
Preoperative Prediction of New Vertebral Fractures after Vertebral Augmentation with a Radiomics Nomogram

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Image Acquisition and Radiomics Feature Extraction
2.3. Radiomics Feature Selection and Radiomics Score Construction
2.4. Construction and Evaluation of a Predictive Radiomics Nomogram
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sets
3.2. Construction and Validation of the Radiomics Score
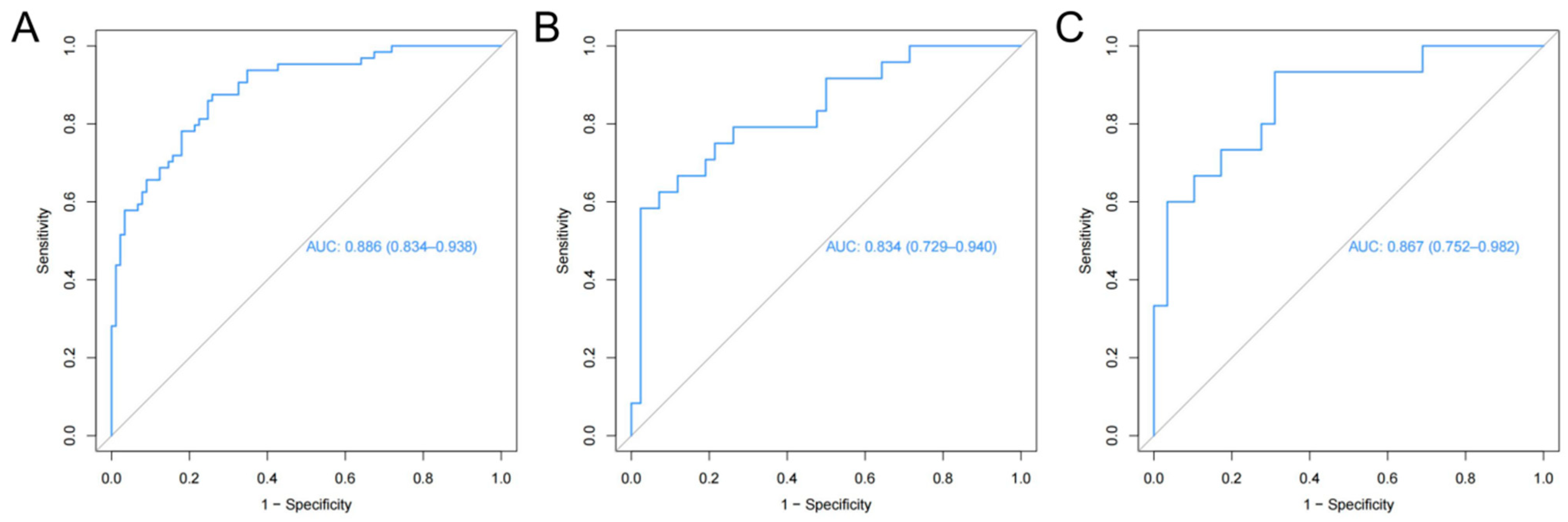
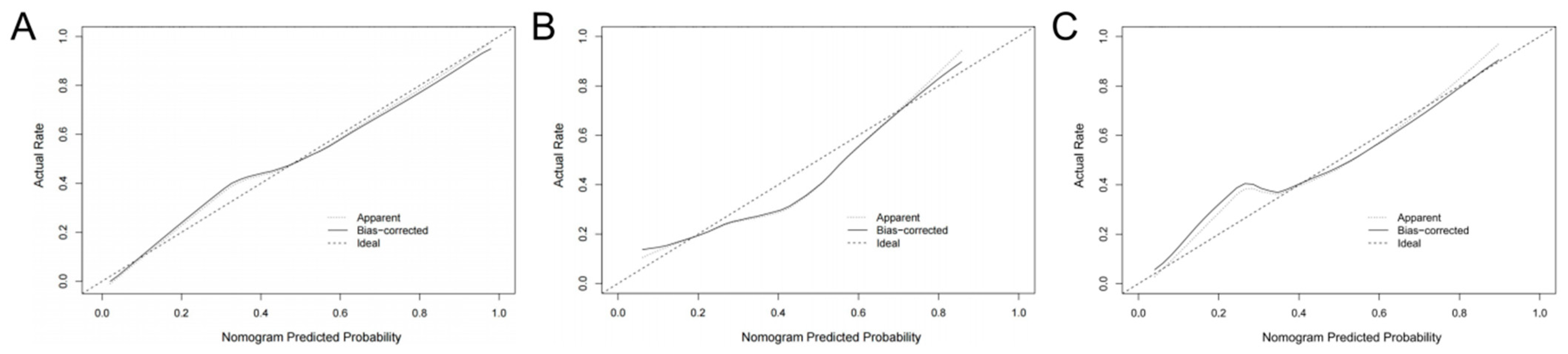
3.3. Prediction Radiomics Nomogram Development and Validation
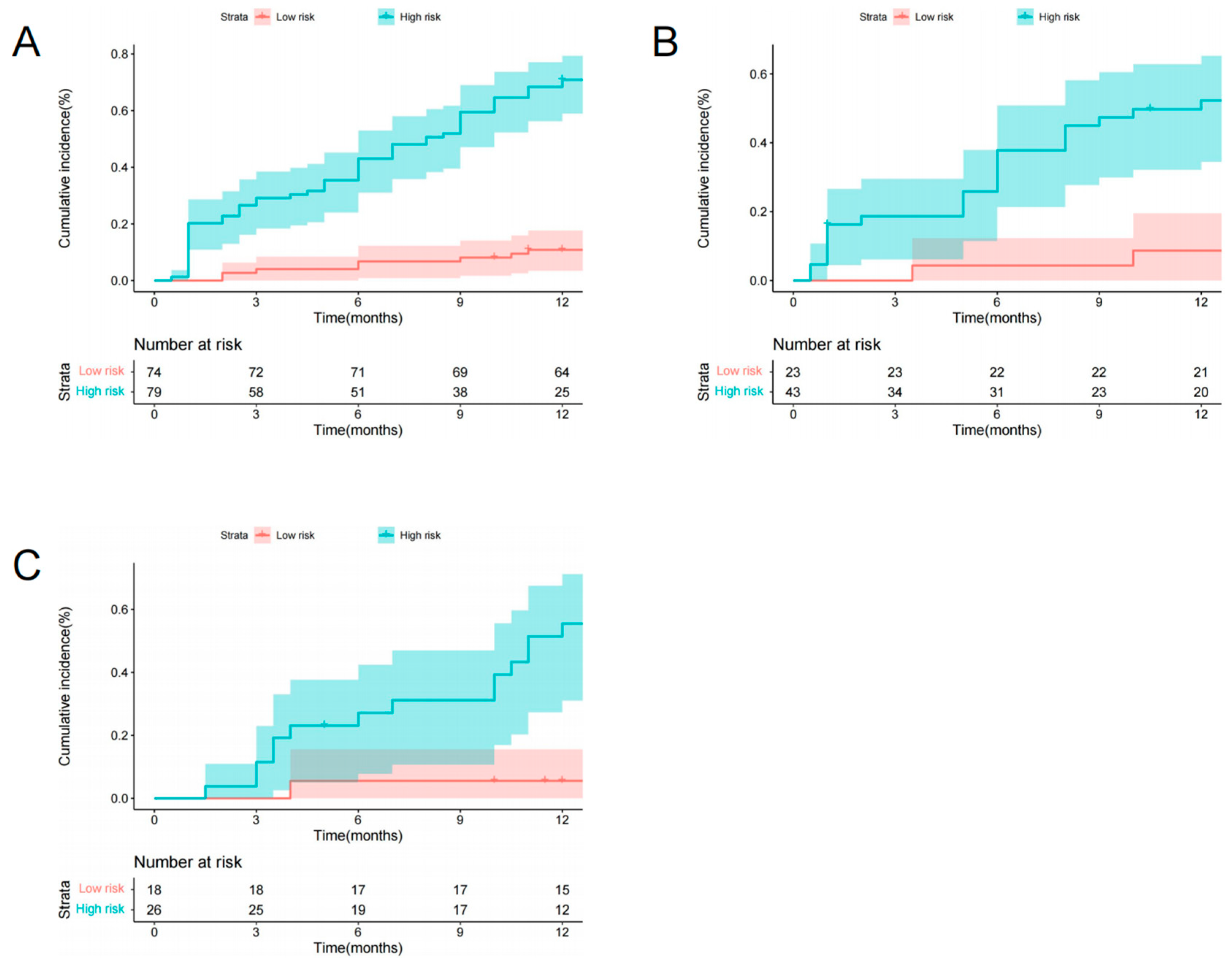
3.4. Risk Stratification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ensrud, K.E.; Crandall, C.J. Osteoporosis. Ann. Intern. Med. 2017, 167, ITC17–ITC32. [Google Scholar] [CrossRef]
- Compston, J.E.; McClung, M.R.; Leslie, W.D. Osteoporosis. Lancet 2019, 393, 364–376. [Google Scholar] [CrossRef]
- Johnell, O. The socioeconomic burden of fractures: Today and in the 21st century. Am. J. Med. 1997, 103, 20S–25S; discussion 25S–26S. [Google Scholar] [CrossRef]
- Schousboe, J.T. Epidemiology of Vertebral Fractures. J. Clin. Densitom. 2016, 19, 8–22. [Google Scholar] [CrossRef]
- Ensrud, K.E.; Schousboe, J.T. Vertebral Fractures. N. Engl. J. Med. 2011, 364, 1634–1642. [Google Scholar] [CrossRef]
- Ebeling, P.R.; Akesson, K.; Bauer, D.C.; Buchbinder, R.; Eastell, R.; Fink, H.A.; Giangregorio, L.; Guanabens, N.; Kado, D.; Kallmes, D.; et al. The Efficacy and Safety of Vertebral Augmentation: A Second ASBMR Task Force Report. J. Bone Miner. Res. 2019, 34, 3–21. [Google Scholar] [CrossRef]
- Anderson, P.A.; Froyshteter, A.B.; Tontz, W.L., Jr. Meta-analysis of vertebral augmentation compared with conservative treatment for osteoporotic spinal fractures. J. Bone Miner. Res. 2013, 28, 372–382. [Google Scholar] [CrossRef]
- De Leacy, R.; Chandra, R.V.; Barr, J.D.; Brook, A.; Cianfoni, A.; Georgy, B.; Jhamb, A.; Lohle, P.N.M.; Manfre, L.; Marcia, S.; et al. The evidentiary basis of vertebral augmentation: A 2019 update. J. NeuroInterventional Surg. 2020, 12, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Edidin, A.A.; Ong, K.L.; Lau, E.; Kurtz, S.M. Morbidity and Mortality After Vertebral Fractures: Comparison of Vertebral Augmentation and Nonoperative Management in the Medicare Population. Spine 2015, 40, 1228–1241. [Google Scholar] [CrossRef]
