
Tumor Heterogeneity of Breast Cancer Assessed with Computed Tomography Texture Analysis: Association with Disease-Free Survival and Clinicopathological Prognostic Factor

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
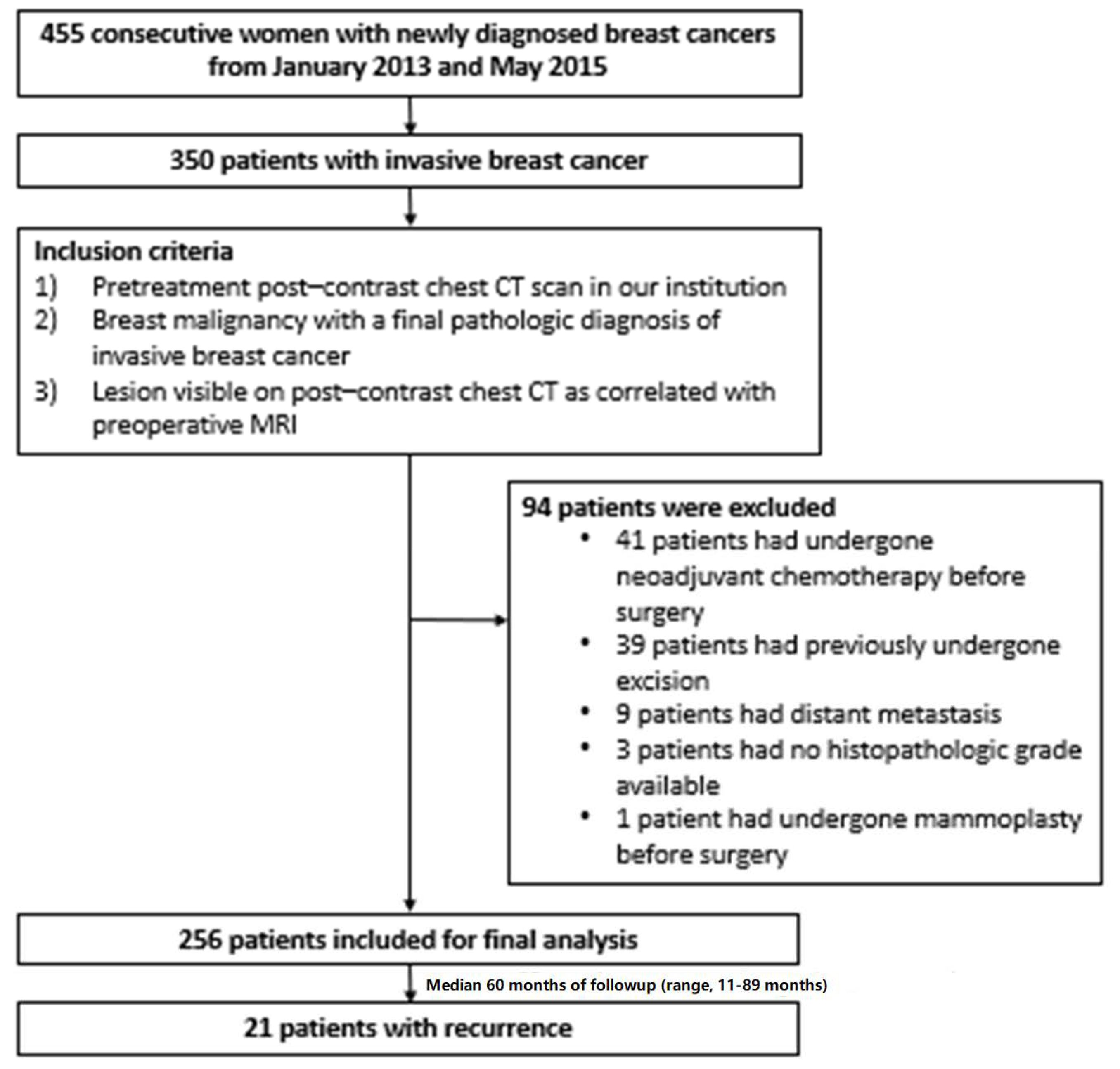
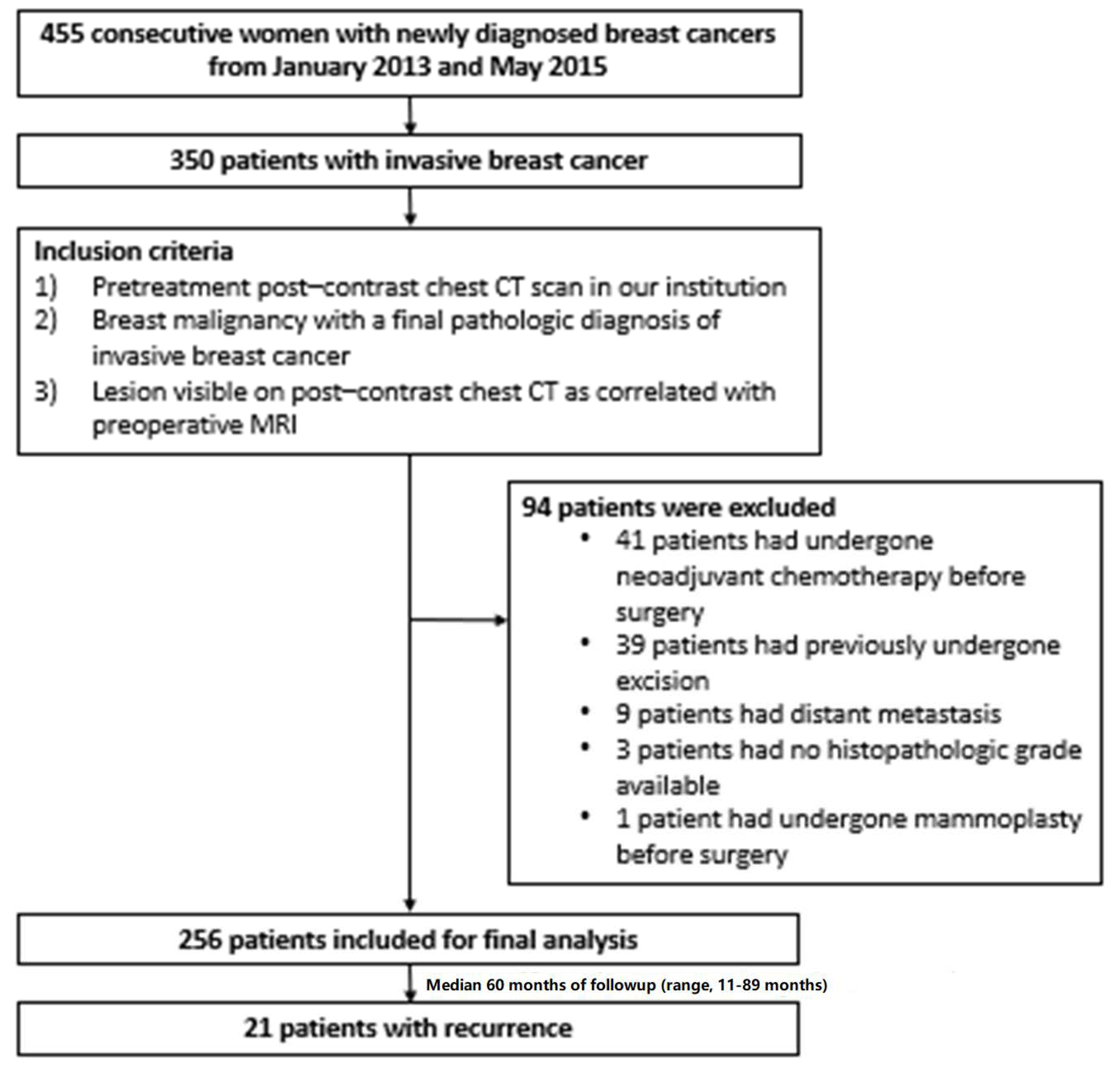
2.1. Patients
2.2. CT Acquisition
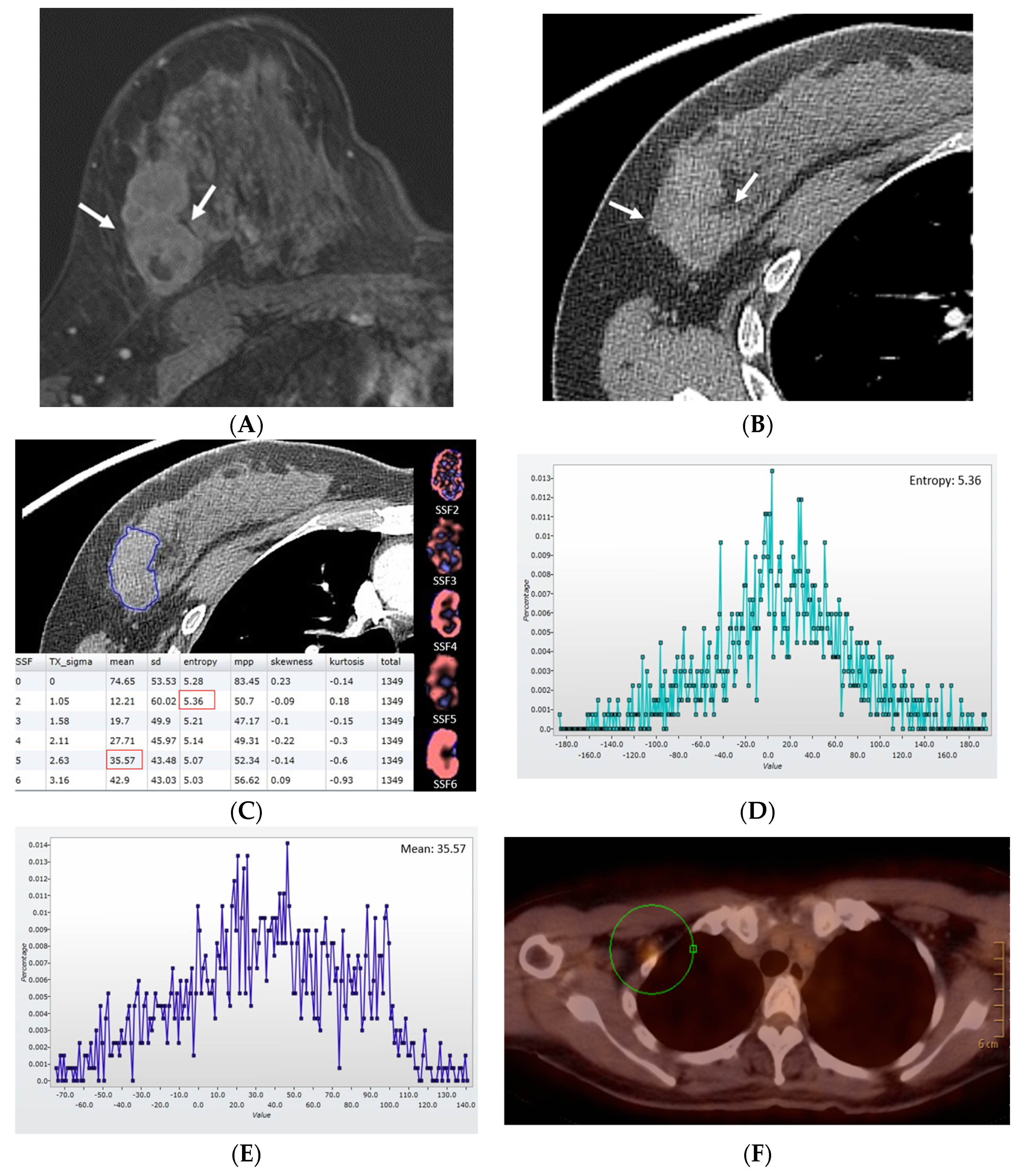
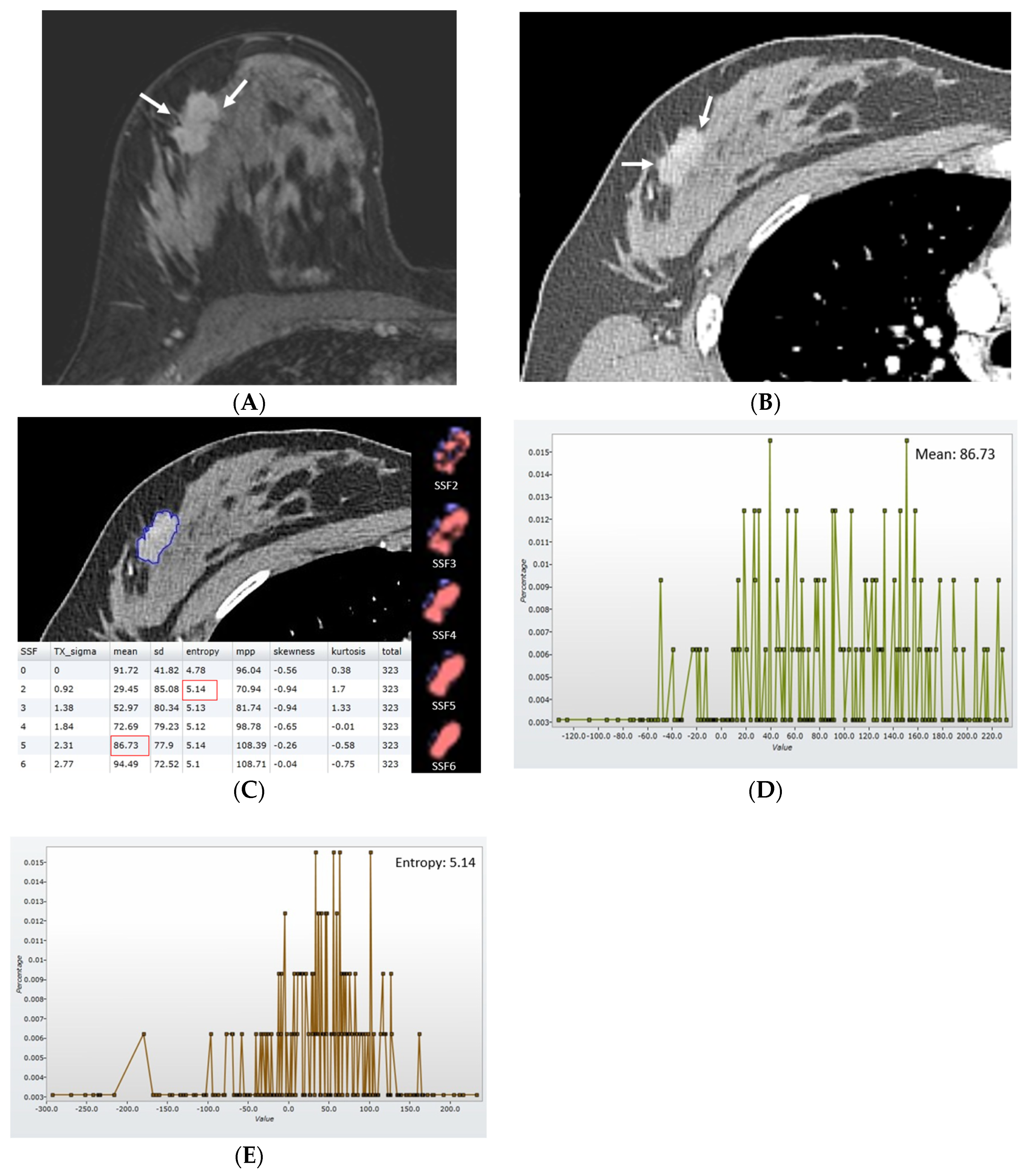
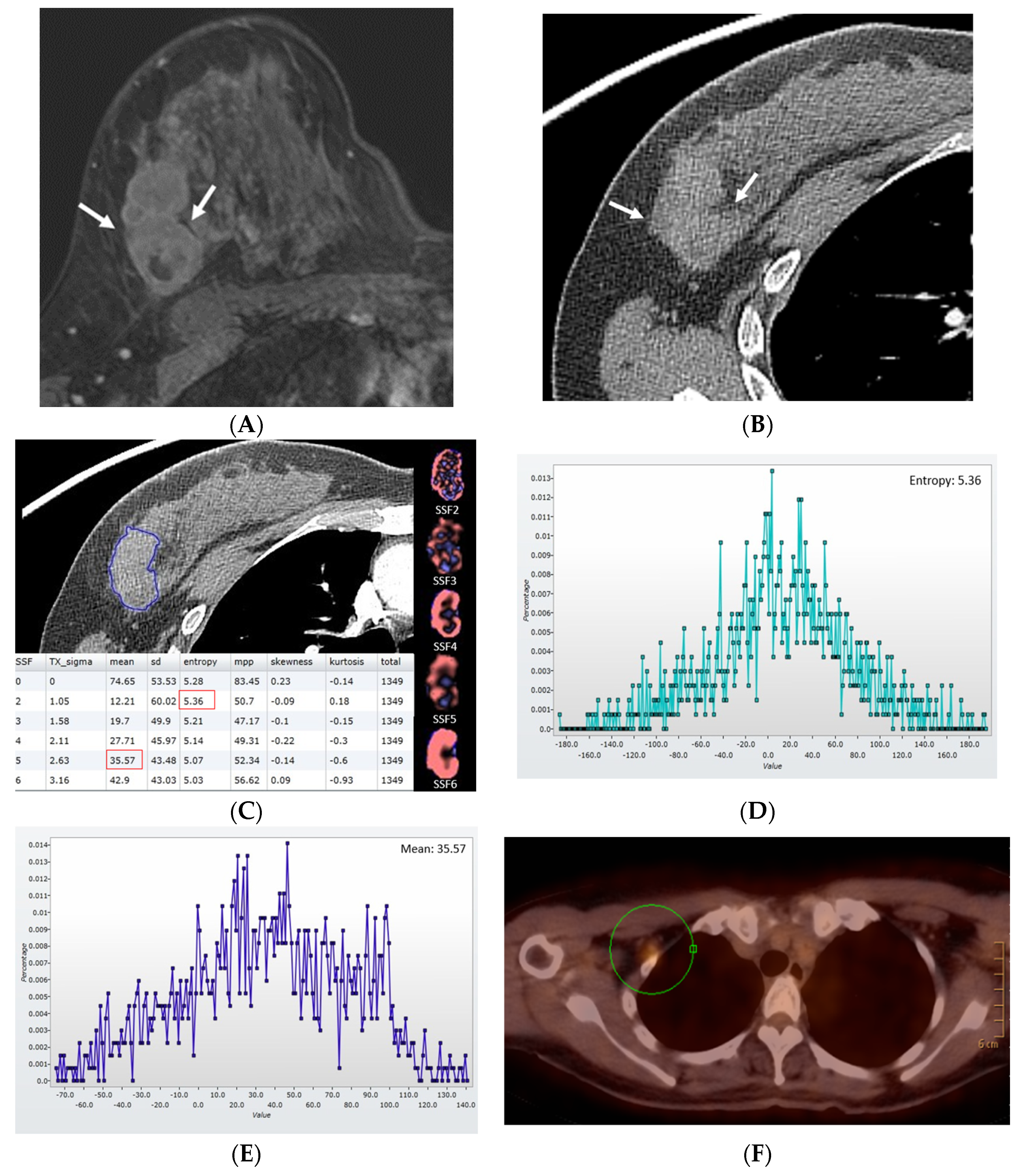
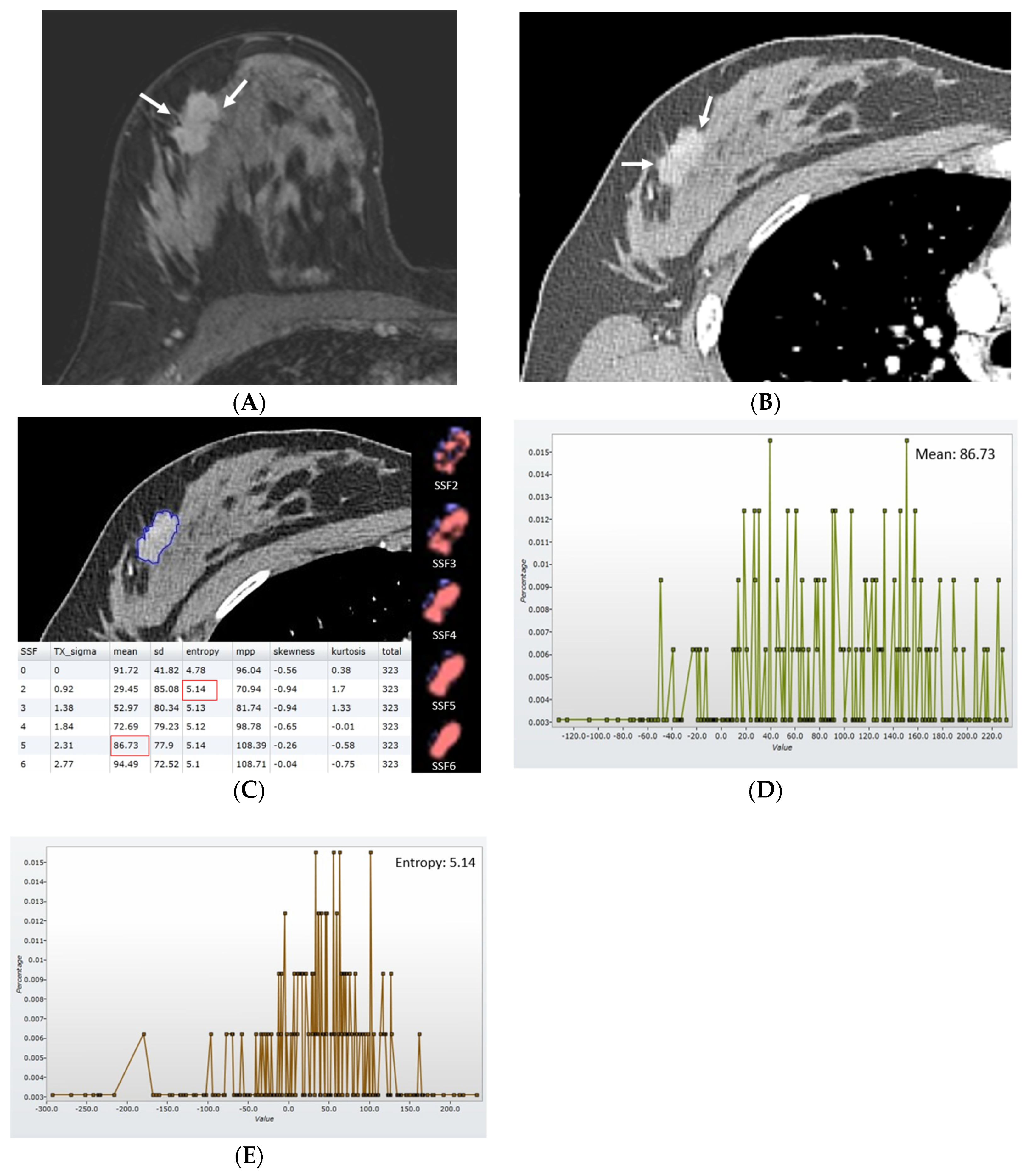
2.3. Texture Analysis
2.4. Clinicopathological Data
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Disease-Free Survival
3.2. CT Texture Features
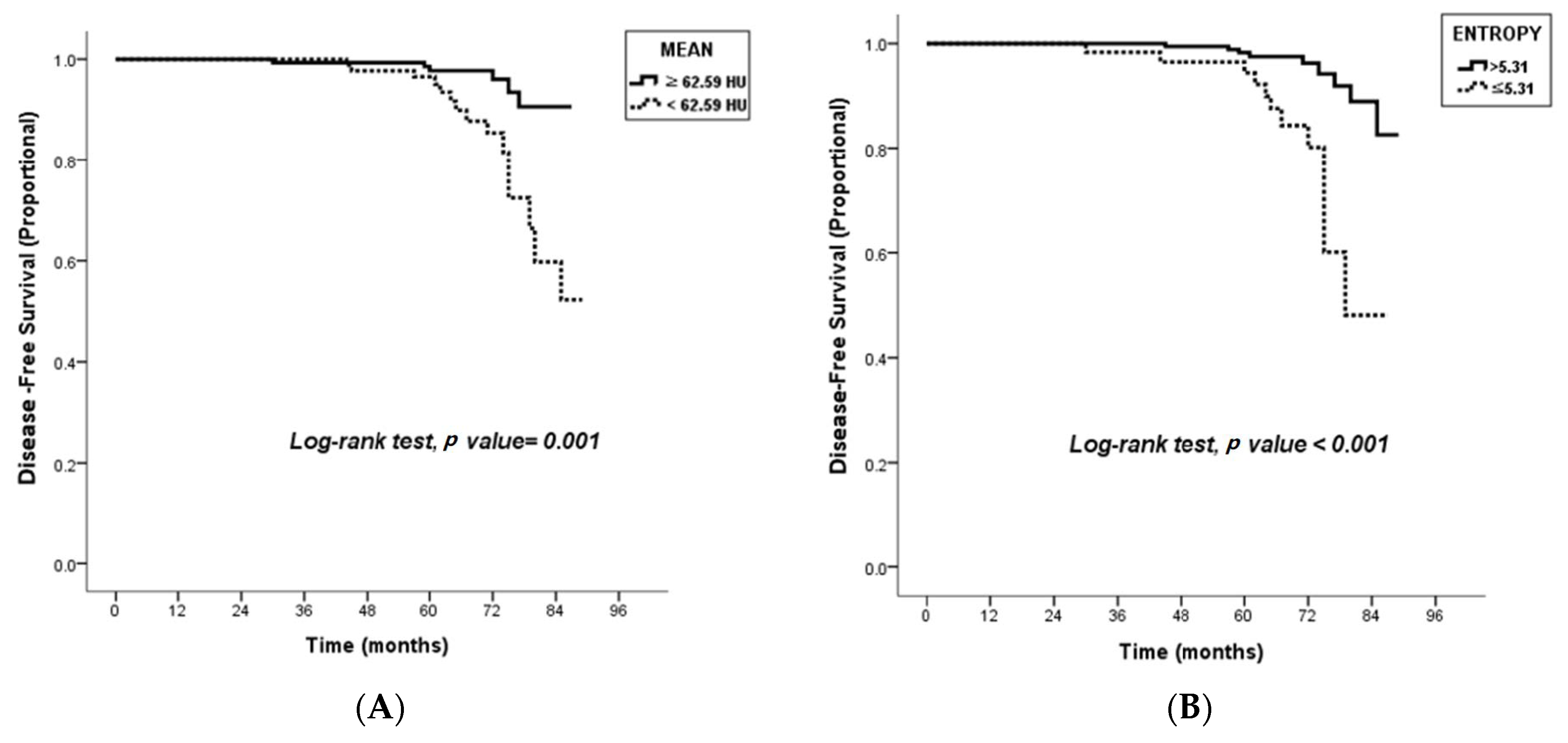
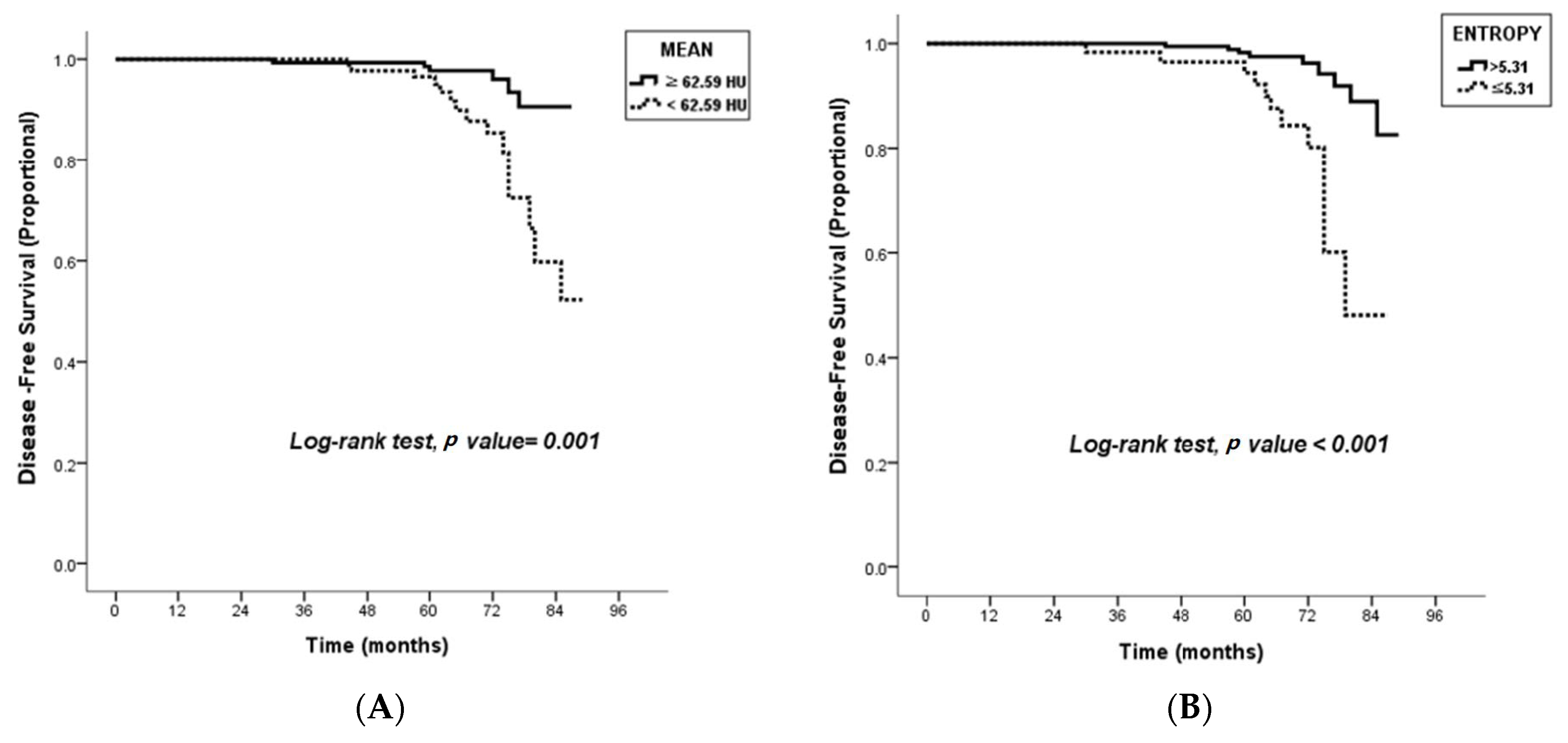
3.3. Survival Analysis Using Cox Proportional Hazard Models
3.4. Association with Textural Features and Clinicopathological Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Martelotto, L.G.; Ng, C.K.; Piscuoglio, S.; Weigelt, B.; Reis-Filho, J.S. Breast cancer intra-tumor heterogeneity. Breast Cancer Res. 2014, 16, 210. [Google Scholar] [CrossRef] [PubMed]
- Bedard, P.L.; Hansen, A.R.; Ratain, M.J.; Siu, L.L. Tumour heterogeneity in the clinic. Nature 2013, 501, 355–364. [Google Scholar] [CrossRef]
- Marusyk, A.; Almendro, V.; Polyak, K. Intra-tumour heterogeneity: A looking glass for cancer? Nat. Rev. Cancer 2012, 12, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.K.; Pemberton, H.N.; Reis-Filho, J.S. Breast cancer intratumor genetic heterogeneity: Causes and implications. Expert. Rev. Anticancer Ther. 2012, 12, 1021–1032. [Google Scholar] [CrossRef] [PubMed]
- Swanton, C. Intratumor heterogeneity: Evolution through space and time. Cancer Res. 2012, 72, 4875–4882. [Google Scholar] [CrossRef] [PubMed]
- Saha, A.; Harowicz, M.R.; Cain, E.H.; Hall, A.H.; Hwang, E.-S.S.; Marks, J.R.; Marcom, P.K.; Mazurowski, M.A. Intra-tumor molecular heterogeneity in breast cancer: Definitions of measures and association with distant recurrence-free survival. Breast Cancer Res. Treat. 2018, 172, 123–132. [Google Scholar] [CrossRef]
- Davnall, F.; Yip, C.S.; Ljungqvist, G.; Selmi, M.; Ng, F.; Sanghera, B.; Ganeshan, B.; Miles, K.A.; Cook, G.J.; Goh, V. Assessment of tumor heterogeneity: An emerging imaging tool for clinical practice? Insights Imaging 2012, 3, 573–589. [Google Scholar] [CrossRef]
- Nelson, D.A.; Tan, T.-T.; Rabson, A.B.; Anderson, D.; Degenhardt, K.; White, E. Hypoxia and defective apoptosis drive genomic instability and tumorigenesis. Genes Dev. 2004, 18, 2095–2107. [Google Scholar] [CrossRef]
- Beca, F.; Polyak, K. Intratumor Heterogeneity in Breast Cancer. Adv. Exp. Med. Biol. 2016, 882, 169–189. [Google Scholar]
