
Ultra-High Frequency UltraSound (UHFUS) Assessment of Barrier Function in Moderate-to-Severe Atopic Dermatitis during Dupilumab Treatment

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iannone, M.; Tonini, G.; Janowska, A.; Dini, V.; Romanelli, M. Definition of treatment goals in terms of clinician-reported disease severity and patient-reported outcomes in moderate-to-severe adult atopic dermatitis: A systematic review. Curr. Med. Res. Opin. 2021, 37, 1295–1301. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Robertson, C.; Stewart, A.; Aït-Khaled, N.; Anabwani, G.; Anderson, R.; Asher, I.; Beasley, R.; Björkstén, B.; Burr, M.; et al. Worldwide variations in the prevalence of symptoms of atopic eczema in the International Study of Asthma and Allergies in Childhood. J. Allergy Clin. Immunol. 1999, 103, 125. [Google Scholar] [CrossRef] [PubMed]
- Odhiambo, J.A.; Williams, H.C.; Clayton, T.O.; Robertson, C.F.; Asher, M.I.; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J. Allergy Clin. Immunol. 2009, 124, 1251. [Google Scholar] [CrossRef] [PubMed]
- Sacotte, R.; Silverberg, J.I. Epidemiology of adult atopic dermatitis. Clin. Dermatol. 2018, 36, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef]
- Calzavara Pinton, P.; Cristaudo, A.; Foti, C.; Canonica, G.W.; Balato, N.; Costanzo, A.; DEPità, O.; DESimone, C.; Patruno, C.; Pellacani, G.; et al. Diagnosis and management of moderate to severe adult atopic dermatitis: A Consensus by the Italian Society of Dermatology and Venereology (SIDeMaST), the Italian Association of Hospital Dermatologists (ADOI), the Italian Society of Allergy, Asthma and Clinical Immunology (SIAAIC), and the Italian Society of Allergological, Environmental and Occupational Dermatology (SIDAPA). G. Ital. Dermatol. Venereol. 2018, 153, 133–145. [Google Scholar]
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Primers. 2018, 4, 1. [Google Scholar] [CrossRef]
- Drucker, A.M.; Wang, A.R.; Li, W.Q.; Sevetson, E.; Block, J.K.; Qureshi, A.A. The Burden of Atopic Dermatitis: Summary of a Report for the National Eczema Association. J. Investig. Dermatol. 2017, 137, 26–30. [Google Scholar] [CrossRef]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A.; et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: Part I. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 657–682, Erratum in J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1436. [Google Scholar] [CrossRef]
- Wollenberg, A.; Barbarot, S.; Bieber, T.; Christen-Zaech, S.; Deleuran, M.; Fink-Wagner, A.; Gieler, U.; Girolomoni, G.; Lau, S.; Muraro, A.; et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: Part II. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 850–878. [Google Scholar] [CrossRef]
- Harb, H.; Chatila, T.A. Mechanisms of Dupilumab. Clin. Exp. Allergy 2020, 50, 5–14. [Google Scholar] [CrossRef]
- McKenzie, A.N.; Culpepper, J.A.; De Waal Malefyt, R.; Briere, F.; Punnonen, J.; Aversa, G.; Sato, A.; Dang, W.; Cocks, B.G.; Menon, S. Interleukin 13, a T-cell-derived cytokine that regulates human monocyte and B-cell function. Proc. Natl. Acad. Sci. USA 1993, 90, 3735–3739. [Google Scholar] [CrossRef] [PubMed]
- Bao, L.; Zhang, H.; Chan, L.S. The involvement of the JAK-STAT signaling pathway in chronic inflammatory skin disease atopic dermatitis. Jak-Stat 2013, 2, e24137. [Google Scholar] [CrossRef]
- Esche, C.; De Benedetto, A.; Beck, L.A. Keratinocytes in atopic dermatitis: Inflammatory signals. Curr. Allergy Asthma Rep. 2004, 4, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Vanbever, R.; Fouchard, D.; Jadoul, A.; De Morre, N.; Préat, V.; Marty, J.P. In vivo noninvasive evaluation of hairless rat skin after high-voltage pulse exposure. Skin Pharmacol. Appl. Skin Physiol. 1998, 11, 23–34. [Google Scholar] [CrossRef]
