
Inferior Vena Caval Measures Do Not Correlate with Carotid Artery Corrected Flow Time Change Measured Using a Wireless Doppler Patch in Healthy Volunteers

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Setting
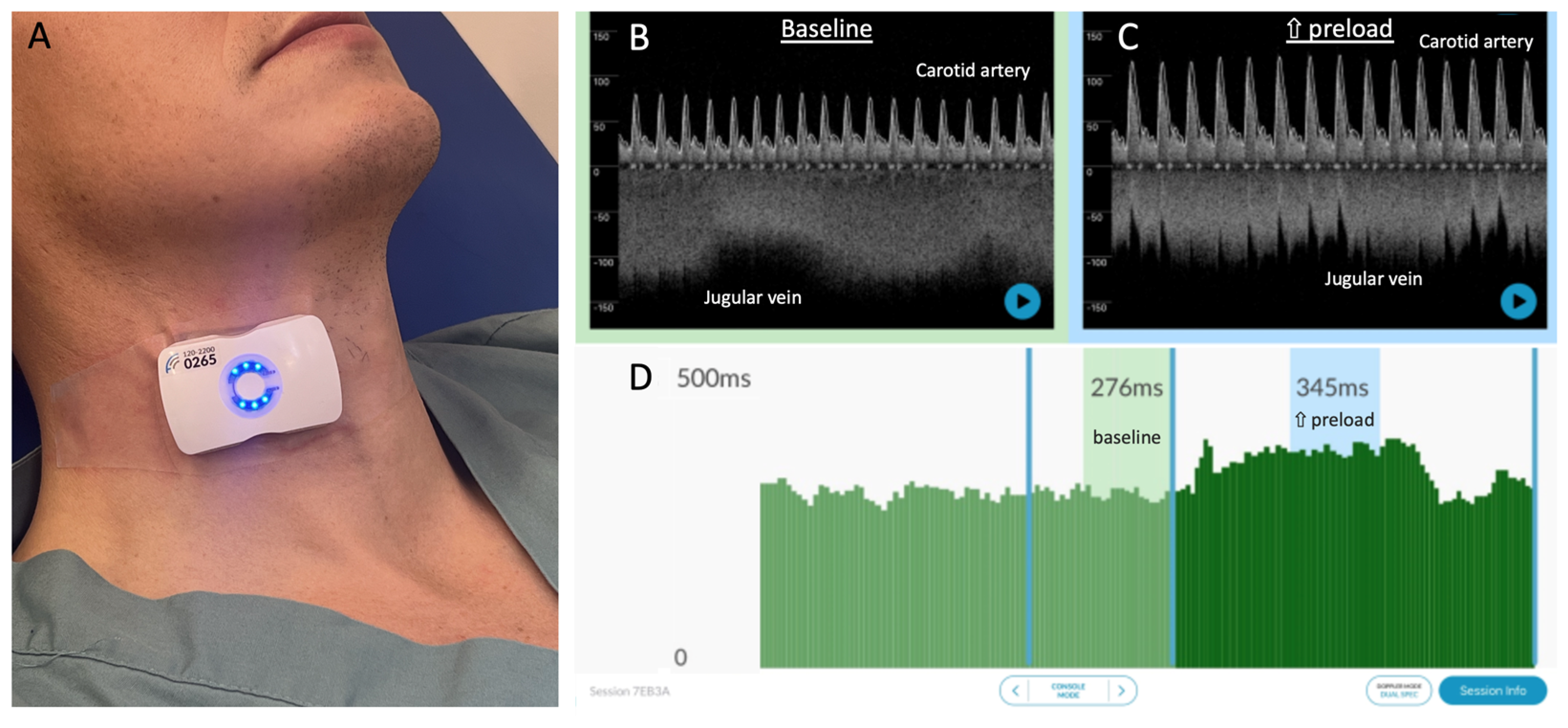
2.2. Carotid Artery Doppler Measures
2.3. Venous Measures
2.4. Tilt-Table Protocol
2.5. Analysis
3. Results
3.1. Patients
3.2. Supine Venous Measures
3.3. Head-Up Baseline ccFT∆
3.4. Supine Baseline ccFT∆
3.5. Relationship between Supine Venous Measures and ccFT∆
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bentzer, P.; Griesdale, D.E.; Boyd, J.; MacLean, K.; Sirounis, D.; Ayas, N.T. Will this hemodynamically unstable patient respond to a bolus of intravenous fluids? JAMA 2016, 316, 1298–1309. [Google Scholar] [CrossRef] [PubMed]
- Michard, F.; Teboul, J.-L. Predicting fluid responsiveness in ICU patients: A critical analysis of the evidence. Chest 2002, 121, 2000–2008. [Google Scholar] [CrossRef] [PubMed]
- Michard, F.; Boussat, S.; Chemla, D.; Anguel, N.; Mercat, A.; Lecarpentier, Y.; Richard, C.; Pinsky, M.R.; Teboul, J.-l. Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am. J. Respir. Crit. Care Med. 2000, 162, 134–138. [Google Scholar] [CrossRef]
- Marik, P.; Bellomo, R. A rational approach to fluid therapy in sepsis. BJA Br. J. Anaesth. 2015, 116, 339–349. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E. Fluid responsiveness and the six guiding principles of fluid resuscitation. Crit. Care Med. 2016, 44, 1920–1922. [Google Scholar] [CrossRef]
- García, M.I.M.; González, P.G.; Romero, M.G.; Cano, A.G.; Oscier, C.; Rhodes, A.; Grounds, R.M.; Cecconi, M. Effects of fluid administration on arterial load in septic shock patients. Intensive Care Med. 2015, 41, 1247–1255. [Google Scholar] [CrossRef]
- Magder, S.; Bafaqeeh, F. The clinical role of central venous pressure measurements. J. Intensive Care Med. 2007, 22, 44–51. [Google Scholar] [CrossRef]
- Ehrman, R.R.; Gallien, J.Z.; Smith, R.K.; Akers, K.G.; Malik, A.N.; Harrison, N.E.; Welch, R.D.; Levy, P.D.; Sherwin, R.L. Resuscitation Guided by Volume Responsiveness Does Not Reduce Mortality in Sepsis: A Meta-Analysis. Crit. Care Explor. 2019, 1, e0015. [Google Scholar] [CrossRef]
- Dubin, A.; Loudet, C.; Kanoore Edul, V.S.; Osatnik, J.; Ríos, F.; Vásquez, D.; Pozo, M.; Lattanzio, B.; Pálizas, F.; Klein, F.; et al. Characteristics of resuscitation, and association between use of dynamic tests of fluid responsiveness and outcomes in septic patients: Results of a multicenter prospective cohort study in Argentina. Ann. Intensive Care 2020, 10, 40. [Google Scholar] [CrossRef]
- Douglas, I.S.; Alapat, P.M.; Corl, K.A.; Exline, M.C.; Forni, L.G.; Holder, A.L.; Kaufman, D.A.; Khan, A.; Levy, M.M.; Martin, G.S. Fluid response evaluation in sepsis hypotension and shock: A randomized clinical trial. Chest 2020, 158, 1431–1445. [Google Scholar] [CrossRef]
