.; Li, X.; Carlier, H.; Adams, D.H.; Maksymowych, W.P. Spinal Radiographic Progression and Predictors of Progression in Patients With Radiographic Axial Spondyloarthritis Receiving Ixekizumab Over 2 Years. J. Rheumatol. 2022, 49, 265–273. [Google Scholar] [CrossRef]
- Baraliakos, X.; Heldmann, F.; Callhoff, J.; Listing, J.; Appelboom, T.; Brandt, J.; Van den Bosch, F.; Breban, M.; Burmester, G.; Dougados, M.; et al. Which spinal lesions are associated with new bone formation in patients with ankylosing spondylitis treated with anti-TNF agents? A long-term observational study using MRI and conventional radiography. Ann. Rheum. Dis. 2014, 73, 1819–1825. [Google Scholar] [CrossRef]
- Maksymowych, W.P.; Chiowchanwisawakit, P.; Clare, T.; Pedersen, S.J.; Østergaard, M.; Lambert, R.G.W. Inflammatory lesions of the spine on magnetic resonance imaging predict the development of new syndesmophytes in ankylosing spondylitis: Evidence of a relationship between inflammation and new bone formation. Arthritis Rheum. 2009, 60, 93–102. [Google Scholar] [CrossRef]
- Thompson, C.; Moga, R.; Crosby, E.T. Failed videolaryngoscope intubation in a patient with diffuse idiopathic skeletal hyperostosis and spinal cord injury. Can. J. Anaesth. 2010, 57, 679–682. [Google Scholar] [CrossRef]
- Baraliakos, X.; Listing, J.; Buschmann, J.C.; Von Der Recke, A.; Braun, J. A comparison of new bone formation in patients with ankylosing spondylitis and patients with diffuse idiopathic skeletal hyperostosis: A retrospective cohort study over six years. Arthritis Rheum. 2012, 64, 1127–1133. [Google Scholar] [CrossRef]
- Gliner-Ron, M.; Bercovich, E.; Herman, A.; Lidar, M.; Militianu, D.; Eshed, I. Osteophytes’ position in subjects with DISH and right-sided aorta: Verification of the ‘aortic pulsation protective effect’ theory. Rheumatology 2022, 61, 4910–4914. [Google Scholar] [CrossRef]
- Bunmaprasert, T.; Keeratiruangrong, J.; Sugandhavesa, N.; Riew, K.D.; Liawrungrueang, W. Surgical management of Diffuse Idiopathic Skeletal Hyperostosis (DISH) causing secondary dysphagia (Narrative review). J. Orthop. Surg. 2021, 29, 1–9. [Google Scholar] [CrossRef]
- Weinfeld, R.M.; Olson, P.N.; Maki, D.D.; Griffiths, H.J. The prevalence of diffuse idiopathic skeletal hyperostosis (DISH) in two large American Midwest metropolitan hospital populations. Skelet. Radiol. 1997, 26, 222–225. [Google Scholar] [CrossRef]
- Kiss, C.; O’Neill, T.; Mituszova, M.; Szilágyi, M.; Poór, G. The prevalence of diffuse idiopathic skeletal hyperostosis in a population-based study in Hungary. Scand. J. Rheumatol. 2002, 31, 226–229. [Google Scholar] [CrossRef]
- Mori, K.; Yayama, T.; Nishizawa, K.; Nakamura, A.; Mimura, T.; Imai, S. Aortic pulsation prevents the development of ossification of anterior longitudinal ligament toward the aorta in patients with diffuse idiopathic skeletal hyperostosis (DISH) in Japanese: Results of chest CT-based cross-sectional study. J. Orthop. Sci. 2019, 24, 30–34. [Google Scholar] [CrossRef]
- Arad, U.; Elkayam, O.; Eshed, I. Magnetic resonance imaging in diffuse idiopathic skeletal hyperostosis: Similarities to axial spondyloarthritis. Ann. Rheum. Dis. 2013, 72, A760–A761. [Google Scholar] [CrossRef]