- McDonald, K.-A.; Kawaguchi, T.; Qi, Q.; Peng, X.; Asaoka, M.; Young, J.; Opyrchal, M.; Yan, L.; Patnaik, S.; Otsuji, E.; et al. Tumor Heterogeneity Correlates with Less Immune Response and Worse Survival in Breast Cancer Patients. Ann. Surg. Oncol. 2019, 26, 2191–2199. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, J.J.; Hwangbo, L.; Suh, H.B.; Kim, S.; Choo, K.S.; Nam, K.J.; Kang, T. Kinetic Heterogeneity of Breast Cancer Determined Using Computer-aided Diagnosis of Preoperative MRI Scans: Relationship to Distant Metastasis-Free Survival. Radiology 2020, 295, 517–526. [Google Scholar] [CrossRef]
- Holli-Helenius, K.; Salminen, A.; Rinta-Kiikka, I.; Koskivuo, I.; Brück, N.; Boström, P.; Parkkola, R. MRI texture analysis in differentiating luminal A and luminal B breast cancer molecular subtypes—A feasibility study. BMC Med. Imaging 2017, 17, 69. [Google Scholar] [CrossRef]
- Lubner, M.G.; Smith, A.D.; Sandrasegaran, K.; Sahani, D.V.; Pickhardt, P.J. CT Texture Analysis: Definitions, Applications, Biologic Correlates, and Challenges. Radiographics 2017, 37, 1483–1503. [Google Scholar] [CrossRef]
- Ganeshan, B.; Panayiotou, E.; Burnand, K.; Dizdarevic, S.; Miles, K. Tumour heterogeneity in non-small cell lung carcinoma assessed by CT texture analysis: A potential marker of survival. Eur. Radiol. 2012, 22, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A.; Ganeshan, B.; Rodriguez-Justo, M.; Goh, V.J.; Ziauddin, Z.; Engledow, A.; Meagher, M.; Endozo, R.; Taylor, S.; Halligan, S.; et al. Multifunctional imaging signature for V-KI-RAS2 Kirsten rat sarcoma viral oncogene homolog (KRAS) mutations in colorectal cancer. J. Nucl. Med. 2014, 55, 386–391. [Google Scholar] [CrossRef]
- Ng, F.; Ganeshan, B.; Kozarski, R.; Miles, K.A.; Goh, V. Assessment of primary colorectal cancer heterogeneity by using whole-tumor texture analysis: Contrast-enhanced CT texture as a biomarker of 5-year survival. Radiology 2013, 266, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.; Landau, D.; Kozarski, R.; Ganeshan, B.; Thomas, R.; Michaelidou, A.; Goh, V. Primary esophageal cancer: Heterogeneity as potential prognostic biomarker in patients treated with definitive chemotherapy and radiation therapy. Radiology 2014, 270, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Graham, C.M.; Elci, O.; Griswold, M.E.; Zhang, X.; Khan, M.A.; Pitman, K.; Caudell, J.; Hamilton, R.; Ganshan, B.; et al. Locally advanced squamous cell carcinoma of the head and neck: CT texture and histogram analysis allow independent prediction of overall survival in patients treated with induction chemotherapy. Radiology 2013, 269, 801–809. [Google Scholar] [CrossRef]
- James, J.; Teo, M.; Ramachandran, V.; Law, M.; Stoney, D.; Cheng, M. A critical review of the chest CT scans performed to detect asymptomatic synchronous metastasis in new and recurrent breast cancers. World J. Surg. Oncol. 2019, 17, 40. [Google Scholar] [CrossRef]
- Ravaioli, A.; Pasini, G.; Polselli, A.; Papi, M.; Tassinari, D.; Arcangeli, V.; Milandri, C.; Amadori, D.; Bravi, M.; Rossi, D.; et al. Staging of breast cancer: New recommended standard procedure. Breast Cancer Res. Treat. 2002, 72, 53–60. [Google Scholar] [CrossRef]