- Lou, S.; Shi, X.; Zhang, X.; Lyu, H.; Li, Z.; Wang, Y. Percutaneous vertebroplasty versus non-operative treatment for osteoporotic vertebral compression fractures: A meta-analysis of randomized controlled trials. Osteoporos. Int. 2019, 30, 2369–2380. [Google Scholar] [CrossRef]
- Yoo, C.M.; Park, K.B.; Hwang, S.H.; Kang, D.H.; Jung, J.M.; Park, I.S. The analysis of patterns and risk factors of newly developed vertebral compression fractures after percutaneous vertebroplasty. J. Korean Neurosurg. Soc. 2012, 52, 339–345. [Google Scholar] [CrossRef] [PubMed]
- LeBoff, M.S.; Greenspan, S.L.; Insogna, K.L.; Lewiecki, E.M.; Saag, K.G.; Singer, A.J.; Siris, E.S. The clinician’s guide to prevention and treatment of osteoporosis. Osteoporos. Int. 2022, 33, 2049–2102. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.K.; Jee, W.H.; Jung, J.Y.; Choi, M.; Lee, S.Y.; Kim, Y.H.; Ha, K.Y.; Park, C.K. Differentiation of acute osteoporotic and malignant compression fractures of the spine- use of additive qualitative and quantitative axial diffusion-weighted MR imaging to conventional MR imaging at 3.0 T. Radiology 2014, 271, 488–498. [Google Scholar] [CrossRef]
- Mauch, J.T.; Carr, C.M.; Cloft, H.; Diehn, F.E. Review of the Imaging Features of Benign Osteoporotic and Malignant Vertebral Compression Fractures. AJNR Am. J. Neuroradiol. 2018, 39, 1584–1592. [Google Scholar] [CrossRef] [PubMed]
- Ferizi, U.; Besser, H.; Hysi, P.; Jacobs, J.; Rajapakse, C.S.; Chen, C.; Saha, P.K.; Honig, S.; Chang, G. Artificial Intelligence Applied to Osteoporosis: A Performance Comparison of Machine Learning Algorithms in Predicting Fragility Fractures from MRI Data. J. Magn. Reason. Imaging 2019, 49, 1029–1038. [Google Scholar] [CrossRef]
- He, L.; Liu, Z.; Liu, C.; Gao, Z.; Ren, Q.; Lei, L.; Ren, J. Radiomics Based on Lumbar Spine Magnetic Resonance Imaging to Detect Osteoporosis. Acad. Radiol. 2021, 28, e165–e171. [Google Scholar] [CrossRef]
