
Clinicopathological Features and Significance of Epidermal Growth Factor Receptor Mutation in Surgically Resected Early-Stage Lung Adenocarcinoma

 ,
,
Abstract
1. Introduction
2. Materials and Methods
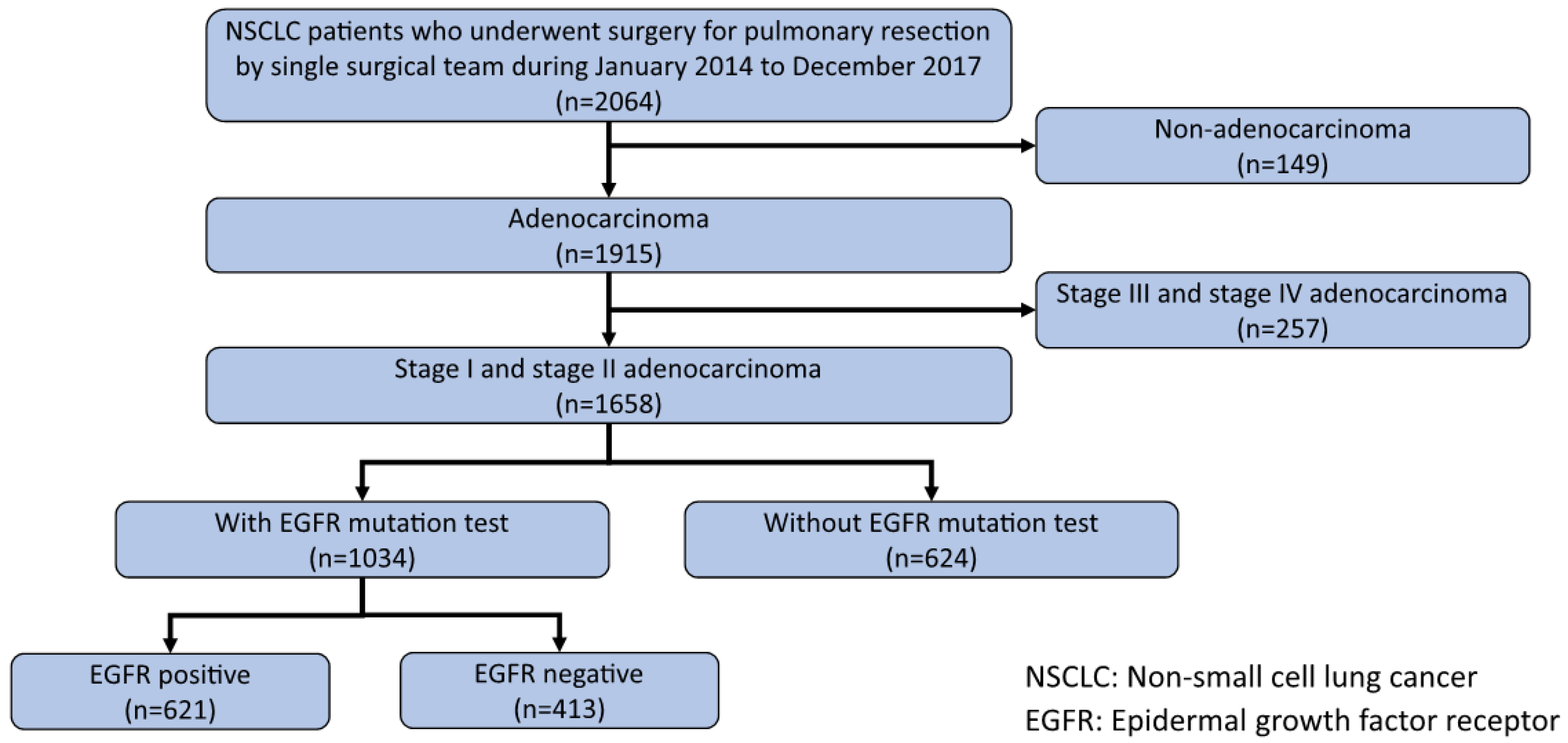
2.1. Study Population
2.2. Management and Follow-up
2.3. Analysis of EGFR Mutation
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics and Clinicopathological Characteristics
3.2. Clinical and Pathological Characteristics of Tumors with EGFR Exon 19 Deletion and L858R Mutation
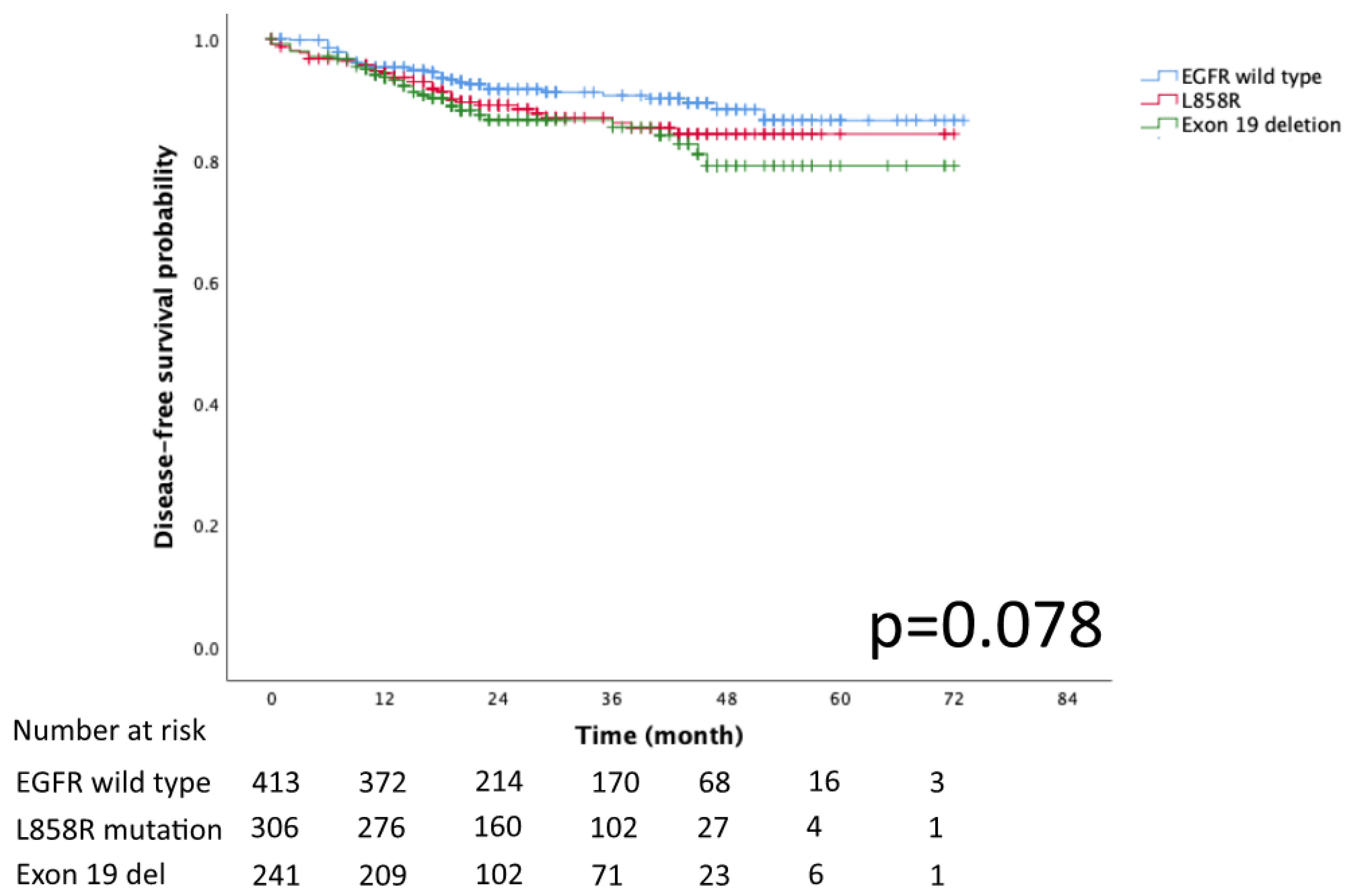
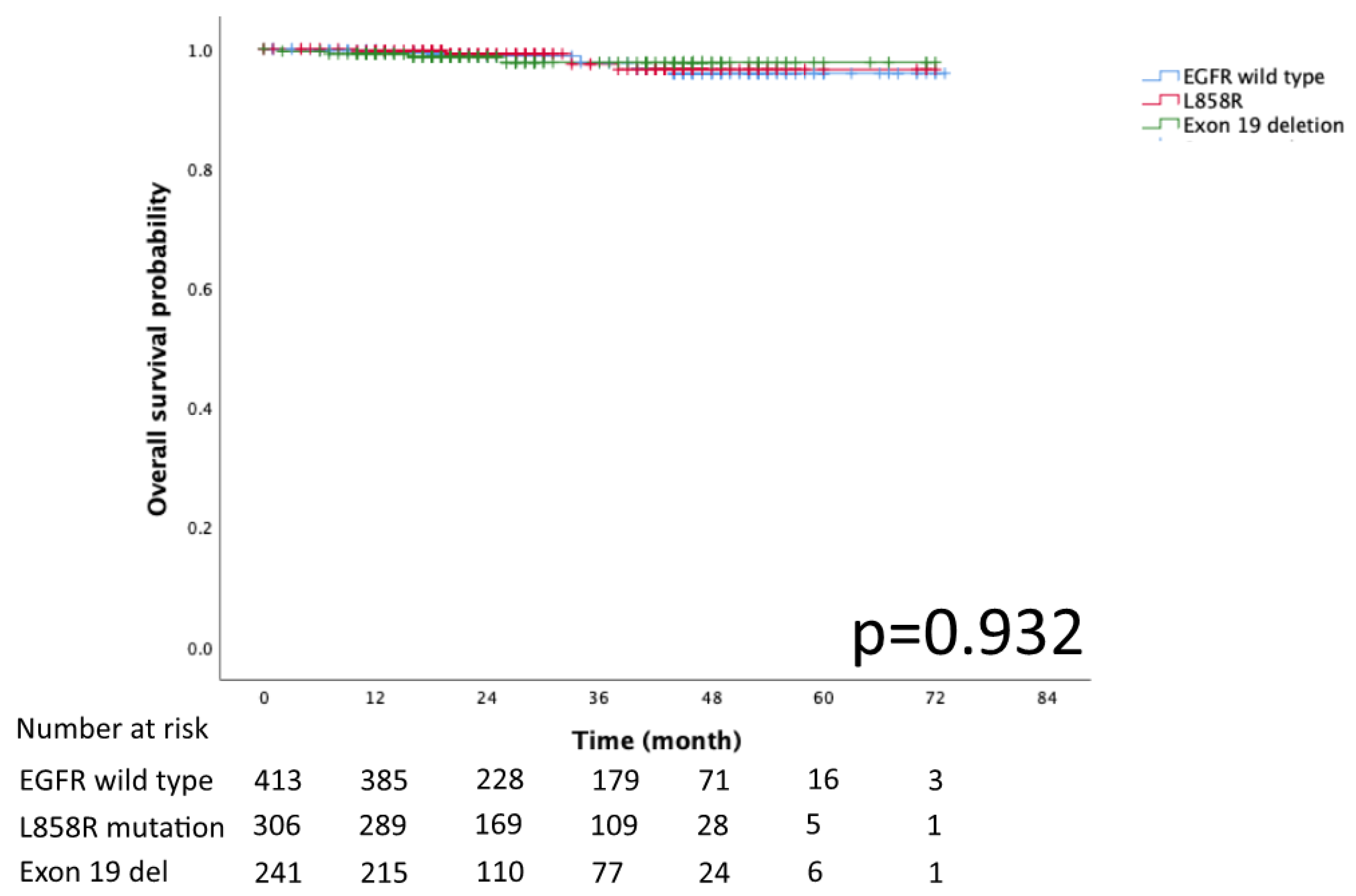
3.3. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gelatti, A.C.Z.; Drilon, A.; Santini, F.C. Optimizing the sequencing of tyrosine kinase inhibitors (TKIs) in epidermal growth factor receptor (EGFR) mutation-positive non-small cell lung cancer (NSCLC). Lung Cancer 2019, 137, 113–122. [Google Scholar] [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; et al. Overall Survival with Osimertinib in Untreated, EGFR-Mutated Advanced NSCLC. N. Engl. J. Med. 2020, 382, 41–50. [Google Scholar] [CrossRef]
- Wu, Y.L.; Tsuboi, M.; He, J.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Laktionov, K.; Kim, S.W.; Kato, T.; et al. Osimertinib in Resected EGFR-Mutated Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2020, 383, 1711–1723. [Google Scholar] [CrossRef]
- Lin, M.W.; Su, K.Y.; Su, T.J.; Chang, C.C.; Lin, J.W.; Lee, Y.H.; Yu, S.L.; Chen, J.S.; Hsieh, M.S. Clinicopathological and genomic comparisons between different histologic components in combined small cell lung cancer and non-small cell lung cancer. Lung Cancer 2018, 125, 282–290. [Google Scholar] [CrossRef]
- Chiang, X.H.; Lu, T.P.; Hsieh, M.S.; Tsai, T.M.; Liao, H.C.; Kao, T.N.; Chang, C.H.; Lin, M.W.; Hsu, H.H.; Chen, J.S. Thoracoscopic Wedge Resection Versus Segmentectomy for cT1N0 Lung Adenocarcinoma. Ann. Surg. Oncol. 2021, 28, 8398–8411. [Google Scholar] [CrossRef]
- Chiang, X.H.; Hsu, H.H.; Hsieh, M.S.; Chang, C.H.; Tsai, T.M.; Liao, H.C.; Tsou, K.C.; Lin, M.W.; Chen, J.S. Propensity-Matched Analysis Comparing Survival After Sublobar Resection and Lobectomy for cT1N0 Lung Adenocarcinoma. Ann. Surg. Oncol. 2020, 27, 703–715. [Google Scholar] [CrossRef]