- Kelleher, M.; Dunn-Galvin, A.; Hourihane, J.O.; Murray, D.; Campbell, L.E.; McLean, W.H.I.; Irvine, A.D. Skin barrier dysfunction measured by transepidermal water loss at 2 days and 2 months predates and predicts atopic dermatitis at 1 year. J. Allergy Clin. Immunol. 2015, 135, 930–935.e1. [Google Scholar] [CrossRef] [PubMed]
- Osseiran, S.; Cruz, J.D.; Jeong, S.; Wang, H.; Fthenakis, C.; Evans, C.L. Characterizing stratum corneum structure, barrier function, and chemical content of human skin with coherent Raman scattering imaging. Biomed. Opt. Express 2018, 9, 6425–6443. [Google Scholar] [CrossRef]
- Werner, Y. The water content of the stratum corneum in patients with atopic dermatitis. Measurement with the Corneometer CM 420. Acta Derm.-Venereol. 1986, 66, 281–284. [Google Scholar]
- Kircik, L.H. Transepidermal water loss (TEWL) and corneometry with hydrogel vehicle in the treatment of atopic dermatitis: A randomized, investigator-blind pilot study. J. Drugs Dermatol. 2012, 11, 180–184. [Google Scholar]
- Polańska, A.; Dańczak-Pazdrowska, A.; Jałowska, M.; Żaba, R.; Adamski, Z. Current applications of high-frequency ultrasonography in dermatology. Postepy Dermatol. Alergol. 2017, 34, 535–542. [Google Scholar] [CrossRef]
- Polańska, A.; Dańczak-Pazdrowska, A.; Silny, W.; Woźniak, A.; Maksin, K.; Jenerowicz, D.; Janicka-Jedyńska, M. Comparison between high-frequency ultrasonography (Dermascan C, version 3) and histopathology in atopic dermatitis. Skin Res. Technol. 2013, 19, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Izzetti, R.; Vitali, S.; Aringhieri, G.; Nisi, M.; Oranges, T.; Dini, V.; Ferro, F.; Baldini, C.; Romanelli, M.; Caramella, D.; et al. Ultra-High Frequency Ultrasound, A Promising Diagnostic Technique: Review of the Literature and Single-Center Experience. Can. Assoc. Radiol. J. 2021, 72, 418–431. [Google Scholar] [CrossRef]
- Sabău, M.; Boca, A.N.; Ilies, R.F.; Tătaru, A. Potential of high-frequency ultrasonography in the management of atopic dermatitis. Exp. Ther. Med. 2019, 17, 1073–1077. [Google Scholar] [CrossRef] [PubMed]
- Simpson, E.L.; Bruin-Weller, M.; Flohr, C.; Ardern-Jones, M.R.; Barbarot, S.; Deleuran, M.; Bieber, T.; Vestergaard, C.; Brown, S.J.; Cork, M.J.; et al. When does atopic dermatitis warrant systemic therapy? Recommendations from an expert panel of the International Eczema Council. J. Am. Acad. Dermatol. 2017, 77, 623. [Google Scholar] [CrossRef]
- Roekevisch, E.; Spuls, P.I.; Kuester, D.; Limpens, J.; Schmitt, J. Efficacy and safety of systemic treatments for moderate-to-severe atopic dermatitis: A systematic review. J. Allergy Clin Immunol. 2014, 133, 429. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; von Kobyletzki, L.; Svensson, A.; Apfelbacher, C. Efficacy and tolerability of proactive treatment with topical corticosteroids and calcineurin inhibitors for atopic eczema: Systematic review and meta-analysis of randomized controlled trials. Br. J. Dermatol. 2011, 164, 415. [Google Scholar] [CrossRef]
- Blauvelt, A.; de Bruin-Weller, M.; Gooderham, M.; Cather, J.C.; Weisman, J.; Pariser, D.; Simpson, E.L.; Papp, K.A.; Hong, H.C.H.; Rubel, D.; et al. Long-term management of moderate-to-severe atopic dermatitis with dupilumab and concomitant topical corticosteroids (LIBERTY AD CHRONOS): A 1-year, randomised, double-blinded, placebo-controlled, phase 3 trial. Lancet 2017, 389, 2287. [Google Scholar] [CrossRef]
- Sawangjit, R.; Dilokthornsakul, P.; Lloyd-Lavery, A.; Lai, N.M.; Dellavalle, R.; Chaiyakunapruk, N. Systemic treatments for eczema: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 9, CD013206. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Bissonnette, R.; Ungar, B.; Suárez-Fariñas, M.; Ardeleanu, M.; Esaki, H.; Suprun, M.; Estrada, Y.; Xu, H.; Peng, X.; et al. Dupilumab progressively improves systemic and cutaneous abnormalities in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2019, 143, 155–172. [Google Scholar] [CrossRef]
