
Evaluation of a 3-Item Health Index in Predicting Mortality Risk: A 12-Year Follow-Up Study

 ,
,  , ,
, , 
Abstract
1. Introduction
- How does the newly developed 3-item HI, integrating objective physiological markers such as resting-state sBP SampEn, SART performance, and UGS, compare with frailty measures such as the 32-item FI and FP in predicting all-cause mortality risk?
- To what extent does the 3-item HI compare with the above frailty measures in identifying individuals at heightened risk of specific-cause mortality (e.g., cardio-respiratory)?
2. Materials and Methods
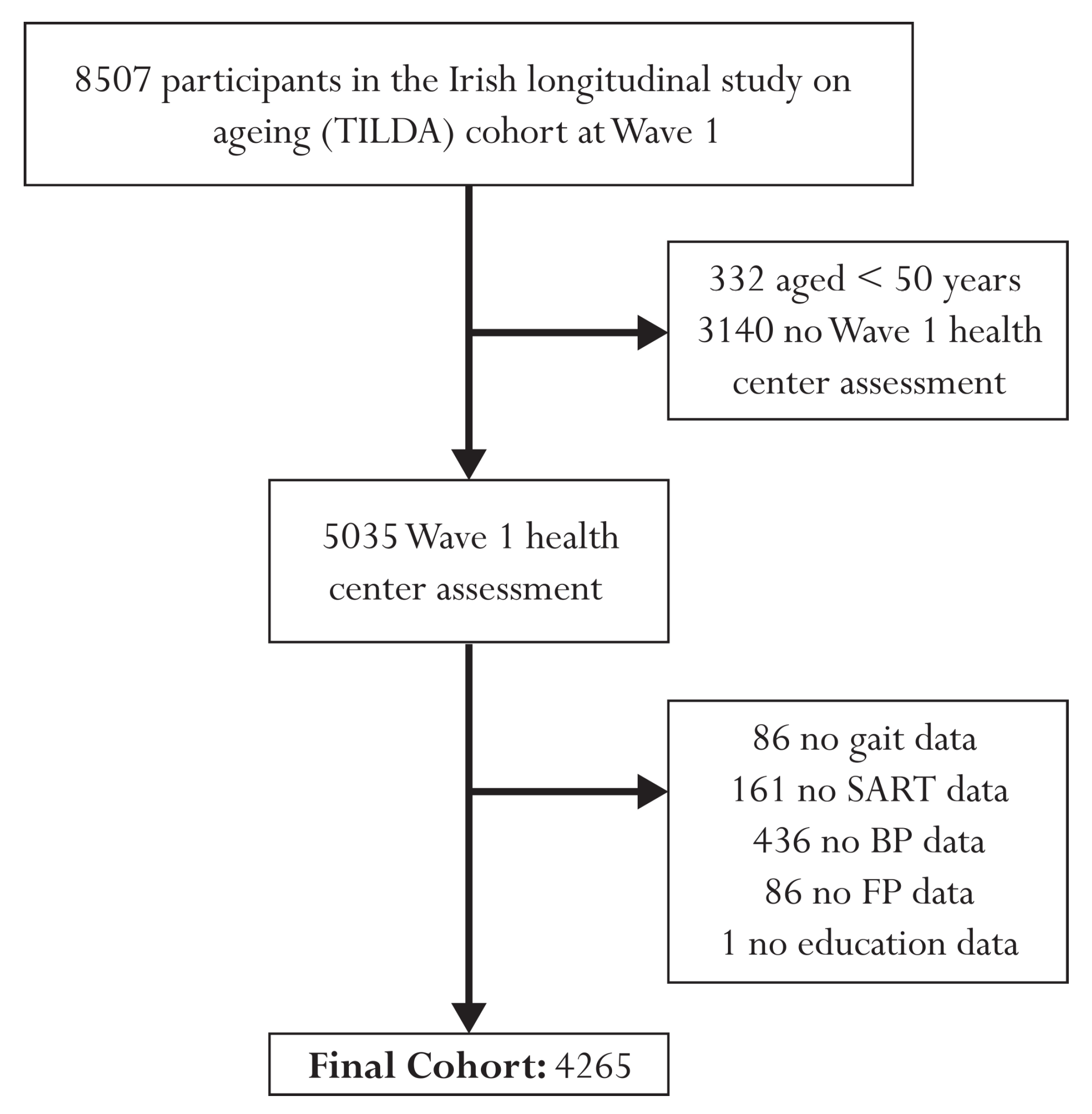
2.1. Design, Setting, and Participants
2.2. Blood Pressure Data
2.3. SART Data
2.4. Gait Data
2.5. Three-Item HI
2.6. Three-Item HI Risk Groups
2.7. Mortality Data
2.8. Frailty Measures
2.9. Covariates
2.10. Statistical Analysis
2.11. MATLAB App and Code
3. Results
Participant Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Three-Item Health Index (HI) Calculation
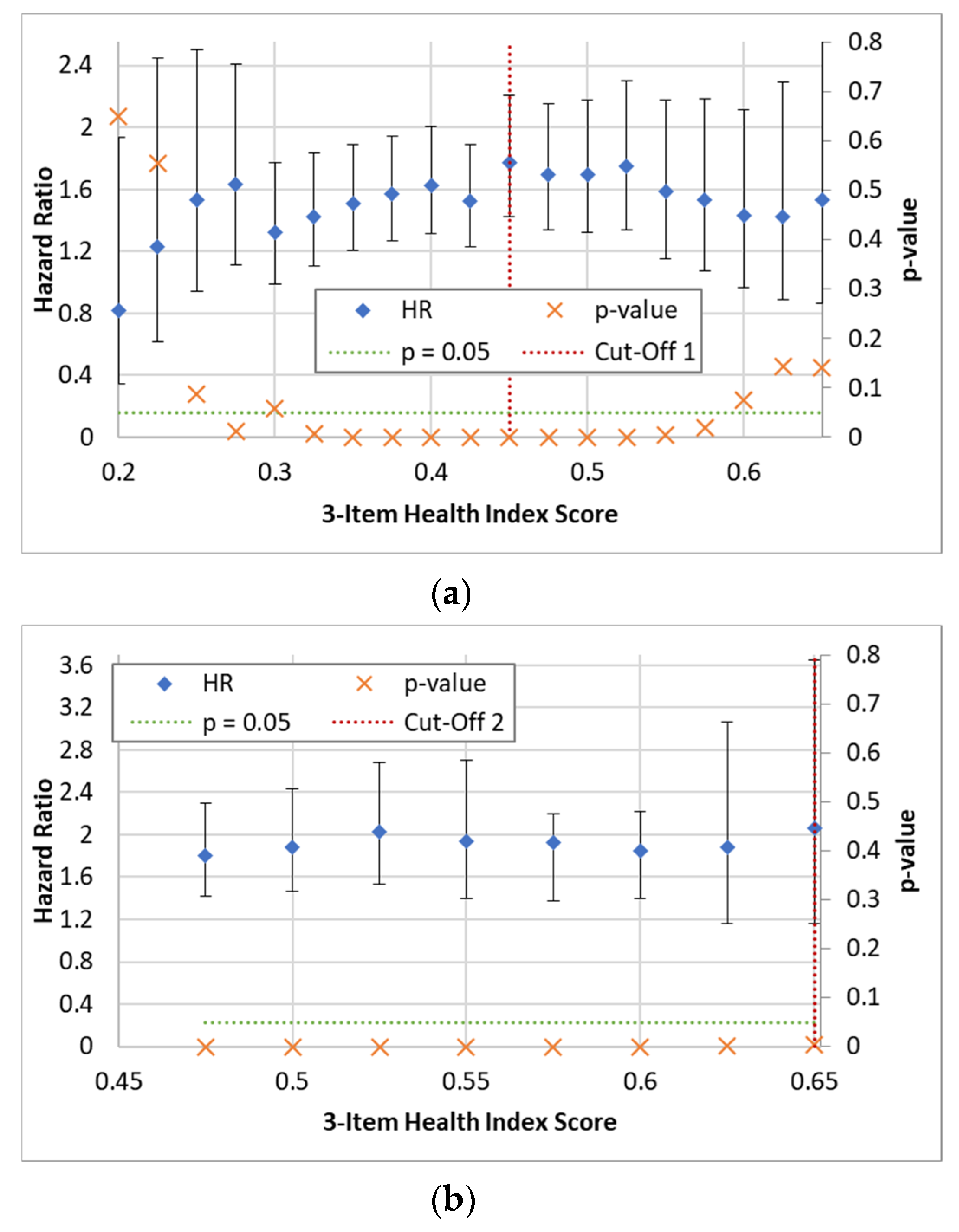
Appendix B. Deriving Cut-Off for 3-Item Health Index

Appendix C. Thirty-Two-Item Frailty Index: Items and Scoring of Individual Items

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Self-Reported Deficit | Scoring |
|---|---|
| Difficulty walking 100 m | 0 = No; 1 = Yes |
| Difficulty rising from a chair | 0 = No; 1 = Yes |
| Difficulty climbing one flight of stairs | 0 = No; 1 = Yes |
| Difficulty stooping, kneeling, or crouching | 0 = No; 1 = Yes |
| Difficulty reaching above shoulder height | 0 = No; 1 = Yes |
| Difficulty pushing/pulling large objects | 0 = No; 1 = Yes |
| Difficulty lifting/carrying weights ≥ 10 pounds (4.5 Kg) | 0 = No; 1 = Yes |
| Difficulty picking up a coin from a table | 0 = No; 1 = Yes |
| Feeling lonely | 0 = None of the time, rarely; 0.5 = Some of the time; 1 = All the time |
| Self-rated physical health | 0 = Excellent, Very good, Good; 0.5 = Fair; 1 = Poor |
| Self-rated vision | 0 = Excellent, Very good, Good; 0.5 = Fair; 1 = Poor |
| Self-rated hearing | 0 = Excellent, Very good, Good; 0.5 = Fair; 1 = Poor |
| Self-rated day-to-day memory | 0 = Excellent, Very good, Good; 0.5 = Fair; 1 = Poor |
| Difficulty following a conversation with one person | 0 = None; 0.5 = Some; 1 = Much/Impossible |
| Daytime sleepiness | 0 = Never, slight chance; 0.5 = Moderate chance; 1 = High chance |
| Polypharmacy | 0 = No; 1 = Yes |
