
The Impact of the Rapid Blood Culture Identification Panel on Antibiotic Treatment and Clinical Outcomes in Bloodstream Infections, Particularly Those Associated with Multidrug-Resistant Micro-Organisms


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Settings
2.2. Conventional Identification and Antimicrobial Susceptibility Methods
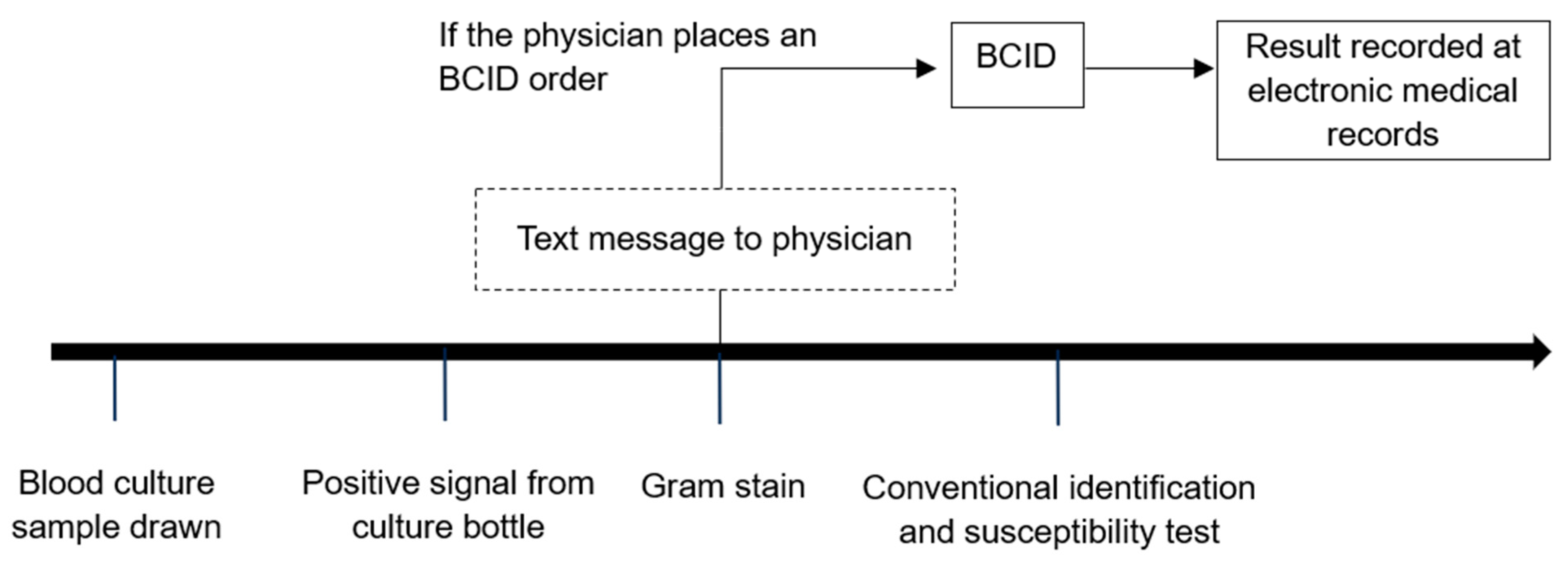
2.3. BCID Testing Process
2.4. BCID Panel Testing Method
2.5. Outcomes and Variables
2.6. Statistical Analysis
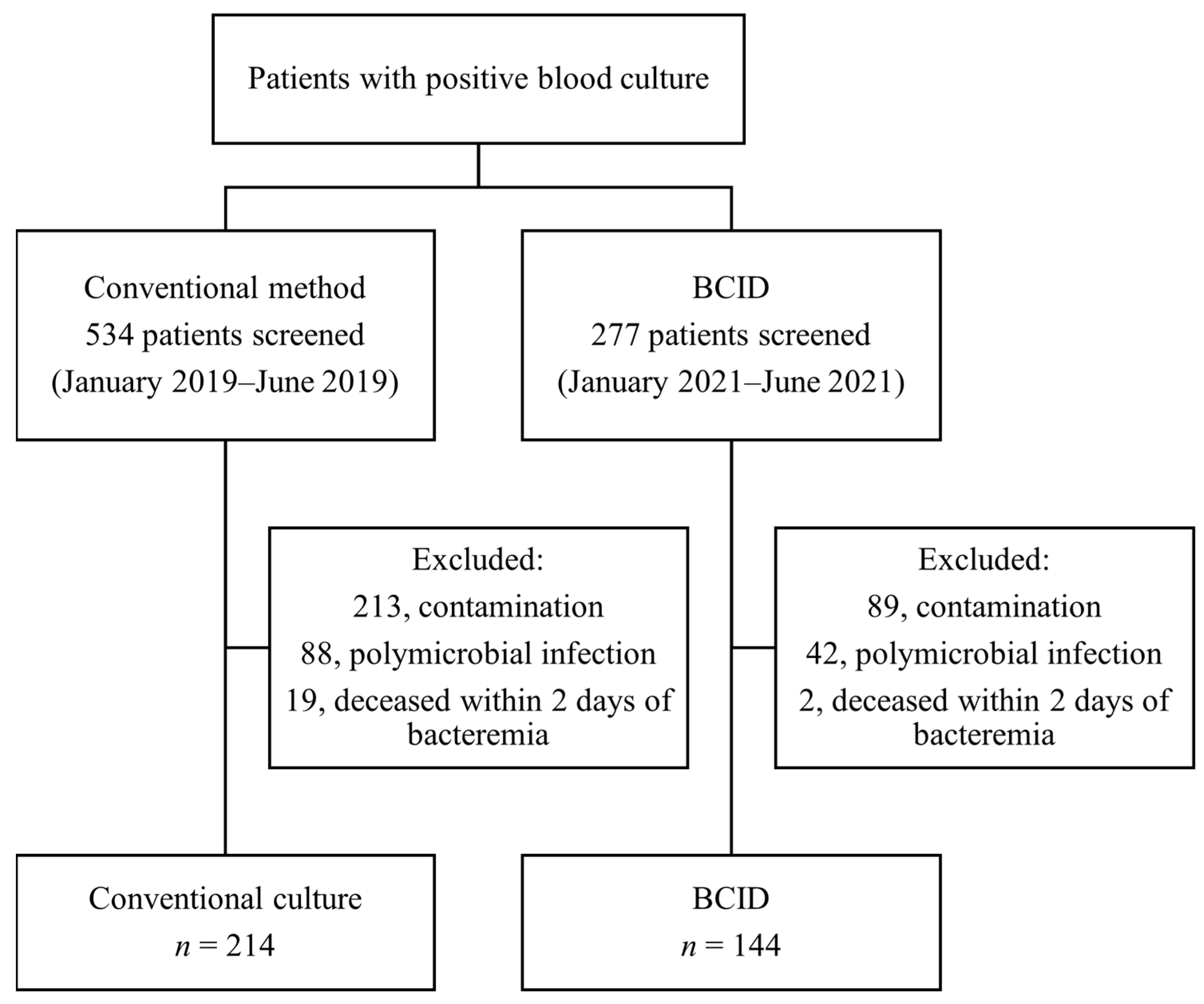
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marchaim, D.; Gottesman, T.; Schwartz, O.; Korem, M.; Maor, Y.; Rahav, G.; Karplus, R.; Lazarovitch, T.; Braun, E.; Sprecher, H.; et al. National multicenter study of predictors and outcomes of bacteremia upon hospital admission caused by Enterobacteriaceae producing extended-spectrum beta-lactamases. Antimicrob. Agents Chemother. 2010, 54, 5099–5104. [Google Scholar] [CrossRef]
- Song, K.H.; Kim, C.J.; Choi, N.K.; Ahn, J.; Choe, P.G.; Park, W.B.; Kim, N.J.; Choi, H.J.; Bae, J.Y.; Kim, E.S.; et al. Clinical and economic burden of bacteremia due to multidrug-resistant organisms in korea: A prospective case control study. J. Glob. Antimicrob. Resist. 2022, 31, 379–385. [Google Scholar] [CrossRef]
- Kumar, A.; Haery, C.; Paladugu, B.; Kumar, A.; Symeoneides, S.; Taiberg, L.; Osman, J.; Trenholme, G.; Opal, S.M.; Goldfarb, R.; et al. The duration of hypotension before the initiation of antibiotic treatment is a critical determinant of survival in a murine model of Escherichia coli septic shock: Association with serum lactate and inflammatory cytokine levels. J. Infect. Dis. 2006, 193, 251–258. [Google Scholar] [CrossRef]
- Lee, C.M.; Kim, C.-J.; Kim, S.E.; Park, K.-H.; Bae, J.Y.; Choi, H.J.; Jung, Y.; Lee, S.S.; Choe, P.G.; Park, W.B.; et al. Risk factors for early mortality in patients with carbapenem-resistant Acinetobacter baumannii bacteraemia. J. Glob. Antimicrob. Resist. 2022, 31, 45–51. [Google Scholar] [CrossRef]
- Timbrook, T.T.; Caffrey, A.R.; Ovalle, A.; Beganovic, M.; Curioso, W.; Gaitanis, M.; LaPlante, K.L. Assessments of opportunities to improve antibiotic prescribing in an emergency department: A period prevalence survey. Infect. Dis. Ther. 2017, 6, 497–505. [Google Scholar] [CrossRef]
- Canalp, H.Z.; Bayraktar, B. Direct rapid identification from positive blood cultures by MALDI-TOF MS: Specific focus on turnaround times. Microbiol. Spectr. 2021, 9, e01103-21. [Google Scholar] [CrossRef]