- Barrett, T.; Bowden, D.J.; Greenberg, D.C.; Brown, C.H.; Wishart, G.C.; Britton, P.D. Radiological staging in breast cancer: Which asymptomatic patients to image and how. Br. J. Cancer 2009, 101, 1522–1528. [Google Scholar] [CrossRef]
- Linkugel, A.; Margenthaler, J.; Dull, B.; Cyr, A. Staging studies have limited utility for newly diagnosed stage I–II breast cancer. J. Surg. Res. 2015, 196, 33–38. [Google Scholar] [CrossRef]
- Jung, S.Y.; Kim, Y.A.; Lee, D.E.; Joo, J.; Back, J.H.; Kong, S.Y.; Lee, E.S. Clinical impact of follow-up imaging on mortality in Korean breast cancer patients: A national cohort study. Cancer Med. 2021, 10, 6480–6491. [Google Scholar] [CrossRef] [PubMed]
- Chee, C.G.; Kim, Y.H.; Lee, K.H.; Lee, Y.J.; Park, J.H.; Lee, H.S.; Ahn, S.; Kim, B. CT texture analysis in patients with locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy: A potential imaging biomarker for treatment response and prognosis. PLoS ONE 2017, 12, e0182883. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Edge, S.B.; Hortobagyi, G.N. Eighth Edition of the AJCC Cancer Staging Manual: Breast Cancer. Ann. Surg. Oncol. 2018, 25, 1783–1785. [Google Scholar] [CrossRef] [PubMed]
- James, D.; Clymer, B.D.; Schmalbrock, P. Texture detection of simulated microcalcification susceptibility effects in magnetic resonance imaging of breasts. J. Magn. Reson. Imaging 2001, 13, 876–881. [Google Scholar] [CrossRef] [PubMed]
- Waugh, S.A.; Purdie, C.A.; Jordan, L.B.; Vinnicombe, S.; Lerski, R.A.; Martin, P.; Thompson, A.M. Magnetic resonance imaging texture analysis classification of primary breast cancer. Eur. Radiol. 2016, 26, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Holli, K.; Lääperi, A.-L.; Harrison, L.; Luukkaala, T.; Toivonen, T.; Ryymin, P.; Dastidar, P.; Soimakallio, S.; Eskola, H. Characterization of breast cancer types by texture analysis of magnetic resonance images. Acad. Radiol. 2010, 17, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Giger, M.L.; Li, H.; Bick, U.; Newstead, G.M. Volumetric texture analysis of breast lesions on contrast-enhanced magnetic resonance images. Magn. Reson. Med. 2007, 58, 562–571. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, P.; Turnbull, L.W. Textural analysis of contrast-enhanced MR images of the breast. Magn. Reson. Med. 2003, 50, 92–98. [Google Scholar] [CrossRef]
- Pickles, M.D.; Lowry, M.; Gibbs, P. Pretreatment Prognostic Value of Dynamic Contrast-Enhanced Magnetic Resonance Imaging Vascular, Texture, Shape, and Size Parameters Compared with Traditional Survival Indicators Obtained From Locally Advanced Breast Cancer Patients. Investig. Radiol. 2016, 51, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Eun, N.L.; Kang, D.; Son, E.J.; Park, J.S.; Youk, J.H.; Kim, J.-A.; Gweon, H.M. Texture Analysis with 3.0-T MRI for Association of Response to Neoadjuvant Chemotherapy in Breast Cancer. Radiology 2020, 294, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Lim, Y.; Lee, K.S.; Han, B.