
Keratoconus Diagnosis: From Fundamentals to Artificial Intelligence: A Systematic Narrative Review

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Placido Disk-Based Corneal Topography
1.2. Orbscan
- Pachymetry of the thinnest point;
- Maximum posterior elevation in the central 3 mm;
- Irregularity in the central 3 mm;
- Vertical decentration of the thinnest point;
- Difference between mean central pachymetry (central zone 2 mm in diameter) and the pachymetry of the thinnest point;
- I–S value [6].
1.3. Pentacam Comprehensive Eye Scanner
1.4. Galilei Corneal Tomography
1.5. Sirius
- Vertical trefoil ;
- Vertical coma ;
- Horizontal coma ;
- Primary spherical aberration ;
- Second-order vertical coma .
- AKf-Apical Keratoscopy Front: the steepest point of the anterior corneal surface;
- Akb-Apical Keratoscopy Back: the steepest point of the posterior corneal surface;
- KVf-Keratoscopy Vertex Front: the highest point of ectasia on the anterior corneal surface;
- KVb-Keratoscopy Vertex Back: the highest point of ectasia on the posterior corneal surface.
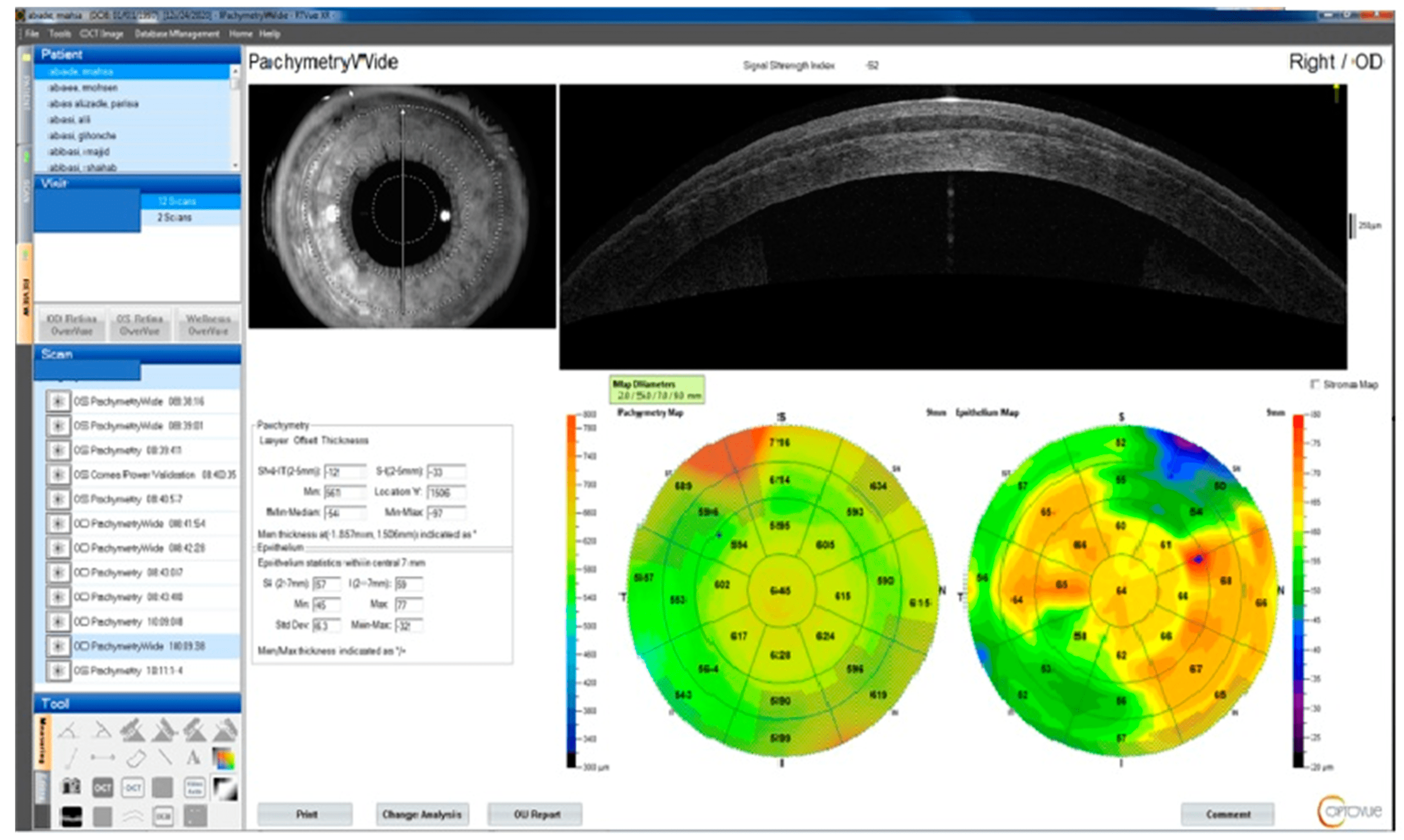
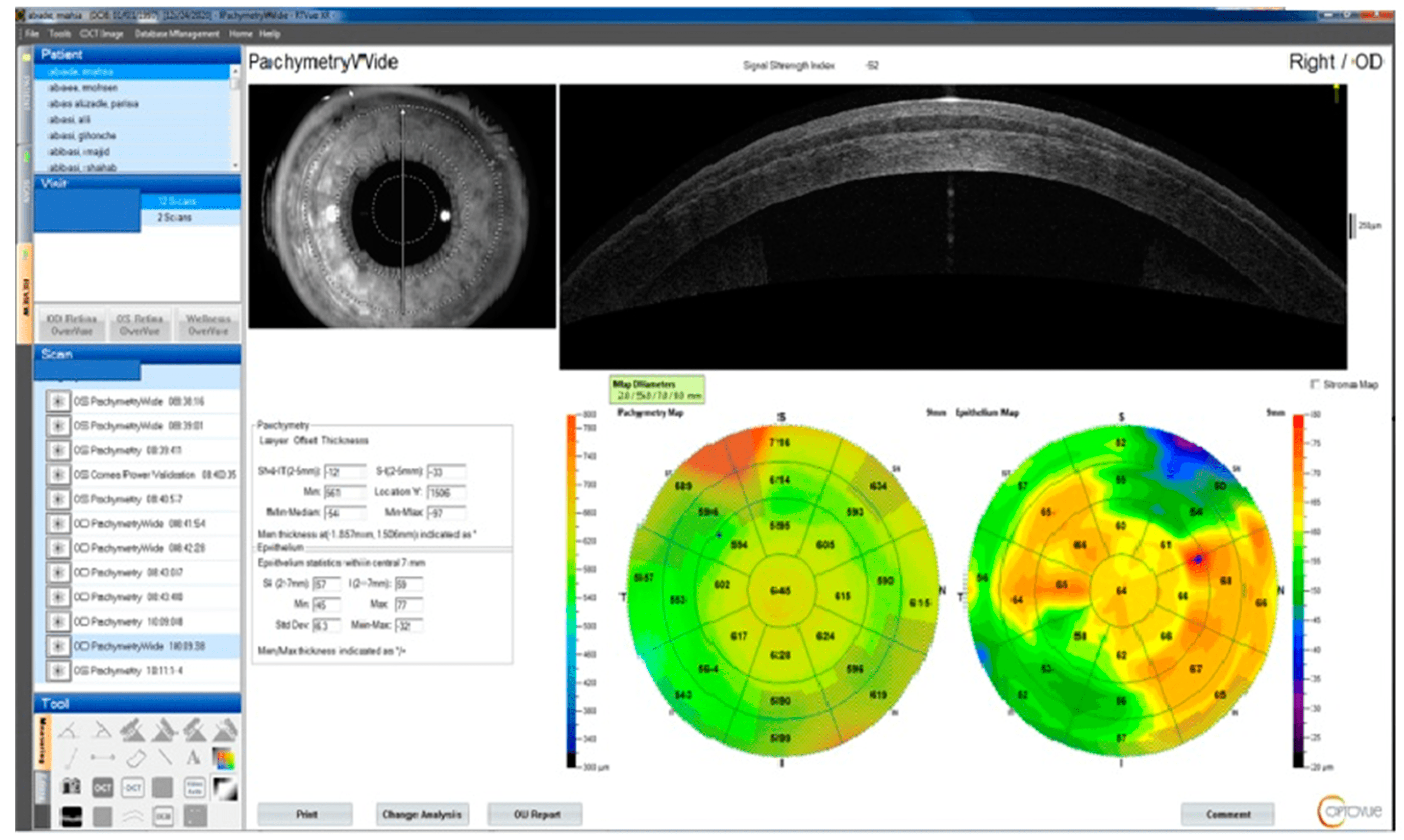
1.6. Optical Coherence Tomography
- The minimal thickness of the cornea (Min);
- The minimal corneal thickness minus the highest corneal thickness (Min–Max);
- The typical variation between the superonasal and inferotemporal corneal thicknesses between rings of two and five diameters (SN-IT);
1.7. Biomechanical Measurements
1.7.1. Ocular Response Analyzer
1.7.2. Corvis ST
1.8. Brillouin Microscopy
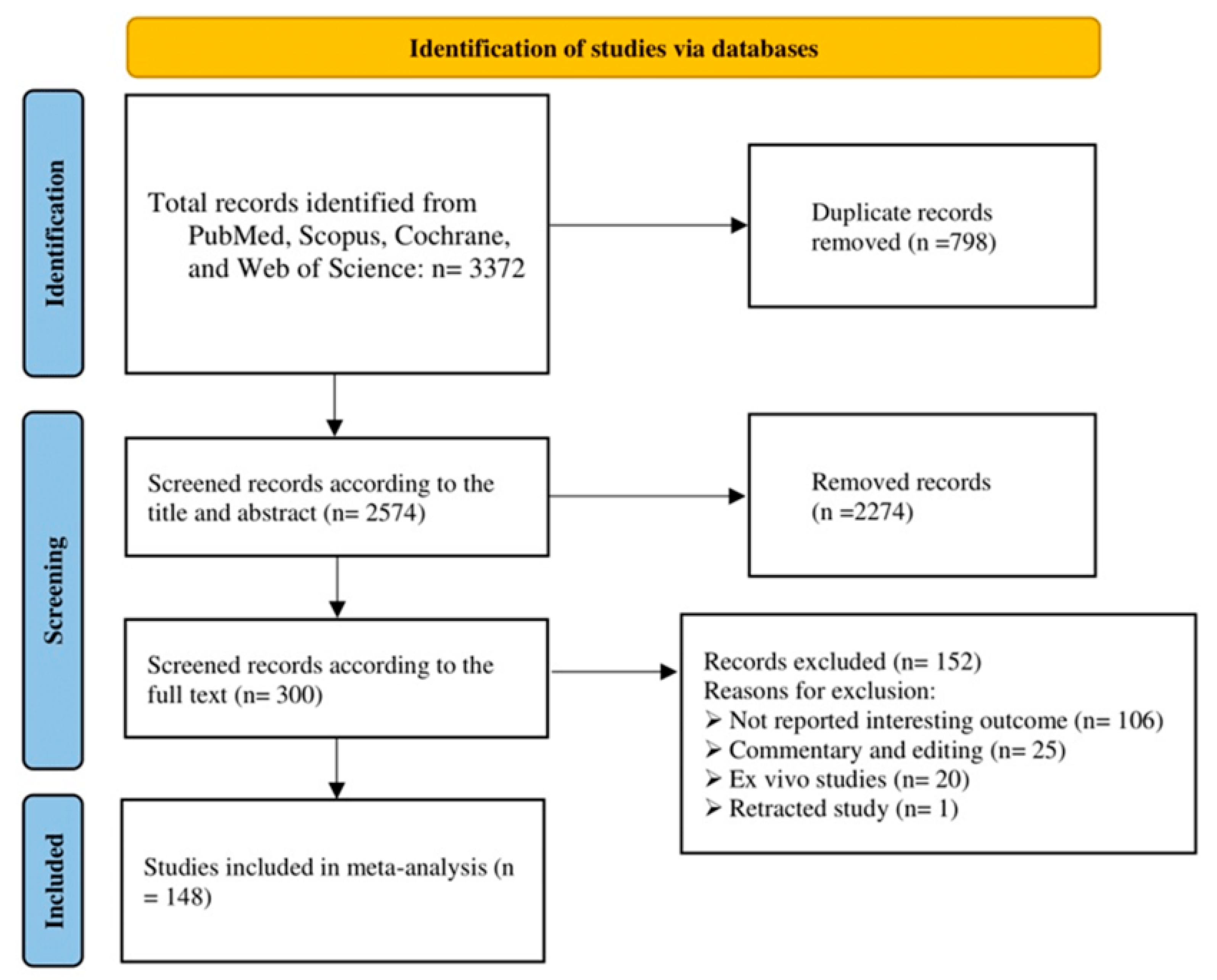
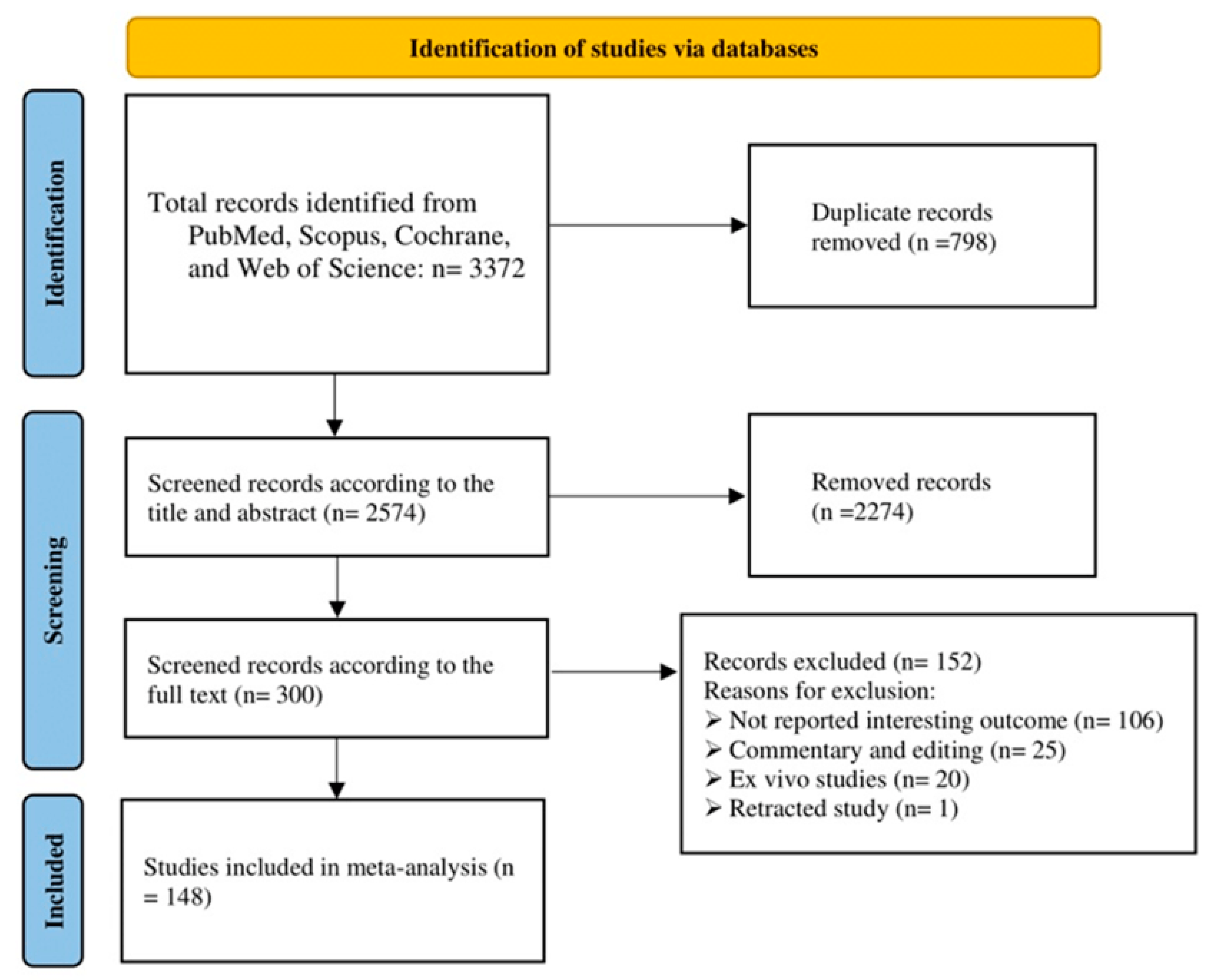
2. Materials and Methods
- 1-
- (“keratoconus”);
- 2-
- AND ((algorithm) OR (machine learn *) OR (deep learn *) OR (artificial intelligence) OR (automatic));
- 3-
- AND ((detect *) OR (diagnos *) OR (screen *) OR (examin *) OR (analys *) OR (investigat *) OR (identif *) OR (discover *) OR (interpret *) OR (test *)).
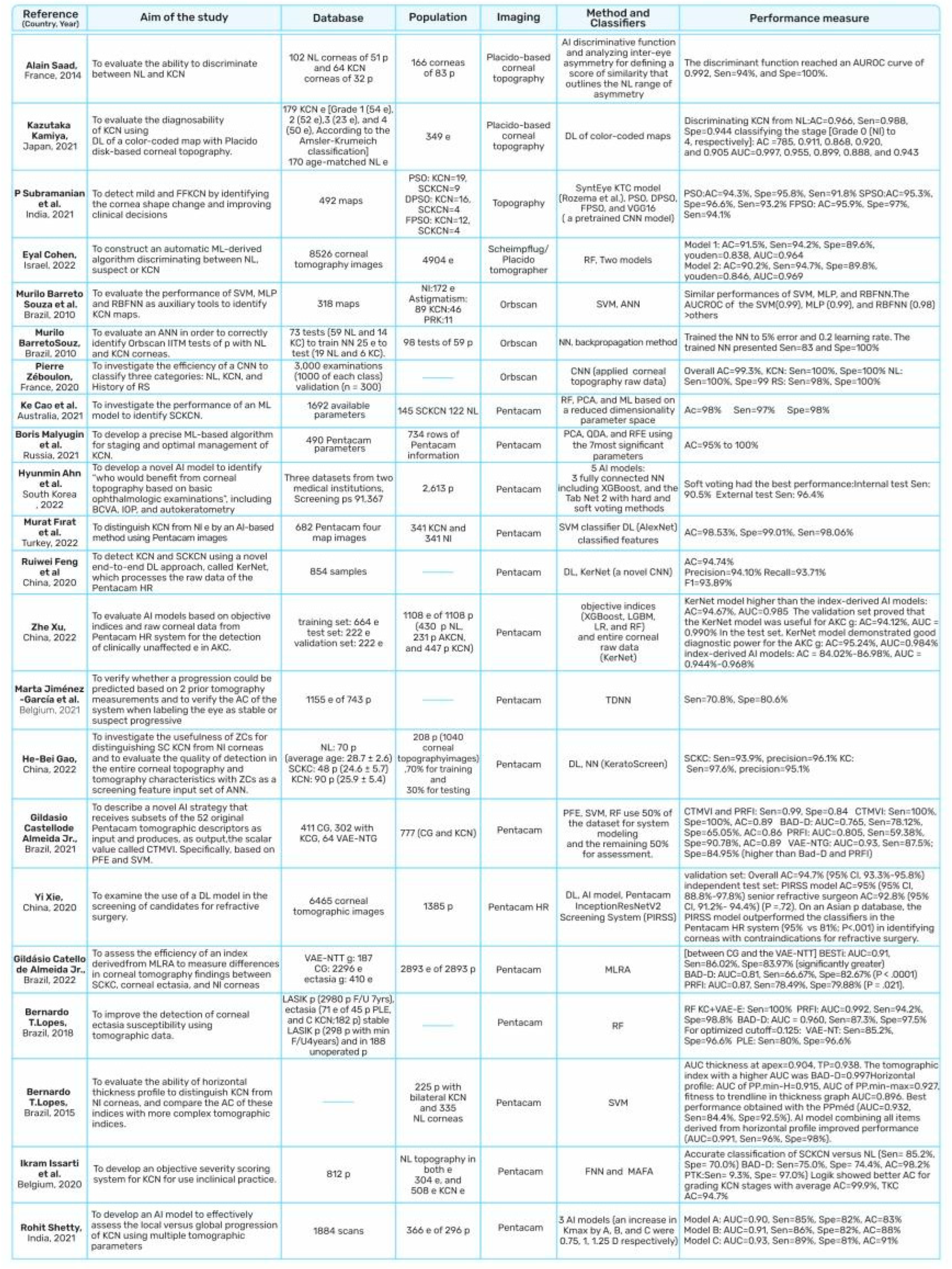
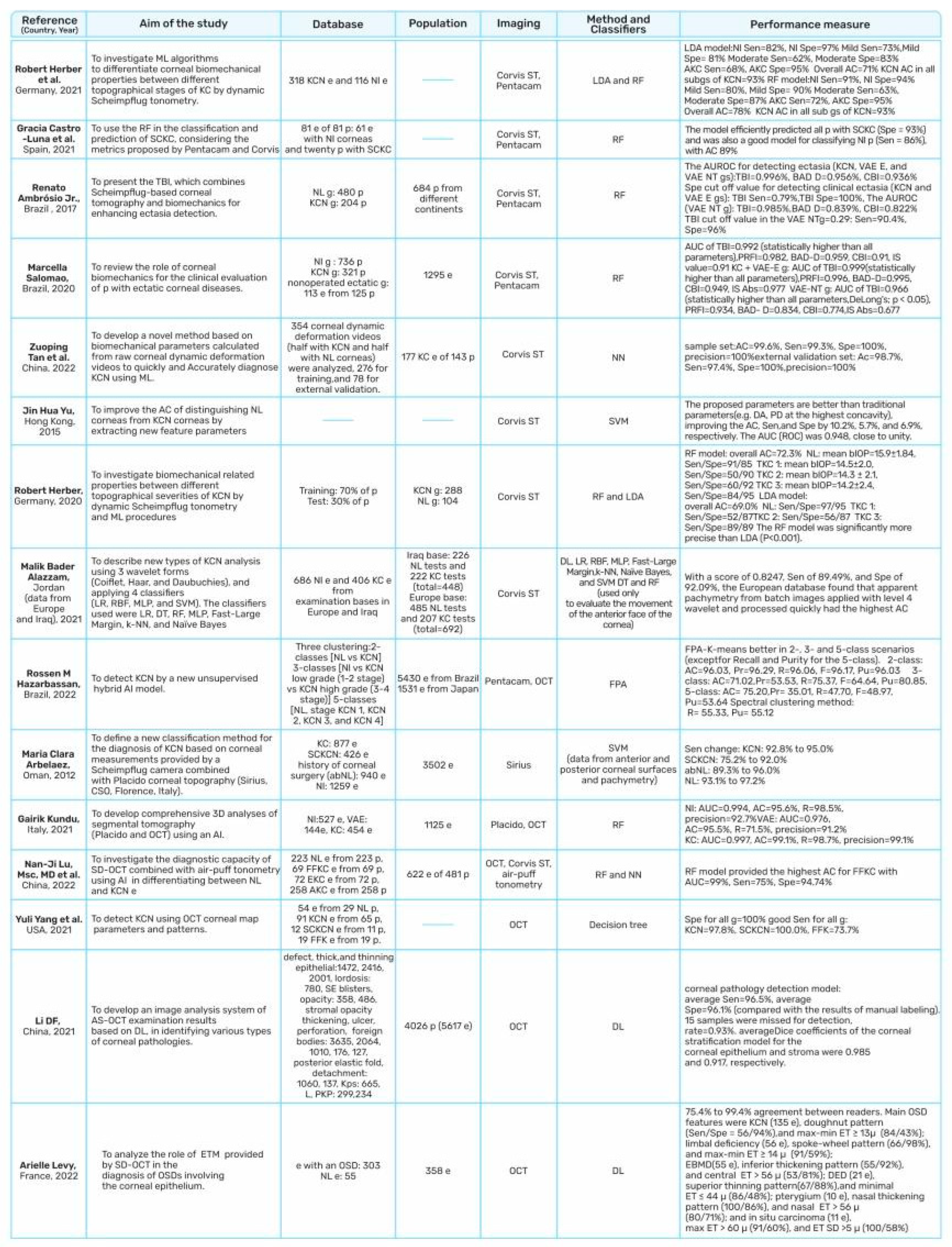
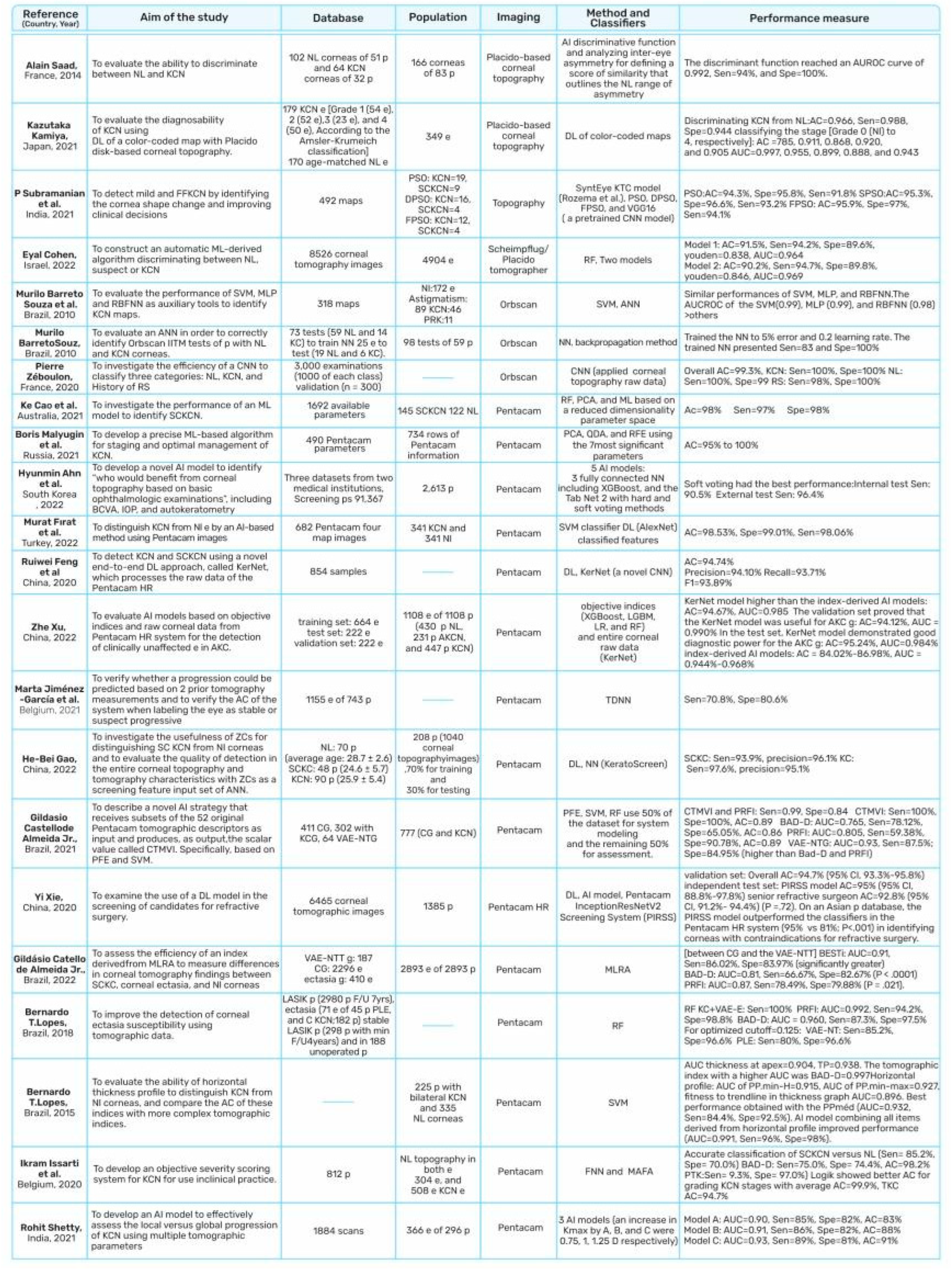
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whitcher, J.P.; Srinivasan, M.; Upadhyay, M.P. Corneal blindness: A global perspective. Bull. World Health Organ. 2001, 79, 214–221. [Google Scholar] [PubMed]
- Cao, K.; Verspoor, K.; Sahebjada, S.; Baird, P.N. Accuracy of Machine Learning Assisted Detection of Keratoconus: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 478. [Google Scholar] [CrossRef]
- Gatinel, D.; Galvis, V.; Tello, A.; Niño, C.A.; Rey, J.J.; Camacho, P.A.; Serrano, S.E. Obstructive Sleep Apnea–Hypopnea Syndrome and Keratoconus: An Epiphenomenon Related to Sleep Position? Cornea 2020, 39, e11–e12. [Google Scholar] [CrossRef] [PubMed]
- Gurnani, B.; Kaur, K. Evolving concepts in etiopathogenesis of keratoconus: Is it quasi-inflammatory or inflammatory? Indian J. Ophthalmol. 2023, 71, 2609–2610. [Google Scholar] [CrossRef] [PubMed]
- Seth, I.; Bulloch, G.; Vine, M.; Outmezguine, J.; Seth, N.; Every, J.; Daniell, M. The association between keratoconus and allergic eye diseases: A systematic review and meta-analysis. Clin. Exp. Ophthalmol. 2023, 51, O1–O16. [Google Scholar] [CrossRef]
- Hashemi, H.; Heydarian, S.; Hooshmand, E.; Saatchi, M.; Yekta, A.A.; Aghamirsalim, M.; Valadkhan, M.; Mortazavi, M.; Hashemi, A.; Khabazkhoob, M. The Prevalence and Risk Factors for Keratoconus: A Systematic Review and Meta-Analysis. Cornea 2020, 39, 263–270. [Google Scholar] [CrossRef]
- Deshmukh, R.; Ong, Z.Z.; Rampat, R.; del Barrio, J.L.A.; Barua, A.; Ang, M.; Mehta, J.S.; Said, D.G.; Dua, H.S.; Ambrósio, R.; et al. Management of keratoconus: An updated review. Front. Med. 2023, 10, 1212314. [Google Scholar] [CrossRef]
- Galvis, V.; Tello, A.; Laiton, A.N.; Salcedo, S.L.L. Indications and techniques of corneal transplantation in a referral center in Colombia, South America (2012–2016). Int. Ophthalmol. 2019, 39, 1723–1733. [Google Scholar] [CrossRef]
- Henriquez, M.A.; Hadid, M.; Izquierdo, L. A Systematic Review of Subclinical Keratoconus and Forme Fruste Keratoconus. J. Refract. Surg. 2020, 36, 270–279. [Google Scholar] [CrossRef]
- Saad, A. Validation of a New Scoring System for the Detection of Early Forme of Keratoconus. Int. J. Keratoconus Ectatic Corneal Dis. 2012, 1, 100–108. [Google Scholar] [CrossRef]
- Saad, A.; Gatinel, D. Topographic and Tomographic Properties of Forme Fruste Keratoconus Corneas. Investig. Ophthalmol. Vis. Sci. 2010, 51, 5546–5555. [Google Scholar] [CrossRef] [PubMed]
- Krachmer, J.H.; Feder, R.S.; Belin, M.W. Keratoconus and related noninflammatory corneal thinning disorders. Surv. Ophthalmol. 1984, 28, 293–322. [Google Scholar] [CrossRef] [PubMed]
- Niazi, S.; Moshirfar, M.; Alizadeh, F.; Doroodgar, F.; Baradaran-Rafii, A.; Filutowski, O.; Niazi, F.; Ambrósio, R. Association of 2 Lysyl Oxidase Gene Single Nucleotide Polymorphisms with Keratoconus. Ophthalmol. Sci. 2023, 3, 100247. [Google Scholar] [CrossRef] [PubMed]
- Loukovitis, E.; Sfakianakis, K.; Syrmakesi, P.; Tsotridou, E.; Orfanidou, M.; Bakaloudi, D.R.; Stoila, M.; Kozei, A.; Koronis, S.; Zachariadis, Z.; et al. Genetic Aspects of Keratoconus: A Literature Review Exploring Potential Genetic Contributions and Possible Genetic Relationships with Comorbidities. Ophthalmol. Ther. 2018, 7, 263–292. [Google Scholar] [CrossRef] [PubMed]
- Bawazeer, A.M.; Hodge, W.G.; Lorimer, B. Atopy and keratoconus: A multivariate analysis. Br. J. Ophthalmol. 2000, 84, 834–836. [Google Scholar] [CrossRef]
