
A Preclinical Feasibility Study of Single-Port Robotic Subcostal Anatomical Lung Resection and Subxiphoid Thymectomy Using the da Vinci® SP System


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Overview of the da Vinci® SP System
2.2. Study Setting
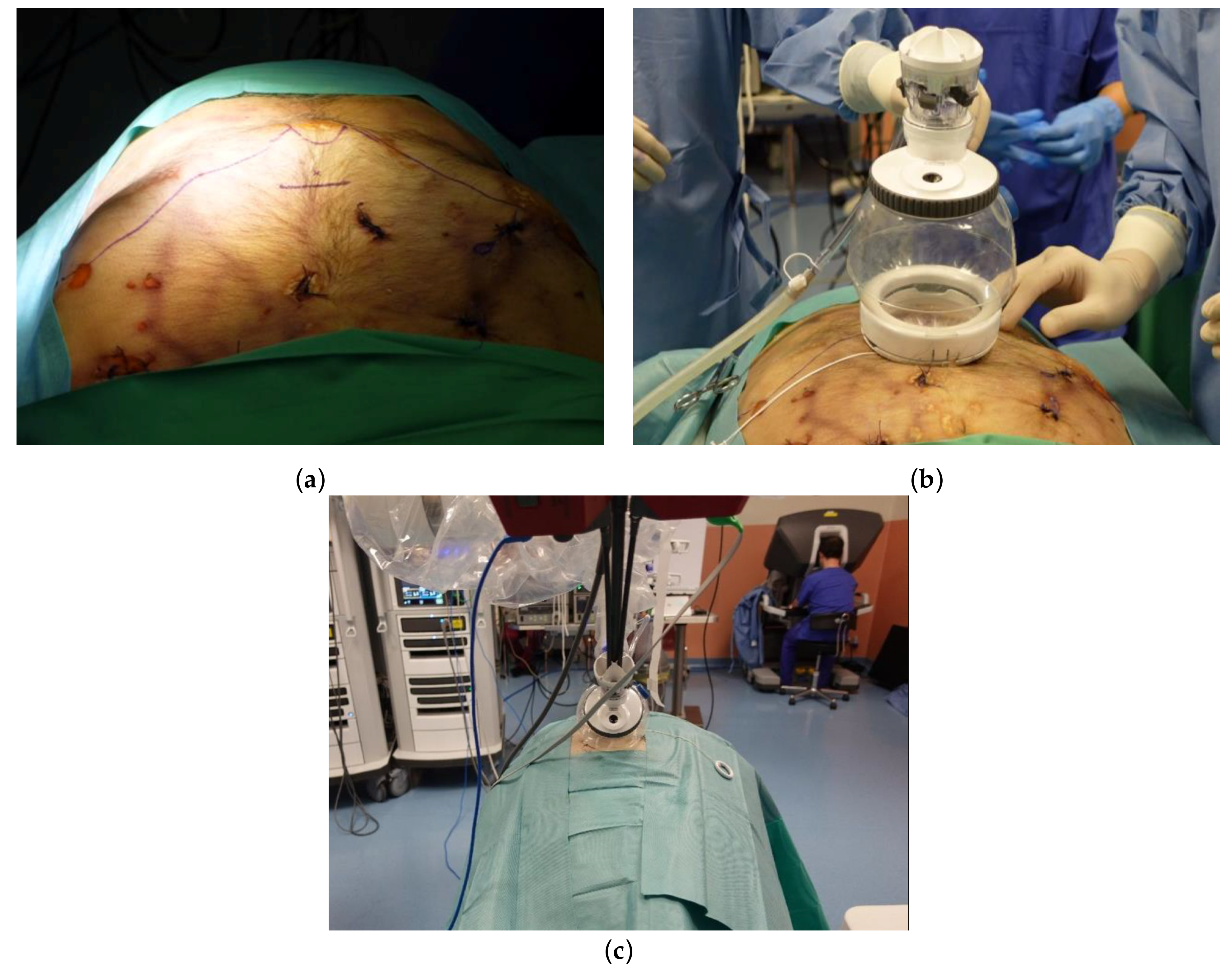
2.3. Uniportal Subxiphoid Thymectomy
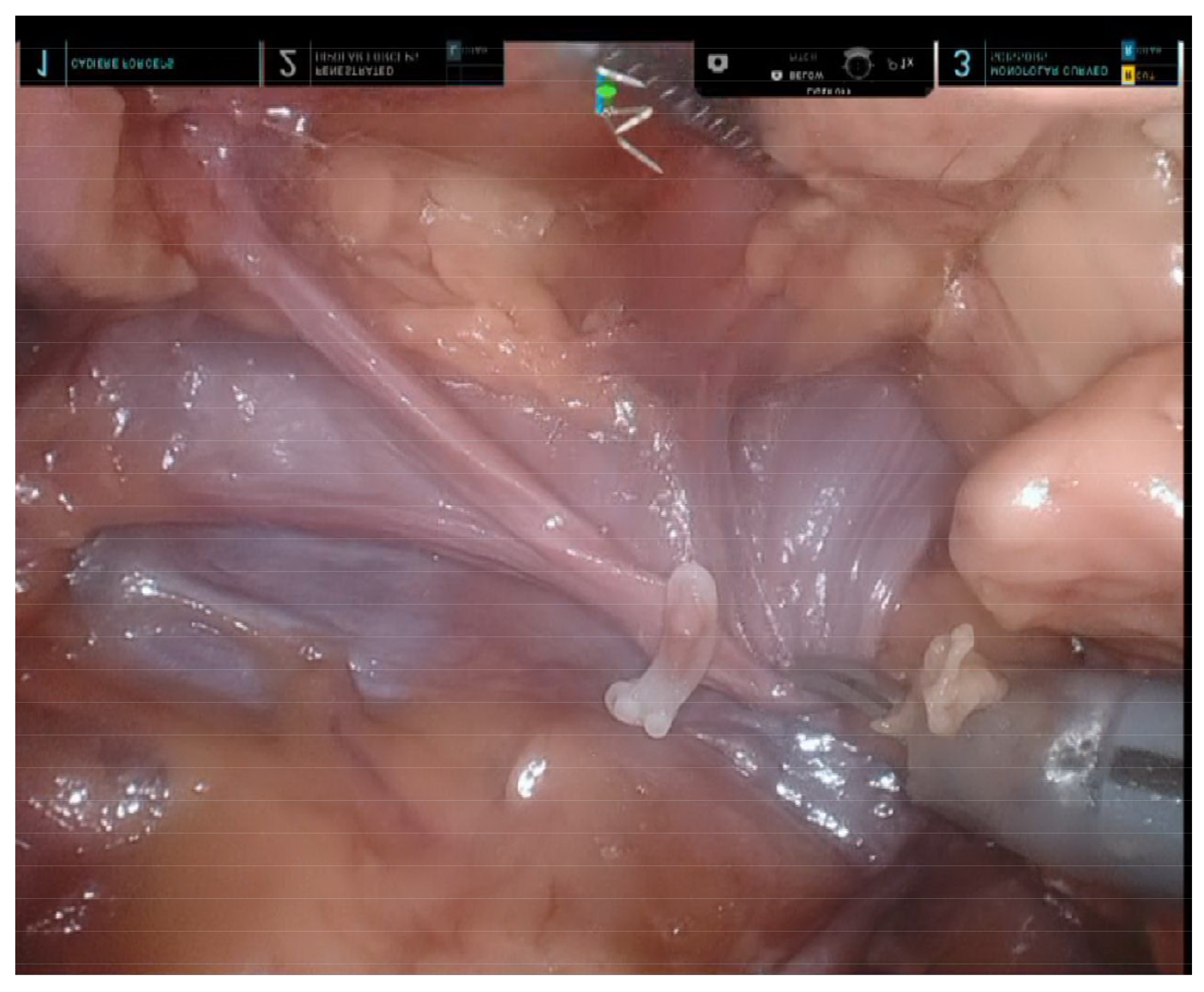
2.4. Uniportal Subcostal Anatomical Lung Resection
3. Results
3.1. Uniportal Subxiphoid Thymectomy
3.2. Uniportal Subcostal Anatomical Lung Resection
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roviaro, G.; Varoli, F.; Rebuffat, C.; Vergani, C.; D’Hoore, A.; Scalambra, S.M.; Maciocco, M.; Grignani, F. Major Pulmonary Resections: Pneumonectomies and Lobectomies. Ann. Thorac. Surg. 1993, 56, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Sihoe, A.D. Video-Assisted Thoracoscopic Surgery as the Gold Standard for Lung Cancer Surgery. Respirology 2020, 25, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Sihoe, A.D. Uniportal Lung Cancer Surgery: State of the Evidence. Ann. Thorac. Surg. 2019, 107, 962–972. [Google Scholar] [CrossRef] [PubMed]
- Bertolaccini, L.; Batirel, H.; Brunelli, A.; Gonzalez-Rivas, D.; Ismail, M.; Ucar, A.M.; Ng, C.S.; Scarci, M.; Sihoe, A.D.; Ugalde, P.A. Uniportal Video-Assisted Thoracic Surgery Lobectomy: A Consensus Report from the Uniportal Vats Interest Group (Uvig) of the European Society of Thoracic Surgeons (Ests). Eur. J. Cardiothorac. Surg. 2019, 56, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Jin, R.; Yang, S.; Park, B.J.; Li, H. Long-Term and Short-Term Outcomes of Robot-Versus Video-Assisted Anatomic Lung Resection in Lung Cancer: A Systematic Review and Meta-Analysis. Eur. J. Cardiothorac. Surg. 2021, 59, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Jin, R.; Zheng, Y.; Yuan, Y.; Han, D.; Cao, Y.; Zhang, Y.; Li, C.; Xiang, J.; Zhang, Z.; Niu, Z. Robotic-Assisted Versus Video-Assisted Thoracoscopic Lobectomy: Short-Term Results of a Randomized Clinical Trial (Rvlob Trial). Ann. Surg. 2022, 275, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.Y.; Tsang, R.K.; Holsinger, F.C.; Tong, M.C.; Ng, C.W.; Chiu, P.W.; Ng, S.S.; Wong, E.W. Prospective Clinical Trial to Evaluate Safety and Feasibility of Using a Single Port Flexible Robotic System for Transoral Head and Neck Surgery. Oral Oncol. 2019, 94, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Lai, A.; Dobbs, R.W.; Talamini, S.; Halgrimson, W.R.; Wilson, J.O.; Vigneswaran, H.T.; Crivellaro, S. Single Port Robotic Radical Prostatectomy: A Systematic Review. Transl. Androl. Urol. 2020, 9, 898. [Google Scholar] [CrossRef] [PubMed]
- Dobbs, R.W.; Halgrimson, W.R.; Talamini, S.; Vigneswaran, H.T.; Wilson, J.O.; Crivellaro, S. Single-Port Robotic Surgery: The Next Generation of Minimally Invasive Urology. World J. Urol. 2020, 38, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Leow, O.Q.Y.; Cheng, C.; Chao, Y.K. Trans-Subxiphoid Robotic Surgery for Anterior Mediastinal Disease: An Initial Case Series. J. Thorac. Dis. 2020, 12, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Morelli, L.; Guadagni, S.; Di Franco, G.; Palmeri, M.; Di Candio, G.; Mosca, F. Da Vinci Single Site© Surgical Platform in Clinical Practice: A Systematic Review. Int. J. Med. Robot 2016, 12, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Kroh, M.; El-Hayek, K.; Rosenblatt, S.; Chand, B.; Escobar, P.; Kaouk, J.; Chalikonda, S. First Human Surgery with a Novel Single-Port Robotic System: Cholecystectomy Using the Da Vinci Single-Site Platform. Surg. Endosc. 2011, 25, 3566–3573. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Han, K.N.; Hong, J.I.; Kim, H.K.; Kim, D.J.; Choi, Y.H. Subxiphoid Approach for Robotic Single-Site-Assisted Thymectomy. Eur. J. Cardiothorac. Surg. 2020, 58, i34–i38. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Kim, H.K.; Jang, D.