- Liu, H.Y.; Hsu, H.H.; Tsai, T.M.; Chiang, X.H.; Lu, T.P.; Chang, C.H.; Chen, P.H.; Wang, M.L.; Hung, M.H.; Cheng, Y.J.; et al. Nonintubated Versus Intubated Uniportal Thoracoscopic Segmentectomy for Lung Tumors. Ann. Thorac. Surg. 2021, 111, 1182–1189. [Google Scholar] [CrossRef]
- Chen, P.H.; Hsu, H.H.; Yang, S.M.; Tsai, T.M.; Tsou, K.C.; Liao, H.C.; Lin, M.W.; Chen, J.S. Preoperative Dye Localization for Thoracoscopic Lung Surgery: Hybrid Versus Computed Tomography Room. Ann. Thorac. Surg. 2018, 106, 1661–1667. [Google Scholar] [CrossRef]
- Matsumura, Y.; Owada, Y.; Yamaura, T.; Muto, S.; Osugi, J.; Hoshino, M.; Higuchi, M.; Ohira, T.; Suzuki, H.; Gotoh, M. Epidermal growth factor receptor gene mutation as risk factor for recurrence in patients with surgically resected lung adenocarcinoma: A matched-pair analysis. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 216–222. [Google Scholar] [CrossRef]
- Isaka, T.; Nakayama, H.; Ito, H.; Yokose, T.; Yamada, K.; Masuda, M. Impact of the epidermal growth factor receptor mutation status on the prognosis of recurrent adenocarcinoma of the lung after curative surgery. BMC Cancer 2018, 18, 959. [Google Scholar] [CrossRef]
- Yotsukura, M.; Yasuda, H.; Shigenobu, T.; Kaseda, K.; Masai, K.; Hayashi, Y.; Hishida, T.; Ohtsuka, T.; Naoki, K.; Soejima, K.; et al. Clinical and pathological characteristics of EGFR mutation in operable early-stage lung adenocarcinoma. Lung Cancer 2017, 109, 45–51. [Google Scholar] [CrossRef]
- Pi, C.; Xu, C.R.; Zhang, M.F.; Peng, X.X.; Wei, X.W.; Gao, X.; Yan, H.H.; Zhou, Q. EGFR mutations in early-stage and advanced-stage lung adenocarcinoma: Analysis based on large-scale data from China. Thorac. Cancer 2018, 9, 814–819. [Google Scholar] [CrossRef]
- Isaka, T.; Ito, H.; Yokose, T.; Saito, H.; Adachi, H.; Murakami, K.; Miura, J.; Kikunishi, N.; Rino, Y. Prognostic factors for relapse-free survival in stage IB-IIIA primary lung adenocarcinoma by epidermal growth factor receptor mutation status. BMC Cancer 2022, 22, 966. [Google Scholar] [CrossRef]
- Takamochi, K.; Oh, S.; Matsunaga, T.; Suzuki, K. Prognostic impacts of EGFR mutation status and subtype in patients with surgically resected lung adenocarcinoma. J. Thorac. Cardiovasc. Surg. 2017, 154, 1768–1774.e1. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Chen, Y.S.; Huang, T.W. Prognostic Impact of EBUS TBNA for Lung Adenocarcinoma Patients with Postoperative Recurrences. Diagnostics 2022, 12, 2547. [Google Scholar] [CrossRef]