- Satterwhite, L.; Latham, H. Fluid Management in Sepsis Hypotension and Septic Shock: Time to Transition the Conversation From Fluid Responsive to Fluid Refractory? Chest 2020, 158, 1319–1320. [Google Scholar] [CrossRef] [PubMed]
- Wiedemann, H.; Wheeler, A.; Bernard, G.; Thompson, B. Comparison of Two Fluid-Management Strategies in Acute Lung Injury. N. Engl. J. Med. 2006, 354, 2564–2575. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.D.; Thompson, B.T.; Ancukiewicz, M.; Steingrub, J.S.; Douglas, I.S.; Matthay, M.A.; Wright, P.; Peterson, M.W.; Rock, P.; Hyzy, R.C. Acute kidney injury in patients with acute lung injury: Impact of fluid accumulation on classification of acute kidney injury and associated outcomes. Crit. Care Med. 2011, 39, 2665. [Google Scholar] [CrossRef] [PubMed]
- Orso, D.; Paoli, I.; Piani, T.; Cilenti, F.L.; Cristiani, L.; Guglielmo, N. Accuracy of Ultrasonographic Measurements of Inferior Vena Cava to Determine Fluid Responsiveness: A Systematic Review and Meta-Analysis. J. Intensive Care Med. 2020, 35, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Beier, L.; Davis, J.; Esener, D.; Grant, C.; Fields, J.M. Carotid Ultrasound to Predict Fluid Responsiveness: A Systematic Review. J. Ultrasound Med. 2020, 39, 1965–1976. [Google Scholar] [CrossRef] [PubMed]
- Singla, D.; Gupta, B.; Varshney, P.; Mangla, M.; Walikar, B.N.; Jamir, T. Role of carotid corrected flow time and peak velocity variation in predicting fluid responsiveness: A systematic review and meta-analysis. Korean J. Anesthesiol. 2023, 76, 183–193. [Google Scholar] [CrossRef]
- Kircher, B.J.; Himelman, R.B.; Schiller, N.B. Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am. J. Cardiol. 1990, 66, 493–496. [Google Scholar] [CrossRef]
- Bodson, L.; Vieillard-Baron, A. Respiratory variation in inferior vena cava diameter: Surrogate of central venous pressure or parameter of fluid responsiveness? Let the physiology reply. Crit. Care 2012, 16, 181. [Google Scholar] [CrossRef]
- Amsallem, M.; Sternbach, J.M.; Adigopula, S.; Kobayashi, Y.; Vu, T.A.; Zamanian, R.; Liang, D.; Dhillon, G.; Schnittger, I.; McConnell, M.V.; et al. Addressing the Controversy of Estimating Pulmonary Arterial Pressure by Echocardiography. J. Am. Soc. Echocardiogr. 2016, 29, 93–102. [Google Scholar] [CrossRef]
- Eskesen, T.; Wetterslev, M.; Perner, A. Systematic review including re-analyses of 1148 individual data sets of central venous pressure as a predictor of fluid responsiveness. Intensive Care Med. 2016, 42, 324–332. [Google Scholar] [CrossRef]
- Barjaktarevic, I.; Toppen, W.E.; Hu, S.; Montoya, E.A.; Ong, S.; Buhr, R.; David, I.J.; Wang, T.; Rezayat, T.; Chang, S.Y. Ultrasound Assessment of the Change in Carotid Corrected Flow Time in Fluid Responsiveness in Undifferentiated Shock. Crit. Care Med. 2018, 11, 1040–1046. [Google Scholar] [CrossRef]
- Jung, S.; Kim, J.; Na, S.; Nam, W.S.; Kim, D.-H. Ability of Carotid Corrected Flow Time to Predict Fluid Responsiveness in Patients Mechanically Ventilated Using Low Tidal Volume after Surgery. J. Clin. Med. 2021, 10, 2676. [Google Scholar] [CrossRef] [PubMed]