- Chee, C.G.; Yoon, M.A.; Kim, K.W.; Ko, Y.; Ham, S.J.; Cho, Y.C.; Park, B.; Chung, H.W. Combined radiomics-clinical model to predict malignancy of vertebral compression fractures on CT. Eur. Radiol. 2021, 31, 6825–6834. [Google Scholar] [CrossRef]
- Rho, Y.J.; Choe, W.J.; Chun, Y.I. Risk factors predicting the new symptomatic vertebral compression fractures after percutaneous vertebroplasty or kyphoplasty. Eur. Spine J. 2012, 21, 905–911. [Google Scholar] [CrossRef]
- Dieckmeyer, M.; Loffler, M.T.; El Husseini, M.; Sekuboyina, A.; Menze, B.; Sollmann, N.; Wostrack, M.; Zimmer, C.; Baum, T.; Kirschke, J.S. Level-Specific Volumetric BMD Threshold Values for the Prediction of Incident Vertebral Fractures Using Opportunistic QCT: A Case-Control Study. Front. Endocrinol. 2022, 13, 882163. [Google Scholar] [CrossRef]
- Liu, J.; Tang, J.; Xia, B.; Gu, Z.; Yin, H.; Zhang, H.; Yang, H.; Song, B. Novel Radiomics-Clinical Model for the Noninvasive Prediction of New Fractures After Vertebral Augmentation. Acad. Radiol. 2023, 30, 1092–1100. [Google Scholar] [CrossRef]
- Zaworski, C.; Cheah, J.; Koff, M.F.; Breighner, R.; Lin, B.; Harrison, J.; Donnelly, E.; Stein, E.M. MRI-based Texture Analysis of Trabecular Bone for Opportunistic Screening of Skeletal Fragility. J. Clin. Endocrinol. Metab. 2021, 106, 2233–2241. [Google Scholar] [CrossRef] [PubMed]
- Anam, A.K.; Insogna, K. Update on Osteoporosis Screening and Management. Med. Clin. N. Am. 2021, 105, 1117–1134. [Google Scholar] [CrossRef]
- King, A.B.; Fiorentino, D.M. Medicare payment cuts for osteoporosis testing reduced use despite tests’ benefit in reducing fractures. Health Aff. 2011, 30, 2362–2370. [Google Scholar] [CrossRef]
- Schuit, S.C.; Van der Klift, M.; Weel, A.E.; De Laet, C.E.; Burger, H.; Seeman, E.; Hofman, A.; Uitterlinden, A.G.; Van Leeuwen, J.P.; Pols, H.A. Fracture incidence and association with bone mineral density in elderly men and women: The Rotterdam Study. Bone 2004, 34, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Qi, J.; Sun, Y.; Gao, J.; Sun, J.; Wang, G. Bone microarchitecture and metabolism in elderly male patients with signs of intravertebral cleft on MRI. Eur. Radiol. 2022, 32, 3931–3943. [Google Scholar] [CrossRef]