- Pierre Mordant, M.D.; Brosseau, S.; Milleron, B.; Santelmo, N.; Fraboulet-Moreau, S.; Besse, B.; Langlais, A.; Gossot, D.; Thomas, P.A.; Pujol, J.L.; et al. Outcome of Patients With Resected Early-Stage Non-small Cell Lung Cancer and EGFR Mutations: Results From the IFCT Biomarkers France Study. Clin. Lung Cancer 2023, 24, 1–10. [Google Scholar] [CrossRef]
- Wu, Y.L.; John, T.; Grohe, C.; Majem, M.; Goldman, J.W.; Kim, S.W.; Kato, T.; Laktionov, K.; Vu, H.V.; Wang, Z.; et al. Postoperative Chemotherapy Use and Outcomes From ADAURA: Osimertinib as Adjuvant Therapy for Resected EGFR-Mutated NSCLC. J. Thorac. Oncol. 2022, 17, 423–433. [Google Scholar] [CrossRef]
- Hardenberg, M.C.; Patel, B.; Matthews, C.; Califano, R.; Garcia Campelo, R.; Grohe, C.; Hong, M.H.; Liu, G.; Lu, S.; de Marinis, F.; et al. The value of disease-free survival (DFS) and osimertinib in adjuvant non-small-cell lung cancer (NSCLC): An international Delphi consensus report. ESMO Open 2022, 7, 100572. [Google Scholar] [CrossRef]
- Isla, D.; Felip, E.; Garrido, P.; Insa, A.; Majem, M.; Remon, J.; Trigo, J.M.; de Castro, J. A Delphi consensus panel about clinical management of early-stage EGFR-mutated non-small cell lung cancer (NSCLC) in Spain: A Delphi consensus panel study. Clin. Transl. Oncol. 2022, 25, 283–291. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. WHO Classification of Tumours: Thoracic Tumors, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021; Volume 5, ISBN 978-92-832-4506-3. [Google Scholar]
- Hsu, K.H.; Ho, C.C.; Hsia, T.C.; Tseng, J.S.; Su, K.Y.; Wu, M.F.; Chiu, K.L.; Yang, T.Y.; Chen, K.C.; Ooi, H.; et al. Identification of five driver gene mutations in patients with treatment-naive lung adenocarcinoma in Taiwan. PLoS ONE 2015, 10, e0120852. [Google Scholar] [CrossRef]
- Castellanos, E.; Feld, E.; Horn, L. Driven by Mutations: The Predictive Value of Mutation Subtype in EGFR-Mutated Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2017, 12, 612–623. [Google Scholar] [CrossRef] [PubMed]
- Villa, C.; Cagle, P.T.; Johnson, M.; Patel, J.D.; Yeldandi, A.V.; Raj, R.; DeCamp, M.M.; Raparia, K. Correlation of EGFR mutation status with predominant histologic subtype of adenocarcinoma according to the new lung adenocarcinoma classification of the International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society. Arch. Pathol. Lab. Med. 2014, 138, 1353–1357. [Google Scholar] [PubMed]