- Latourte, A.; Charlon, S.; Etcheto, A.; Feydy, A.; Allanore, Y.; Dougados, M.; Molto, A. Imaging Findings Suggestive of Axial Spondyloarthritis in Diffuse Idiopathic Skeletal Hyperostosis. Arthritis Care Res. 2017, 70, 145–152. [Google Scholar] [CrossRef]
- Mader, R.; Baraliakos, X.; Eshed, I.; Novofastovski, I.; Bieber, A.; Verlaan, J.-J.J.-J.; Kiefer, D.; Pappone, N.; Atzeni, F. Imaging of diffuse idiopathic skeletal hyperostosis (DISH). RMD Open 2020, 6, e001151. [Google Scholar] [CrossRef]
- Verlaan, J.J.; Boswijk, P.F.; de Ru, J.A.; Dhert, W.J.; Oner, F.C. Diffuse idiopathic skeletal hyperostosis of the cervical spine: An underestimated cause of dysphagia and airway obstruction. Spine J. 2011, 11, 1058–1067. [Google Scholar] [CrossRef]
- Kim, B.S.; Moon, M.S.; Yoon, M.G.; Kim, S.T.; Kim, S.J.; Kim, M.S.; Kim, D.S. Prevalence of Diffuse Idiopathic Skeletal Hyperostosis Diagnosed by Whole Spine Computed Tomography: A Preliminary Study. Clin. Orthop. Surg. 2018, 10, 41–46. [Google Scholar] [CrossRef]
- Bakker, J.T.; Kuperus, J.S.; Kuijf, H.J.; Oner, F.C.; De Jong, P.A.; Verlaan, J.-J. Morphological characteristics of diffuse idiopathic skeletal hyperostosis in the cervical spine. PLoS ONE 2017, 12, e0188414. [Google Scholar] [CrossRef]
- Verlaan, J.J.; Westerveld, L.A.; van Keulen, J.W.; Bleys, R.L.A.W.; Dhert, W.J.; van Herwaarden, J.A.; Moll, F.L.; Oner, F.C. Quantitative analysis of the anterolateral ossification mass in diffuse idiopathic skeletal hyperostosis of the thoracic spine. Eur. Spine J. 2011, 20, 1474–1479. [Google Scholar] [CrossRef]
- Scholz, C.; Naseri, Y.; Hohenhaus, M.; Hubbe, U.; Klingler, J.-H. Long-term results after surgical treatment of diffuse idiopathic skeletal hyperostosis (DISH) causing dysphagia. J. Clin. Neurosci. 2019, 67, 151–155. [Google Scholar] [CrossRef]
- Camarda, A.J.; Deschamps, C.; Forest, D.I. Stylohyoid chain ossification: A discussion of etiology. Oral Surg. Oral Med. Oral Pathol. 1989, 67, 508–514. [Google Scholar] [CrossRef]
- Omnell, K.A.; Gandhi, C.; Omnell, M.L. Ossification of the human stylohyoid ligament: A longitudinal study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 226–232. [Google Scholar] [CrossRef]
- Emary, P.C.; Dornink, M.; Taylor, J.A. A rare case of Eagle syndrome and diffuse idiopathic skeletal hyperostosis in the cervical spine. J. Can. Chiropr. Assoc. 2017, 61, 167–170. [Google Scholar]
- Levy, T.; Bader, S.; Hermann, K.-G.; Yaniv, G.; Grinberg, G.; Mozes, O.; Lidar, M.; Eshed, I. Styloid Process Elongation on Cervical Spine Computed Tomography is Associated with the Enthesopathy-Related Diseases of Ankylosing Spondylitis and Diffuse Idiopathic Skeletal Hyperostosis. Isr. Med. Assoc. J. IMAJ 2017, 19, 670–673. [Google Scholar] [PubMed]
- Costantinides, F.; Vidoni, G.; Bodin, C.; Di Lenarda, R. Eagle’s syndrome: Signs and symptoms. Cranio J. Craniomandib. Pract. 2013, 31, 56–60. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Khan, M.A.; Marzo-Ortega, H.; O’connor, P.; Gibbon, W.; Emery, P. Enthesitis in spondyloarthropathy. Curr. Opin. Rheumatol. 1999, 11, 244–250. [Google Scholar] [CrossRef]
- Hirai, T.; Yoshii, T.; Nagoshi, N.; Takeuchi, K.; Mori, K.; Ushio, S.; Iwanami, A.; Yamada, T.; Seki, S.; Tsuji, T.; et al. Distribution of ossified spinal lesions in patients with severe ossification of the posterior longitudinal ligament and prediction of ossification at each segment based on the cervical OP index classification: A multicenter study (JOSL CT study). BMC Musculoskelet. Disord. 2018, 19, 107. [Google Scholar] [CrossRef] [PubMed]