- Ferdi, A.C.; Nguyen, V.; Gore, D.M.; Allan, B.D.; Rozema, J.J.; Watson, S.L. Keratoconus Natural Progression. Ophthalmology 2019, 126, 935–945. [Google Scholar] [CrossRef]
- Jiménez-García, M.; Issarti, I.; Kreps, E.O.; Dhubhghaill, S.N.; Koppen, C.; Varssano, D.; Rozema, J.J.; on behalf of The REDCAKE Study Group. Forecasting Progressive Trends in Keratoconus by Means of a Time Delay Neural Network. J. Clin. Med. 2021, 10, 3238. [Google Scholar] [CrossRef]
- Kato, N.; Masumoto, H.; Tanabe, M.; Sakai, C.; Negishi, K.; Torii, H.; Tabuchi, H.; Tsubota, K. Predicting Keratoconus Progression and Need for Corneal Crosslinking Using Deep Learning. J. Clin. Med. 2021, 10, 844. [Google Scholar] [CrossRef]
- Maile, H.P.; Li, J.-P.O.; Fortune, M.D.; Royston, P.; Leucci, M.T.; Moghul, I.; Szabo, A.; Balaskas, K.; Allan, B.D.; Hardcastle, A.J.; et al. Personalized Model to Predict Keratoconus Progression From Demographic, Topographic, and Genetic Data. Am. J. Ophthalmol. 2022, 240, 321–329. [Google Scholar] [CrossRef]
- Shetty, R.; Kundu, G.; Narasimhan, M.R.; Khamar, P.; Gupta, K.; Singh, N.; Nuijts, R.M.; Roy, A.S. Artificial Intelligence Efficiently Identifies Regional Differences in the Progression of Tomographic Parameters of Keratoconic Corneas. J. Refract. Surg. 2021, 37, 240–248. [Google Scholar] [CrossRef]
- Klyce, S.D.; Smolek, M.K.; Maeda, N. Keratoconus Detection with the KISA% Method—Another View. J. Cataract. Refract. Surg. 2000, 26, 472–473. [Google Scholar] [CrossRef] [PubMed]
- Maeda, N.; Klyce, S.D.; Smolek, M.K.; Thompson, H.W. Automated keratoconus screening with corneal topography analysis. Investig. Ophthalmol. Vis. Sci. 1994, 35, 2749–2757. [Google Scholar]
- Smolek, M.K.; Klyce, S.D. Current keratoconus detection methods compared with a neural network approach. Investig. Ophthalmol. Vis. Sci. 1997, 38, 2290–2299. [Google Scholar]
- Maeda, N.; Klyce, S.D.; Smolek, M.K. Neural network classification of corneal topography. Preliminary demonstration. Investig. Ophthalmol. Vis. Sci. 1995, 36, 1327–1335. [Google Scholar]
- Castro-Luna, G.M.; Martínez-Finkelshtein, A.; Ramos-López, D. Robust keratoconus detection with Bayesian network classifier for Placido-based corneal indices. Cont. Lens Anterior Eye 2020, 43, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Souza, M.B.; Medeiros, F.W.; Souza, D.B.; Garcia, R.; Alves, M.R. Evaluation of machine learning classifiers in keratoconus detection from orbscan II examinations. Clinics 2010, 65, 1223–1228. [Google Scholar] [CrossRef]
- Souza, M.B.; de Medeiros, F.W.; Souza, D.B.; Alves, M.R. Diagnóstico do ceratocone baseado no Orbscan com o auxílio de uma rede neural. Arq. Bras. Oftalmol. 2009, 71, 65–68. [Google Scholar] [CrossRef]
- Castro-Luna, G.; Jiménez-Rodríguez, D.; Castaño-Fernández, A.B.; Pérez-Rueda, A. Diagnosis of Subclinical Keratoconus Based on Machine Learning Techniques. J. Clin. Med. 2021, 10, 4281. [Google Scholar] [CrossRef]
- Lopes, B.T.; Ramos, I.C.; Salomão, M.Q.; Guerra, F.P.; Schallhorn, S.C.; Schallhorn, J.M.; Vinciguerra, R.; Vinciguerra, P.; Price, F.W., Jr.; Price, M.O.; et al. Enhanced tomographic assessment to detect corneal ectasia based on artificial intel-ligence. Am. J. Ophthalmol. 2018, 195, 223–232. [Google Scholar] [CrossRef]
- Kovács, I.; Miháltz, K.; Kránitz, K.; Juhász, É.; Takács, Á.; Dienes, L.; Gergely, R.; Nagy, Z.Z. Accuracy of machine learning classifiers using bilateral data from a Scheimpflug camera for identifying eyes with preclinical signs of keratoconus. J. Cataract. Refract. Surg. 2016, 42, 275–283. [Google Scholar] [CrossRef]
- Issarti, I.; Consejo, A.; Jiménez-García, M.; Hershko, S.; Koppen, C.; Rozema, J.J. Computer aided diagnosis for suspect keratoconus detection. Comput. Biol. Med. 2019, 109, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Issarti, I.; Consejo, A.; Jiménez-García, M.; Kreps, E.O.; Koppen, C.; Rozema, J.J. Logistic index for keratoconus detection and severity scoring (Logik). Comput. Biol. Med. 2020, 122, 103809. [Google Scholar] [CrossRef] [PubMed]
- Smadja, D.; Touboul, D.; Cohen, A.; Doveh, E.; Santhiago, M.R.; Mello, G.R.; Krueger, R.R.; Colin, J. Detection of Subclinical Keratoconus Using an Automated Decision Tree Classification. Am. J. Ophthalmol. 2013, 156, 237–246.e1. [Google Scholar] [CrossRef] [PubMed]
- Golan, O.; Hwang, E.S.; Lang, P.; Santhiago, M.R.; Abulafia, A.; Touboul, D.; Krauthammer, M.; Smadja, D. Differences in posterior corneal features between normal corneas and subclinical kerato-conus. J. Refract. Surg. 2018, 34, 664–670. [Google Scholar] [CrossRef]
- Velázquez-Blázquez, J.S.; Bolarín, J.M.; Cavas-Martínez, F.; Alió, J.L. EMKLAS: A New Automatic Scoring System for Early and Mild Keratoconus Detection. Transl. Vis. Sci. Technol. 2020, 9, 30. [Google Scholar] [CrossRef]
- Shi, C.; Wang, M.; Zhu, T.; Zhang, Y.; Ye, Y.; Jiang, J.; Chen, S.; Lu, F.; Shen, M. Machine learning helps improve diagnostic ability of subclinical keratoconus using Scheimpflug and OCT imaging modalities. Eye Vis. 2020, 7, 48. [Google Scholar] [CrossRef] [PubMed]
- Ambrósio, R.; Lopes, B.T.; Faria-Correia, F.; Salomão, M.Q.; Bühren, J.; Roberts, C.J.; Elsheikh, A.; Vinciguerra, R.; Vinciguerra, P. Integration of Scheimpflug-Based Corneal Tomography and Biomechanical Assessments for Enhancing Ectasia Detection. J. Refract. Surg. 2017, 33, 434–443. [Google Scholar] [CrossRef]
- Ambrósio, R.; Machado, A.P.; Leão, E.; Lyra, J.M.G.; Salomão, M.Q.; Esporcatte, L.G.P.; Filho, J.B.d.F.; Ferreira-Meneses, E.; Sena, N.B.; Haddad, J.S.; et al. Optimized Artificial Intelligence for Enhanced Ectasia Detection Using Scheimpflug-Based Corneal Tomography and Biomechanical Data. Am. J. Ophthalmol. 2022, 251, 126–142. [Google Scholar] [CrossRef]