-K.; Ko, E.Y.; Hahn, S.Y.; Nam, S.J. Breast Cancer Heterogeneity: MR Imaging Texture Analysis and Survival Outcomes. Radiology 2017, 282, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Lim, Y.; Cho, H.-H.; Lee, J.E.; Han, B.-K.; Ko, E.Y.; Choi, J.S.; Park, K.W. Radiomics Signature on Magnetic Resonance Imaging: Association with Disease-Free Survival in Patients with Invasive Breast Cancer. Clin. Cancer Res. 2018, 24, 4705–4714. [Google Scholar] [CrossRef]
- Perrone, A.; Lo Mele, L.; Sassi, S.; Marini, M.; Testaverde, L.; Izzo, L.; Marini, M. MDCT of the breast. AJR Am. J. Roentgenol. 2008, 190, 1644–1651. [Google Scholar] [CrossRef] [PubMed]
- Shan, X.; Wang, D.; Chen, J.; Xiao, X.B.; Jiang, Y.; Wang, Y.B.; Fan, Y. Necrosis degree displayed in computed tomography images correlated with hypoxia and angiogenesis in breast cancer. J. Comput. Assist. Tomogr. 2013, 37, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M.; Vaupel, P. Tumor hypoxia: Definitions and current clinical, biologic, and molecular aspects. J. Natl. Cancer Inst. 2001, 93, 266–276. [Google Scholar] [CrossRef]
- Matoori, S.; Thian, Y.; Koh, D.-M.; Sohaib, A.; Larkin, J.; Pickering, L.; Gutzeit, A. Contrast-Enhanced CT Density Predicts Response to Sunitinib Therapy in Metastatic Renal Cell Carcinoma Patients. Transl. Oncol. 2017, 10, 679–685. [Google Scholar] [CrossRef]
- Yun, G.; Kim, Y.H.; Lee, Y.J.; Kim, B.; Hwang, J.-H.; Choi, D.J. Tumor heterogeneity of pancreas head cancer assessed by CT texture analysis: Association with survival outcomes after curative resection. Sci. Rep. 2018, 8, 7226. [Google Scholar] [CrossRef]
- Cassinotto, C.; Chong, J.; Zogopoulos, G.; Reinhold, C.; Chiche, L.; Lafourcade, J.P.; Cuggia, A.; Terrebonne, E.; Dohan, A.; Gallix, B. Resectable pancreatic adenocarcinoma: Role of CT quantitative imaging biomarkers for predicting pathology and patient outcomes. Eur. J. Radiol. 2017, 90, 152–158. [Google Scholar] [CrossRef]
- Macmillan, R.; Barbera, D.; Hadjiminas, D.; Rampaul, R.; Lee, A.; Pinder, S.; Ellis, I.; Blamey, R.; Geraghty, J. Sentinel node biopsy for breast cancer may have little to offer four-node-samplers. results of a prospective comparison study. Eur. J. Cancer 2001, 37, 1076–1080. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.M.; Henson, D.E.; Chen, D.; Rajamarthandan, S. Histologic grade remains a prognostic factor for breast cancer regardless of the number of positive lymph nodes and tumor size: A study of 161,708 cases of breast cancer from the SEER Program. Arch. Pathol. Lab. Med. 2014, 138, 1048–1052. [Google Scholar] [CrossRef] [PubMed]