- Banerjee, R.; Teng, C.B.; Cunningham, S.A.; Ihde, S.M.; Steckelberg, J.M.; Moriarty, J.P.; Shah, N.D.; Mandrekar, J.N.; Patel, R. Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification and susceptibility testing. Clin. Infect. Dis. 2015, 61, 1071–1080. [Google Scholar] [CrossRef]
- Prod’hom, G.; Durussel, C.; Greub, G.J. A simple blood-culture bacterial pellet preparation for faster accurate direct bacterial identification and antibiotic susceptibility testing with the VITEK 2 system. Med. Microbiol. 2013, 62 Pt 5, 773–777. [Google Scholar] [CrossRef]
- Clerc, O.; Prod’hom, G.; Vogne, C.; Bizzini, A.; Calandra, T.; Greub, G. Impact of matrix-assisted laser desorption ionization time-of-flight mass spectrometry on the clinical management of patients with Gram-negative bacteremia: A prospective observational study. Clin. Infect. Dis. 2013, 56, 1101–1107. [Google Scholar] [CrossRef]
- BioFire Diagnostics, I. Filmarray Blood Culture Identification Panel: Instruction Booklet; BioFire Diagnostics, Inc.: Salt Lake City, UT, USA, 2013. [Google Scholar]
- Blaschke, A.J.; Heyrend, C.; Byington, C.L.; Fisher, M.A.; Barker, E.; Garrone, N.F.; Thatcher, S.A.; Pavia, A.T.; Barney, T.; Alger, G.D.; et al. Rapid identification of pathogens from positive blood cultures by multiplex polymerase chain reaction using the filmarray system. Diagn. Microbiol. Infect. Dis. 2012, 74, 349–355. [Google Scholar] [CrossRef]
- Yang, M.; Tao, C. Diagnostic efficiency of the filmarray blood culture identification (BCID) panel: A systematic review and meta-analysis. J. Med. Microbiol. 2023, 72, 001608. [Google Scholar] [CrossRef]
- So, M.-K.; Kim, S.-K.; Chung, H.-S.; Bae, J.-Y.; Lee, M. Large-scale clinical evaluation of rapid blood culture identification panels for bloodstream infections at a tertiary hospital. Diagnostics 2023, 13, 1177. [Google Scholar] [CrossRef]
- MacVane, S.H.; Nolte, F.S. Benefits of adding a rapid PCR-based blood culture identification panel to an established antimicrobial stewardship program. J. Clin. Microbiol. 2016, 54, 2455–2463. [Google Scholar] [CrossRef]
- Carver, P.L.; Lin, S.W.; DePestel, D.D.; Newton, D.W. Impact of meca gene testing and intervention by infectious disease clinical pharmacists on time to optimal antimicrobial therapy for Staphylococcus aureus bacteremia at a university hospital. J. Clin. Microbiol. 2008, 46, 2381–2383. [Google Scholar] [CrossRef]
- Frye, A.M.; Baker, C.A.; Rustvold, D.L.; Heath, K.A.; Hunt, J.; Leggett, J.E.; Oethinger, M. Clinical impact of a real-time PCR assay for rapid identification of staphylococcal bacteremia. J. Clin. Microbiol. 2012, 50, 127–133. [Google Scholar] [CrossRef]