- Kondo, Y.; Ichinose, J.; Ninomiya, H.; Hashimoto, K.; Matsuura, Y.; Nakao, M.; Ishikawa, Y.; Okumura, S.; Satoh, Y.; Mun, M. Combination of epidermal growth factor receptor mutation and the presence of high-grade patterns is associated with recurrence in resected stage I lung adenocarcinoma. Interact. Cardiovasc. Thorac. Surg. 2022, 35, ivac062. [Google Scholar] [CrossRef]
- Nie, Y.; Gao, W.; Li, N.; Chen, W.; Wang, H.; Li, C.; Zhang, H.; Han, P.; Zhang, Y.; Lv, X.; et al. Relationship between EGFR gene mutation and local metastasis of resectable lung adenocarcinoma. World J. Surg. Oncol. 2017, 15, 55. [Google Scholar] [CrossRef]
- Deng, C.; Zheng, Q.; Zhang, Y.; Jin, Y.; Shen, X.; Nie, X.; Fu, F.; Ma, X.; Ma, Z.; Wen, Z.; et al. Validation of the Novel International Association for the Study of Lung Cancer Grading System for Invasive Pulmonary Adenocarcinoma and Association With Common Driver Mutations. J. Thorac. Oncol. 2021, 16, 1684–1693. [Google Scholar] [CrossRef]
- Chen, H.; Carrot-Zhang, J.; Zhao, Y.; Hu, H.; Freeman, S.S.; Yu, S.; Ha, G.; Taylor, A.M.; Berger, A.C.; Westlake, L.; et al. Genomic and immune profiling of pre-invasive lung adenocarcinoma. Nat. Commun. 2019, 10, 5472. [Google Scholar] [CrossRef]
- Zhou, J.; Ben, S. Comparison of therapeutic effects of EGFR-tyrosine kinase inhibitors on 19Del and L858R mutations in advanced lung adenocarcinoma and effect on cellular immune function. Thorac. Cancer 2018, 9, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Sheng, J.; Kang, S.; Fang, W.; Yan, Y.; Hu, Z.; Hong, S.; Wu, X.; Qin, T.; Liang, W.; et al. Patients with exon 19 deletion were associated with longer progression-free survival compared to those with L858R mutation after first-line EGFR-TKIs for advanced non-small cell lung cancer: A meta-analysis. PLoS ONE 2014, 9, e107161. [Google Scholar] [CrossRef]
- Yu, J.Y.; Yu, S.F.; Wang, S.H.; Bai, H.; Zhao, J.; An, T.T.; Duan, J.C.; Wang, J. Clinical outcomes of EGFR-TKI treatment and genetic heterogeneity in lung adenocarcinoma patients with EGFR mutations on exons 19 and 21. Chin. J. Cancer 2016, 35, 30. [Google Scholar] [CrossRef]