- Kenny, J.-É.S.; Barjaktarevic, I.; Mackenzie, D.C.; Eibl, A.M.; Parrotta, M.; Long, B.F.; Eibl, J.K. Diagnostic characteristics of 11 formulae for calculating corrected flow time as measured by a wearable Doppler patch. Intensive Care Med. Exp. 2020, 8, 54. [Google Scholar] [CrossRef] [PubMed]
- Kenny, J.-É.S.; Barjaktarevic, I.; Mackenzie, D.C.; Elfarnawany, M.; Yang, Z.; Eibl, A.M.; Eibl, J.K.; Kim, C.-H.; Johnson, B.D. Carotid Doppler ultrasonography correlates with stroke volume in a human model of hypovolaemia and resuscitation: Analysis of 48 570 cardiac cycles. Br. J. Anaesth. 2021, 127, e60–e63. [Google Scholar] [CrossRef] [PubMed]
- Kerrebijn, I.; Atwi, S.; Horner, C.; Elfarnawany, M.; Eibl, A.M.; Eibl, J.K.; Taylor, J.L.; Kim, C.H.; Johnson, B.D.; Kenny, J.S. Correlation between changing carotid artery corrected flow time and ascending aortic Doppler flow velocity. Br. J. Anaesth. 2023, 131, e192–e195. [Google Scholar] [CrossRef]
- Kenny, J.S.; Barjaktarevic, I.; Eibl, A.M.; Parrotta, M.; Long, B.F.; Elfarnawany, M.; Eibl, J.K. Temporal concordance between pulse contour analysis, bioreactance and carotid doppler during rapid preload changes. PLoS ONE 2022, 17, e0265711. [Google Scholar] [CrossRef] [PubMed]
- Kenny, J.S.; Clarke, G.; Kerrebijn, I.; Savery, T.; Knott, M.; Munding, C.E.; Elfarnawany, M.; Eibl, A.E.; Eibl, J.K.; Nalla, B.; et al. Carotid Artery Corrected Flow Time Detects Stroke Volume Change Measured by Trans-Esophageal Echocardiography. Intensive Care Med. Exp. 2023, 11, 195. [Google Scholar]
- Beaubien-Souligny, W.; Rola, P.; Haycock, K.; Bouchard, J.; Lamarche, Y.; Spiegel, R.; Denault, A.Y. Quantifying systemic congestion with Point-Of-Care ultrasound: Development of the venous excess ultrasound grading system. Ultrasound J. 2020, 12, 16. [Google Scholar] [CrossRef]
- Argaiz, E.R. VExUS Nexus: Bedside Assessment of Venous Congestion. Adv. Chronic. Kidney Dis. 2021, 28, 252–261. [Google Scholar] [CrossRef]
- Spiegel, R.; Teeter, W.; Sullivan, S.; Tupchong, K.; Mohammed, N.; Sutherland, M.; Leibner, E.; Rola, P.; Galvagno, S.M.; Murthi, S.B. The use of venous Doppler to predict adverse kidney events in a general ICU cohort. Crit. Care 2020, 24, 615. [Google Scholar] [CrossRef]
- Longino, A.; Martin, K.; Leyba, K.; Siegel, G.; Gill, E.; Douglas, I.S.; Burke, J. Correlation between the VExUS score and right atrial pressure: A pilot prospective observational study. Crit. Care 2023, 27, 205. [Google Scholar] [CrossRef]
- Søndergaard, S. Observational study on passive leg raising and the autonomic nervous system. Physiol. Rep. 2022, 10, e15537. [Google Scholar] [CrossRef] [PubMed]
- Corl, K.A.; George, N.R.; Romanoff, J.; Levinson, A.T.; Chheng, D.B.; Merchant, R.C.; Levy, M.M.; Napoli, A.M. Inferior vena cava collapsibility detects fluid responsiveness among spontaneously breathing critically-ill patients. J. Crit. Care 2017, 41, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.; Iida, N.; Yamamoto, M.; Machino-Ohtsuka, T.; Ishizu, T.; Aonuma, K. Estimation of Central Venous Pressure Using the Ratio of Short to Long Diameter from Cross-Sectional Images of the Inferior Vena Cava. J. Am. Soc. Echocardiogr. 2017, 30, 461–467. [Google Scholar] [CrossRef]