| Knee pain | 0 = No; 1 = Yes |
| Hypertension | 0 = No; 1 = Yes |
| Angina | 0 = No; 1 = Yes |
| Heart attack | 0 = No; 1 = Yes |
| Diabetes | 0 = No; 1 = Yes |
| Stroke or Transient ischemic attack | 0 = No; 1 = Yes |
| High cholesterol | 0 = No; 1 = Yes |
| Irregular heart rhythm | 0 = No; 1 = Yes |
| Other cardiovascular disease | 0 = No; 1 = Yes |
| Cataracts | 0 = No; 1 = Yes |
| Glaucoma or Age-related macular degeneration | 0 = No; 1 = Yes |
| Arthritis | 0 = No; 1 = Yes |
| Osteoporosis | 0 = No; 1 = Yes |
| Cancer | 0 = No; 1 = Yes |
| Varicose ulcer | 0 = No; 1 = Yes |
| Urinary incontinence | 0 = Never, slight chance; 0.5 = Moderate chance; 1 = High chance |
Appendix D. User Guide for MATLAB App
Appendix D.1. Installing the MATLAB App
- Ensure that you have MATLAB installed on your computer (version R2018a or later).
- Clone or download the App repository from the provided GitHub link (https://github.com/SilvinPKnight/3ItemHealthIndexCalculator, accessed on 18 July 2023).
- Extract the contents of the downloaded ZIP file to a desired location on your computer.
- Navigate to the directory where the extracted App files are located and double click the ‘3-Item Health Index Calculator.mlappinstall’ MATLAB App Installer file; this should launch MATLAB and provide the option to install the App.
- To launch the 3-Item Health Index App, navigate to the ‘APPS’ tab in MATLAB, locate and click on the ‘3-Item Health Index Calculator’ button; this should launch the App (shown in Figure A2).

Appendix D.2. Providing Data to the App
Appendix D.2.1. BtB sBP Data
- Matrix 1: Contains the absolute values of systolic blood pressure (sBP; mmHg) at each beat.
- Matrix 2: Contains the corresponding time point values for each beat (milliseconds (ms)).
Appendix D.2.2. SART Data
Appendix D.2.3. Usual Gait Speed Data
Appendix D.3. Additional Instructions
- Before running the App, double-check that the data files are in the appropriate format (see above).
- Follow the on-screen instructions and prompts to load the BtB sBP, SART, and gait speed data into the App.
- The App then performs the necessary calculations and generate the 3-item HI score for each participant based on the provided data. It also provides the risk-stratified groups, coded as follows: 0, Low-Risk; 1, Medium-Risk; and 2, High-Risk.
- The results can be downloaded in .csv format within the App’s interface.