- Ruiz Hidalgo, I.; Rodriguez, P.; Rozema, J.J.; Ní Dhubhghaill, S.; Zakaria, N.; Tassignon, M.-J.; Koppen, C. Evaluation of a Machine-Learning Classifier for Keratoconus Detection Based on Scheimpflug Tomography. Cornea 2016, 35, 827–832. [Google Scholar] [CrossRef]
- Kuo, B.-I.; Chang, W.-Y.; Liao, T.-S.; Liu, F.-Y.; Liu, H.-Y.; Chu, H.-S.; Chen, W.-L.; Hu, F.-R.; Yen, J.-Y.; Wang, I.-J. Keratoconus Screening Based on Deep Learning Approach of Corneal Topography. Transl. Vis. Sci. Technol. 2020, 9, 53. [Google Scholar] [CrossRef]
- Cao, K.; Verspoor, K.; Sahebjada, S.; Baird, P.N. Evaluating the Performance of Various Machine Learning Algorithms to Detect Subclinical Keratoconus. Transl. Vis. Sci. Technol. 2020, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- Vinciguerra, R.; Ambrósio, R.; Roberts, C.J.; Azzolini, C.; Vinciguerra, P. Biomechanical Characterization of Subclinical Keratoconus Without Topographic or Tomographic Abnormalities. J. Refract. Surg. 2017, 33, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Klyce, S.D. Computer-assisted corneal topography. High-resolution graphic presentation and analysis of keratoscopy. Investig. Ophthalmol. Vis. Sci. 1984, 25, 1426–1435. [Google Scholar]
- Klyce, S.D.; Wilson, S.E. Imaging, Reconstruction, and Display of Corneal Topography. In New Methods in Microscopy and Low Light Imaging; SPIE: Bellingham, WA, USA, 1989; Volume 1161, pp. 409–417. [Google Scholar] [CrossRef]
- Rabinowitz, Y.S.; Garbus, J.; McDonnell, P.J. Computer-assisted corneal topography in family members of patients with kerato-conus. Arch. Ophthalmol. 1990, 108, 365–371. [Google Scholar] [CrossRef]
- Rabinowitz, Y.S.; Rasheed, K. KISA% index: A quantitative videokeratography algorithm embodying minimal topographic criteria for diagnosing keratoconus. J. Cataract. Refract. Surg. 1999, 25, 1327–1335. [Google Scholar] [CrossRef]
- Cohen, E.; Bank, D.; Sorkin, N.; Giryes, R.; Varssano, D. Use of machine learning to achieve keratoconus detection skills of a corneal expert. Int. Ophthalmol. 2022, 42, 3837–3847. [Google Scholar] [CrossRef]
- Kundu, G.; Shetty, R.; Khamar, P.; Mullick, R.; Gupta, S.; Nuijts, R.; Roy, A.S. Universal architecture of corneal segmental tomography biomarkers for artificial intelligence-driven diagnosis of early keratoconus. Br. J. Ophthalmol. 2021, 107, 635–643. [Google Scholar] [CrossRef]
- Kamiya, K.; Ayatsuka, Y.; Kato, Y.; Shoji, N.; Mori, Y.; Miyata, K. Diagnosability of Keratoconus Using Deep Learning With Placido Disk-Based Corneal Topography. Front. Med. 2021, 8, 724902. [Google Scholar] [CrossRef]
- Klyce, S.D.; Karon, M.D.; Smolek, M.K. Screening Patients With the Corneal Navigator. J. Refract. Surg. 2005, 21, S617–S622. [Google Scholar] [CrossRef]
- Schiano-Lomoriello, D.; Bono, V.; Abicca, I.; Savini, G. Repeatability of anterior segment measurements by optical coherence to-mography combined with Placido disk corneal topography in eyes with keratoconus. Sci. Rep. 2020, 10, 1124. [Google Scholar] [CrossRef]
- Rainer, G.; Findl, O.; Petternel, V.; Kiss, B.; Drexler, W.; Skorpik, C.; Georgopoulos, M.; Schmetterer, L. Central corneal thickness measurements with partial coherence interferometry, ultrasound, and the Orbscan system. Ophthalmology 2004, 111, 875–879. [Google Scholar] [CrossRef] [PubMed]
- Gharieb, H.M.; Othman, I.S.; Oreaba, A.H.; Abdelatif, M.K. Topographic, elevation, and keratoconus indices for diagnosis of kera-toconus by a combined Placido and Scheimpflug topography system. Eur. J. Ophthalmol. 2021, 31, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Ang, M.; Saad, A.; Chua, D.; Mejia, M.; Lim, L.; Gatinel, D. Validation of an Objective Scoring System for Forme Fruste Keratoconus Detection and Post-LASIK Ectasia Risk Assessment in Asian Eyes. Cornea 2015, 34, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Bühren, J.; Schäffeler, T.; Kohnen, T. Validation of metrics for the detection of subclinical keratoconus in a new patient collective. J. Cataract. Refract. Surg. 2014, 40, 259–268. [Google Scholar] [CrossRef]
- Zéboulon, P.; Debellemanière, G.; Bouvet, M.; Gatinel, D. Corneal Topography Raw Data Classification Using a Convolutional Neural Network. Am. J. Ophthalmol. 2020, 219, 33–39. [Google Scholar] [CrossRef]
- Lazouni, M.E.A.; Messadi, M.; Feroui, A.; Mahmoudi, S. Early Keratoconus Disease Detection Using Orbscan II Corneal Topography. J. Mech. Med. Biol. 2022, 23, 2350001. [Google Scholar] [CrossRef]
- Ali, A.H.; Ghaeb, N.H.; Musa, Z.M. Support vector machine for keratoconus detection by using topographic maps with the help of image processing techniques. IOSR J. Pharm. Biol. Sci. 2017, 12, 50–58. [Google Scholar]
- Ambrósio, R., Jr.; Belin, M.W. Imaging of the cornea: Topography vs tomography. J. Refract. Surg. 2010, 26, 847–849. [Google Scholar] [CrossRef]
- Salomão, M.; Hoffling-Lima, A.L.; Lopes, B.; Belin, M.W.; Sena, N.; Dawson, D.G.; Ambrósio, R. Recent developments in keratoconus diagnosis. Expert Rev. Ophthalmol. 2018, 13, 329–341. [Google Scholar] [CrossRef]
- Hernández-Camarena, J.C.; Chirinos-Saldaña, P.; Navas, A.; Ramirez-Miranda, A.; de la Mota, A.; Jimenez-Corona, A.; Graue-Hernández, E.O. Repeatability, Reproducibility, and Agreement Between Three Different Scheimpflug Systems in Measuring Corneal and Anterior Segment Biometry. J. Refract. Surg. 2014, 30, 616–621. [Google Scholar] [CrossRef]