- Bakhsh, W.; Saleh, A.; Yokogawa, N.; Gruber, J.; Rubery, P.T.; Mesfin, A. Cervical Ossification of the Posterior Longitudinal Ligament: A Computed Tomography–Based Epidemiological Study of 2917 Patients. Glob. Spine J. 2019, 9, 820–825. [Google Scholar] [CrossRef]
- Ramos-Remus, C.; Russell, A.S.; Gomez-Vargas, A.; Hernandez-Chavez, A.; Maksymowych, W.P.; I Gamez-Nava, J.; Gonzalez-Lopez, L.; García-Hernández, A.; Meoño-Morales, E.; Burgos-Vargas, R.; et al. Ossification of the posterior longitudinal ligament in three geographically and genetically different populations of ankylosing spondylitis and other spondyloarthropathies. Ann. Rheum. Dis. 1998, 57, 429–433. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.C.T.; Yahara, Y.; Yasuda, T.; Seki, S.; Suzuki, K.; Watanabe, K.; Makino, H.; Kamei, K.; Mori, K.; Kawaguchi, Y. Morphological characteristics of DISH in patients with OPLL and its association with high-sensitivity CRP: Inflammatory DISH. Rheumatology 2022, 61, 3981–3988. [Google Scholar] [CrossRef]
- Shingyouchi, Y.; Nagahama, A.; Niida, M. Ligamentous ossification of the cervical spine in the late middle-aged Japanese men. Its relation to body mass index and glucose metabolism. Spine 1996, 21, 2474–2478. [Google Scholar] [CrossRef]
- Murray, J.R.D.; Holmes, E.J.; Misra, R.R. Diffuse Idiopathic Skeletal Hyperostosis (DISH), in A-Z of Musculoskeletal and Trauma Radiology; Cambridge University Press: Cambridge, UK, 2008; pp. 53–54. [Google Scholar]
- Slonimsky, E.; Lidar, M.; Stern, M.; Eshed, I. Degenerative changes of the thoracic spine do exist in patients with diffuse idiopathic skeletal hyperostosis: A detailed thoracic spine CT analysis. Acta Radiol. 2018, 59, 1343–1350. [Google Scholar] [CrossRef]
- Ahmed, O.; Ramachandran, K.; Patel, Y.; Dhanapaul, S.; Meena, J.; Shetty, A.P.; Thippeswamy, P.B.; Kanna, R.M.; Rajasekaran, S. Diffuse Idiopathic Skeletal Hyperostosis Prevalence, Characteristics, and Associated Comorbidities: A Cross-Sectional Study of 1815 Whole Spine CT Scans. Glob. Spine J. 2022. [Google Scholar] [CrossRef]
- Kornelis, A.P. Diffuse Idiopathic Skeletal Hyperostosis, in Decision Making in Spinal Care; Anderson, G., Vaccaro, A.R., Eds.; Thieme Medical Publishers, Inc.: New York, NY, USA, 2007; pp. 165–167. [Google Scholar]
- Culver, G.J.; Pirson, H.S. Preventive effect of aortic pulsations on osteophyte formation in the thoracic spine. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1960, 84, 937–940. [Google Scholar] [PubMed]
- Tan, S.; Dasgupta, A.; Flynn, J.A.; Ward, M.M. Aortic-vertebral interaction in ankylosing spondylitis: Syndesmophyte development at the juxta-aortic vertebral rim. Ann. Rheum. Dis. 2019, 78, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Kuperus, J.S.; Buckens, C.F.; Šprem, J.; Oner, F.C.; de Jong, P.A.; Verlaan, J.-J. The Natural Course of Diffuse Idiopathic Skeletal Hyperostosis in the Thoracic Spine of Adult Males. J. Rheumatol. 2018, 45, 1116–1123. [Google Scholar] [CrossRef]
- Tavolaro, C.; Ghaffar, S.; Zhou, H.; Nguyen, Q.T.; Bellabarba, C.; Bransford, R.J. Is routine MRI of the spine necessary in trauma patients with ankylosing spinal disorders or is a CT scan sufficient? Spine J 2019, 19, 1331–1339. [Google Scholar] [CrossRef] [PubMed]