Appendix D.4. Example Data
- “example_sBP_BtB_values.csv”: This file contains the sBP absolute values at each beat in mmHg. Each row represents the data for an individual participant, with the sBP values listed sequentially.
- “example_sBP_BtB_timepoints.csv”: This file contains the corresponding time points for each sBP beat in ms. It enables the synchronization of the sBP values with the respective time intervals. Similar to the previous file, each row corresponds to a participant, and the time point values are listed sequentially.
- “example_SART_data.csv”: This file contains the SART data. Each row represents a participant, and the columns represent the reaction time values in ms, listed sequentially for each of the 217 SART trials.
- “example_gait_speed.csv”: This file contains the usual gait speed data. It is structured as a single column vector, where each value represents the gait speed in centimeters per second (cm/s) for an individual participant.
Appendix D.5. Troubleshooting
Appendix D.6. Conclusions
Appendix E. Demographic Characteristics of Excluded Participants
| Total | Excluded | Included | |
|---|---|---|---|
| N = 8507 | N = 4242 (49.9%) | N = 4265 (50.1%) | |
| Mortality Status (Deceased) (% (n)) | 17% (1432) | 24% (1016) | 10% (416) |
| Age (years) (median (IQR)) | 62.0 (15.0) | 64.0 (19.0) | 60.0 (12.0) |
| Sex (Female) (% (n)) | 56% (4722) | 57% (2411) | 54% (2311) |
| Highest education achieved (% (n)) | |||
| Primary/none | 30% (2520) | 38% (1624) | 21% (896) |
| Secondary | 40% (3430) | 39% (1659) | 42% (1771) |
| Third/higher | 30% (2547) | 22% (949) | 37% (1598) |
| BMI (kg/m2) (median (IQR)) | 28.1 (6.1) | 28.2 (6.5) | 28.1 (6.0) |
| Self-reported diabetic (Yes) (% (n)) | 8% (641) | 9% (381) | 6% (260) |
| No. of Cardiovascular Diseases (% (n)) | |||
| None | 81% (6915) | 80% (3392) | 83% (3523) |
| 1 | 14% (1163) | 14% (606) | 13% (557) |
| 2 or more | 5% (423) | 6% (238) | 4% (185) |
| Antihypertensive Medications (Yes) (% (n)) | 37% (3123) | 41% (1724) | 33% (1399) |
| Smoker (% (n)) | |||
| Never | 44% (3725) | 41% (1750) | 46% (1975) |
| Past | 38% (3212) | 36% (1543) | 39% (1669) |
| Current | 18% (1563) | 22% (942) | 15% (621) |
| CAGE Alcohol Scale (% (n)) | |||
| CAGE < 2 | 73% (6167) | 67% (2825) | 78% (3342) |
| CAGE ≥ 2 | 10% (866) | 7% (317) | 13% (549) |
| No response | 17% (1468) | 26% (1094) | 9% (374) |
| Number of ADL impairments (% (n)) | |||
| 0 | 92% (7792) | 89% (3781) | 94% (4011) |
| 1 | 5% (457) | 6% (269) | 4% (188) |
| 2 or more | 3% (252) | 4% (186) | 2% (66) |
| Number of IADL impairments (% (n)) | |||
| 0 | 93% (7888) | 89% (3773) | 96% (4115) |
| 1 | 4% (318) | 5% (211) | 3% (107) |
| 2 or more | 3% (295) | 6% (252) | 1% (43) |
References
- He, W.; Goodkind, D.; Kowal, P. An Aging World: 2015; U.S. Census Bureau, U.S. Government Publishing Office: Washington, DC, USA, 2016; Volume P95/16-1. [Google Scholar]
- Smith, S.M.; Wallace, E.; O’Dowd, T.; Fortin, M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst. Rev. 2016, 3, Cd006560. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef] [PubMed]
- Rockwood, K.; Stadnyk, K.; MacKnight, C.; McDowell, I.; Hébert, R.; Hogan, D.B. A brief clinical instrument to classify frailty in elderly people. Lancet 1999, 353, 205–206. [Google Scholar] [CrossRef]
- Speechley, M.; Tinetti, M. Falls and Injuries in Frail and Vigorous Community Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 46–52. [Google Scholar] [CrossRef]
- Winograd, C.H. Targeting strategies: An overview of criteria and outcomes. J. Am. Geriatr. Soc. 1991, 39 Pt 2, 25s–35s. [Google Scholar] [CrossRef] [PubMed]
- Turner, G.; Clegg, A. Best practice guidelines for the management of frailty: A British Geriatrics Society, Age UK and Royal College of General Practitioners report. Age Ageing 2014, 43, 744–747. [Google Scholar] [CrossRef]
- Knight, S.P.; Ward, M.; Newman, L.; Davis, J.; Duggan, E.; Kenny, R.A.; Romero-Ortuno, R. Cardiovascular Signal Entropy Predicts All-Cause Mortality: Evidence from The Irish Longitudinal Study on Ageing (TILDA). Entropy 2022, 24, 676. [Google Scholar] [CrossRef]
- Knight, S.P.; Newman, L.; O’Connor, J.D.; Davis, J.; Kenny, R.A.; Romero-Ortuno, R. Associations between Neurocardiovascular Signal Entropy and Physical Frailty. Entropy 2021, 23, 4. [Google Scholar] [CrossRef]
- Knight, S.P.; Duggan, E.; Romero-Ortuno, R. Blood Pressure Signal Entropy as a Novel Marker of Physical Frailty: Results from the FRAILMatics Clinical Cohort. J. Clin. Med. 2023, 12, 53. [Google Scholar] [CrossRef]
- Knight, S.P.; Newman, L.; Scarlett, S.; O’Connor, J.D.; Davis, J.; De Looze, C.; Kenny, R.A.; Romero-Ortuno, R. Associations between Cardiovascular Signal Entropy and Cognitive Performance over Eight Years. Entropy 2021, 23, 1337. [Google Scholar] [CrossRef]
- Knight, S.P.; Davis, J.; Duggan, E.; Kenny, R.A.; Romero-Ortuno, R. Associations between cardiovascular signal entropy and future falls, syncope, and fear of falling. Age Ageing 2022, 51 (Suppl. S3), afac218-148. [Google Scholar] [CrossRef]
- Robertson, I.H.; Manly, T.; Andrade, J.; Baddeley, B.T.; Yiend, J. ‘Oops!’: Performance correlates of everyday attentional failures in traumatic brain injured and normal subjects. Neuropsychologia 1997, 35, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Helton, W.S.; Kern, R.P.; Walker, D.R. Conscious thought and the sustained attention to response task. Conscious. Cogn. 2009, 18, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Paus, T.; Zatorre, R.J.; Hofle, N.; Caramanos, Z.; Gotman, J.; Petrides, M.; Evans, A.C. Time-Related Changes in Neural Systems Underlying Attention and Arousal During the Performance of an Auditory Vigilance Task. J. Cogn. Neurosci. 1997, 9, 392–408. [Google Scholar] [CrossRef]