- Hijikata, Y.; Kamitani, T.; Nakahara, M.; Kumamoto, S.; Sakai, T.; Itaya, T.; Yamazaki, H.; Ogawa, Y.; Kusumegi, A.; Inoue, T.; et al. Development and internal validation of a clinical prediction model for acute adjacent vertebral fracture after vertebral augmentation: The AVA score. Bone Jt. J. 2022, 104-B, 97–102. [Google Scholar] [CrossRef]
- Zhu, S.; Su, Q.; Zhang, Y.; Sun, Z.; Yin, P.; Hai, Y. Risk factors of cemented vertebral refracture after percutaneous vertebral augmentation: A systematic review and meta-analysis. Neuroradiology 2020, 62, 1353–1360. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.C.; McGirt, M.J. Vertebral compression fractures: A review of current management and multimodal therapy. J. Multidiscip. Healthc. 2013, 6, 205–214. [Google Scholar] [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics- Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef]
- Jiang, Y.W.; Xu, X.J.; Wang, R.; Chen, C.M. Radiomics analysis based on lumbar spine CT to detect osteoporosis. Eur. Radiol. 2022, 32, 8019–8026. [Google Scholar] [CrossRef]
- Wang, M.; Chen, X.; Cui, W.; Wang, X.; Hu, N.; Tang, H.; Zhang, C.; Shen, J.; Xie, C.; Chen, X. A Computed Tomography-based Radiomics Nomogram for Predicting Osteoporotic Vertebral Fractures: A Longitudinal Study. J. Clin. Endocrinol. Metab. 2023, 108, e283–e294. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Huang, D.; Jiang, Y.; Ma, X.; Zhang, Y.; Chang, R. Correlation of R2* with fat fraction and bone mineral density and its role in quantitative assessment of osteoporosis. Eur. Radiol. 2023, 33, 6001–6008. [Google Scholar] [CrossRef] [PubMed]
- Dieckmeyer, M.; Junker, D.; Ruschke, S.; Mookiah, M.R.K.; Subburaj, K.; Burian, E.; Sollmann, N.; Kirschke, J.S.; Karampinos, D.C.; Baum, T. Vertebral Bone Marrow Heterogeneity Using Texture Analysis of Chemical Shift Encoding-Based MRI: Variations in Age, Sex, and Anatomical Location. Front. Endocrinol. 2020, 11, 555931. [Google Scholar] [CrossRef]
- Bermeo, S.; Gunaratnam, K.; Duque, G. Fat and Bone Interactions. Curr. Osteoporos. Rep. 2014, 12, 235–242. [Google Scholar] [CrossRef]