- Okada, E.; Yoshii, T.; Yamada, T.; Watanabe, K.; Katsumi, K.; Hiyama, A.; Watanabe, M.; Nakagawa, Y.; Okada, M.; Endo, T.; et al. Spinal fractures in patients with Diffuse idiopathic skeletal hyperostosis:A nationwide multi-institution survey. J. Orthop. Sci. 2019, 24, 601–606. [Google Scholar] [CrossRef]
- Westerveld, L.; van Bemmel, J.; Dhert, W.; Oner, F.; Verlaan, J. Clinical outcome after traumatic spinal fractures in patients with ankylosing spinal disorders compared with control patients. Spine J. 2014, 14, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, I.; D’Angelo, S.; Cutro, M.S.; Padula, A.; Peruz, G.; Montaruli, M.; Scarano, E.; Giasi, V.; Palazzi, C.; Khan, M.A. Diffuse idiopathic skeletal hyperostosis may give the typical postural abnormalities of advanced ankylosing spondylitis. Rheumatology 2007, 46, 1709–1711. [Google Scholar] [CrossRef] [PubMed]
- Kevin, B.H. Diffuse Idiopathic Skeletal Hyperostosis, in Musculoskeletal Imaging; Mihra, S.T., Imran, M.O., Kevin, B.H., Tyson, S.C., Eds.; Oxford University Press: Oxford, UK, 2019; p. 221. [Google Scholar]
- Magerl, F.; Aebi, M.; Gertzbein, S.D.; Harms, J.; Nazarian, S. A comprehensive classification of thoracic and lumbar injuries. Eur. Spine J. 1994, 3, 184–201. [Google Scholar] [CrossRef]
- Barkay, G.; Dan Lantsman, C.; Menachem, S.; Shtewee, A.; Ackshota, N.; Caspi, I.; Eshed, I.; Friedlander, A. Limitations of Plain Film Radiography in Identification of Hyperextension Fractures in Patients With Ankylosing Spinal Disorders. Glob. Spine J. 2020, 12, 24–28. [Google Scholar] [CrossRef]
- Otsuki, B.; Fujibayashi, S.; Tanida, S.; Shimizu, T.; Lyman, S.; Matsuda, S. Outcomes of lumbar decompression surgery in patients with diffuse idiopathic skeletal hyperostosis (DISH). J. Orthop. Sci. 2019, 24, 957–962. [Google Scholar] [CrossRef]
- Yamada, K.; Satoh, S.; Abe, Y.; Yanagibashi, Y.; Hyakumachi, T.; Masuda, T. Diffuse Idiopathic Skeletal Hyperostosis Extended to the Lumbar Segment Is a Risk Factor of Reoperation in Patients Treated Surgically for Lumbar Stenosis. Spine 2018, 43, 1446–1453. [Google Scholar] [CrossRef] [PubMed]
- Otsuki, B.; Fujibayashi, S.; Takemoto, M.; Kimura, H.; Shimizu, T.; Matsuda, S. Diffuse idiopathic skeletal hyperostosis (DISH) is a risk factor for further surgery in short-segment lumbar interbody fusion. Eur. Spine J. 2015, 24, 2514–2519. [Google Scholar] [CrossRef] [PubMed]
- Resnick, D.; Shapiro, R.F.; Wiesner, K.B.; Niwayama, G.; Utsinger, P.D.; Shaul, S.R. Diffuse idiopathic skeletal hyperostosis (DISH) [ankylosing hyperostosis of forestier and Rotes-Querol]. Semin. Arthritis Rheum. 1978, 7, 153–187. [Google Scholar] [CrossRef]
- Maertens, M.; Mielants, H.; Verstraete, K.; Veys, E.M. Evaluation of the involvement of axial entheses and sacroiliac joints in relation to diagnosis: Comparison among diffuse idiopathic skeletal hyperostostis (DISH), osteoarthrosis and ankylosing spondylitis. Clin. Rheumatol. 1992, 11, 551–557. [Google Scholar] [CrossRef]
- Dar, G.; Peleg, S.; Masharawi, Y.; Steinberg, N.; Rothschild, B.M.; Hershkovitz, I. The Association of Sacroiliac Joint Bridging With Other Enthesopathies in the Human Body. Spine 2007, 32, E303–E308. [Google Scholar] [CrossRef]