- Passmore, R. Researches on the Measurement of Human Performance. Br. J. Soc. Med. 1951, 5, 63. [Google Scholar] [CrossRef][Green Version]
- Fassbender, C.; Murphy, K.; Foxe, J.J.; Wylie, G.R.; Javitt, D.C.; Robertson, I.H.; Garavan, H. A topography of executive functions and their interactions revealed by functional magnetic resonance imaging. Brain Res. Cogn. Brain Res. 2004, 20, 132–143. [Google Scholar] [CrossRef]
- O’Connor, C.; Robertson, I.H.; Levine, B. the prosthetics of vigilant attention: Random cuing cuts processing demands. Neuropsychology 2011, 25, 535–543. [Google Scholar] [CrossRef]
- Sturm, W.; De Simone, A.; Krause, B.J.; Specht, K.; Hesselmann, V.; Radermacher, I.; Herzog, H.; Tellmann, L.; Müller-Gärtner, H.W.; Willmes, K. Functional anatomy of intrinsic alertness: Evidencefor a fronto-parietal-thalamic-brainstem network in theright hemisphere. Neuropsychologia 1999, 37, 797–805. [Google Scholar] [CrossRef]
- Coull, J.T. Neural correlates of attention and arousal: Insights from electrophysiology, functional neuroimaging and psychopharmacology. Prog. Neurobiol. 1998, 55, 343–361. [Google Scholar] [CrossRef]
- Helton, W.S. Impulsive responding and the sustained attention to response task. J. Clin. Exp. Neuropsychol. 2009, 31, 39–47. [Google Scholar] [CrossRef]
- O’Halloran, A.M.; Finucane, C.; Savva, G.M.; Robertson, I.H.; Kenny, R.A. Sustained attention and frailty in the older adult population. J. Gerontol. B Psychol. Sci. Soc. Sci. 2014, 69, 147–156. [Google Scholar] [CrossRef]
- O’Halloran, A.M.; Pénard, N.; Galli, A.; Fan, C.W.; Robertson, I.H.; Kenny, R.A. Falls and falls efficacy: The role of sustained attention in older adults. BMC Geriatr. 2011, 11, 85. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Zhao, Y. Associations between functional fitness and walking speed in older adults. Geriatr. Nurs. 2021, 42, 540–543. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, C.; Tringali, V.; Rhodes, R.; Kershisnik, K.; Creditt, D.; Gonzalez-Mejia, J.; Lugo-Vargas, J.; Eby, J. Walking at work: Maximum gait speed is related to work ability in hospital nursing staff. J. Occup. Health 2020, 62, e12171. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Comfortable and maximum walking speed of adults aged 20-79 years: Reference values and determinants. Age Ageing 1997, 26, 15–19. [Google Scholar] [CrossRef]
- Kawajiri, H.; Mishina, H.; Asano, S.; Kono, Y.; Hayashi, H.; Niwa, J.I.; Doyu, M.; Kimura, S.; Yamada, S. Maximum Walking Speed at Discharge Could Be a Prognostic Factor for Vascular Events in Patients with Mild Stroke: A Cohort Study. Arch. Phys. Med. Rehabil. 2019, 100, 230–238. [Google Scholar] [CrossRef]
- O’Donoghue, P.J.; Claffey, P.; Rice, C.; Byrne, L.; Cunningham, C.; Kenny, R.A.; Romero-Ortuno, R. Association between gait speed and the SHARE Frailty Instrument in a Falls and Syncope Clinic. Eur. Geriatr. Med. 2021, 12, 1101–1105. [Google Scholar] [CrossRef]
- James, E.G.; Conatser, P.; Karabulut, M.; Leveille, S.G.; Hausdorff, J.M.; Travison, T.; Bean, J.F. Walking Speed Affects Gait Coordination and Variability Among Older Adults With and Without Mobility Limitations. Arch. Phys. Med. Rehabil. 2020, 101, 1377–1382. [Google Scholar] [CrossRef]
- Samson, M.M.; Crowe, A.; De Vreede, P.L.; Dessens, J.A.; Duursma, S.A.; Verhaar, H.J. Differences in gait parameters at a preferred walking speed in healthy subjects due to age, height and body weight. Aging 2001, 13, 16–21. [Google Scholar] [CrossRef]
- Rockwood, K.; Mitnitski, A. Limits to deficit accumulation in elderly people. Mech. Ageing Dev. 2006, 127, 494–496. [Google Scholar] [CrossRef]
- Matthews, S.; Ward, M.; Nolan, A.; Normand, C.; Kenny, R.A.; May, P. Predicting mortality in The Irish Longitudinal Study on Ageing (TILDA): Development of a four-year index and comparison with international measures. BMC Geriatr. 2022, 22, 510. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, L.C.; Jackson, S.E.; Lee, S.J.; Wardle, J.; Steptoe, A. The development and validation of an index to predict 10-year mortality risk in a longitudinal cohort of older English adults. Age Ageing 2017, 46, 427–432. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Lindquist, K.; Segal, M.R.; Covinsky, K.E. Development and Validation of a Prognostic Index for 4-Year Mortality in Older Adults. JAMA 2006, 295, 801–808. [Google Scholar] [CrossRef]
- Donoghue, O.A.; McGarrigle, C.A.; Foley, M.; Fagan, A.; Meaney, J.; Kenny, R.A. Cohort Profile Update: The Irish Longitudinal Study on Ageing (TILDA). Int. J. Epidemiol. 2018, 47, 1398–1398l. [Google Scholar] [CrossRef] [PubMed]
- Kearney, P.M.; Cronin, H.; O’Regan, C.; Kamiya, Y.; Savva, G.M.; Whelan, B.; Kenny, R. Cohort profile: The Irish Longitudinal Study on Ageing. Int. J. Epidemiol. 2011, 40, 877–884. [Google Scholar] [CrossRef]
- Whelan, B.J. Ransam—Random sample design for Ireland. Econ. Soc. Rev. 1979, 10, 169. [Google Scholar]
- Martínez-Cagigal, V. Sample Entropy. 2018. Available online: https://uk.mathworks.com/matlabcentral/fileexchange/69381-sample-entropy (accessed on 10 January 2020).