- Pateras, E.; Nousi, A. The Reliability between Placido Topography and Scheimpflug Topography in Normal Corneas with Astigmatism less Than 0.50 Dc. Ophthalmol. Res. Int. J. 2020, 12, 27–35. [Google Scholar] [CrossRef]
- Shehata, A.E.M.; Foster, J.W.; Jun, A.S.; Soiberman, U.S. The Correlation between Corneal Findings and Disease Severity in Keratoconus per Scheimpflug Corneal Tomography. J. Ophthalmol. 2020, 2020, 4130643. [Google Scholar] [CrossRef] [PubMed]
- Kamiya, K.; Ishii, R.; Shimizu, K.; Igarashi, A. Evaluation of corneal elevation, pachymetry and keratometry in keratoconic eyes with respect to the stage of Amsler-Krumeich classification. Br. J. Ophthalmol. 2014, 98, 459–463. [Google Scholar] [CrossRef] [PubMed]
- Orucoglu, F.; Toker, E. Comparative Analysis of Anterior Segment Parameters in Normal and Keratoconus Eyes Generated by Scheimpflug Tomography. J. Ophthalmol. 2015, 2015, 925414. [Google Scholar] [CrossRef]
- Randleman, J.B.; Dupps, W.J.J.; Santhiago, M.R.; Rabinowitz, Y.S.; Koch, D.D.; Stulting, R.D.; Klyce, S.D. Screening for Keratoconus and Related Ectatic Corneal Disorders. Cornea 2015, 34, e20–e22. [Google Scholar] [CrossRef] [PubMed]
- Motlagh, M.N.; Moshirfar, M.; Murri, M.S.; Skanchy, D.F.; Momeni-Moghaddam, H.; Ronquillo, Y.C.; Hoopes, P.C. Pentacam® Corneal Tomography for Screening of Refractive Surgery Candidates: A Review of the Literature, Part I. Med. Hypothesis Discov. Innov. Ophthalmol. 2019, 8, 177–203. [Google Scholar]
- De Sanctis, U.; Loiacono, C.; Richiardi, L.; Turco, D.; Mutani, B.; Grignolo, F.M. Sensitivity and Specificity of Posterior Corneal Elevation Measured by Pentacam in Discriminating Keratoconus/Subclinical Keratoconus. Ophthalmology 2008, 115, 1534–1539. [Google Scholar] [CrossRef]
- Chan, T.; Wang, Y.; Yu, M.; Jhanji, V. Comparison of corneal dynamic parameters and tomographic measurements using Scheimpflug imaging in keratoconus. Br. J. Ophthalmol. 2018, 102, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Bae, G.H.; Kim, J.R.; Kim, C.H.; Lim, D.H.; Chung, E.S.; Chung, T.Y. Corneal topographic and tomographic analysis of fellow eyes in unilateral keratoconus patients using Pentacam. Am. J. Ophthalmol. 2014, 157, 103–109.e1. [Google Scholar] [CrossRef]
- Shajari, M.; Steinwender, G.; Herrmann, K.; Kubiak, K.B.; Pavlovic, I.; Plawetzki, E.; Schmack, I.; Kohnen, T. Evaluation of keratoconus progression. Br. J. Ophthalmol. 2019, 103, 551–557. [Google Scholar] [CrossRef]
- Huseynli, S.; Abdulaliyeva, F. Evaluation of Scheimpflug Tomography Parameters in Subclinical Keratoconus, Clinical Keratoconus and Normal Caucasian Eyes. Turk. J. Ophthalmol. 2018, 48, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Shetty, R.; Arora, V.; Jayadev, C.; Nuijts, R.M.M.A.; Kumar, M.; Puttaiah, N.K.; Kummelil, M.K. Repeatability and Agreement of Three Scheimpflug-Based Imaging Systems for Measuring Anterior Segment Parameters in Keratoconus. Investig. Ophthalmol. Vis. Sci. 2014, 55, 5263–5268. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Beiranvand, A.; Yekta, A.; Maleki, A.; Yazdani, N.; Khabazkhoob, M. Pentacam top indices for diagnosing subclinical and definite keratoconus. J. Curr. Ophthalmol. 2016, 28, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Arbelaez, M.C.; Versaci, F.; Vestri, G.; Barboni, P.; Savini, G. Use of a Support Vector Machine for Keratoconus and Subclinical Keratoconus Detection by Topographic and Tomographic Data. Ophthalmology 2012, 119, 2231–2238. [Google Scholar] [CrossRef]
- Belin, M.; Duncan, J. Keratoconus: The ABCD grading system. Klin. Monatsbl. Augenheilkd. 2016, 233, 701–707. [Google Scholar] [CrossRef]
- Ambrósio, R.; Faria-Correia, F.; Ramos, I.; Valbon, B.F.; Lopes, B.; Jardim, D.; Luz, A. Enhanced Screening for Ectasia Susceptibility Among Refractive Candidates: The Role of Corneal Tomography and Biomechanics. Curr. Ophthalmol. Rep. 2013, 1, 28–38. [Google Scholar] [CrossRef]
- Sedaghat, M.R.; Momeni-Moghaddam, H.; Ambrósio, R., Jr.; Heidari, H.R.; Maddah, N.; Danesh, Z.; Sabzi, F. Diagnostic ability of corneal shape and biomechanical parameters for detecting frank keratoconus. Cornea 2018, 37, 1025–1034. [Google Scholar] [CrossRef]
- Ramos, I.; Correia, F.F.; Lopes, B.; Salomão, M.Q.; O Correa, R. Topometric and Tomographic Indices for the Diagnosis of Keratoconus. Int. J. Keratoconus Ectatic Corneal Dis. 2012, 1, 92–99. [Google Scholar] [CrossRef]
- Steinberg, J.; Aubke-Schultz, S.; Frings, A.; Hülle, J.; Druchkiv, V.; Richard, G.; Katz, T.; Linke, S.J. Correlation of the KISA% index and Scheimpflug tomography in ‘normal’, ‘subclinical’, ‘keratoconus-suspect’ and ‘clinically manifest’ keratoconus eyes. Acta Ophthalmol. 2015, 93, e199–e207. [Google Scholar] [CrossRef]
- Martínez-Abad, A.; Piñero, D.P. New perspectives on the detection and progression of keratoconus. J. Cataract. Refract. Surg. 2017, 43, 1213–1227. [Google Scholar] [CrossRef]
- Muftuoglu, O.; Ayar, O.; Ozulken, K.; Ozyol, E.; Akıncı, A. Posterior corneal elevation and back difference corneal elevation in diagnosing forme fruste keratoconus in the fellow eyes of unilateral keratoconus patients. J. Cataract. Refract. Surg. 2013, 39, 1348–1357. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, P.R.R.; Galletti, J.D.; Minguez, N.; Delrivo, M.; Bonthoux, F.F.; Pförtner, T.; Galletti, J.G. Pentacam Scheimpflug Tomography Findings in Topographically Normal Patients and Subclinical Keratoconus Cases. Am. J. Ophthalmol. 2014, 158, 32–40.e2. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Zhang, X.; Hu, Q.; Zhou, W.-Y.; Yang, F. Evaluation of Corneal Thickness and Volume Parameters of Subclinical Keratoconus Using a Pentacam Scheimflug System. Curr. Eye Res. 2016, 41, 923–926. [Google Scholar] [CrossRef]