- Touvier, J.; Winzenrieth, R.; Johansson, H.; Roux, J.P.; Chaintreuil, J.; Toumi, H.; Jennane, R.; Hans, D.; Lespessailles, E. Fracture discrimination by combined bone mineral density (BMD) and microarchitectural texture analysis. Calcif. Tissue Int. 2015, 96, 274–283. [Google Scholar] [CrossRef]
- Liang, W.; Yang, P.; Huang, R.; Xu, L.; Wang, J.; Liu, W.; Zhang, L.; Wan, D.; Huang, Q.; Lu, Y.; et al. A Combined Nomogram Model to Preoperatively Predict Histologic Grade in Pancreatic Neuroendocrine Tumors. Clin. Cancer Res. 2019, 25, 584–594. [Google Scholar] [CrossRef]
- Ji, G.W.; Zhu, F.P.; Xu, Q.; Wang, K.; Wu, M.Y.; Tang, W.W.; Li, X.C.; Wang, X.H. Radiomic Features at Contrast-enhanced CT Predict Recurrence in Early Stage Hepatocellular Carcinoma: A Multi-Institutional Study. Radiology 2020, 294, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Valentinitsch, A.; Trebeschi, S.; Alarcon, E.; Baum, T.; Kaesmacher, J.; Zimmer, C.; Lorenz, C.; Kirschke, J.S. Regional analysis of age-related local bone loss in the spine of a healthy population using 3D voxel-based modeling. Bone 2017, 103, 233–240. [Google Scholar] [CrossRef]
- Khosla, S.; Hofbauer, L.C. Osteoporosis treatment: Recent developments and ongoing challenges. Lancet Diabetes Endocrinol. 2017, 5, 898–907. [Google Scholar] [CrossRef]
- Kanis, J.A.; Harvey, N.C.; McCloskey, E.; Bruyere, O.; Veronese, N.; Lorentzon, M.; Cooper, C.; Rizzoli, R.; Adib, G.; Al-Daghri, N.; et al. Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos. Int. 2020, 31, 1–12. [Google Scholar] [CrossRef]
- Parmar, C.; Barry, J.D.; Hosny, A.; Quackenbush, J.; Aerts, H. Data Analysis Strategies in Medical Imaging. Clin. Cancer Res. 2018, 24, 3492–3499. [Google Scholar] [CrossRef]
- Chen, Y.; Gao, Y.; Li, K.; Zhao, L.; Zhao, J. Vertebrae Identification and Localization Utilizing Fully Convolutional Networks and a Hidden Markov Model. IEEE Trans. Med. Imaging 2020, 39, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Anitha, D.P.; Baum, T.; Kirschke, J.S.; Subburaj, K. Effect of the intervertebral disc on vertebral bone strength prediction: A finite-element study. Spine J. 2020, 20, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shi, T.; Li, W.; Sun, J.; Yao, Z.; Liu, W. Role of paraspinal muscle degeneration in the occurrence and recurrence of osteoporotic vertebral fracture: A meta-analysis. Front. Endocrinol. 