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol. Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef]
- Rizzo, R.; Knight, S.P.; Davis, J.R.C.; Newman, L.; Duggan, E.; Kenny, R.A.; Romero-Ortuno, R. SART and Individual Trial Mistake Thresholds: Predictive Model for Mobility Decline. Geriatrics 2021, 6, 85. [Google Scholar] [CrossRef]
- Rizzo, R.; Knight, S.P.; Davis, J.R.C.; Newman, L.; Duggan, E.; Kenny, R.A.; Romero-Ortuno, R. Longitudinal Study on Sustained Attention to Response Task (SART): Clustering Approach for Mobility and Cognitive Decline. Geriatrics 2022, 7, 51. [Google Scholar] [CrossRef]
- Donoghue, O.; Feeney, J.; O’Leary, N.; Kenny, R.A. Baseline Mobility is Not Associated with Decline in Cognitive Function in Healthy Community-Dwelling Older Adults: Findings From The Irish Longitudinal Study on Ageing (TILDA). Am. J. Geriatr. Psychiatry 2018, 26, 438–448. [Google Scholar] [CrossRef]
- Miller, M.E.; Magaziner, J.; Marsh, A.P.; Fielding, R.A.; Gill, T.M.; King, A.C.; Kritchevsky, S.; Manini, T.; McDermott, M.M.; Neiberg, R.; et al. Gait Speed and Mobility Disability: Revisiting Meaningful Levels in Diverse Clinical Populations. J. Am. Geriatr. Soc. 2018, 66, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; May, P.; Briggs, R.; McNicholas, T.; Normand, C.; Kenny, R.A.; Nolan, A. Linking death registration and survey data: Procedures and cohort profile for The Irish Longitudinal Study on Ageing (TILDA) [version 2; peer review: 3 approved]. HRB Open Res. 2020, 3, 43. [Google Scholar] [PubMed]
- Peklar, J.; O’Halloran, A.M.; Maidment, I.D.; Henman, M.C.; Kenny, R.A.; Kos, M. Sedative load and frailty among community-dwelling population aged ≥65 years. J. Am. Med. Dir. Assoc. 2015, 16, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Savva, G.M.; Donoghue, O.A.; Horgan, F.; O’Regan, C.; Cronin, H.; Kenny, R.A. Using timed up-and-go to identify frail members of the older population. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 441–446. [Google Scholar] [CrossRef]
- Donoghue, O.; O’Connell, M.; Kenny, R. Walking to Wellbeing: Physical Activity, Social Participation and Psychological Health in Irish Adults Aged 50 Years or Older. Available online: https://tilda.tcd.ie/publications/reports/pdf/ReportPhysicalActivity.pdf (accessed on 3 October 2020).
- Orme, J.G.; Reis, J.; Herz, E.J. Factorial and discriminant validity of the Center for Epidemiological Studies Depression (CES-D) scale. J. Clin. Psychol. 1986, 42, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Roe, L.; Normand, C.; Wren, M.-A.; Browne, J.; O’halloran, A.M. The impact of frailty on healthcare utilisation in Ireland: Evidence from the Irish longitudinal study on ageing. BMC Geriatr. 2017, 17, 203. [Google Scholar] [CrossRef]
- Searle, S.D.; Mitnitski, A.; Gahbauer, E.A.; Gill, T.M.; Rockwood, K. A standard procedure for creating a frailty index. BMC Geriatr. 2008, 8, 24. [Google Scholar] [CrossRef]