- Hamilton, J.D.; Suárez-Fariñas, M.; Dhingra, N.; Cardinale, I.; Li, X.; Kostic, A.; Ming, J.E.; Radin, A.R.; Krueger, J.G.; Graham, N.; et al. Dupilumab improves the molecular signature in skin of patients with moderate-to-severe atopic dermatitis. J. Allergy Clin. Immunol. 2014, 134, 1293–1300. [Google Scholar] [CrossRef]
- Mihm, M.C., Jr.; Soter, N.A.; Dvorak, H.F.; Austen, K.F. The structure of normal skin and the morphology of atopic eczema. J. Investig. Dermatol. 1976, 67, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Fariñas, M.; Tintle, S.J.; Shemer, A.; Chiricozzi, A.; Nograles, K.; Cardinale, I.; Duan, S.; Bowcock, A.M.; Krueger, J.G.; Guttman-Yassky, E. Nonlesional atopic dermatitis skin is characterized by broad terminal differentiation defects and variable immune abnormalities. J. Allergy Clin. Immunol. 2011, 127, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Fornage, B.D.; McGavran, M.H.; Duvic, M.; Waldron, C.A. Imaging of the skin with 20-MHz US. Radiology 1993, 189, 69–76. [Google Scholar] [CrossRef]
- Gutierrez, M.; Wortsman, X.; Filippucci, E.; De Angelis, R.; Filosa, G.; Grassi, W. High-frequency sonography in the evaluation of psoriasis: Nail and skin involvement. J. Ultrasound Med. 2009, 28, 1569–1574. [Google Scholar] [CrossRef]
- Marina, M.E.; Botar Jid, C.; Roman, I.I.; Mihu, C.M.; Tătaru, A.D. Ultrasonography in psoriatic disease. Med. Ultrason. 2015, 17, 377–382. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yazdanparast, T.; Yazdani, K.; Humbert, P.; Khatami, A.; Nasrollahi, S.A.; Firouzabadi, L.I.; Firooz, A. Biophysical Measurements and Ultrasonographic Findings in Chronic Dermatitis in Comparison with Uninvolved Skin. Indian J. Dermatol. 2019, 64, 90–96. [Google Scholar]
- Polańska, A.; Jenerowicz, D.; Paszyńska, E.; Żaba, R.; Adamski, Z.; Dańczak-Pazdrowska, A. High-Frequency Ultrasonography-Possibilities and Perspectives of the Use of 20 MHz in Teledermatology. Front. Med. 2021, 8, 619965. [Google Scholar] [CrossRef] [PubMed]
- Dańczak-Pazdrowska, A.; Polańska, A.; Silny, W.; Sadowska, A.; Osmola-Mańkowska, A.; Czarnecka-Operacz, M.; Zaba, R.; Jenerowicz, D. Seemingly healthy skin in atopic dermatitis: Observations with the use of high-frequency ultrasonography, preliminary study. Skin Res. Technol. 2012, 18, 162–167. [Google Scholar] [CrossRef]
- Osmola-Mańkowska, A.; Polańska, A.; Silny, W.; Żaba, R.; Adamski, Z.; Dańczak-Pazdrowska, A. Topical tacrolimus vs medium-dose ultraviolet A1 phototherapy in the treatment of atopic dermatitis-A preliminary study in relation to parameters of the epidermal barrier function and high-frequency ultrasonography. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 3927–3934. [Google Scholar]
- Jasaitiene, D.; Valiukeviciene, S.; Linkeviciute, G.; Raisutis, R.; Jasiuniene, E.; Kazys, R. Principles of high-frequency ultrasonography for investigation of skin pathology. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 375–382. [Google Scholar] [CrossRef]
- Lee, H.J.; Hong, Y.J.; Kim, M. Angiogenesis in Chronic Inflammatory Skin Disorders. Int. J. Mol. Sci. 2021, 22, 12035. [Google Scholar] [CrossRef] [PubMed]
- Genovese, A.; Detoraki, A.; Granata, F.; Galdiero, M.R.; Spadaro, G.; Marone, G. Angiogenesis, lymphangiogenesis and atopic dermatitis. Chem. Immunol. Allergy 2012, 96, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Agenzia Italiana del Farmaco. DETERMINA 24 Novembre 2020. Regime di Rimborsabilita’ e Prezzo a Seguito di Nuove Indicazioni Terapeutiche e Riclassificazione del Medicinale per uso Umano «Dupixent», ai sensi dell;art. 8, Comma 10, della Legge 24 Dicembre 1993, n. 537. (Determina n. DG/1204/2020). (20A06599). Available online: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2020-12-09&atto.codiceRedazionale=20A06601&elenco30giorni=true (accessed on 24 November 2020).