-S.; Han, K.N.; Kim, D.J. Initial Experiences with Robotic Single-Site Thoracic Surgery for Mediastinal Masses. Ann. Thorac. Surg. 2019, 107, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Chiu, C.H.; Chao, Y.K.; Liu, Y.H. Subxiphoid Approach for Video-Assisted Thoracoscopic Surgery: An Update. J. Thorac. Dis. 2018, 10, S1662–S1665. [Google Scholar] [CrossRef] [PubMed]
- Suda, T.; Hachimaru, A.; Tochii, D.; Maeda, R.; Tochii, S.; Takagi, Y. Video-Assisted Thoracoscopic Thymectomy Versus Subxiphoid Single-Port Thymectomy: Initial Results. Eur. J. Cardiothorac. Surg. 2016, 49, i54–i58. [Google Scholar] [CrossRef] [PubMed]
- Kang, C.H.; Na, K.J.; Song, J.W.; Bae, S.Y.; Park, S.; Park, I.K.; Kim, Y.T. The Robotic Thymectomy Via the Subxiphoid Approach: Technique and Early Outcomes. Eur. J. Cardiothorac. Surg. 2020, 58, i39–i43. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.F.; Cheng, C.; Suen, K.H.; Stein, H.; Chao, Y.K. A Preclinical Feasibility Study of Single-Port Robotic Subcostal Anatomical Lung Resection and Subxiphoid Thymectomy Using the da Vinci® SP System. Diagnostics 2023, 13, 460. https://doi.org/10.3390/diagnostics13030460
Wu CF, Cheng C, Suen KH, Stein H, Chao YK. A Preclinical Feasibility Study of Single-Port Robotic Subcostal Anatomical Lung Resection and Subxiphoid Thymectomy Using the da Vinci® SP System. Diagnostics. 2023; 13(3):460. https://doi.org/10.3390/diagnostics13030460
Chicago/Turabian StyleWu, Ching Feng, Chuan Cheng, Ka Hei Suen, Hubert Stein, and Yin Kai Chao. 2023. "A Preclinical Feasibility Study of Single-Port Robotic Subcostal Anatomical Lung Resection and Subxiphoid Thymectomy Using the da Vinci® SP System" Diagnostics 13, no. 3: 460. https://doi.org/10.3390/diagnostics13030460
APA StyleWu, C. F., Cheng, C., Suen, K. H., Stein, H., & Chao, Y. K. (2023). A Preclinical Feasibility Study of Single-Port Robotic Subcostal Anatomical Lung Resection and Subxiphoid Thymectomy Using the da Vinci® SP System. Diagnostics, 13(3), 460. https://doi.org/10.3390/diagnostics13030460