- Peña, F.G.; Theou, O.; Wallace, L.; Brothers, T.D.; Gill, T.M.; Gahbauer, E.A.; Kirkland, S.; Mitnitski, A.; Rockwood, K. Comparison of alternate scoring of variables on the performance of the frailty index. BMC Geriatr. 2014, 14, 25. [Google Scholar] [CrossRef]
- Romero-Ortuno, R. An alternative method for Frailty Index cut-off points to define frailty categories. Eur. Geriatr. Med. 2013, 4, 299–303. [Google Scholar] [CrossRef]
- Ewing, J.A. Detecting alcoholism. The CAGE questionnaire. JAMA 1984, 252, 1905–1907. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Dos-Santos-Silva, I.; Leon, D.A.; Douglas, I.J.; Smeeth, L. Association of BMI with overall and cause-specific mortality: A population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018, 6, 944–953. [Google Scholar] [CrossRef]
- World Health Organization. Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- Xu, J.; Wei, Z.; Wang, X.; Li, X.; Wang, W. The risk of cardiovascular and cerebrovascular disease in overlap syndrome: A meta-analysis. J. Clin. Sleep Med. 2020, 16, 1199–1207. [Google Scholar] [CrossRef]
- Peng, Y.; Zhong, G.-C.; Zhou, X.; Guan, L.; Zhou, L. Frailty and risks of all-cause and cause-specific death in community-dwelling adults: A systematic review and meta-analysis. BMC Geriatr. 2022, 22, 725. [Google Scholar] [CrossRef]
- Romero-Ortuno, R.; Hartley, P.; Kenny, R.A.; O’halloran, A.M. Frail by different measures: A comparison of 8-year mortality in The Irish Longitudinal Study on Ageing (TILDA). Eur. Geriatr. Med. 2022, 13, 279–284. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Volpato, S.; Zuliani, G.; Maggi, S.; Cesari, M.; Lipnicki, D.M.; Smith, L.; Schofield, P.; Firth, J.; et al. Association Between Gait Speed With Mortality, Cardiovascular Disease and Cancer: A Systematic Review and Meta-analysis of Prospective Cohort Studies. J. Am. Med. Dir. Assoc. 2018, 19, 981–988.e7. [Google Scholar] [CrossRef] [PubMed]
- Gale, C.R.; Martyn, C.N.; Cooper, C. Cognitive impairment and mortality in a cohort of elderly people. BMJ 1996, 312, 608–611. [Google Scholar] [CrossRef]
- Smits, C.H.M.; Deeg, D.J.H.; Kriegsman, D.M.W.; Schmand, B. Cognitive Functioning and Health as Determinants of Mortality in an Older Population. Am. J. Epidemiol. 1999, 150, 978–986. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuno, R.; Hartley, P.; Davis, J.; Knight, S.P.; Rizzo, R.; Hernández, B.; Kenny, R.A.; O’Halloran, A.M. Transitions in frailty phenotype states and components over 8 years: Evidence from The Irish Longitudinal Study on Ageing. Arch. Gerontol. Geriatr. 2021, 95, 104401. [Google Scholar] [CrossRef]
- Romero-Ortuno, R.; Hartley, P.; Knight, S.P.; Kenny, R.A.; O’Halloran, A.M. Frailty index transitions over eight years were frequent in The Irish Longitudinal Study on Ageing [version 1; peer review: 3 approved, 1 approved with reservations]. HRB Open Res. 2021, 4, 63. [Google Scholar] [CrossRef]
- Kearney, P.M.; Cronin, H.; O’Regan, C.; Kamiya, Y.; Whelan, B.J.; Kenny, R.A. Comparison of centre and home-based health assessments: Early experience from the Irish Longitudinal Study on Ageing (TILDA). Age Ageing 2010, 40, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed]