2022, 13, 1073013. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Set (n = 153) | Internal Validation Set (n = 66) | External Validation Set (n = 44) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristic | without NVFs | with NVFs | p-Value | without NVFs | with NVFs | p-Value | without NVFs | with NVFs | p-Value |
| Age, yr, median | 74 (66–82) | 79 (72–82) | 0.016 | 73 (65–81) | 75 (69–81) | 0.169 | 73 (70–76) | 77 (71–82) | 0.124 |
| BMI (kg/m2) | 23.09 ± 1.78 | 23.26 ± 1.68 | 0.555 | 23.35 ± 1.72 | 23.24 ± 1.90 | 0.817 | 23.15 ± 1.98 | 23.19 ± 2.08 | 0.958 |
| BMD T-score | −3.16 ± 0.61 | −3.24 ± 0.65 | 0.426 | −3.13 ± 0.54 | −3.20 ± 0.60 | 0.592 | −3.20 ± 0.74 | −3.44 ± 0.54 | 0.278 |
| Sex | |||||||||
| Male | 25 (28.1) | 23 (35.9) | 0.302 | 12 (28.6) | 8 (33.3) | 0.686 | 8 (27.6) | 3 (20.0) | 0.722 |
| Female | 64 (71.9) | 41 (64.1) | 30 (71.4) | 16 (66.7) | 21 (72.4) | 12 (80.0) | |||
| Smoking | |||||||||
| Absent | 70 (78.7) | 53 (82.8) | 0.523 | 33 (78.6) | 20 (83.3) | 0.755 | 26 (89.7) | 12 (80.0) | 0.394 |
| Present | 19 (21.3) | 11 (17.2) | 9 (21.4) | 4 (16.7) | 3 (10.3) | 3 (20.0) | |||
| Surgical procedure | |||||||||
| VP | 57 (64.0) | 46 (71.9) | 0.308 | 25 (59.5) | 17 (70.8) | 0.358 | 20 (69.0) | 11 (73.3) | 0.763 |
| BKP | 32 (36.0) | 18 (28.1) | 17 (40.5) | 7 (29.2) | 9 (31.0) | 4 (26.7) | |||
| IVC | |||||||||
| Absent | 78 (87.6) | 41 (64.1) | 0.001 | 39 (92.9) | 17 (70.8) | 0.029 | 27 (93.1) | 10 (66.7) | 0.036 |
| Present | 11 (12.4) | 23 (35.9) | 3 (7.1) | 7 (29.2) | 2 (6.9) | 5 (33.3) | |||
| Number of treated vertebra | |||||||||
| 1/2/3/4 | 70/16/3/0 | 52/5/4/3 | 0.046 | 35/6/1/0 | 16/4/2/2 | 0.183 | 26/3/0/0 | 12/1/2/0 | 0.235 |
| Location of treated vertebra | |||||||||
| non-TL-Junction | 25 (28.1) | 27 (42.2) | 0.069 | 17 (40.5) | 12 (50) | 0.453 | 9 (31.0) | 5 (33.3) | 0.877 |
| TL-Junction | 64 (71.9) | 37 (57.8) | 25 (59.5) | 12 (50) | 20 (69.0) | 10 (66.7) | |||