- Truong, P.T.; Yong, C.M.; Abnousi, F.; Lee, J.; Kader, H.A.; Hayashi, A.; Olivotto, I.A. Lymphovascular invasion is associated with reduced locoregional control and survival in women with node-negative breast cancer treated with mastectomy and systemic therapy. J. Am. Coll. Surg. 2005, 200, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Miles, K.A.; Ganeshan, B.; Griffiths, M.R.; Young, R.C.D.; Chatwin, C.R. Colorectal cancer: Texture analysis of portal phase hepatic CT images as a potential marker of survival. Radiology 2009, 250, 444–452. [Google Scholar] [CrossRef]
- Smith, A.D.; Gray, M.R.; Del Campo, S.M.; Shlapak, D.; Ganeshan, B.; Zhang, X.; Carson, W.E., III. Predicting Overall Survival in Patients with Metastatic Melanoma on Antiangiogenic Therapy and RECIST Stable Disease on Initial Posttherapy Images Using CT Texture Analysis. AJR Am. J. Roentgenol. 2015, 205, W283–W293. [Google Scholar] [CrossRef]
- Johnson, D.Y.; Farjat, A.E.; Vernuccio, F.; Hurwitz, L.M.; Nelson, R.C.; Marin, D. Evaluation of Intraindividual Contrast Enhancement Variability for Determining the Maximum Achievable Consistency in CT. AJR Am. J. Roentgenol. 2020, 214, 18–23. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | All Patients (n = 256) * | Nonrecurrence Group (n = 235) | Recurrence Group (n = 21) | p-Value |
|---|---|---|---|---|
| Patient age (years) | 54.86 ± 11.34 | 54.82 ± 11.10 | 55.28 ± 14.06 | 0.860 |
| Histological type | 1.000 | |||
| Invasive ductal | 218 (85.1) | 200 (85.1) | 18 (85.7) | |
| Others | 38 (14.9) | 35 (14.8) | 3 (14.3) | |
| Histological grade | <0.001 | |||
| I or II | 180 (70.3) | 173 (73.6) | 7 (33.3) | |
| III | 76 (29.7) | 62 (26.4) | 14 (66.7) | |
| Tumor size | 0.006 | |||
| ≤2 cm | 157 (61.3) | 150 (63.8) | 7 (33.3) | |
| >2 cm | 99 (38.7) | 85 (36.2) | 14 (66.7) | |
| LN a status | 0.063 | |||
| Negative | 169 (66.0) | 159 (67.7) | 10 (47.6) | |
| Positive | 87 (34.0) | 76 (32.3) | 11 (52.4) | |
| Lymphovascular invasion | 0.013 | |||
| Absent | 218 (85.2) | 204 (86.8) | 14 (66.7) | |
| Present | 38 (14.8) | 31 (13.2) | 7 (33.3) | |
| ER b status | 0.069 | |||
| Negative | 57 (22.3) | 49 (20.9) | 8 (38.1) | |
| Positive | 199 (77.7) | 186 (79.1) | 13 (61.9) | |
| PR c status | 0.230 | |||
| Negative | 69 (27.0) | 61 (26.0) | 8 (38.1) | |
| Positive | 187 (73.0) | 174 (74.0) | 13 (61.9) | |
| HER2 d status | 1.000 | |||
| Negative | 206 (80.5) | 189 (80.4) | 17 (81.0) | |
| Positive | 50 (19.5) | 46 (19.6) | 4 (19.0) | |
| Molecular subtype | 0.197 | |||
| Luminal-like | 167 (65.2) | 156 (66.4) | 11 (52.4) | |
| HER2-like | 50 (19.5) | 46 (19.6) | 4 (19.0) | |
| Basal-like | 39 (15.2) | 33 (14.0) | 6 (28.6) | |
| Ki-67 status | 0.001 | |||
| Low (<14%) | 159 (62.1) | 153 (65.1) | 6 (28.6) | |
| High (≥14%) | 97 (37.9) | 82 (34.9) | 15 (71.4) |
| CT Textural Features | All Patients (n = 256) * | Nonrecurrence Group (n = 235) | Recurrence Group (n = 21) | p-Value | Adjusted p-Value † |
|---|---|---|---|---|---|
| SSF a 0 | |||||
| Mean | 84.68 (66.98, 101.34) | 85.00 (67.17, 103.04) | 82.54 (53.17, 94.06) | 0.175 | |
| SD b | 47.16 (41.91, 52.78) | 47.09 (42.24, 53.10) | 47.98 (38.47, 50.17) | 0.339 | |
