
Perilesional Targeted Biopsy Combined with MRI-TRUS Image Fusion-Guided Targeted Prostate Biopsy: An Analysis According to PI-RADS Scores

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
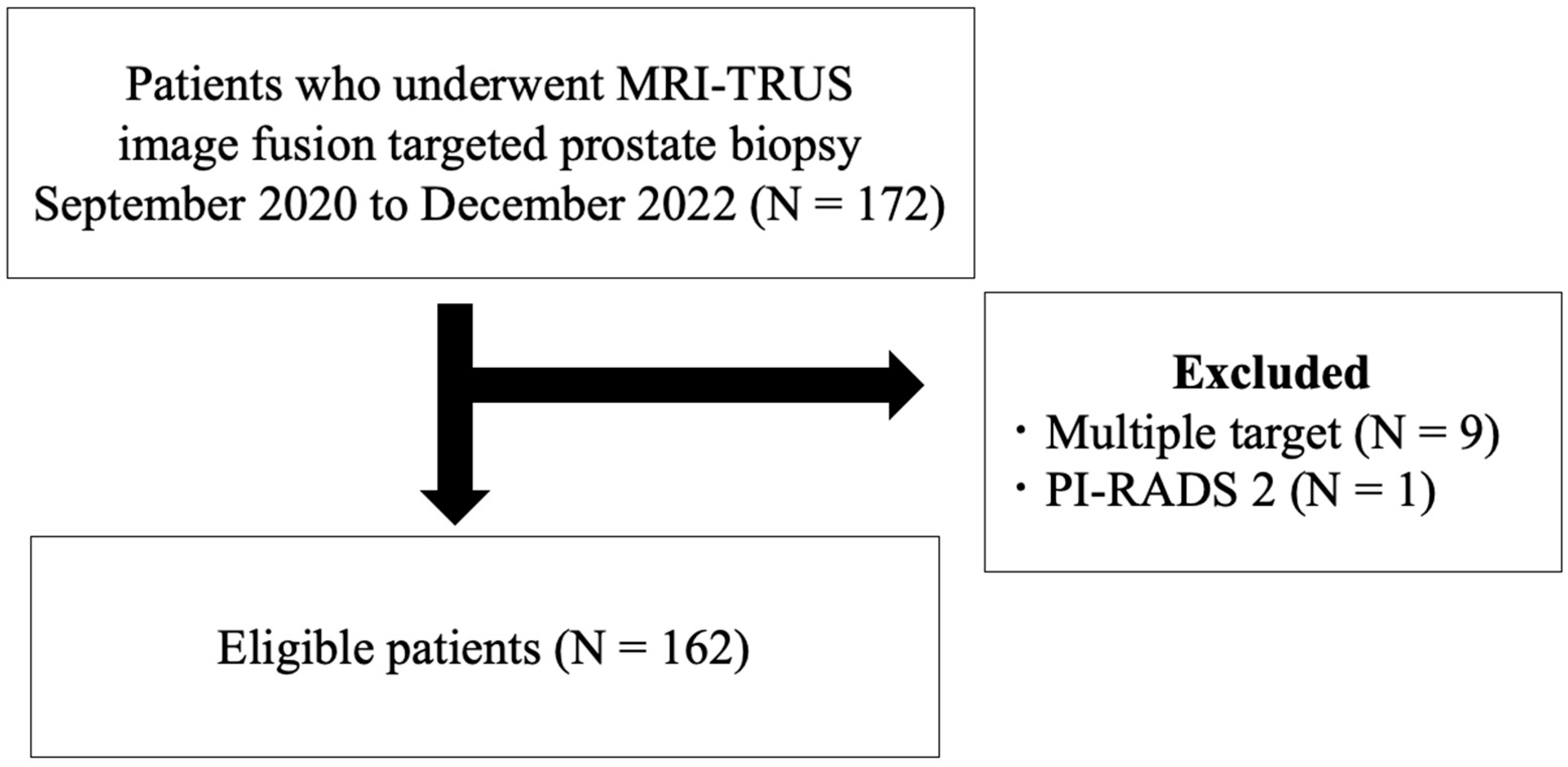
2.1. Patient Population
2.2. Multiparametric Magnetic Resonance Imaging (mpMRI)
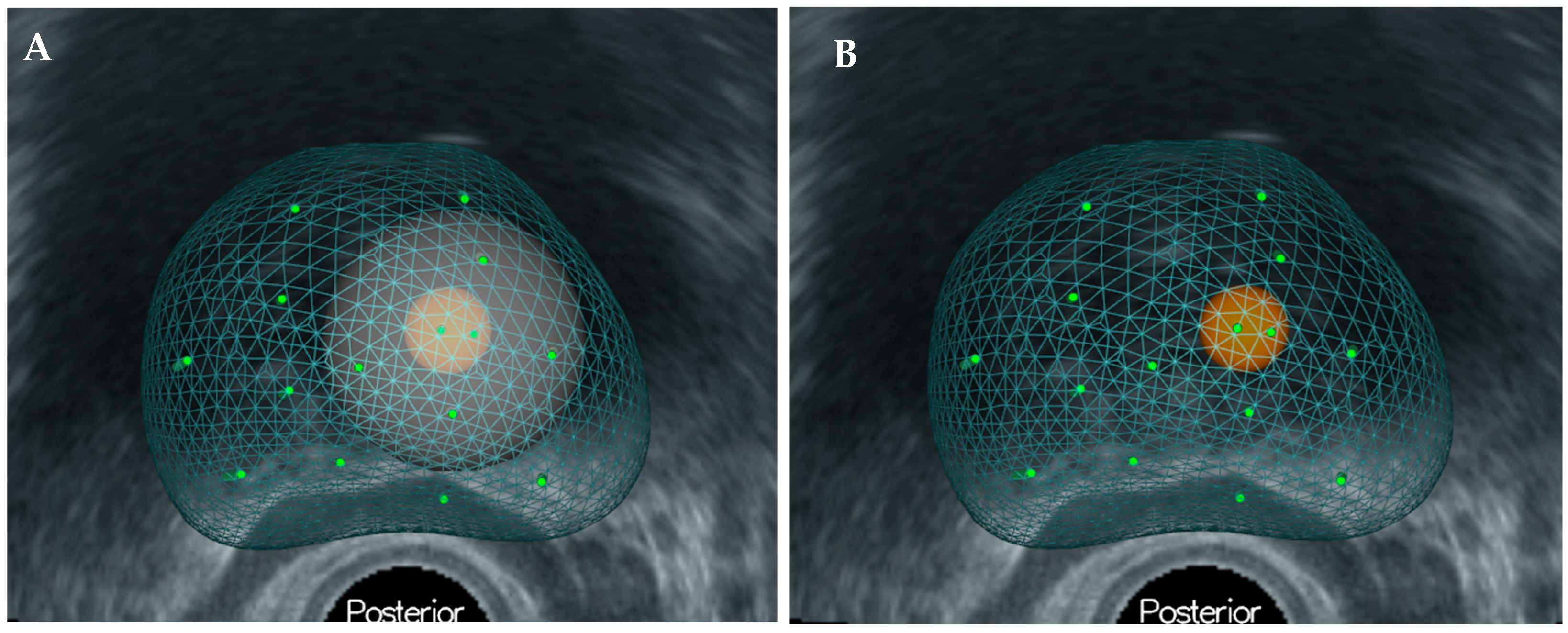
2.3. Prostate Biopsy Protocol