- Kenny, J.-E.S.; Prager, R.; Rola, P.; McCulloch, G.; Eibl, J.K.; Haycock, K. The effect of gravity-induced preload change on the venous excess ultrasound (VExUS) score and internal jugular vein Doppler in healthy volunteers. Intensive Care Med. Exp. 2023, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.-G.; Xu, L.-Y.; Luo, J.-C.; Hou, J.-Y.; Hao, G.-W.; Su, Y.; Liu, K.; Yu, S.-J.; Tu, G.-W.; Luo, Z. Change in left ventricular velocity time integral during Trendelenburg maneuver predicts fluid responsiveness in cardiac surgical patients in the operating room. Quant. Imaging Med. Surg. 2021, 11, 3133. [Google Scholar] [CrossRef] [PubMed]
- Terai, C.; Anada, H.; Matsushima, S.; Shimizu, S.; Okada, Y. Effects of mild Trendelenburg on central hemodynamics and internal jugular vein velocity, cross-sectional area, and flow. Am. J. Emerg. Med. 1995, 13, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Jabot, J.; Teboul, J.L.; Richard, C.; Monnet, X. Passive leg raising for predicting fluid responsiveness: Importance of the postural change. Intensive Care Med. 2009, 35, 85–90. [Google Scholar] [CrossRef]
- Godfrey, G.E.; Dubrey, S.W.; Handy, J.M. A prospective observational study of stroke volume responsiveness to a passive leg raise manoeuvre in healthy non-starved volunteers as assessed by transthoracic echocardiography. Anaesthesia 2014, 69, 306–313. [Google Scholar] [CrossRef]
- Monnet, X.; Teboul, J.-L. Passive leg raising. Intensive Care Med. 2008, 34, 659–663. [Google Scholar] [CrossRef]
- Hernández, G.; Ospina-Tascón, G.A.; Damiani, L.P.; Estenssoro, E.; Dubin, A.; Hurtado, J.; Friedman, G.; Castro, R.; Alegría, L.; Teboul, J.-L. Effect of a resuscitation strategy targeting peripheral perfusion status vs serum lactate levels on 28-day mortality among patients with septic shock: The ANDROMEDA-SHOCK randomized clinical trial. JAMA 2019, 321, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Kattan, E.; Ospina-Tascón, G.A.; Teboul, J.-L.; Castro, R.; Cecconi, M.; Ferri, G.; Bakker, J.; Hernández, G.; Investigators, A.-S. Systematic assessment of fluid responsiveness during early septic shock resuscitation: Secondary analysis of the ANDROMEDA-SHOCK trial. Crit. Care 2020, 24, 23. [Google Scholar] [CrossRef] [PubMed]
- Millington, S.J. Ultrasound assessment of the inferior vena cava for fluid responsiveness: Easy, fun, but unlikely to be helpful. Can. J. Anesth./J. Can. D’anesthésie 2019, 66, 633–638. [Google Scholar] [CrossRef]
- Millington, S.J.; Koenig, S. Ultrasound Assessment of the Inferior Vena Cava for Fluid Responsiveness: Making the Case for Skepticism. J. Intensive Care Med. 2021, 36, 1223–1227. [Google Scholar] [CrossRef] [PubMed]