| MPP c | 90.02 (73.36, 105.63) | 89.91 (73.75, 106.77) | 90.20 (63.92, 96.75) | 0.157 | |
| Entropy | 4.78 (4.50, 5.01) | 4.78 (4.48, 5.01) | 4.96 (4.59, 5.16) | 0.098 | |
| Skewness | −0.03 (−0.19, 0.13) | −0.04 (−0.21, 0.13) | 0.10 (−0.13, 0.17) | 0.102 | |
| Kurtosis | −0.09 (−0.31, 0.09) | −0.09 (−0.09, 0.10) | −0.05 (−0.27, 0.02) | 0.802 | |
| SSF2 | |||||
| Mean | 40.44 (29.00, 65.40) | 42.78 (29.45, 67.47) | 32.74 (18.89, 43.07) | 0.004 | 0.032 |
| SD | 73.52 (63.57, 88.54) | 74.10 (63.67, 88.62) | 65.68 (61.30, 88.52) | 0.395 | |
| MPP | 78.55 (63.68, 100.52) | 79.68 (64.16, 101.72) | 64.31 (57.68, 83.45) | 0.016 | 0.039 |
| Entropy | 5.06 (4.71, 5.31) | 5.05 (1.70, 5.28) | 5.32 (4.82, 5.42) | 0.039 | 0.022 |
| Skewness | −0.09 (−0.34, 0.10) | −0.11 (−0.36, 0.10) | −0.04 (−0.60, 0.31) | 0.821 | |
| Kurtosis | −0.14 (−0.51, 0.27) | −0.16 (−0.52, 0.25) | 0.18 (−0.39, 0.38) | 0.322 | |
| SSF3 | |||||
| Mean | 57.10 (−0.51, 0.27) | 60.29 (41.44, 94.53) | 40.32 (26.46, 58.78) | 0.002 | 0.022 |
| SD | 69.06 (55.99, 80.75) | 69.08 (56.92, 80.82) | 63.91 (51.06, 80.98) | 0.265 | |
| MPP | 83.67 (66.04, 113.85) | 85.01 (68.63, 116.69) | 65.78 (53.74, 87.30) | 0.002 | 0.022 |
| Entropy | 5.00 (4.67, 5.22) | 4.99 (4.67, 5.21) | 5.21 (4.65, 5.34) | 0.107 | |
| Skewness | −0.18 (−0.44, 0.04) | −0.18 (−0.44, 0.04) | −0.19 (−0.38, 0.03) | 0.712 | |
| Kurtosis | −0.36 (−0.72, 0.11) | −0.37 (−0.73, 0.10) | −0.33 (−0.62, 0.36) | 0.265 | |
| SSF4 | |||||
| Mean | 70.51 (47.99, 100.00) | 72.14 (49.72, 109.77) | 48.06 (30.58, 68.78) | 0.004 | 0.032 |
| SD | 64.09 (50.95, 80.32) | 64.88 (51.67, 80.62) | 58.75 (45.97, 79.03) | 0.502 | |
| MPP | 89.97 (67.77, 122.21) | 91.39 (69.00, 123.78) | 67.27 (52.29, 90.34) | 0.006 | 0.036 |
| Entropy | 4.98 (4.63, 5.19) | 4.96 (4.62, 5.19) | 5.16 (4.63, 5.30) | 0.126 | |
| Skewness | −0.24 (−0.52, −0.01) | −0.24 (−0.52, 0.00) | −0.24 (−0.74, 0.40) | 0.862 | |
| Kurtosis | −0.49 (−0.85, −0.12) | −0.51 (−0.87, −0.02) | −0.30 (−0.74, 0.40) | 0.061 | |
| SSF5 | |||||
| Mean | 72.55 (47.57, 105.26) | 74.22 (50.81, 110.82) | 49.97 (31.48, 79.34) | 0.004 | 0.032 |
| SD | 60.84 (45.76, 79.58) | 61.08 (45.97, 80.23) | 57.88 (44.10, 75.15) | 0.502 | |
| MPP | 88.76 (67.56, 124.56) | 91.13 (69.23, 126.48) | 68.64 (53.83, 99.96) | 0.006 | 0.036 |
| Entropy | 4.94 (4.57, 5.21) | 4.92 (4.58, 5.18) | 5.11 (4.56, 5.28) | 0.126 | |
| Skewness | −0.26 (−0.51, −0.05) | −0.26 (−0.50, −0.05) | −0.29 (−0.62, 0.02) | 0.862 | |
| Kurtosis | −0.60 (−0.60, −0.19) | −0.64 (−0.89, −0.22) | −0.40 (−0.71, 0.23) | 0.061 | |
| SSF6 | |||||
| Mean | 69.69 (43.71, 102.11) | 74.22 (45.80, 104.65) | 42.90 (24.56, 77.29) | 0.011 | 0.039 |
| SD | 57.27 (41.61, 79.39) | 56.63 (41.67, 81.58) | 60.03 (40.98, 73.46) | 0.777 | |
| MPP | 89.16 (59.21, 122.40) | 90.03 (61.50, 124.24) | 68.90(51.85, 100.47) | 0.020 | 0.039 |