- Demir, S.; Ortak, H.; Yeter, V.; Alim, S.; Sayn, O.; Taş, U.; Sönmez, B. Mapping Corneal Thickness Using Dual-Scheimpflug Imaging at Different Stages of Keratoconus. Cornea 2013, 32, 1470–1474. [Google Scholar] [CrossRef]
- Jiménez-García, M.; Kreps, E.O.; Dhubhghaill, S.N.; Koppen, C.; Rozema, J.J.; The REDCAKE Study Group. Determining the Most Suitable Tomography-Based Parameters to Describe Progression in Keratoconus. The Retrospective Digital Computer Analysis of Keratoconus Evolution Project. Eye Contact Lens 2021, 47, 486–493. [Google Scholar] [CrossRef]
- Guber, I.; McAlinden, C.; Majo, F.; Bergin, C. Identifying more reliable parameters for the detection of change during the follow-up of mild to moderate keratoconus patients. Eye Vis. 2017, 4, 24. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Li, W.; Jiang, J.; Zhuang, X.; Chen, W.; Peng, M.; Wang, J.; Lu, F.; Shen, M.; Wang, Y. Characteristic of entire corneal topography and tomography for the detection of sub-clinical keratoconus with Zernike polynomials using Pentacam. Sci. Rep. 2017, 7, 16486. [Google Scholar] [CrossRef]
- Heidari, Z.; Mohammadpour, M.; Amanzadeh, K.; Fotouhi, A. Evaluation of corneal topographic, tomographic and biomechanical indices for detecting clinical and subclinical keratoconus: A comprehensive three-device study. Int. J. Ophthalmol. 2021, 14, 228–239. [Google Scholar] [CrossRef]
- Değirmenci, C.; Palamar, M.; Ismayilova, N.; Eğrilmez, S.; Yağcı, A. Topographic Evaluation of Unilateral Keratoconus Patients. Turk. J. Ophthalmol. 2019, 49, 117–122. [Google Scholar] [CrossRef]
- Salomão, M.Q.; Hofling-Lima, A.L.; Esporcatte, L.P.G.; Lopes, B.; Vinciguerra, R.; Vinciguerra, P.; Bühren, J.; Sena, N.; Hilgert, G.S.L.; Ambrósio, R. The Role of Corneal Biomechanics for the Evaluation of Ectasia Patients. Int. J. Environ. Res. Public Health 2020, 17, 2113. [Google Scholar] [CrossRef]
- Li, X.; Yang, H.; Rabinowitz, Y.S. Keratoconus: Classification scheme based on videokeratography and clinical signs. J. Cataract. Refract. Surg. 2009, 35, 1597–1603. [Google Scholar] [CrossRef] [PubMed]
- Koh, S.; Inoue, R.; Ambrósio, R., Jr.; Maeda, N.; Miki, A.; Nishida, K. Correlation between corneal biomechanical indices and the severity of keratoconus. Cornea 2020, 39, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, J.; Katz, T.; Lücke, K.; Frings, A.; Druchkiv, V.M.; Linke, S.J. Screening for Keratoconus With New Dynamic Biomechanical In Vivo Scheimpflug Analyses. Cornea 2015, 34, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-García, M.; Dhubhghaill, S.N.; Koppen, C.; Varssano, D.; Rozema, J.J.; The REDCAKE Study Group. Baseline Findings in the Retrospective Digital Computer Analysis of Keratoconus Evolution (REDCAKE) Project. Cornea 2020, 40, 156–167. [Google Scholar] [CrossRef]
- Colin, J.; Smadja, D.; Touboul, D. Comparative Evaluation of Elevation, Keratometric, Pachymetric and Wavefront Parameters in Normal Eyes, Subclinical Keratoconus and Keratoconus with a Dual Scheimpflug Analyzer. Int. J. Keratoconus Ectatic Corneal Dis. 2012, 1, 158–166. [Google Scholar] [CrossRef]
- Bilen, N.B.; Hepsen, I.F.; Arce, C.G. Correlation between visual function and refractive, topographic, pachymetric and aberrometric data in eyes with keratoconus. Int. J. Ophthalmol. 2016, 9, 1127–1133. [Google Scholar] [CrossRef]
- Shetty, R.; Rao, H.; Khamar, P.; Sainani, K.; Vunnava, K.; Jayadev, C.; Kaweri, L. Keratoconus Screening Indices and Their Diagnostic Ability to Distinguish Normal from Ectatic Corneas. Am. J. Ophthalmol. 2017, 181, 140–148. [Google Scholar] [CrossRef]
- Feizi, S.; Yaseri, M.; Kheiri, B. Predictive ability of galilei to distinguish subclinical keratoconus and keratoconus from normal corneas. J. Ophthalmic Vis. Res. 2016, 11, 8–16. [Google Scholar] [CrossRef]
- Wang, L.; Shirayama, M.; Koch, D.D. Repeatability of corneal power and wavefront aberration measurements with a dual-Scheimpflug Placido corneal topographer. J. Cataract. Refract. Surg. 2010, 36, 425–430. [Google Scholar] [CrossRef]
- Tellouck, J.; Touboul, D.; Santhiago, M.R.; Tellouck, L.; Paya, C.; Smadja, D. Evolution Profiles of Different Corneal Parameters in Progressive Keratoconus. Cornea 2016, 35, 807–813. [Google Scholar] [CrossRef]
- Reddy, J.C.; Rapuano, C.J.; Cater, J.R.; Suri, K.; Nagra, P.K.; Hammersmith, K.M. Comparative evaluation of dual Scheimpflug imaging parameters in keratoconus, early keratoconus, and normal eyes. J. Cataract. Refract. Surg. 2014, 40, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Moshirfar, M.; Motlagh, M.N.; Murri, M.S.; Momeni-Moghaddam, H.; Ronquillo, Y.C.; Hoopes, P.C. Galilei Corneal Tomography for Screening of Refractive Surgery Candidates: A Review of the Literature, Part II. Med. Hypothesis, Discov. Innov. Ophthalmol. 2019, 8, 204–218. [Google Scholar]
- Mahmoud, A.M.; Nuñez, M.X.; Blanco, C.; Koch, D.D.; Wang, L.; Weikert, M.P.; Frueh, B.E.; Tappeiner, C.; Twa, M.D.; Roberts, C.J. Expanding the Cone Location and Magnitude Index to Include Corneal Thickness and Posterior Surface Information for the Detection of Keratoconus. Am. J. Ophthalmol. 2013, 156, 1102–1111. [Google Scholar] [CrossRef]
- Savini, G.; Barboni, P.; Carbonelli, M.; Hoffer, K.J. Repeatability of automatic measurements by a new Scheimpflug camera combined with Placido topography. J. Cataract. Refract. Surg. 2011, 37, 1809–1816. [Google Scholar] [CrossRef] [PubMed]