- Britt, N.S.; Khader, K.; He, T.; Willson, T.M.; Effiong, A.; Timbrook, T.T.; Potter, E.M.; Lodise, T.P. Examining the clinical impact of rapid multiplex polymerase chain reaction-based diagnostic testing for bloodstream infections in a national cohort of the veterans health administration. Pharmacotherapy 2023, 43, 24–34. [Google Scholar] [CrossRef]
- Pardo, J.; Klinker, K.P.; Borgert, S.J.; Butler, B.M.; Giglio, P.G.; Rand, K.H. Clinical and economic impact of antimicrobial stewardship interventions with the filmarray blood culture identification panel. Diagn. Microbiol. Infect. Dis. 2016, 84, 159–164. [Google Scholar] [CrossRef]
- Carvalhaes, C.G.; Picão, R.C.; Nicoletti, A.G.; Xavier, D.E.; Gales, A.C. Cloverleaf test (modified hodge test) for detecting carbapenemase production in Klebsiella pneumoniae: Be aware of false positive results. J. Antimicrob. Chemother. 2010, 65, 249–251. [Google Scholar] [CrossRef]
- Nordmann, P.; Poirel, L.; Dortet, L. Rapid detection of carbapenemase-producing Enterobacteriaceae. Emerg. Infect. Dis. 2012, 18, 1503–1507. [Google Scholar] [CrossRef]
- Dortet, L.; Poirel, L.; Nordmann, P. Rapid identification of carbapenemase types in Enterobacteriaceae and Pseudomonas spp. by using a biochemical test. Antimicrob. Agents Chemother. 2012, 56, 6437–6440. [Google Scholar] [CrossRef]
- CLSI. Performance Standards for Antimicrobial Susceptibility Testing, 28th ed.; Clinical and Laboratory Standards Institute: Malvern, PA, USA, 2023. [Google Scholar]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson comorbidity index: A critical review of clinimetric properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef]
- Al-Hasan, M.N.; Baddour, L.M. Resilience of the pitt bacteremia score: 3 decades and counting. Clin. Infect. Dis. 2019, 70, 1834–1836. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Berinson, B.; Both, A.; Berneking, L.; Christner, M.; Lütgehetmann, M.; Aepfelbacher, M.; Rohde, H. Usefulness of biofire filmarray BCID2 for blood culture processing in clinical practice. J. Clin. Microbiol. 2021, 59, e0054321. [Google Scholar] [CrossRef]
- Donnars, A.; Mahieu, R.; Declerck, C.; Chenouard, R.; Lemarié, C.; Pailhoriès, H.; Requin, J.; Kempf, M.; Eveillard, M. Biofire® blood culture identification 2 (BCID2) panel for early adaptation of antimicrobial therapy in adult patients with bloodstream infections: A real-life experience. Diagn. Microbiol. Infect. Dis. 2023, 105, 115858. [Google Scholar] [CrossRef]