- Fargnoli, M.C.; Esposito, M.; Ferrucci, S.; Girolomoni, G.; Offidani, A.; Patrizi, A.; Peris, K.; Costanzo, A.; Malara, G.; Pellacani, G.; et al. Real-life experience on effectiveness and safety of dupilumab in adult patients with moderate-to-severe atopic dermatitis. J. Dermatol. Treat. 2021, 32, 507–513. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Time Line | t0 | t1 | t2 | ||||
|---|---|---|---|---|---|---|---|
| PARAMETERS | Mean | SD | Mean | SD | Mean | SD | p-Value |
| EASI | 28.425 | 12.339 | 9.875 | 9.360 | 8.033 | 8.815 | <0.001 |
| IGA | 3.250 | 0.452 | 1.833 | 0.718 | 1.750 | 0.866 | <0.001 |
| DLQI | 12,750 | 6.426 | 3.667 | 3.284 | 3.417 | 3.942 | 0.001 |
| Sleep-NRS | 5.750 | 3.019 | 1.167 | 1.946 | 2.417 | 2.778 | 0.002 |
| Itch-NRS | 8.500 | 1.382 | 3.250 | 2.340 | 3.333 | 2.309 | <0.001 |
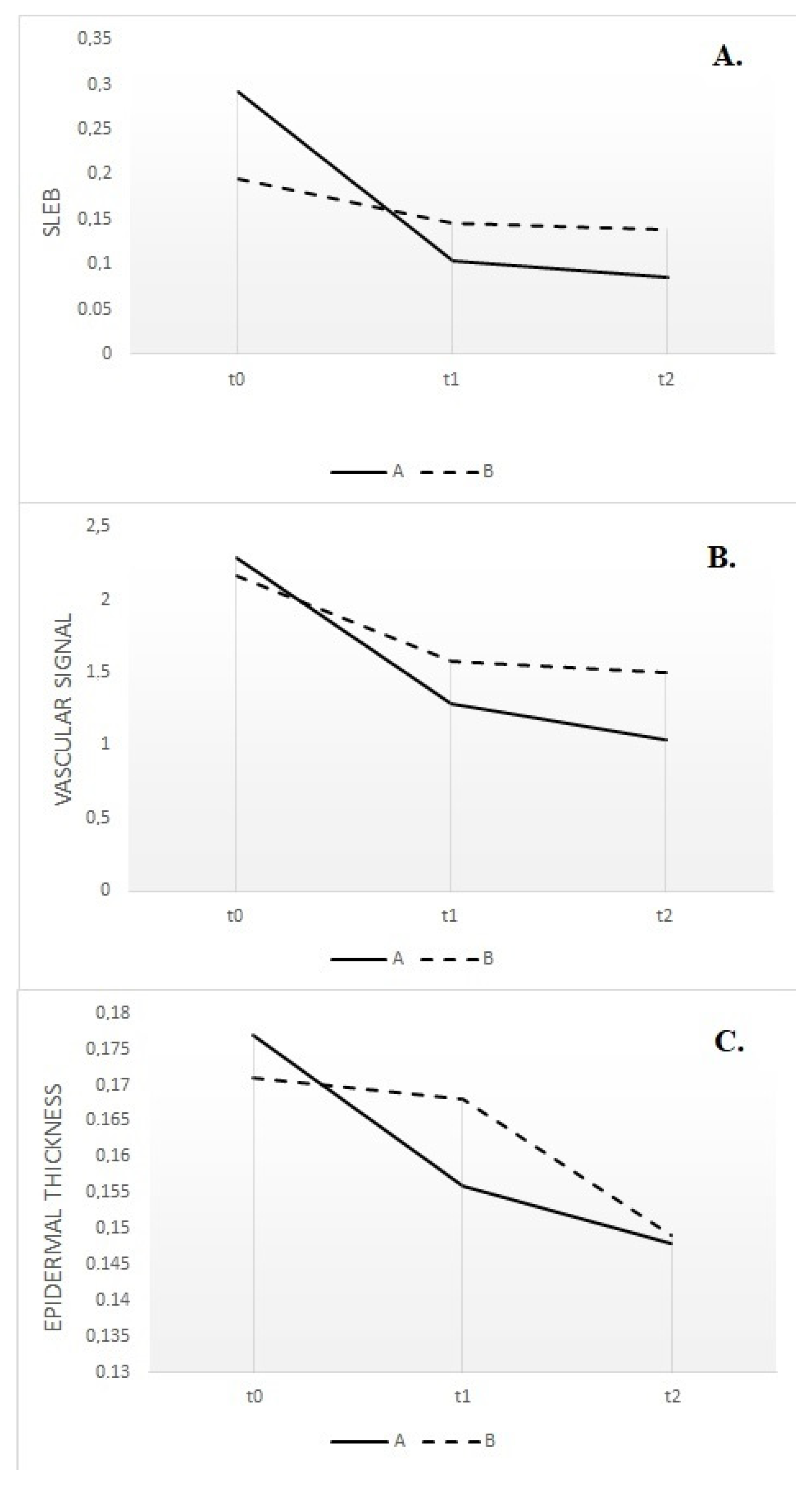
| Lesional skin SLEB (mm) | 0.291 | 0.126 | 0.103 | 0.072 | 0.085 | 0.100 | <0.001 |
| Non-lesional skin SLEB (mm) | 0.053 | 0.040 | 0.057 | 0.080 | 0.030 | 0.035 | ns |
| Lesional skin epidermic thickness (mm) | 0.177 | 0.030 | 0.156 | 0.037 | 0.148 | 0.028 | 0.002 |
| Non-lesional skin epidermic thickness (mm) | 0.146 | 0.027 | 0.142 | 0.023 | 0.138 | 0.020 | ns |
| Lesional skin dermis thickness (mm) | 1.749 | 0.480 | 1.656 | 0.690 | 1.607 | 0.678 | ns |
| Non-lesional skin dermis thickness (mm) | 1.559 | 0.451 | 1.650 | 0.567 | 1.589 | 0.527 | ns |
| Lesional skin vascularization | 2.292 | 0.450 | 1.292 | 0.450 | 1.042 | 0.396 | <0.001 |
| Non-lesional skin vascularization | 0.750 | 0.584 | 0.625 | 0.483 | 0.625 | 0.483 | ns |
| Lesion skin TEWL | 40.833 | 22,904 | 29,250 | 12,624 | 28,150 | 12,697 | ns |