- Altinkurt, E.; Avci, O.; Muftuoglu, O.; Ugurlu, A.; Cebeci, Z.; Ozbilen, K.T. Logistic Regression Model Using Scheimpflug-Placido Cornea Topographer Parameters to Diagnose Keratoconus. J. Ophthalmol. 2021, 2021, 5528927. [Google Scholar] [CrossRef]
- Salman, A.; Darwish, T.; Ali, A.; Ghabra, M.; Shaaban, R. Sensitivity and specificity of Sirius indices in diagnosis of keratoconus and suspect keratoconus. Eur. J. Ophthalmol. 2022, 32, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Safarzadeh, M.; Nasiri, N. Anterior segment characteristics in normal and keratoconus eyes evaluated with a combined Scheimpflug/Placido corneal imaging device. J. Curr. Ophthalmol. 2016, 28, 106–111. [Google Scholar] [CrossRef]
- Asam, J.S.; Polzer, M.; Tafreshi, A.; Hirnschall, N.; Findl, O. Anterior segment OCT. In High Resolution Imaging in Microscopy and Ophthalmology; Springer: Cham, Switzerland, 2019; pp. 285–299. [Google Scholar]
- Li, Y.; Meisler, D.M.; Tang, M.; Lu, A.T.; Thakrar, V.; Reiser, B.J.; Huang, D. Keratoconus Diagnosis with Optical Coherence Tomography Pachymetry Mapping. Ophthalmology 2008, 115, 2159–2166. [Google Scholar] [CrossRef]
- Yang, Y.; Pavlatos, E.; Chamberlain, W.; Huang, D.; Li, Y. Keratoconus detection using OCT corneal and epithelial thickness map parameters and patterns. J. Cataract. Refract. Surg. 2021, 47, 759–766. [Google Scholar] [CrossRef]
- Pavlatos, E.; Harkness, B.; Louie, D.; Chamberlain, W.; Huang, D.; Li, Y. Differentiating Between Contact Lens Warpage and Kera-toconus Using OCT Maps of Corneal Mean Curvature and Epithelial Thickness. J. Refract. Surg. 2022, 38, 112–119. [Google Scholar] [CrossRef]
- Doroodgar, F.; Jabbarvand, M.; Niazi, S.; Karimian, F.; Niazi, F.; Sanginabadi, A.; Ghoreishi, M.; Alinia, C.; Hashemi, H.; Alió, J.L. Customized Stromal Lenticule Implantation for Keratoconus. J. Refract. Surg. 2020, 36, 786–794. [Google Scholar] [CrossRef] [PubMed]
- Kanellopoulos, J.; Aslanides, I.; Asimelis, G. Correlation between epithelial thickness in normal corneas, untreated ectatic corneas, and ectatic corneas previously treated with CXL; is overall epithelial thickness a very early ectasia prognostic factor? Clin. Ophthalmol. 2012, 6, 789–800. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, Q. Investigation of the Human Anterior Segment in Normal Chinese Subjects Using a Dual Scheimpflug Analyzer. Ophthalmology 2013, 120, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Yousefi, S.; Yousefi, E.; Takahashi, H.; Hayashi, T.; Tampo, H.; Inoda, S.; Arai, Y.; Asbell, P. Keratoconus severity identification using unsupervised machine learning. PLoS ONE 2019, 13, e0205998. [Google Scholar] [CrossRef]
- Yousefi, S.; Takahashi, H.; Hayashi, T.; Tampo, H.; Inoda, S.; Arai, Y.; Tabuchi, H.; Asbell, P. Predicting the likelihood of need for future keratoplasty intervention using artificial intelligence. Ocul. Surf. 2020, 18, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Lu, M.N.-J.; Elsheikh, A.; Rozema, M.J.J.; Hafezi, N.; Aslanides, I.M.; Hillen, M.; Eckert, M.D.; Funck, M.C.; Koppen, C.; Cui, L.-L.; et al. Combining Spectral-Domain OCT and Air-Puff Tonometry Analysis to Diagnose Keratoconus. J. Refract. Surg. 2022, 38, 374–380. [Google Scholar] [CrossRef]
- Li, D.F.; Dong, Y.L.; Xie, S.; Guo, Z.; Li, S.X.; Guo, Y.; Lyu, B.; Xie, L.X. Deep learning based lesion detection from anterior segment optical coherence tomography images and its application in the diagnosis of keratoconus. Chin. J. Ophthalmol. 2021, 57, 447–453. [Google Scholar] [CrossRef]
- Esporcatte, L.P.G.; Salomão, M.Q.; Lopes, B.T.; Vinciguerra, P.; Vinciguerra, R.; Roberts, C.; Elsheikh, A.; Dawson, D.G.; Jr, R.A. Biomechanical diagnostics of the cornea. Eye Vis. 2020, 7, 9. [Google Scholar] [CrossRef]
- Schweitzer, C.; Roberts, C.J.; Mahmoud, A.M.; Colin, J.; Maurice-Tison, S.; Kerautret, J. Screening of Forme Fruste Keratoconus with the Ocular Response Analyzer. Investig. Ophthalmol. Vis. Sci. 2010, 51, 2403–2410. [Google Scholar] [CrossRef]
- Ventura, B.V.; Machado, A.P.; Ambrósio, R.; Ribeiro, G.; Araújo, L.N.; Luz, A.; Lyra, J.M. Analysis of Waveform-Derived ORA Parameters in Early Forms of Keratoconus and Normal Corneas. J. Refract. Surg. 2013, 29, 637–643. [Google Scholar] [CrossRef]
- Luz, A.; Lopes, B.; Hallahan, K.M.; Valbon, B.; Ramos, I.; Faria-Correia, F.; Schor, P.; Dupps, W.; Ambrósio, R. Enhanced Combined Tomography and Biomechanics Data for Distinguishing Forme Fruste Keratoconus. J. Refract. Surg. 2016, 32, 479–494. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Xu, J.; Wei, A.; Deng, S.X.; Cui, X.; Yu, X.; Sun, X. A New Tonometer—The Corvis ST Tonometer: Clinical Comparison with Noncontact and Goldmann Applanation Tonometers. Investig. Ophthalmol. Vis. Sci. 2013, 54, 659–665. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Xu, L.; Fan, Q.; Zhao, D.; Ren, S. Repeatability and comparison of new Corvis ST parameters in normal and keratoconus eyes. Sci. Rep. 2019, 9, 15379. [Google Scholar] [CrossRef] [PubMed]
- Vinciguerra, R.; Ambrósio, R.; Elsheikh, A.; Roberts, C.J.; Lopes, B.; Morenghi, E.; Azzolini, C.; Vinciguerra, P. Detection of Keratoconus With a New Biomechanical Index. J. Refract. Surg. 2016, 32, 803–810. [Google Scholar] [CrossRef] [PubMed]
- Ambrósio, R., Jr.; Nogueira, L.P.; Caldas, D.L.; Fontes, B.M.; Luz, A.; Cazal, J.O.; Alves, M.R.; Belin, M.W. Evaluation of corneal shape and biomechanics before LASIK. Int. Ophthalmol. Clin. 2011, 51, 11–38. [Google Scholar] [CrossRef]