2.4. Pathological Analysis
2.5. Statistical Analysis
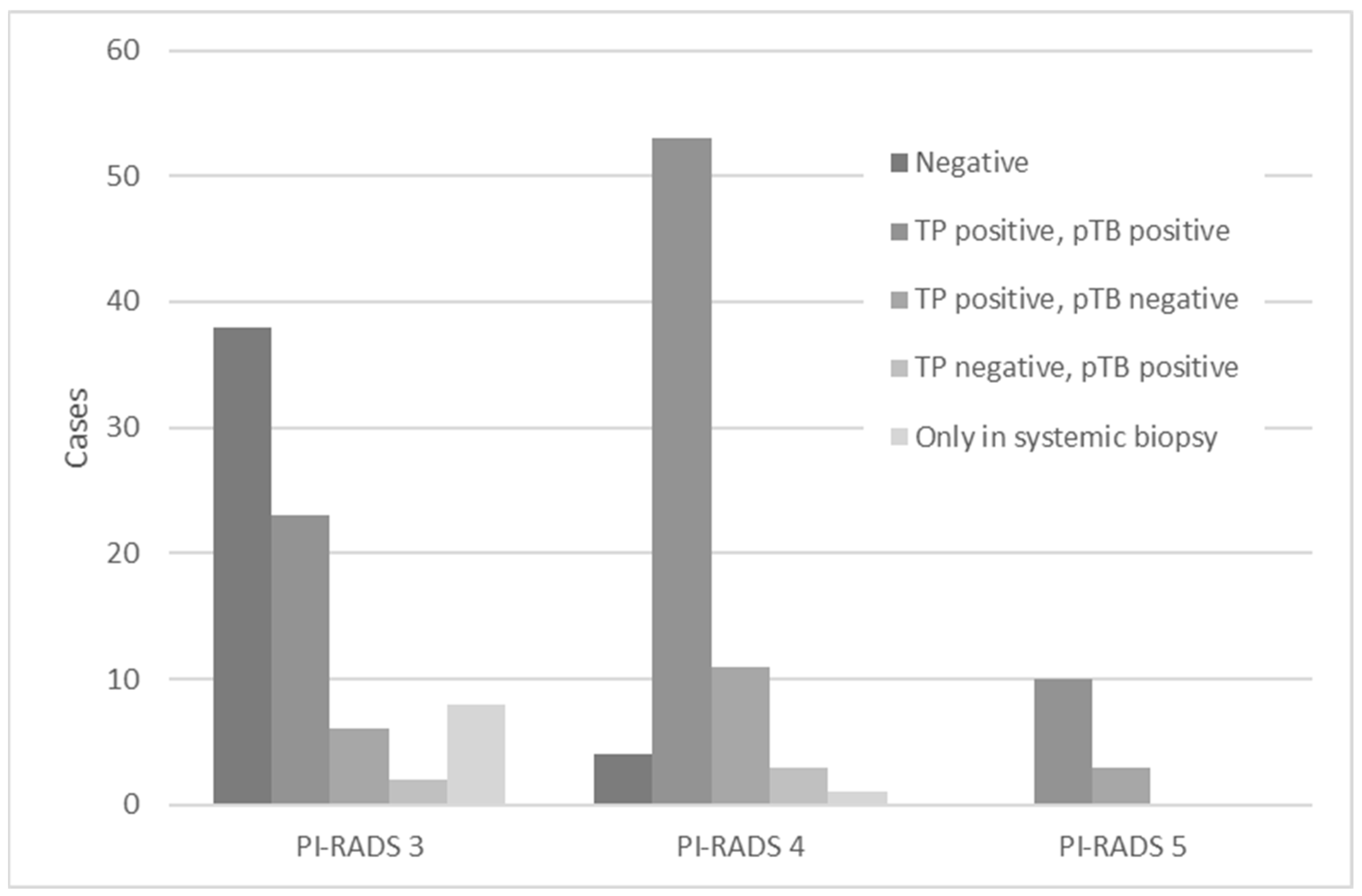
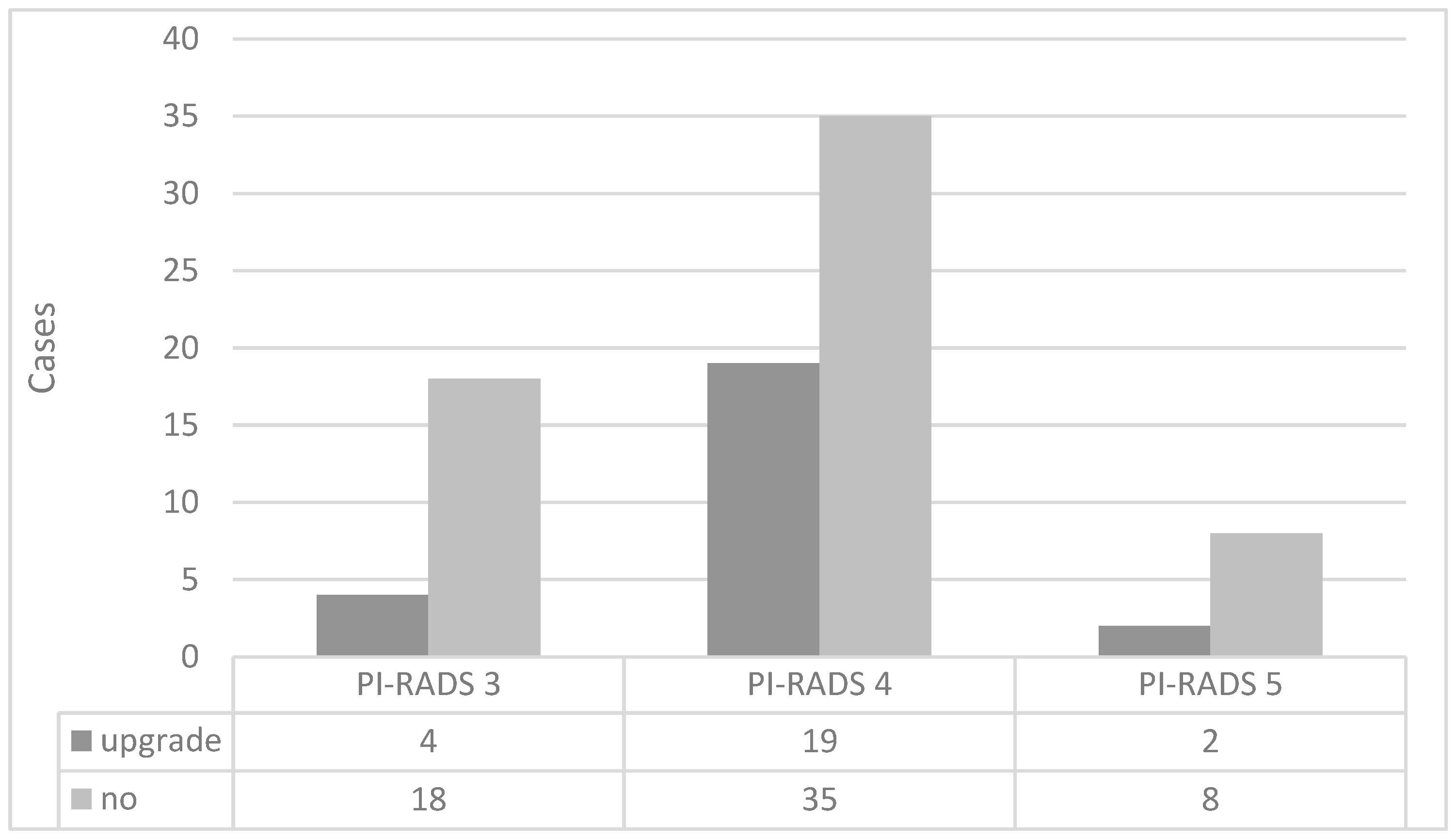
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Uno, H.; Taniguchi, T.; Seike, K.; Kato, D.; Takai, M.; Iinuma, K.; Horie, K.; Nakane, K.; Koie, T. The accuracy of prostate cancer diagnosis in biopsy-naive patients using combined magnetic resonance imaging and transrectal ultrasound fusion-targeted prostate biopsy. Transl. Androl. Urol. 2021, 10, 2982–2989. [Google Scholar] [CrossRef] [PubMed]
- Kato, D.; Ozawa, K.; Takeuchi, S.; Kawase, M.; Kawase, K.; Nakai, C.; Takai, M.; Iinuma, K.; Nakane, K.; Kato, H.; et al. The Utility of Combined Target and Systematic Prostate Biopsies in the Diagnosis of Clinically Significant Prostate Cancer Using Prostate Imaging Reporting and Data System Version 2 Based on Biparametric Magnetic Resonance Imaging. Curr. Oncol. 2021, 28, 1294–1301. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- 5rostate Cancer. NCCN Guidelines®. 2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf (accessed on 30 May 2023).