- Durback, M.A.; Edelstein, G.; Schumacher, H.R., Jr. Abnormalities of the sacroiliac joints in diffuse idiopathic skeletal hyperostosis: Demonstration by computed tomography. J. Rheumatol. 1988, 15, 1506–1511. [Google Scholar] [PubMed]
- Leibushor, N.; Slonimsky, E.; Aharoni, D.; Lidar, M.; Eshed, I. CT Abnormalities in the Sacroiliac Joints of Patients With Diffuse Idiopathic Skeletal Hyperostosis. Am. J. Roentgenol. 2017, 208, 834–837. [Google Scholar] [CrossRef] [PubMed]
- Yahara, Y.; Yasuda, T.; Kawaguchi, Y.; Suzuki, K.; Seki, S.; Kondo, M.; Makino, H.; Kamei, K.; Kanamori, M.; Kimura, T. Sacroiliac joint variation associated with diffuse idiopathic skeletal hyperostosis. BMC Musculoskelet. Disord. 2020, 21, 93. [Google Scholar] [CrossRef] [PubMed]
- Littlejohn, G.O.; Urowitz, M.B. Peripheral enthesopathy in diffuse idiopathic skeletal hyperostosis (DISH): A radiologic study. J. Rheumatol. 1982, 9, 568–572. [Google Scholar]
- Utsinger, P.D.; Resnick, D.; Shapiro, R. Diffuse skeletal abnormalities in Forestier disease. Arch. Intern. Med. 1976, 136, 763–768. [Google Scholar] [CrossRef]
- Fahrer, H.; Barandum, R.; Gerber, N.J.; Friederich, N.F.; Burkhardt, B.; Weisman, M.H. Pelvic manifestations of diffuse idiopathic skeletal hyperostosis (DISH): Are they clinically relevant? Rheumatol. Int. 1989, 8, 257–261. [Google Scholar] [CrossRef]
- Haller, J.; Resnick, D.; Miller, C.W.; Schils, J.P.; Kerr, R.; Bielecki, D.; Sartoris, D.J.; Gundry, C.R. Diffuse idiopathic skeletal hyperostosis: Diagnostic significance of radiographic abnormalities of the pelvis. Radiology 1989, 172, 835–839. [Google Scholar] [CrossRef]
- Mader, R.; Novofastovski, I.; Iervolino, S.; Pavlov, A.; Chervinsky, L.; Schwartz, N.; Pappone, N. Ultrasonography of peripheral entheses in the diagnosis and understanding of diffuse idiopathic skeletal hyperostosis (DISH). Rheumatol. Int. 2014, 35, 493–497. [Google Scholar] [CrossRef]
- Beyeler, C.; Thomann, S.R.; Gerber, N.J.; Kunze, C.; Aeberli, D. Diffuse idiopathic skeletal hyperostosis (DISH) of the elbow: A controlled radiological study. BMC Musculoskelet. Disord. 2015, 16, 119. [Google Scholar] [CrossRef]
- Broitman, S.; Herman, A.; Stern, M.; Lidar, M.; Eshed, I. Enthesopathy of the anterior chest wall joints in patients with diffuse idiopathic skeletal hyperostosis (DISH): A retrospective analysis of computed tomography scans. Skelet. Radiol. 2019, 49, 461–467. [Google Scholar] [CrossRef]
- Mader, R.; Sarzi-Puttini, P.; Atzeni, F.; Olivieri, I.; Pappone, N.; Verlaan, J.-J.; Buskila, D. Extraspinal manifestations of diffuse idiopathic skeletal hyperostosis. Rheumatology 2009, 48, 1478–1481. [Google Scholar] [CrossRef]
- Kuperus, J.S.; Waalwijk, J.F.; Regan, E.; Van Der Horst-Bruinsma, I.E.; Oner, F.C.; De Jong, P.A.; Verlaan, J.-J. Simultaneous occurrence of ankylosing spondylitis and diffuse idiopathic skeletal hyperostosis: A systematic review. Rheumatology 2018, 57, 2120–2128. [Google Scholar] [CrossRef]
- Hermann, K.-G.A.; Zejden, A.; Sudoł-Szopińska, I.; Eshed, I. Imaging to Differentiate the Various Forms of Seronegative Arthritis. Semin. Musculoskelet. Radiol. 2018, 22, 189–196. [Google Scholar] [CrossRef]
- Bywaters, E.G.; Dixon, A.S. Paravertebral ossification in psoriatic arthritis. Ann. Rheum. Dis. 1965, 24, 313–331. [Google Scholar] [CrossRef]