- Cortazzo, V.; D’Inzeo, T.; Giordano, L.; Menchinelli, G.; Liotti, F.M.; Fiori, B.; De Maio, F.; Luzzaro, F.; Sanguinetti, M.; Posteraro, B.; et al. Comparing biofire filmarray BCID2 and BCID panels for direct detection of bacterial pathogens and antimicrobial resistance genes from positive blood cultures. J. Clin. Microbiol. 2021, 59, e03163-20. [Google Scholar] [CrossRef]
- Kanda, N.; Hashimoto, H.; Suzuki, T.; Nakamura, K. Performance of the new filmarray blood culture identification 2 panel and its potential impact on clinical use in patients with gram-negative bacteremia. J. Infect. Chemother. 2022, 28, 1037–1040. [Google Scholar] [CrossRef]
- Nasef, R.; El Lababidi, R.; Alatoom, A.; Krishnaprasad, S.; Bonilla, F. The impact of integrating rapid PCR-based blood culture identification panel to an established antimicrobial stewardship program in the united arab of emirates. Int. J. Infect. Dis. 2020, 91, 124–128. [Google Scholar] [CrossRef]
- Donner, L.M.; Campbell, W.S.; Lyden, E.; Schooneveld, T.C.V. Assessment of rapid-blood-culture-identification result interpretation and antibiotic prescribing practices. J. Clin. Microbiol. 2017, 55, 1496–1507. [Google Scholar] [CrossRef]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the infectious diseases society of america and the society for healthcare epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- Chiasson, J.M.; Smith, W.J.; Jodlowski, T.Z.; Kouma, M.A.; Cutrell, J.B. Impact of a rapid blood culture diagnostic panel on time to optimal antimicrobial therapy at a veterans affairs medical center. J. Pharm. Pract. 2022, 35, 722–729. [Google Scholar] [CrossRef]
- Ibrahim, E.H.; Sherman, G.; Ward, S.; Fraser, V.J.; Kollef, M.H. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the icu setting. Chest 2000, 118, 146–155. [Google Scholar] [CrossRef]
- Kang, C.-I.; Kim, S.-H.; Kim, H.-B.; Park, S.-W.; Choe, Y.-J.; Oh, M.-d.; Kim, E.-C.; Choe, K.-W. Pseudomonas aeruginosa bacteremia: Risk factors for mortality and influence of delayed receipt of effective antimicrobial therapy on clinical outcome. Clin. Infect. Dis. 2003, 37, 745–751. [Google Scholar] [CrossRef]
- Tellor, B.; Skrupky, L.P.; Symons, W.; High, E.; Micek, S.T.; Mazuski, J.E. Inadequate source control and inappropriate antibiotics are key determinants of mortality in patients with intra-abdominal sepsis and associated bacteremia. Surg. Infect. 2015, 16, 785–793. [Google Scholar] [CrossRef]