| Entropy | 4.92 (4.52, 5.20) | 4.90 (4.51, 5.19) | 5.03 (4.59, 5.36) | 0.113 | |
| Skewness | −0.03 (−0.19, 0.13) | −0.29 (−0.53, −0.07) | −0.41 (−0.67, 0.09) | 0.898 | |
| Kurtosis | −0.09 (−0.09, 0.09) | −0.70 (−0.93, −0.31) | −0.27 (−0.76, 0.24) | 0.018 | 0.039 |
| Univariate Analysis | |||
|---|---|---|---|
| Variable | HR | 95% CI | p-Value |
| Clinicopathologic features | |||
| Histological grade | 0.002 | ||
| III | 4.260 | 1.713–10.590 | |
| I or II | Reference | ||
| Tumor size | 0.008 | ||
| >2 cm | 3.461 | 1.392–8.606 | |
| ≤2 cm | Reference | ||
| Stage | |||
| II | 2.398 | 0.872–6.593 | 0.090 |
| I | Reference | ||
| Lymphovascular invasion | 0.034 | ||
| Present | 2.678 | 1.077–6.664 | |
| Absent | Reference | ||
| Ki-67 status | 0.015 | ||
| High (≥14%) | 3.269 | 1.263–8.464 | |
| Low (<14%) | Reference | ||
| Textural Features | |||
| Mean using SSF2 a 32.76 HU 32.76 HU | 23.267 Reference | 0.025–21,555.829 | 0.367 |
| MPP b at SSF2 | |||
| <68.06 HU | 2.395 | 1.006–5.702 | 0.048 |
| 68.06 HU | Reference | ||
| Entropy using SSF2 | <0.001 | ||
| >5.31 | 4.809 | 2.007–11.523 | |
| ≤5.31 | Reference | ||
| Mean using SSF3 | 0.017 | ||
| <47.31 HU | 2.926 | 1.209, 7.077 | |
| 47.31 HU | Reference | ||
| MPP using SSF3 | 0.001 | ||
| <66.74 HU | 4.597 | 1.901–11.114 | |
| 66.74 HU | Reference | ||
| Mean using SSF4 | 0.001 | ||
| <54.97 HU | 4.401 | 1.771–10.934 | |
| 54.97 HU | Reference | ||
| MPP using SSF4 | 0.004 | ||
| <80.81 HU | 4.023 | 1.559–10.383 | |
| 80.81 HU | Reference | ||
| Mean using SSF5 | 0.002 | ||
| 62.59 HU | 4.390 | 1.698–11.348 | |
| 62.59 HU | Reference | ||
| MPP using SSF5 | 0.005 | ||
| <74.50 HU | 3.530 | 1.459–8.540 | |
| 74.50 HU | Reference | ||
| Mean using SSF6 | 0.012 | ||
| <52.45 HU | 3.057 | 1.283–7.281 | |
| 52.45 HU | Reference | ||
| MPP using SSF6 | 0.021 | ||
| <86.40 HU | 3.070 | 1.188–7.931 | |
| 86.40 HU | Reference | ||
| Kurtosis using SSF6 | 0.168 | ||
| >−0.50 | 1.844 | 0.773–4.399 | |
| ≤−0.50 | Reference | ||
| Multivariate Analysis | |||
|---|---|---|---|
| Variable | HR | 95% CI | p-Value |
| Clinicopathological features | |||
| Histologic grade | <0.001 | ||
| III | 6.128 | 2.322–16.172 | |
| I or II | Reference | ||
| Lymphovascular invasion | 0.029 | ||
| Present | 2.931 | 1.116–7.696 | |
| Absent | Reference | ||
| Textural features | |||
| Mean using SSF5 a | 0.003 | ||
| 62.59 HU | 4.714 | 1.685–13.183 | |
| 62.59 HU | Reference | ||
| Entropy using SSF2 | 0.036 | ||
| >5.31 | 2.770 | 1.068–7.184 | |
| ≤5.31 | Reference | ||
| Features | Mean Using SSF5 a | Entropy Using SSF2 | ||
|---|---|---|---|---|
| Mean Value | p | Mean Value | p | |
| Histological type | 0.684 | 0.266 | ||
| Invasive ductal | 80.00 ± 51.24 | 4.95 ± 0.43 | ||
| Others | 76.83 ± 39.70 | 5.04 ± 0.44 | ||
| Histological grade | 0.967 | 0.002 | ||
| I or II | 79.94 ± 51.41 | 4.91 ± 0.43 | ||
| III | 79.66 ± 45.50 | 5.09 ± 0.41 | ||
| Tumor size | <0.001 | <0.001 | ||