- Haddad, A.; Thavaneswaran, A.; Toloza, S.; Chandran, V.; Gladman, D.D. Diffuse Idiopathic Skeletal Hyperostosis in Psoriatic Arthritis. J. Rheumatol. 2013, 40, 1367–1373. [Google Scholar] [CrossRef]
- McEwen, C.; Ditata, D.; Lingg, C.; Porini, A.; Good, A.; Rankin, T. Ankylosing Spondylitis and Spondylitis Accompanying Ulcerative Colitis, Regional Enteritis, Psoriasis and Reiter’s Disease. A Comparative Study. Arthritis Rheum. 1971, 14, 291–318. [Google Scholar] [CrossRef] [PubMed]
- Vernon-Roberts, B.; Pirie, C.J.; Trenwith, V. Pathology of the dorsal spine in ankylosing hyperostosis. Ann. Rheum. Dis. 1974, 33, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Slobodin, G.; Sagiv, M.; Khreish, T.; Croitoru, S.; Shouval, A.; Eshed, I. Facet joint disease in patients with axial spondyloarthritis: A retrospective computed tomography study. Semin. Arthritis Rheum. 2022, 55, 151991. [Google Scholar] [CrossRef]
- Olivieri, I.; D’Angelo, S.; Palazzi, C.; Padula, A.; Mader, R.; Khan, M.A. Diffuse idiopathic skeletal hyperostosis: Differentiation from ankylosing spondylitis. Curr. Rheumatol. Rep. 2009, 11, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Weiss, B.G.; Bachmann, L.M.; Pfirrmann, C.W.; Kissling, R.O.; Zubler, V. Whole Body Magnetic Resonance Imaging Features in Diffuse Idiopathic Skeletal Hyperostosis in Conjunction with Clinical Variables to Whole Body MRI and Clinical Variables in Ankylosing Spondylitis. J. Rheumatol. 2015, 43, 335–342. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DISH | SpA | |
|---|---|---|
| Age | Elderly (>50 years) | Young adults (>20–40) |
| Gender | M > F | M > F |
| Pathogenesis | Mechanical/localized inflammation | Inflammatory |
| Enthesopathy | Axial and peripheral | Axial and peripheral |
| Thick and pronounced With no accompanied erosions and sclerosis | Thin, with accompanied erosions and sclerosis | |
| Spine | ||
| Bone production | Thick, bridging horizontal osteophytes | Thin, slender, vertical syndesmophytes |
| MRI | ||
| BME corners | Present but uncommon | Common |
| Fat corners | Present, not rare | Common |
| Periarticular fat metaplasia | Rare | Common |
| Sacroiliac joints | ||
| Bone production | Bridging osteophytes Anterior to SIJ | Intra-articular bridging osteophytes |
| Erosions | Rare | Common |
| MRI | ||
| Periarticular BME, suggestive of SpA | Rare Upper part of SIJ | Common Along entire SIJ |
| Periarticular fat metaplasia | Rare | Common |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eshed, I. Imaging Characteristics of Diffuse Idiopathic Skeletal Hyperostosis: More Than Just Spinal Bony Bridges. Diagnostics 2023, 13, 563. https://doi.org/10.3390/diagnostics13030563
Eshed I. Imaging Characteristics of Diffuse Idiopathic Skeletal Hyperostosis: More Than Just Spinal Bony Bridges. Diagnostics. 2023; 13(3):563. https://doi.org/10.3390/diagnostics13030563
Chicago/Turabian StyleEshed, Iris. 2023. "Imaging Characteristics of Diffuse Idiopathic Skeletal Hyperostosis: More Than Just Spinal Bony Bridges" Diagnostics 13, no. 3: 563. https://doi.org/10.3390/diagnostics13030563
APA StyleEshed, I. (2023). Imaging Characteristics of Diffuse Idiopathic Skeletal Hyperostosis: More Than Just Spinal Bony Bridges. Diagnostics, 13(3), 563. https://doi.org/10.3390/diagnostics13030563