- Flockerzi, E.; Vinciguerra, R.; Belin, M.W.; Vinciguerra, P.; Ambrósio, R., Jr.; Seitz, B. Combined biomechanical and tomographic ker-atoconus staging: Adding a biomechanical parameter to the ABCD keratoconus staging system. Acta Ophthalmol. 2022, 100, e1135–e1142. [Google Scholar] [CrossRef]
- Flockerzi, E.; Vinciguerra, R.; Belin, M.W.; Vinciguerra, P.; Ambrósio, R.J.; Seitz, B. Correlation of the Corvis Biomechanical Factor with tomographic parameters in keratoconus. J. Cataract. Refract. Surg. 2022, 48, 215–221. [Google Scholar] [CrossRef]
- Yang, K.; Xu, L.; Fan, Q.; Gu, Y.; Song, P.; Zhang, B.; Zhao, D.; Pang, C.; Ren, S. Evaluation of new Corvis ST parameters in normal, Post-LASIK, Post-LASIK keratectasia and keratoconus eyes. Sci. Rep. 2020, 10, 5676. [Google Scholar] [CrossRef]
- Herber, R.; Pillunat, L.E.; Raiskup, F. Development of a classification system based on corneal biomechanical properties using artificial intelligence predicting keratoconus severity. Eye Vis. 2021, 8, 21. [Google Scholar] [CrossRef]
- Yu, J.-H.; Ji, C.-H.; Li, T.-J.; Tian, L.; Huang, Y.-F.; Wang, Y.-Y.; Zheng, Y.-P. Extracting features from normal corneas and keratoconus based on wavelet analysis. Opt. Precis. Eng. 2015, 23, 2919–2926. [Google Scholar] [CrossRef]
- Karimi, A.; Meimani, N.; Razaghi, R.; Rahmati, S.M.; Jadidi, K.; Rostami, M. Biomechanics of the Healthy and Keratoconic Corneas: A Combination of the Clinical Data, Finite Element Analysis, and Artificial Neural Network. Curr. Pharm. Des. 2018, 24, 4474–4483. [Google Scholar] [CrossRef]
- Scarcelli, G.; Pineda, R.; Yun, S.H. Brillouin Optical Microscopy for Corneal Biomechanics. Investig. Ophthalmol. Vis. Sci. 2012, 53, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Seiler, T.G.; Shao, P.; Eltony, A.; Yun, S.-H. Brillouin Spectroscopy of Normal and Keratoconus Corneas. Am. J. Ophthalmol. 2019, 202, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Eliasy, A.; Lopes, B.; Abass, A.; Vinciguerra, R.; Vinciguerra, P.; Ambrósio, R.J.; Roberts, C.J.; Elsheikh, A. Stress–Strain Index Map: A New Way to Represent Corneal Material Stiffness. Front. Bioeng. Biotechnol. 2021, 9, 155. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.; Guilbert, E.; Gatinel, D. Corneal Enantiomorphism in Normal and Keratoconic Eyes. J. Refract. Surg. 2014, 30, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, P.; Ramesh, G.P. Diagnosis of Keratoconus with Corneal Features Obtained through LBP, LDP, LOOP, and CSO. Trends Sci. 2021, 18, 22. [Google Scholar] [CrossRef]
- Malyugin, B.; Sakhnov, S.; Izmailova, S.; Boiko, E.; Pozdeyeva, N.; Axenova, L.; Axenov, K.; Titov, A.; Terentyeva, A.; Zakaraiia, T.; et al. Keratoconus Diagnostic and Treatment Algorithms Based on Machine-Learning Methods. Diagnostics 2021, 11, 1933. [Google Scholar] [CrossRef]
- Ahn, H.; Kim, N.E.; Chung, J.L.; Kim, Y.J.; Jun, I.; Kim, T.-I.; Seo, K.Y. Patient Selection for Corneal Topographic Evaluation of Keratoconus: A Screening Approach Using Artificial Intelligence. Front. Med. 2022, 9, 934865. [Google Scholar] [CrossRef]
- Firat, M.; Cankaya, C.; Cinar, A.; Tuncer, T. Automatic Detection of Keratoconus on Pentacam Images Using Feature Selection Based on Deep Learning. Int. J. Imaging Syst. Technol. 2022, 32, 1548–1560. [Google Scholar] [CrossRef]
- Feng, R.; Xu, Z.; Zheng, X.; Hu, H.; Jin, X.; Chen, D.Z.; Yao, K.; Wu, J. KerNet: A Novel Deep Learning Approach for Keratoconus and Sub-Clinical Keratoconus Detection Based on Raw Data of the Pentacam HR System. IEEE J. Biomed. Health Inform. 2021, 25, 3898–3910. [Google Scholar] [CrossRef]
- Xu, Z.; Feng, R.; Jin, X.; Hu, H.; Ni, S.; Xu, W.; Zheng, X.; Wu, J.; Yao, K. Evaluation of Artificial Intelligence Models for the Detection of Asymmetric Keratoconus Eyes Using Scheimpflug Tomography. Clin. Exp. Ophthalmol. 2022, 50, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.B.; Pan, Z.G.; Shen, M.X.; Lu, F.; Li, H.; Zhang, X.Q. KeratoScreen: Early Keratoconus Classification with Zernike Polynomial Using Deep Learning. Cornea 2022, 41, 1158–1165. [Google Scholar] [CrossRef] [PubMed]
- Almeida, G.C.; Guido, R.C.; Balarin Silva, H.M.; Brandão, C.C.; de Mattos, L.C.; Lopes, B.T.; Machado, A.P.; Ambrósio, R.J. New Artificial Intelligence Index Based on Scheimpflug Corneal Tomography to Distinguish Subclinical Keratoconus from Healthy Corneas. J. Cataract. Refract. Surg. 2022, 48, 1168–1174. [Google Scholar] [CrossRef] [PubMed]
- Lopes, B.T.; Ramos, I.C.; Salomão, M.Q.; Canedo, A.L.C.; Ambrósio, R., Jr. Horizontal Pachymetric Profile for the Detection of Keratoconus. Rev. Bras. Oftalmol. 2015, 74, 382–385. [Google Scholar] [CrossRef]
- Tan, Z.; Chen, X.; Li, K.; Liu, Y.; Cao, H.; Li, J.; Jhanji, V.; Zou, H.; Liu, F.; Wang, R.; et al. Artificial Intelligence-Based Diagnostic Model for Detecting Keratoconus Using Videos of Corneal Force Deformation. Transl. Vis. Sci. Technol. 2022, 11, 32. [Google Scholar] [CrossRef] [PubMed]
- Alazzam, M.B.; Alghamdi, A.S.; Alshamrani, S.S. Corneal Biomechanics Computational Analysis for Keratoconus Diagnosis. Comput. Math. Methods Med. 2021, 2021, 6126503. [Google Scholar] [CrossRef]
- Levy, A.; Georgeon, C.; Knoeri, J.; Tourabaly, M.; Leveziel, L.; Bouheraoua, N.; Borderie, V.M. Corneal Epithelial Thickness Mapping in the Diagnosis of Ocular Surface Disorders Involving the Corneal Epithelium: A Comparative Study. Cornea 2022, 41, 1353–1361. [Google Scholar] [CrossRef]