- Schoots, I.G.; Roobol, M.J.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Hunink, M.G. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: A systematic review and meta-analysis. Eur. Urol. 2015, 68, 438–450. [Google Scholar] [CrossRef] [PubMed]
- Brisbane, W.G.; Priester, A.M.; Ballon, J.; Kwan, L.; Delfin, M.K.; Felker, E.R.; Sisk, A.E.; Hu, J.C.; Marks, L.S. Targeted Prostate Biopsy: Umbra, Penumbra, and Value of Perilesional Sampling. Eur. Urol. 2022, 82, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Priester, A.; Natarajan, S.; Khoshnoodi, P.; Margolis, D.J.; Raman, S.S.; Reiter, R.E.; Huang, J.; Grundfest, W.; Marks, L.S. Magnetic Resonance Imaging Underestimation of Prostate Cancer Geometry: Use of Patient Specific Molds to Correlate Images with Whole Mount Pathology. J. Urol. 2017, 197, 320–326. [Google Scholar] [CrossRef]
- Hagens, M.J.; Salamanca, M.F.; Padhani, A.R.; van Leeuwen, P.J.; van der Poel, H.G.; Schoots, I.G. Diagnostic Performance of a Magnetic Resonance Imaging-directed Targeted plus Regional Biopsy Approach in Prostate Cancer Diagnosis: A Systematic Review and Meta-analysis. Eur. Urol. Open Sci. 2022, 40, 95–103. [Google Scholar] [CrossRef] [PubMed]
- van der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Multicenter Clinical Study. Eur. Urol. 2019, 75, 570–578. [Google Scholar]
- Tschirdewahn, S.; Wiesenfarth, M.; Bonekamp, D.; Püllen, L.; Reis, H.; Panic, A.; Kesch, C.; Darr, C.; Heß, J.; Giganti, F.; et al. Detection of Significant Prostate Cancer Using Target Saturation in Transperineal Magnetic Resonance Imaging/Transrectal Ultrasonography–Fusion Biopsy. Eur. Urol. Focus 2021, 7, 1300–1307. [Google Scholar] [CrossRef]
- Lahoud, J.; Doan, P.; Kim, L.; Patel, M.I. Perilesional Biopsies Increase Detection of Significant Prostate Cancer in Men with PI-RADS 4/5 Lesions: Validation of the PI-RADS Steering Committee Recommendation. Eur. Urology. 2021, 80, 260–261. [Google Scholar] [CrossRef] [PubMed]
- Padhani, A.R.; Weinreb, J.; Rosenkrantz, A.B.; Villeirs, G.; Turkbey, B.; Barentsz, J. Prostate Imaging-Reporting and Data System Steering Committee: PI-RADS v2 Status Update and Future Directions. Eur. Urol. 2019, 75, 385–396. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Kato, D.; Ebara, S.; Tatenuma, T.; Sasaki, T.; Ikehata, Y.; Nakayama, A.; Toide, M.; Yoneda, T.; Sakaguchi, K.; Teishima, J.; et al. Short-term oncological and surgical outcomes of robot-assisted radical prostatectomy: A retrospective multicenter cohort study in Japan (the MSUG94 group). Asian J. Endosc. Surg. 2022, 15, 745–752. [Google Scholar] [CrossRef]
- Iinuma, K.; Nakano, M.; Kato, T.; Kato, D.; Takai, M.; Maekawa, Y.M.; Nakane, K.; Mizutani, K.; Tsuchiya, T.; Ishihara, T.; et al. Assessment of Long-term Changes in Lower Urinary Tract Symptoms in Patients With Prostate Cancer Who Underwent Low-dose-rate Prostate Brachytherapy. Urology 2020, 142, 213–220. [Google Scholar] [CrossRef]
- Noguchi, M.; Stamey, T.A.; McNeal, J.E.; Nolley, R. Prognostic Factors for Multifocal Prostate Cancer in Radical Prostatectomy Specimens: Lack of Significance of Secondary Cancers. J. Urol. 2003, 170, 459–463. [Google Scholar] [CrossRef]