| Number of previous VF | |||||||||
| 0/1/2 | 62/20/7 | 24/23/17 | <0.001 | 24/11/7 | 8/8/8 | 0.141 | 19/9/1 | 7/5/3 | 0.192 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Variable | OR (95% CI) | p-Value | OR (95% CI) | p-Value |
| Age | 1.505 (1.072, 2.113) | 0.018 * | 1.235 (0.795, 1.917) | 0.347 |
| Sex | 0.845 (0.614, 1.164) | 0.303 | - | - |
| Smoking | 0.899 (0.648, 1.247) | 0.523 | - | - |
| BMI | 1.102 (0.799, 1.521) | 0.553 | - | - |
| BMD | 0.874 (0.629, 1.212) | 0.419 | - | - |
| Radiomics signature | 6.049 (3.415, 10.714) | <0.001 * | 5.495 (3.035, 9.951) | <0.001 * |
| IVC | 1.775 (1.267, 2.488) | 0.001 * | 1.524 (0.990, 2.346) | 0.056 |
| Surgical procedure | 0.844 (0.609, 1.170) | 0.309 | - | - |
| Number of treated vertebra | 1.160 (0.843, 1.596) | 0.364 | - | - |
| Location of treated vertebra | 0.744 (0.539, 1.025) | 0.071 | - | - |
| Number of previous VF | 2.041 (1.437, 2.900) | <0.001 * | 1.907 (1.200, 3.031) | 0.006 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, Y.; Zhang, W.; Huang, S.; Huang, Q.; Ye, H.; Zeng, Y.; Hua, X.; Cai, J.; Liu, Z.; Liu, Q. Preoperative Prediction of New Vertebral Fractures after Vertebral Augmentation with a Radiomics Nomogram. Diagnostics 2023, 13, 3459. https://doi.org/10.3390/diagnostics13223459
Jiang Y, Zhang W, Huang S, Huang Q, Ye H, Zeng Y, Hua X, Cai J, Liu Z, Liu Q. Preoperative Prediction of New Vertebral Fractures after Vertebral Augmentation with a Radiomics Nomogram. Diagnostics. 2023; 13(22):3459. https://doi.org/10.3390/diagnostics13223459
Chicago/Turabian StyleJiang, Yang, Wei Zhang, Shihao Huang, Qing Huang, Haoyi Ye, Yurong Zeng, Xin Hua, Jinhui Cai, Zhifeng Liu, and Qingyu Liu. 2023. "Preoperative Prediction of New Vertebral Fractures after Vertebral Augmentation with a Radiomics Nomogram" Diagnostics 13, no. 22: 3459. https://doi.org/10.3390/diagnostics13223459
APA StyleJiang, Y., Zhang, W., Huang, S., Huang, Q., Ye, H., Zeng, Y., Hua, X., Cai, J., Liu, Z., & Liu, Q. (2023). Preoperative Prediction of New Vertebral Fractures after Vertebral Augmentation with a Radiomics Nomogram. Diagnostics, 13(22), 3459. https://doi.org/10.3390/diagnostics13223459