- Lahey, T.; Shah, R.; Gittzus, J.; Schwartzman, J.; Kirkland, K. Infectious diseases consultation lowers mortality from Staphylococcus aureus bacteremia. Medicine 2009, 88, 263–267. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| BCID (n = 144) | Conventional (n = 214) | p | |
|---|---|---|---|
| Age, mean (SD) | 68 (16) | 68 (16) | 0.932 |
| Male sex, n (%) | 65 (45.1) | 104 (48.6) | 0.520 |
| ICU, n (%) | 58 (40.3) | 62 (29.0) | 0.026 |
| Hematology department, n (%) | 13 (9.0) | 24 (11.2) | 0.505 |
| Hospital-acquired, n (%) | 39 (27.1) | 80 (37.4) | 0.043 |
| Pitt bacteremia score, median (IQR) | 2 (0–4) | 2 (0–3) | 0.306 |
| Charlson comorbidity index, median (IQR) | 2 (1–4) | 2 (1–3) | 0.808 |
| Gram-positive, n (%) | 58 (40.3) | 112 (52.3) | 0.025 |
| Gram-negative, n (%) | 84 (58.3) | 97 (45.3) | 0.016 |
| Yeasts, n (%) | 2 (1.4) | 5 (2.3) | 0.706 |
| MRSA, n (%) | 7 (4.9) | 7 (3.3) | 0.447 |
| VRE, n (%) | 5 (3.5) | 9 (4.2) | 0.726 |
| CRE, n (%) | 0 (0.0) | 1 (0.5) | 1.000 |
| CRAB, n (%) | 2 (1.4) | 6 (2.8) | 0.483 |
| 30-day mortality, n (%) | 14 (9.7) | 23 (10.7) | 0.755 |
| Length of stay, d, median (IQR) | 15 (9–27) | 14 (8–30) | 0.504 |
| Time to effective antibiotics, h, median (IQR) | 3 (0–32) | 3 (0–41) | 0.789 |
| Time to appropriate antibiotics, h, median (IQR) | 37 (1–90) | 44 (1–93) | 0.727 |
| BCID (n = 144) | Conventional (n = 214) | |
|---|---|---|
| Micro-organisms included in BCID panel, n (%) | 135 (93.8) | 194 (90.7) |
| Gram-positive | ||
| Enterococcus faecalis | 6 | 9 |
| Enterococcus faecium | 8 | 19 |
| other Enterococcus spp. | 0 | 2 |
| Staphylococcus aureus | 17 | 19 |
| coagulase-negative staphylococci | 16 | 30 |
| Streptococcus spp. | 5 | 20 |
| Gram-negative | ||
| Citrobacter freundii | 0 | 1 |
| Citrobacter koseri | 0 | 1 |
| Enterobacter cloacae | 1 | 2 |
| Enterobacter aerogenes | 1 | 1 |
| Enterobacter ludwigii | 1 | 0 |
| Escherichia coli | 43 | 55 |
| Klebsiella pneumonia | 24 | 18 |
| other Klebsiella spp. | 2 | 2 |
| Proteus mirabilis | 3 | 0 |
| Salmonella spp. | 1 | 1 |
| Serratia marcescens | 1 | 0 |
| Acinetobacter baumannii | 2 | 6 |
| Pseudomonas aeruginosa | 3 | 3 |
| Yeasts | ||
| Candida spp. | 1 | 5 |
| Micro-organisms not included in BCID panel, n (%) | 9 (6.3) | 20 (9.3) |
| Granulicatella adiacens | 0 | 1 |
| Corynebacterium striatum | 0 | 3 |
| Actinotignum schaalii | 1 | 0 |
| Clostridium spp. | 2 | 7 |
| Eggerthia catenaformis | 1 | 0 |
| Eubacterium spp. | 1 | 2 |
| Lactobacillus spp. | 1 | 0 |
| Acinetobacter ursingii | 1 | 0 |
| Chryseobacterium meningosepticum | 0 | 1 |
| Bacteroides spp. | 1 | 4 |
| Fusobacterium periodonticum | 0 | 1 |
| Prevotella nigrescens | 0 | 1 |