- Won, Y.W.; Han, J.Y.; Lee, G.K.; Park, S.Y.; Lim, K.Y.; Yoon, K.A.; Yun, T.; Kim, H.T.; Lee, J.S. Comparison of clinical outcome of patients with non-small-cell lung cancer harbouring epidermal growth factor receptor exon 19 or exon 21 mutations. J. Clin. Pathol. 2011, 64, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Koyama, N.; Watanabe, Y.; Iwai, Y.; Kawamura, R.; Miwa, C.; Nagai, Y.; Hagiwara, K.; Koyama, S. Distinct Benefit of Overall Survival between Patients with Non-Small-Cell Lung Cancer Harboring EGFR Exon 19 Deletion and Exon 21 L858R Substitution. Chemotherapy 2017, 62, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.S.; Lin, H.M.; Crossland, V.; Churchill, E.N.; Curran, E.; Forsythe, A.; Tomaras, D.; Ou, S.I. Non-small cell lung cancer with EGFR exon 20 insertion mutation: A systematic literature review and meta-analysis of patient outcomes. Curr. Med. Res. Opin. 2022, 38, 1341–1350. [Google Scholar] [CrossRef] [PubMed]
- Janning, M.; Suptitz, J.; Albers-Leischner, C.; Delpy, P.; Tufman, A.; Velthaus-Rusik, J.L.; Reck, M.; Jung, A.; Kauffmann-Guerrero, D.; Bonzheim, I.; et al. Treatment outcome of atypical EGFR mutations in the German National Network Genomic Medicine Lung Cancer (nNGM). Ann. Oncol. 2022, 33, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Ito, H.; Date, H.; Shintani, Y.; Miyaoka, E.; Nakanishi, R.; Kadokura, M.; Endo, S.; Chida, M.; Yoshino, I.; Suzuki, H.; et al. The prognostic impact of lung adenocarcinoma predominance classification relating to pathological factors in lobectomy, the Japanese Joint Committee of Lung Cancer Registry Database in 2010. BMC Cancer 2022, 22, 875. [Google Scholar] [CrossRef] [PubMed]
- Noma, D.; Inamura, K.; Matsuura, Y.; Hirata, Y.; Nakajima, T.; Yamazaki, H.; Hirai, Y.; Ichinose, J.; Nakao, M.; Ninomiya, H.; et al. Prognostic Effect of Lymphovascular Invasion on TNM Staging in Stage I Non-Small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, e109–e122. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Li, Q.; Lin, S.; Li, W.; Yu, L.; Wang, L.; Dong, X.; Yu, L.; Li, S.; Liu, W.; et al. Prognostic implication of EGFR mutation status and subtype in resected lung adenocarcinoma patients irrespective of therapy. Clin. Transl. Oncol. 2019, 21, 298–303. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | EGFR(+) n = 621 | EGFR(−) n = 413 | p-Value |