- Via, G.; Tavazzi, G.; Price, S. Ten situations where inferior vena cava ultrasound may fail to accurately predict fluid responsiveness: A physiologically based point of view. Intensive Care Med. 2016, 42, 1164–1167. [Google Scholar] [CrossRef] [PubMed]
- Juhl-Olsen, P.; Frederiksen, C.A.; Hermansen, J.F.; Jakobsen, C.J.; Sloth, E. Echocardiographic Measures of Diastolic Function Are Preload Dependent during Triggered Positive Pressure Ventilation: A Controlled Crossover Study in Healthy Subjects. Crit. Care Res. Pract. 2012, 2012, 703196. [Google Scholar] [CrossRef]
- Juhl-Olsen, P.; Vistisen, S.T.; Christiansen, L.K.; Rasmussen, L.A.; Frederiksen, C.A.; Sloth, E. Ultrasound of the inferior vena cava does not predict hemodynamic response to early hemorrhage. J. Emerg. Med. 2013, 45, 592–597. [Google Scholar] [CrossRef]
- Juhl-Olsen, P.; Frederiksen, C.A.; Sloth, E. Ultrasound assessment of inferior vena cava collapsibility is not a valid measure of preload changes during triggered positive pressure ventilation: A controlled cross-over study. Ultraschall. Med. 2012, 33, 152–159. [Google Scholar] [CrossRef]
- Koratala, A. Isolated Inferior Vena Cava Ultrasound in Hyponatremia: The Power and Peril of Point-of-Care Imaging. J. Ultrasound Med. 2023, 42, 2683–2684. [Google Scholar] [CrossRef]
- Rola, P.; Haycock, K.; Spiegel, R. What every intensivist should know about the IVC. J. Crit. Care 2023, 154455. [Google Scholar] [CrossRef]
- Di Nicolò, P.; Tavazzi, G.; Nannoni, L.; Corradi, F. Inferior Vena Cava Ultrasonography for Volume Status Evaluation: An Intriguing Promise Never Fulfilled. J. Clin. Med. 2023, 12, 2217. [Google Scholar] [CrossRef] [PubMed]
- Kory, P. COUNTERPOINT: Should Acute Fluid Resuscitation Be Guided Primarily by Inferior Vena Cava Ultrasound for Patients in Shock? No. Chest 2017, 151, 533–536. [Google Scholar] [CrossRef]
- Berlin, D.A.; Bakker, J. Starling curves and central venous pressure. Crit. Care 2015, 19, 55. [Google Scholar] [CrossRef]
- Kenny, J.-E.S. Assessing Fluid Intolerance with Doppler Ultrasonography: A Physiological Framework. Med. Sci. 2022, 10, 12. [Google Scholar] [CrossRef]
- Kenny, J.-E.; Prager, R.; Rola, P.; Haycock, K.; Basmaji, J.; Hernández, G. Unifying Fluid Responsiveness and Tolerance with Physiology: A dynamic interpretation of the Diamond-Forrester classification. Crit. Care Explor. 2023, in press. [Google Scholar]
- Monnet, X.; Shi, R.; Teboul, J.-L. Prediction of fluid responsiveness. What’s new? Ann. Intensive Care 2022, 12, 46. [Google Scholar] [CrossRef]
- Abbasi, A.; Azab, N.; Nayeemuddin, M.; Schick, A.; Lopardo, T.; Phillips, G.S.; Merchant, R.C.; Levy, M.M.; Blaivas, M.; Corl, K.A. Change in Carotid Blood Flow and Carotid Corrected Flow Time Assessed by Novice Sonologists Fails to Determine Fluid Responsiveness in Spontaneously Breathing Intensive Care Unit Patients. Ultrasound Med. Biol. 2020, 46, 2659–2666. [Google Scholar] [CrossRef]