- White, D.K.; Neogi, T.; Nevitt, M.C.; Peloquin, C.E.; Zhu, Y.; Boudreau, R.M.; Cauley, J.A.; Ferrucci, L.; Harris, T.B.; Satterfield, S.M.; et al. Trajectories of gait speed predict mortality in well-functioning older adults: The Health, Aging and Body Composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 456–464. [Google Scholar] [CrossRef] [PubMed]




| Total | Low-Risk | Medium-Risk | High-Risk | |
|---|---|---|---|---|
| N = 4265 | N = 3604 | N = 625 | N = 36 | |
| Mortality Status (Deceased) (% (n)) | 10% (416) | 7% (265) | 22% (138) | 36% (13) |
| sBP SampEn (mean (SD)) | 0.640 (0.178) | 0.614 (0.166) | 0.782 (0.164) | 0.843 (0.184) |
| Usual Gait Speed (cm/s) (median (IQR)) | 136.7 (25.8) | 139.6 (24.0) | 118.9 (26.6) | 105.1 (32.2) |
| No. SART Bad Performances (median (IQR)) | 20 (4.0) | 2.0 (3.0) | 8.0 (7.0) | 19.5 (3.5) |
| 3-item Health Index Score (median (IQR)) | 0.345 (0.116) | 0.329 (0.094) | 0.499 (0.069) | 0.681 (0.055) |
| 32-item Frailty Index (% (n)) | ||||
| Non-frail | 60% (2553) | 64% (2313) | 36% (228) | 33% (12) |
| Pre-frail | 30% (1281) | 29% (1034) | 38% (236) | 31% (11) |
| Frail | 10% (431) | 7% (257) | 26% (161) | 36% (13) |
| Fried Frailty Phenotype (% (n)) | ||||
| Non-frail | 73% (3123) | 77% (2772) | 55% (341) | 28% (10) |
| Pre-frail | 26% (1088) | 23% (811) | 41% (258) | 53% (19) |
| Frail | 1% (54) | 1% (21) | 4% (26) | 19% (7) |
| Age (years) (median (IQR)) | 60.0 (12.0) | 59.0 (12.0) | 67.0 (13.0) | 73.5 (10.5) |
| Sex (Female) (% (n)) | 54% (2311) | 52% (1891) | 63% (392) | 78% (28) |
| Highest education achieved (% (n)) | ||||
| Primary/none | 21% (896) | 17% (626) | 40% (250) | 56% (20) |
| Secondary | 42% (1771) | 42% (1522) | 38% (238) | 31% (11) |
| Third/higher | 37% (1598) | 40% (1456) | 22% (137) | 14% (5) |
| BMI (kg/m2) (median (IQR)) | 28.1 (6.0) | 27.8 (5.7) | 29.9 (6.2) | 29.3 (5.3) |
| Self-reported diabetic (% (n)) | 6% (260) | 5% (178) | 12% (76) | 17% (6) |
| No. of Cardiovascular Diseases (% (n)) | ||||
| None | 83% (3523) | 84% (3031) | 75% (467) | 69% (25) |
| 1 | 13% (557) | 12% (440) | 17% (109) | 22% (8) |
| 2 or more | 4% (185) | 4% (133) | 8% (49) | 8% (3) |
| Antihypertensive Medications (Yes) (% (n)) | 33% (1399) | 30% (1072) | 49% (306) | 58% (21) |
| Smoker (% (n)) | ||||
| Never | 46% (1975) | 47% (1694) | 42% (262) | 53% (19) |
| Past | 39% (1669) | 39% (1405) | 40% (252) | 33% (12) |
| Current | 15% (621) | 14% (505) | 18% (111) | 14% (5) |
| CAGE Alcohol Scale (% (n)) | ||||
| CAGE < 2 | 78% (3342) | 78% (2820) | 79% (496) | 72% (26) |
| CAGE ≥ 2 | 13% (549) | 14% (487) | 10% (60) | 6% (2) |
| No response | 9% (374) | 8% (297) | 11% (69) | 22% (8) |
| Number of ADL impairments (% (n)) | ||||
| 0 | 94% (4011) | 95% (2922) | 91% (1060) | 81% (29) |
| 1 | 4% (188) | 4% (110) | 6% (74) | 11% (4) |
| 2 or more | 2% (66) | 1% (31) | 3% (32) | 8% (3) |
| Number of IADL impairments (% (n)) | ||||
| 0 | 96% (4115) | 98% (2991) | 94% (1094) | 83% (30) |