|---|---|---|---|
| Sex, n (%) | 0.893 | ||
| Female | 411 (66.2) | 275 (66.4) | |
| Male | 210 (33.8) | 138 (33.6) | |
| Age | <0.001 | ||
| ≤65 | 365 (58.7) | 299 (72.5) | |
| >65 | 256 (41.3) | 114 (27.5) | |
| Smoking, n (%) | 0.137 | ||
| No | 538 (86.7) | 344 (83.1) | |
| Yes | 83 (13.3) | 69 (16.9) | |
| Family lung cancer history | 0.307 | ||
| No | 499 (80.4) | 321 (77.8) | |
| Yes | 122 (19.6) | 92 (22.2) | |
| CEA level | |||
| ≤5 ng/mL | 549 (88.3) | 381 (92.3) | 0.044 |
| >5 ng/mL | 72 (11.7) | 32 (7.7) | |
| Histologic predominant subtype, n (%) | <0.001 | ||
| Lepidic predominant | 52 (8.4) | 102 (24.6) | |
| Non-lepidic predominant | 569 (91.6) | 311 (75.4) | |
| Pleural invasion, PI, n (%) | 0.02 | ||
| PL0 | 510 (58.4) | 364 (88.2) | |
| PL1 | 66 (10.6) | 41 (9.9) | |
| PL2 | 39 (6.3) | 7 (1.7) | |
| PL3 | 6 (0.9) | 1 (0.2) | |
| Lymphovascular invasion, n (%) | 0.001 | ||
| Absent | 504 (81.2) | 367 (88.9) | |
| Present | 117 (18.8) | 46 (11.1) | |
| Histologic grade, n (%), | <0.001 | ||
| 1 | 135 (20.9) | 164 (39.4) | |
| 2 | 386 (59.8) | 198 (46.1) | |
| 3 | 98 (14.1) | 48 (11.1) | |
| T stage, n (%) | <0.001 | ||
| T1mi | 23 (4.0) | 68 (16.5) | |
| 1a | 109 (17.6) | 134 (32.4) | |
| 1b | 189 (30.4) | 92 (22.3) | |
| 1c | 123 (19.8) | 34 (8.2) | |
| Stage 2 and 3 | 177 (28.5) | 85 (20.6) | |
| LN metastasis | 0.165 | ||
| N0 | 557 (86.2) | 381 (88.1) | |
| N1 | 64 (13.8) | 32 (11.9) | |
| Pathological stage, n (%) | 0.022 | ||
| IA | 440 (70.9) | 327 (79.2) | |
| IB | 141 (22.7) | 63 (15.2) | |
| IIA | 16 (2.6) | 9 (2.2) | |
| IIB | 24 (3.9) | 14 (3.4) |
| Variables | Del-19 (n = 241) | L858R (n = 306) | p-Value |
|---|---|---|---|
| Sex, n (%) | 0.076 | ||
| Female | 152 (63.2) | 215 (70.3) | |
| Male | 89 (36.8) | 91 (29.7) | |
| Age | 0.185 | ||
| ≤65 | 149 (61.6) | 172 (56.2) | |
| >65 | 92 (38.4) | 134 (43.8) | |
| Smoking, n (%) | 0.006 | ||
| Absent | 198 (82.2) | 276 (90.2) | |
| Present | 43 (17.3) | 30 (9.8) | |
| Family lung cancer history | 0.617 | ||
| Absent | 194 (80.6) | 241 (78.8) | |
| Present | 47 (19.4) | 65 (21.2) | |
| Preoperative CEA > 5 ng/mL, n (%) | 0.530 | ||
| Absent | 210 (96.0) | 272 (96.9) | |
| Present | 31 (4.0) | 34 (3.1) | |
| Histologic predominant subtype, n (%) | 0.019 | ||
| Lepidic predominant | 12 (5.0) | 32 (10.5) | |