- Bussmann, B.M.; Sharma, S.; Mcgregor, D.; Hulme, W.; Harris, T. Observational study in healthy volunteers to define interobserver reliability of ultrasound haemodynamic monitoring techniques performed by trainee doctors. Eur. J. Emerg. Med. 2019, 26, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Preau, S.; Bortolotti, P.; Colling, D.; Dewavrin, F.; Colas, V.; Voisin, B.; Onimus, T.; Drumez, E.; Durocher, A.; Redheuil, A.; et al. Diagnostic Accuracy of the Inferior Vena Cava Collapsibility to Predict Fluid Responsiveness in Spontaneously Breathing Patients With Sepsis and Acute Circulatory Failure. Crit. Care Med. 2017, 45, e290–e297. [Google Scholar] [CrossRef] [PubMed]
- Corl, K.A.; Azab, N.; Nayeemuddin, M.; Schick, A.; Lopardo, T.; Zeba, F.; Phillips, G.; Baird, G.; Merchant, R.C.; Levy, M.M.; et al. Performance of a 25% Inferior Vena Cava Collapsibility in Detecting Fluid Responsiveness When Assessed by Novice Versus Expert Physician Sonologists. J. Intensive Care Med. 2020, 35, 1520–1528. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| n = 14 | Mean | Std |
|---|---|---|
| Patient Age | 29.6 | ±9.3 |
| Patient Height (m) | 1.7 | ±0.1 |
| Patient Weight (kg) | 69.1 | ±16.0 |
| BMI (kg/m2) | 23.1 | ±4.2 |
| MAP (mmHg) | 96.3 | ±10.6 |
| HR (bpm) | 73.5 | ±10.6 |
| Systolic Blood Pressure (mmHg) | 127.7 | ±16.3 |
| Corrected Carotid Flow Time∆ | Supine Venous Measures | ||||
|---|---|---|---|---|---|
| IVCEE | IVC% | SIIVC | PIPORTAL | ||
| Head-up baseline | ccFT absolute∆ | R2 = 0.041 | R2 = 0.25 | R2 = 0.0006 | R2 = 0.11 |
| ccFT %∆ | R2 = 0.029 | R2 = 0.29 | R2 = 0.0009 | R2 = 0.097 | |
| Supine baseline | ccFT absolute∆ | R2 = 0.0001 | R2 = 0.16 | R2 = 0.011 | R2 = 0.075 |
| ccFT %∆ | R2 = 0.000008 | R2 = 0.16 | R2 = 0.0095 | R2 = 0.077 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kenny, J.-E.S.; Prager, R.; Rola, P.; McCulloch, G.; Atwi, S.; Munding, C.E.; Eibl, J.K.; Haycock, K. Inferior Vena Caval Measures Do Not Correlate with Carotid Artery Corrected Flow Time Change Measured Using a Wireless Doppler Patch in Healthy Volunteers. Diagnostics 2023, 13, 3591. https://doi.org/10.3390/diagnostics13233591
Kenny J-ES, Prager R, Rola P, McCulloch G, Atwi S, Munding CE, Eibl JK, Haycock K. Inferior Vena Caval Measures Do Not Correlate with Carotid Artery Corrected Flow Time Change Measured Using a Wireless Doppler Patch in Healthy Volunteers. Diagnostics. 2023; 13(23):3591. https://doi.org/10.3390/diagnostics13233591
Chicago/Turabian StyleKenny, Jon-Emile S., Ross Prager, Philippe Rola, Garett McCulloch, Sarah Atwi, Chelsea E. Munding, Joseph K. Eibl, and Korbin Haycock. 2023. "Inferior Vena Caval Measures Do Not Correlate with Carotid Artery Corrected Flow Time Change Measured Using a Wireless Doppler Patch in Healthy Volunteers" Diagnostics 13, no. 23: 3591. https://doi.org/10.3390/diagnostics13233591
APA StyleKenny, J.-E. S., Prager, R., Rola, P., McCulloch, G., Atwi, S., Munding, C. E., Eibl, J. K., & Haycock, K. (2023). Inferior Vena Caval Measures Do Not Correlate with Carotid Artery Corrected Flow Time Change Measured Using a Wireless Doppler Patch in Healthy Volunteers. Diagnostics, 13(23), 3591. https://doi.org/10.3390/diagnostics13233591