| 1 | 3% (107) | 2% (52) | 4% (51) | 11% (4) |
| 2 or more | 1% (43) | 1% (20) | 2% (21) | 6% (2) |
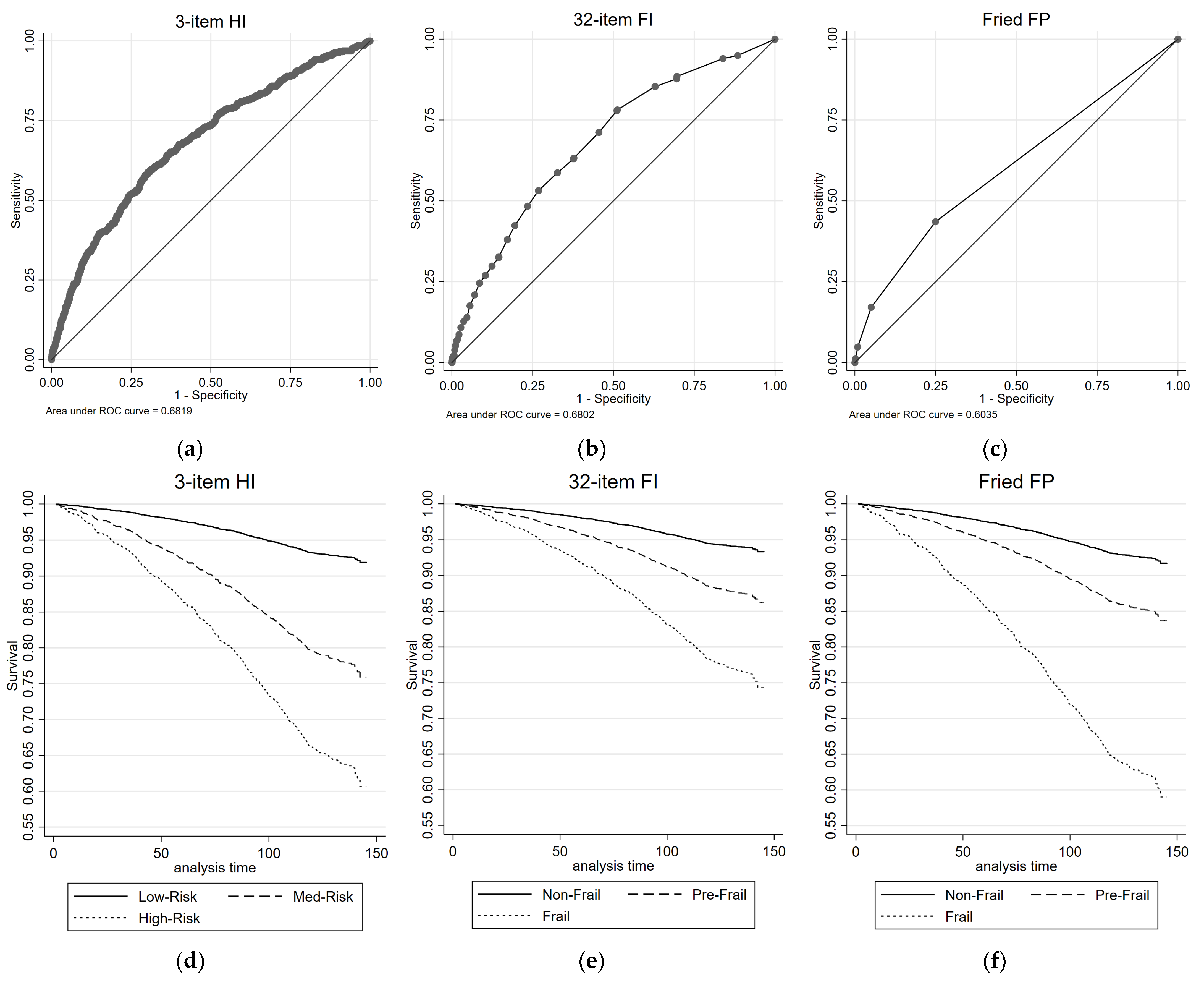
| Mortality Prediction (All-Cause, 416 Deaths) | ||||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| Measure | N | HR (95% CIs) | p-Value | HR (95% CIs) | p-Value | AUC |
| 3-item Health Index | 0.68 | |||||
| Low-Risk (ref) | 3604 | 1 | 1 | |||
| Medium-Risk | 625 | 3.27 (2.66, 4.01) | <0.001 | 1.75 (1.40, 2.19) | <0.001 | |
| High-Risk | 36 | 5.91 (3.38, 10.34) | <0.001 | 2.06 (1.16, 3.65) | 0.013 | |
| 32-item Frailty Index | 0.68 | |||||
| Non-Frail (ref) | 2553 | 1 | 1 | |||
| Pre-Frail | 1281 | 2.15 (1.72, 2.69) | <0.001 | 1.19 (0.92, 1.54) | 0.182 | |
| Frail | 431 | 4.31 (3.36, 5.53) | <0.001 | 1.68 (1.22, 2.32) | 0.001 | |
| Fried Frailty Phenotype | 0.60 | |||||
| Non-Frail (ref) | 3123 | 1 | 1 | |||
| Pre-Frail | 1088 | 2.06 (1.69, 2.52) | <0.001 | 1.34 (1.08, 1.65) | 0.007 | |
| Frail | 54 | 6.11 (3.84, 9.71) | <0.001 | 2.26 (1.42, 3.60) | 0.001 | |
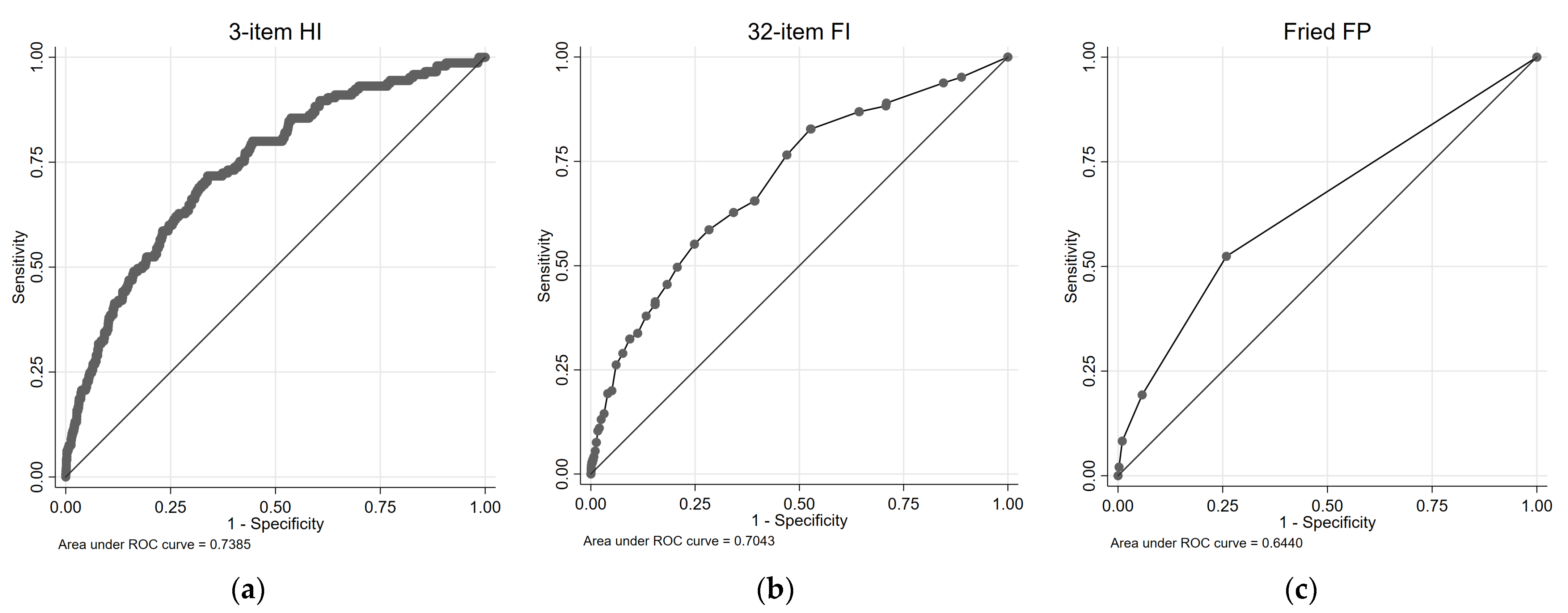
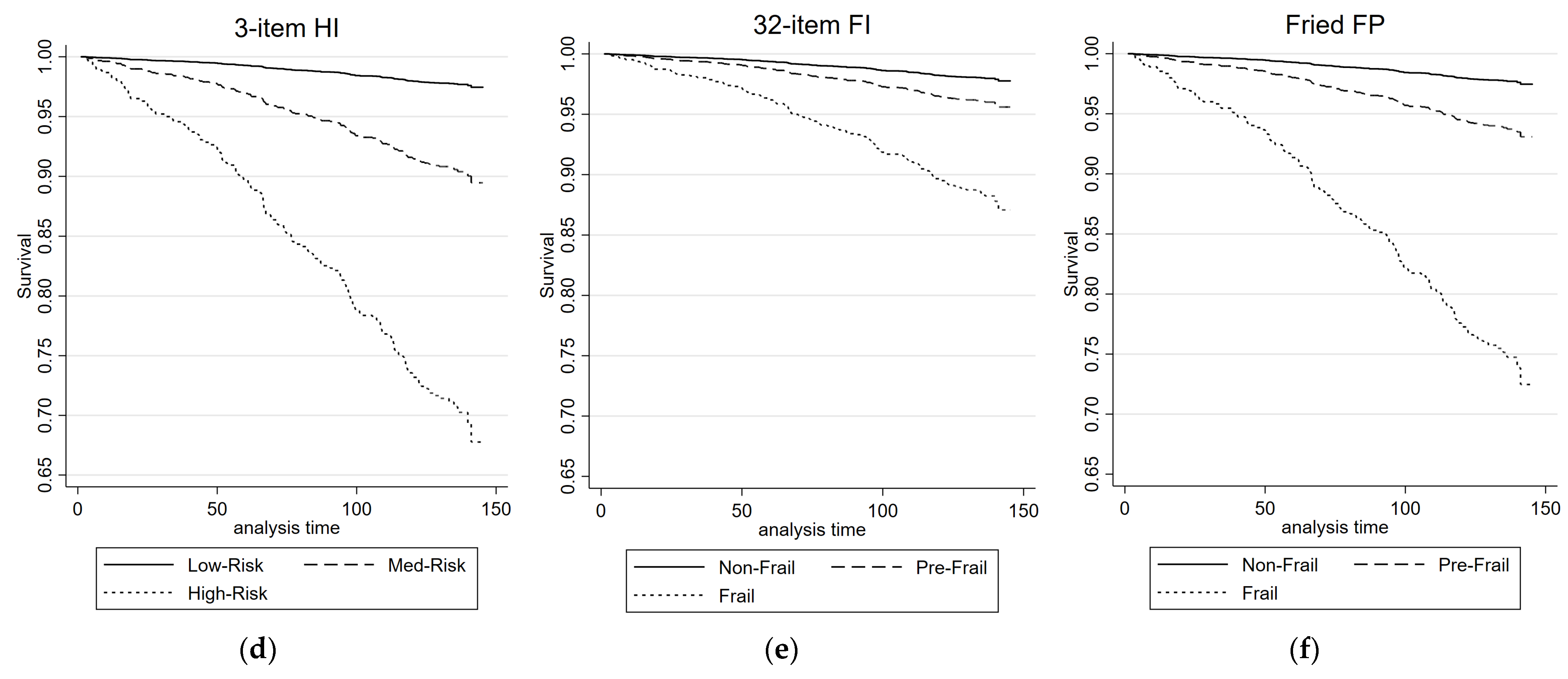
| Mortality Prediction (Cardiovascular and Respiratory, 145 Deaths) | ||||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| Measure | N | HR (95% CIs) | p-Value | HR (95% CIs) | p-Value | AUC |
| 3-item Health Index | 0.74 | |||||
| Low-Risk (ref) | 3604 | 1 | 1 | |||
| Medium-Risk | 625 | 4.32 (3.06, 6.09) | <0.001 | 2.17 (1.47, 3.19) | <0.001 | |
| High-Risk | 36 | 15.10 (7.79, 29.28) | <0.001 | 5.61 (2.84, 11.05) | <0.001 | |
| 32-item Frailty Index | 0.70 | |||||
| Non-Frail (ref) | 2553 | 1 | 1 | |||
| Pre-Frail | 1281 | 1.99 (1.34, 2.96) | 0.001 | 0.91 (0.58, 1.43) | 0.690 | |
| Frail | 431 | 6.12 (4.11, 9.11) | <0.001 | 1.73 (1.02, 2.92) | 0.041 | |
| Fried Frailty Phenotype | 0.64 | |||||
| Non-Frail (ref) | 3123 | 1 | 1 | |||
| Pre-Frail | 1088 | 2.79 (1.99, 3.91) | <0.001 | 1.72 (1.21, 2.46) | 0.003 | |
| Frail | 54 | 12.53 (6.76, 23.26) | <0.001 | 3.31 (1.69, 6.49) | 0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knight, S.P.; Ward, M.; Duggan, E.; Xue, F.; Kenny, R.A.; Romero-Ortuno, R. Evaluation of a 3-Item Health Index in Predicting Mortality Risk: A 12-Year Follow-Up Study. Diagnostics 2023, 13, 2801. https://doi.org/10.3390/diagnostics13172801
Knight SP, Ward M, Duggan E, Xue F, Kenny RA, Romero-Ortuno R. Evaluation of a 3-Item Health Index in Predicting Mortality Risk: A 12-Year Follow-Up Study. Diagnostics. 2023; 13(17):2801. https://doi.org/10.3390/diagnostics13172801
Chicago/Turabian StyleKnight, Silvin P., Mark Ward, Eoin Duggan, Feng Xue, Rose Anne Kenny, and Roman Romero-Ortuno. 2023. "Evaluation of a 3-Item Health Index in Predicting Mortality Risk: A 12-Year Follow-Up Study" Diagnostics 13, no. 17: 2801. https://doi.org/10.3390/diagnostics13172801
APA StyleKnight, S. P., Ward, M., Duggan, E., Xue, F., Kenny, R. A., & Romero-Ortuno, R. (2023). Evaluation of a 3-Item Health Index in Predicting Mortality Risk: A 12-Year Follow-Up Study. Diagnostics, 13(17), 2801. https://doi.org/10.3390/diagnostics13172801