| Non-lepidic predominant | 229 (95.0) | 274 (89.5) | |
| Pleural invasion, PI, n (%) | 0.555 | ||
| PL0 | 199 (82.6) | 249 (81.4) | |
| PL1 | 24 (10.0) | 33 (10.8) | |
| PL2 | 17 (7.0) | 19 (6.2) | |
| PL3 | 1 (0.4) | 5 (1.6) | |
| Lymphovascular invasion, n (%) | 0.011 | ||
| Absent | 185 (76.9) | 261 (85.3) | |
| Present | 56 (23.1) | 45 (14.7) | |
| Histologic grade, n (%), | 0.424 | ||
| 1 | 58 (24.1) | 66 (21.6) | |
| 2 | 141 (58.5) | 196 (64.1) | |
| 3 | 41 (17.0) | 43 (14.1) | |
| LN metastasis | 0.097 | ||
| N0 | 210 (87.1) | 280 (91.5) | |
| N1 | 31 (12.9) | 26 (8.5) | |
| Pathological stage, n (%) | 0.457 | ||
| IA | 171 (71.1) | 214 (70.0) | |
| IB | 56 (23.1) | 72 (23.5) | |
| IIA | 8 (3.3) | 6 (1.9) | |
| IIB | 6 (2.5) | 14 (4.6) |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | ||||||
| ≤65 | ref. | ref. | ||||
| >65 | 1.788 | 1.240–2.577 | 0.002 | 1.508 | 1.032–2.203 | 0.034 |
| Sex | ||||||
| Female | ref. | ref. | ||||
| Male | 0.833 | 0.571–1.216 | 0.344 | 0.942 | 0.590–1.505 | 0.804 |
| Smoking | ||||||
| Absent | ref. | ref. | ||||
| Present | 1.722 | 1.106–2.683 | 0.016 | 1.251 | 0.710–2.204 | 0.438 |
| CEA level | ||||||
| ≤5 ng/mL | ref. | ref. | ||||
| >5 ng/mL | 4.311 | 2.832–6.563 | <0.001 | 1.895 | 1.204–2.982 | 0.006 |
| Tumor size | ||||||
| ≤ 20 mm | ref. | ref. | ||||
| >20 mm | 4.828 | 3.222–7.234 | <0.001 | 2.494 | 1.574–3.953 | <0.001 |
| Histologic predominant subtype | ||||||
| Non-Lepidic | ref. | ref. | ||||
| Lepidic | 0.330 | 0.154–0.709 | 0.004 | 0.697 | 0.314–1.549 | 0.376 |
| Pleural invasion, PI, n (%) | ||||||
| Absent | ref. | ref. | ||||
| Present | 3.505 | 2.391–5.136 | <0.001 | 1.509 | 0.992–2.295 | 0.055 |
| Lymphovascular invasion | ||||||
| Absent | ref. | ref. | ||||
| Present | 4.131 | 2.838–6.014 | <0.001 | 1.742 | 1.118–2.714 | 0.014 |
| Lymph node metastasis | ||||||
| N0 | ref. | ref. | ||||
| N1 | 5.303 | 3.548–7.924 | <0.001 | 2.055 | 1.282–3.293 | 0.003 |
| EGFR mutation | ||||||
| Absent | ref. | ref. | ||||
| Present | 1.581 | 1.065–2.346 | 0.023 | 1.964 | 0.698–1.622 | 0.772 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | ||||||
| ≤65 | ref. | ref. | ||||
| >65 | 1.253 | 0.512–3.067 | 0.621 | 1.596 | 0.618–4.119 | 0.334 |
| Sex | ||||||
| Female | ref. | ref. | ||||
| Male | 1.363 | 0.557–3.336 | 0.497 | 1.392 | 0.500–3.876 | 0.527 |