| Saccharomyces cerevisiae | 1 | 0 |
| Adjusted OR | 95% CI | p | |
|---|---|---|---|
| Pitt bacteremia score | 1.304 | 1.133–1.501 | <0.001 |
| Charlson comorbidity index | 1.317 | 1.147–1.513 | <0.001 |
| BCID | 0.833 | 0.398–1.743 | 0.627 |
| Subgroup | Adjusted OR | 95% CI | p |
|---|---|---|---|
| ICU | 1.563 | 0.558–4.378 | 0.396 |
| Hematology department | 1.718 | 0.200–14.788 | 0.622 |
| Hospital-acquired | 1.162 | 0.380–3.549 | 0.792 |
| Gram-positive organism | 1.519 | 0.534–4.317 | 0.433 |
| Gram-negative organism | 0.485 | 0.153–1.540 | 0.220 |
| BCID | Conventional | p | |
|---|---|---|---|
| CRE | n = 15 | n = 7 | |
| Time to effective antibiotics, h, median (IQR) | 39 (27–53) | 93 (63–98) | 0.012 |
| 30-day mortality, n (%) | 6 (40.0) | 1 (14.3) | 0.354 |
| CRAB | n = 52 | n = 34 | |
| Time to effective antibiotics, h, median (IQR) | 29 (16–52) | 42 (6–78) | 0.340 |
| 30-day mortality, n (%) | 31 (59.6) | 18 (52.9) | 0.541 |
| VRE | n = 40 | n = 41 | |
| Time to effective antibiotics, h, median (IQR) | 50 (33–86) | 92 (77–102) | <0.001 |
| 30-day mortality, n (%) | 8 (20.0) | 12 (29.3) | 0.333 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bae, J.-Y.; Bae, J.; So, M.-K.; Choi, H.-J.; Lee, M. The Impact of the Rapid Blood Culture Identification Panel on Antibiotic Treatment and Clinical Outcomes in Bloodstream Infections, Particularly Those Associated with Multidrug-Resistant Micro-Organisms. Diagnostics 2023, 13, 3504. https://doi.org/10.3390/diagnostics13233504
Bae J-Y, Bae J, So M-K, Choi H-J, Lee M. The Impact of the Rapid Blood Culture Identification Panel on Antibiotic Treatment and Clinical Outcomes in Bloodstream Infections, Particularly Those Associated with Multidrug-Resistant Micro-Organisms. Diagnostics. 2023; 13(23):3504. https://doi.org/10.3390/diagnostics13233504
Chicago/Turabian StyleBae, Ji-Yun, Jiyeon Bae, Min-Kyung So, Hee-Jung Choi, and Miae Lee. 2023. "The Impact of the Rapid Blood Culture Identification Panel on Antibiotic Treatment and Clinical Outcomes in Bloodstream Infections, Particularly Those Associated with Multidrug-Resistant Micro-Organisms" Diagnostics 13, no. 23: 3504. https://doi.org/10.3390/diagnostics13233504
APA StyleBae, J.-Y., Bae, J., So, M.-K., Choi, H.-J., & Lee, M. (2023). The Impact of the Rapid Blood Culture Identification Panel on Antibiotic Treatment and Clinical Outcomes in Bloodstream Infections, Particularly Those Associated with Multidrug-Resistant Micro-Organisms. Diagnostics, 13(23), 3504. https://doi.org/10.3390/diagnostics13233504