- Shanthi, S.; Aruljyothi, L.; Balasundaram, M.B.; Janakiraman, A.; Nirmala, D.K.; Pyingkodi, M. Artificial intelligence applications in different imaging modalities for corneal topography. Surv. Ophthalmol. 2021, 67, 801–816. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Corvis ST Parameters | ||
|---|---|---|
| Parameters | Abbreviation | Description |
| Biomechanically corrected intraocular pressure | bIOP | Derived by finite element simulations that take into account the influence of central corneal thickness, age, and dynamic corneal response (DCR) parameters |
| First applanation | A1 | Moment at the first applanation of the cornea during the air puff |
| A1 time (ms) | A1T(T1) | Time from start to A1 |
| A1 velocity (m/s) | A1V(V1) | Velocity (speed) of corneal apex at A1 |
| A1 deformation amplitude | A1DA | Moving distance of the corneal apex from the initial position to that at the A1 time |
| A1 deflection length | A1DL | Length of the flattened cornea at A1 |
| A1 deflection amplitude | A1DeflA, A1DLA | After approaching the highest displacement secondary to WEM, the whole eye displays a nonlinear motion in the ant–post direction, so A1DeflA is similar to A1DA without WEM |
| A1 delta arc length | A1dArclength, A1dArcL | Change in arc length from the initial state to A1, in a defined 7 mm zone |
| Second applanation | A2 | Moment at the first applanation of the cornea during the air puff |
| A2 time (ms) | A2T(T2) | Time from start to A2 |
| A2 velocity (m/s) | A2V | Speed of corneal apex at A2 |
| A2 deformation amplitude | A2DA | Moving distance of the corneal apex from the initial position to that at A2 time |
| A2 deflection length | A2DL | Length of the flattened cornea at A2 |
| A2 deflection amplitude | A2DeflA, A2DLA | Similar to A2DA without whole eye movement |
| A2 delta arc length | A2dArclength, A2dArcL | Change in arc length from the initial state to A2, in a defined 7 mm zone |
| Highest (maximum) concavity | HC, MC | Moment that the cornea assumes its maximum concavity during the air puff |
| HC time | HCT | Time to reach the maximum deformation |
| Radius (mm) | Rad | Central curvature radius at the HC state secondary to parabolic fit |
| HC (Max) deformation amplitude | HCDA, MDA | Maximum depth of ant–post corneal displacement at the moment of maximum concavity |
| HC deflection length | HCDL | Length of the flattened cornea at highest concavity |
| HC deflection amplitude | HCDeflA, HCDLA | “Displaced” area of the cornea in the horizontal plane secondary to corneal deformation |
| Peak distance | PD | Distance between the two peaks of the cornea in temporal–nasal direction at the maximum concavity state, which is not the same as the deflection length |
| HC delta Arc length | HCdArclength | Change in arc length in a defined 7 mm zone during HC from the initial state |
| Maximum | Max | Similar to HC |
| Max deformation amplitude | Max DA | Distance of the corneal apex movement from the initiation of the deformation to the HC |
| Max deflection amplitude | Max DeflA | Ratio between the deformation/deflection amplitude at the apex and the average deformation/deflection amplitude in a nasal and temporal zone 1 or 2 mm (2 mm for DefA ratio) from the center; higher values (greater 1) of DA Ratio and DefA Ratio can be associated with less resistant corneas |
| Max delta arc length | MaxdArclength | Change in arc length during the highest concavity moment from the initial state, in a 7 mm with horizontal direction (3.5 mm from the apex to both sides) |
| Vinciguerra screening parameters (VSP) | ||
| Deformation amplitude ratio max (2 mm) | DA ratio max(DAR2mm) | Ratio between the deformation amplitude at the apex and the average deformation amplitude measured at 2 mm central–peripheral |
| Ambrósio’s relational thickness to the horizontal profile | ARTh | Ratio between the deformation amplitude at the apex and the average deformation amplitude measured at 2 mm from the center |
| Integrated radius | INR(IR) | Area under the inverse concave radius vs. time curve; in fact, 1/R is plotted during the time of an air pulse and is entirely measured between the period of first and second applanations |
| Stiffness parameter at A1 | SP-A1 | Corneal stiffness at A1, the ratio of resultant pressure to deflection amplitude |
| Corvis biomechanical index | CBI | Overall biomechanical index for keratoconus detection |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niazi, S.; Jiménez-García, M.; Findl, O.; Gatzioufas, Z.; Doroodgar, F.; Shahriari, M.H.; Javadi, M.A. Keratoconus Diagnosis: From Fundamentals to Artificial Intelligence: A Systematic Narrative Review. Diagnostics 2023, 13, 2715. https://doi.org/10.3390/diagnostics13162715
Niazi S, Jiménez-García M, Findl O, Gatzioufas Z, Doroodgar F, Shahriari MH, Javadi MA. Keratoconus Diagnosis: From Fundamentals to Artificial Intelligence: A Systematic Narrative Review. Diagnostics. 2023; 13(16):2715. https://doi.org/10.3390/diagnostics13162715
Chicago/Turabian StyleNiazi, Sana, Marta Jiménez-García, Oliver Findl, Zisis Gatzioufas, Farideh Doroodgar, Mohammad Hasan Shahriari, and Mohammad Ali Javadi. 2023. "Keratoconus Diagnosis: From Fundamentals to Artificial Intelligence: A Systematic Narrative Review" Diagnostics 13, no. 16: 2715. https://doi.org/10.3390/diagnostics13162715
APA StyleNiazi, S., Jiménez-García, M., Findl, O., Gatzioufas, Z., Doroodgar, F., Shahriari, M. H., & Javadi, M. A. (2023). Keratoconus Diagnosis: From Fundamentals to Artificial Intelligence: A Systematic Narrative Review. Diagnostics, 13(16), 2715. https://doi.org/10.3390/diagnostics13162715