| ≤2 cm | 87.70 ± 55.38 | 4.82 ± 0.42 | ||
| >2 cm | 67.43 ± 35.72 | 5.21 ± 0.32 | ||
| LN a status | 0.347 | 0.040 | ||
| Negative | 81.85 ± 52.22 | 4.93 ± 0.44 | ||
| Positive | 75.79 ± 44.22 | 5.04 ± 0.40 | ||
| Lymphovascular invasion | 0.189 | 0.004 | ||
| Absent | 81.56 ± 50.19 | 4.93 ± 0.43 | ||
| Present | 70.09 ± 45.80 | 5.15 ± 0.37 | ||
| ER b status | 0.830 | 0.153 | ||
| Negative | 79.50 ± 50.28 | 4.95 ± 0.43 | ||
| Positive | 81.10 ± 47.76 | 5.04 ± 0.41 | ||
| PR c status | 0.497 | 0.166 | ||
| Negative | 78.58 ± 50.35 | 4.94 ± 0.42 | ||
| Positive | 83.33 ± 47.88 | 5.03 ± 0.44 | ||
| HER2 d status | 0.784 | 0.015 | ||
| Negative | 78.33 ± 41.70 | 5.10 ± 0.39 | ||
| Positive | 80.23 ± 51.47 | 4.93 ± 0.43 | ||
| Molecular subtype | 0.450 | 0.142 | ||
| Luminal-like | 79.81 ± 52.24 | 4.92 ± 0.43 | ||
| HER2-like | 78.33 ± 41.70 | 5.10 ± 0.39 | ||
| Basal-like | 82.04 ± 48.65 | 4.97 ± 0.42 | ||
| Ki-67 status | 0.872 | 0.004 | ||
| Low (<14%) | 79.46 ± 48.07 | 4.91 ± 0.43 | ||
| High (≥14%) | 80.51 ± 52.37 | 5.06 ± 0.40 | ||
| Features | β (SE b) | Odds Ratio | 95% CI | p |
|---|---|---|---|---|
| Histologic type † | −0.009 (0.070) | −0.135 | −0.147–0.128 | 0.893 |
| Histological grade ‡ | 0.039 (0.062) | 0.627 | −0.083–0.161 | 0.531 |
| Tumor size †† | 0.358 (0.054) | 6.598 | 0.251–0.465 | <0.001 |
| LN status § | 0.025 (0.055) | 0.451 | −0.083–0.132 | 0.652 |
| Lymphovascular invasion * | 0.054 (0.074) | 0.731 | −0.092–0.200 | 0.466 |
| HER2 a status # | −0.075 (0.062) | −1.195 | −0.197–0.048 | 0.233 |
| Ki-67 status √ | 0.111 (0.057) | 1.949 | −0.001–0.223 | 0.049 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, H.; Cho, K.R.; Song, S.E.; Cho, Y.; Jung, S.P.; Sung, K. Tumor Heterogeneity of Breast Cancer Assessed with Computed Tomography Texture Analysis: Association with Disease-Free Survival and Clinicopathological Prognostic Factor. Diagnostics 2023, 13, 3569. https://doi.org/10.3390/diagnostics13233569
Yoo H, Cho KR, Song SE, Cho Y, Jung SP, Sung K. Tumor Heterogeneity of Breast Cancer Assessed with Computed Tomography Texture Analysis: Association with Disease-Free Survival and Clinicopathological Prognostic Factor. Diagnostics. 2023; 13(23):3569. https://doi.org/10.3390/diagnostics13233569
Chicago/Turabian StyleYoo, Hyeongyu, Kyu Ran Cho, Sung Eun Song, Yongwon Cho, Seung Pil Jung, and Kihoon Sung. 2023. "Tumor Heterogeneity of Breast Cancer Assessed with Computed Tomography Texture Analysis: Association with Disease-Free Survival and Clinicopathological Prognostic Factor" Diagnostics 13, no. 23: 3569. https://doi.org/10.3390/diagnostics13233569
APA StyleYoo, H., Cho, K. R., Song, S. E., Cho, Y., Jung, S. P., & Sung, K. (2023). Tumor Heterogeneity of Breast Cancer Assessed with Computed Tomography Texture Analysis: Association with Disease-Free Survival and Clinicopathological Prognostic Factor. Diagnostics, 13(23), 3569. https://doi.org/10.3390/diagnostics13233569