| Non-lesional skin TEWL | 16,067 | 11,271 | 21,583 | 15,967 | 14,392 | 9.104 | ns |
| Lesion skin corneometry | 131,000 | 68,621 | 132,667 | 81,615 | 103,833 | 37,365 | ns |
| Non-lesional skin corneometry | 107,333 | 39,919 | 119,667 | 83,049 | 101,167 | 33,526 | ns |
| Time Line | t0 | t1 | t2 | ||||
|---|---|---|---|---|---|---|---|
| PARAMETERS | Mean | SD | Mean | SD | Mean | SD | p-Value |
| EASI | 12,050 | 7.584 | 6.183 | 3.945 | 5.667 | 5.297 | 0.020 |
| IGA | 2167 | 0.753 | 1.667 | 0.816 | 1.500 | 1.049 | 0.063 |
| DLQI | 9833 | 6.494 | 4.667 | 3.011 | 1.667 | 1.506 | 0.083 |
| Sleep-NRS | 3333 | 2.944 | 1.833 | 2.483 | 1.667 | 2.338 | ns |
| Itch-NRS | 6667 | 1.033 | 2.833 | 2.927 | 3.333 | 2.338 | 0.033 |
| Lesional skin SLEB (mm) | 0.195 | 0.085 | 0.146 | 0.084 | 0.139 | 0.159 | ns |
| Non-lesional skin SLEB (mm) | 0.038 | 0.049 | 0.050 | 0.045 | 0.044 | 0.040 | ns |
| Lesional skin epidermic thickness (mm) | 0.171 | 0.055 | 0.168 | 0.023 | 0.149 | 0.034 | 0.043 |
| Non-lesional skin epidermic thickness (mm) | 0.138 | 0.044 | 0.127 | 0.024 | 0.146 | 0.019 | ns |
| Lesional skin dermis thickness (mm) | 1.544 | 0.273 | 1.387 | 0.200 | 1.360 | 0.329 | ns |
| Non-lesional skin dermis thickness (mm) | 1.311 | 0.345 | 1.341 | 0.282 | 1.306 | 0.374 | ns |
| Lesional skin vascularization | 2.167 | 0.516 | 1.583 | 0.585 | 1.500 | 0.837 | ns |
| Non-lesional skin vascularization | 0.583 | 0.492 | 0.667 | 0.753 | 0.750 | 0.274 | ns |
| Lesion skin TEWL | 40.983 | 21,505 | 28,367 | 8.641 | 46,350 | 25,401 | ns |
| Not-lesional skin TEWL | 28,417 | 22,668 | 26,000 | 17,535 | 41,100 | 14,846 | ns |