| Smoking | ||||||
| Absent | ref. | ref. | ||||
| Present | 1.093 | 0.320–3.730 | 0.887 | 1.473 | 0.364–5.955 | 0.587 |
| CEA level | ||||||
| ≤5 ng/mL | ref. | ref | ||||
| >5 ng/mL | 1.515 | 0.348–6.594 | 0.580 | 1.904 | 0.408–8.884 | 0.412 |
| Tumor size | ||||||
| ≤20 mm | ref. | ref | ||||
| >20 mm | 3.359 | 1.340–8.420 | 0.010 | 1.385 | 0.441–4.350 | 0.577 |
| Histologic predominant subtype | ||||||
| Non-lepidic | ref. | ref | ||||
| Lepidic | 0.888 | 0.260–3.033 | 0.850 | 0.508 | 0.129–2.000 | 0.332 |
| Pleural invasion | ||||||
| Absent | ref. | ref | ||||
| Present | 4.162 | 1.699–10.197 | 0.002 | 1.895 | 0.654–5.493 | 0.239 |
| Lymphovascular invasion | ||||||
| Absent | ref. | ref | ||||
| Present | 7.329 | 3.034–17.703 | <0.001 | 3.744 | 1.175–11.937 | 0.026 |
| Lymph node metastasis | ||||||
| N0 | ref. | ref | ||||
| N1 | 8.895 | 3.684–21.473 | <0.001 | 3.719 | 1.145–12.076 | 0.029 |
| EGFR mutation | ||||||
| Absent | ref. | ref | ||||
| Present | 0.908 | 0.376–2.193 | 0.829 | 0.680 | 0.262–1.770 | 0.430 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, C.-W.; Lin, M.-W.; Chiang, X.-H.; Hsu, H.-H.; Hsieh, M.-S.; Chen, J.-S. Clinicopathological Features and Significance of Epidermal Growth Factor Receptor Mutation in Surgically Resected Early-Stage Lung Adenocarcinoma. Diagnostics 2023, 13, 390. https://doi.org/10.3390/diagnostics13030390
Lu C-W, Lin M-W, Chiang X-H, Hsu H-H, Hsieh M-S, Chen J-S. Clinicopathological Features and Significance of Epidermal Growth Factor Receptor Mutation in Surgically Resected Early-Stage Lung Adenocarcinoma. Diagnostics. 2023; 13(3):390. https://doi.org/10.3390/diagnostics13030390
Chicago/Turabian StyleLu, Chao-Wen, Mong-Wei Lin, Xu-Heng Chiang, Hsao-Hsun Hsu, Min-Shu Hsieh, and Jin-Shing Chen. 2023. "Clinicopathological Features and Significance of Epidermal Growth Factor Receptor Mutation in Surgically Resected Early-Stage Lung Adenocarcinoma" Diagnostics 13, no. 3: 390. https://doi.org/10.3390/diagnostics13030390
APA StyleLu, C.-W., Lin, M.-W., Chiang, X.-H., Hsu, H.-H., Hsieh, M.-S., & Chen, J.-S. (2023). Clinicopathological Features and Significance of Epidermal Growth Factor Receptor Mutation in Surgically Resected Early-Stage Lung Adenocarcinoma. Diagnostics, 13(3), 390. https://doi.org/10.3390/diagnostics13030390