| Lesion skin corneometry | 248,333 | 257,498 | 117,667 | 95,406 | 151,000 | 62,846 | ns |
| Not-lesional skin corneometry | 194,500 | 146,020 | 158,000 | 101,052 | 166,167 | 76,583 | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dini, V.; Iannone, M.; Michelucci, A.; Manzo Margiotta, F.; Granieri, G.; Salvia, G.; Oranges, T.; Janowska, A.; Morganti, R.; Romanelli, M. Ultra-High Frequency UltraSound (UHFUS) Assessment of Barrier Function in Moderate-to-Severe Atopic Dermatitis during Dupilumab Treatment. Diagnostics 2023, 13, 2721. https://doi.org/10.3390/diagnostics13172721
Dini V, Iannone M, Michelucci A, Manzo Margiotta F, Granieri G, Salvia G, Oranges T, Janowska A, Morganti R, Romanelli M. Ultra-High Frequency UltraSound (UHFUS) Assessment of Barrier Function in Moderate-to-Severe Atopic Dermatitis during Dupilumab Treatment. Diagnostics. 2023; 13(17):2721. https://doi.org/10.3390/diagnostics13172721
Chicago/Turabian StyleDini, Valentina, Michela Iannone, Alessandra Michelucci, Flavia Manzo Margiotta, Giammarco Granieri, Giorgia Salvia, Teresa Oranges, Agata Janowska, Riccardo Morganti, and Marco Romanelli. 2023. "Ultra-High Frequency UltraSound (UHFUS) Assessment of Barrier Function in Moderate-to-Severe Atopic Dermatitis during Dupilumab Treatment" Diagnostics 13, no. 17: 2721. https://doi.org/10.3390/diagnostics13172721
APA StyleDini, V., Iannone, M., Michelucci, A., Manzo Margiotta, F., Granieri, G., Salvia, G., Oranges, T., Janowska, A., Morganti, R., & Romanelli, M. (2023). Ultra-High Frequency UltraSound (UHFUS) Assessment of Barrier Function in Moderate-to-Severe Atopic Dermatitis during Dupilumab Treatment. Diagnostics, 13(17), 2721. https://doi.org/10.3390/diagnostics13172721