- Wise, A.M.; Stamey, T.A.; McNeal, J.E.; Clayton, J.L. Morphologic and Clinical Significance of Multifocal Prostate Cancers in Radical Prostatectomy Specimens. Urology 2002, 60, 264–269. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Okamoto, A.; Imai, A.; Yoneyama, T.; Hatakeyama, S.; Yoneyama, T.; Koie, T.; Kamimura, N.; Ohyama, C. Biochemical outcome of small-volume or insignificant prostate cancer treated with radical prostatectomy in Japanese population. Int. J. Clin. Oncol. 2012, 17, 119–123. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic Accuracy of Multi-Parametric MRI and TRUS Biopsy in Prostate Cancer (PROMIS): A Paired Validating Confirmatory Study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Hugosson, J.; Månsson, M.; Wallström, J.; Axcrona, U.; Carlsson, S.V.; Egevad, L.; Kjell Geterud, K.; Khatami, A.; Kimia Kohestani, K.; Pihl, C.G.; et al. Prostate Cancer Screening with PSA and MRI Followed by Targeted Biopsy Only. N. Engl. J. Med. 2022, 387, 2126–2137. [Google Scholar] [CrossRef]
- Franklin, A.; Gianduzzo, T.; Yaxley, J.; Kua, B.; Coughlin, G.; Samaratunga, H.; Gianduzzo, T. Use of a trizonal schema to assess targeting accuracy in prostatic fusion biopsy. BJU Int. 2020, 126, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of Prostate Systematic and Targeted Biopsy on the Basis of Multiparametric MRI in Biopsy-Naive Patients (MRI-FIRST): A Prospective, Multicentre, Paired Diagnostic Study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. [Google Scholar] [CrossRef]
- Radtke, J.P.; Kuru, T.H.; Boxler, S.; Alt, C.D.; Popeneciu, I.V.; Huettenbrink, C.; Klein, T.; Steinemann, S.; Bergstraesser, C.; Roethke, M.; et al. Comparative analysis of transperineal template saturation prostate biopsy versus magnetic resonance imaging targeted biopsy with magnetic resonance imaging-ultrasound fusion guidance. J. Urol. 2015, 193, 87–94. [Google Scholar] [CrossRef]
- Alqahtani, S.; Wei, C.; Zhang, Y.; Szewczyk-Bieda, M.; Wilson, J.; Huang, Z.; Nabi, G. Prediction of prostate cancer Gleason score upgrading from biopsy to radical prostatectomy using pre-biopsy multiparametric MRI PIRADS scoring system. Sci. Rep. 2020, 10, 7722. [Google Scholar] [CrossRef]
- Stabile, A.; Dell’Oglio, P.; De Cobelli, F.; Esposito, A.; Gandaglia, G.; Fossati, N.; Brembilla, G.; Cristel, G.; Cardone, G.; Deho’, F.; et al. Association Between Prostate Imaging Reporting and Data System (PI-RADS) Score for the Index Lesion and Multifocal, Clinically Significant Prostate Cancer. Eur. Urol. Oncol. 2018, 1, 29–36. [Google Scholar] [CrossRef]
- Koie, T.; Mitsuzuka, K.; Narita, S.; Yoneyama, T.; Kawamura, S.; Kaiho, Y.; Tsuchiya, N.; Tochigi, T.; Habuchi, T.; Arai, Y.; et al. A solitary positive prostate cancer biopsy does not predict a unilateral lesion in radical prostatectomy specimens. Scand. J. Urol. 2015, 49, 103–107. [Google Scholar] [CrossRef]
- Jang, W.S.; Koh, D.H.; Kim, J.; Lee, J.S.; Chung, D.Y.; Ham, W.S.; Rha, K.H.; Choi, Y.D. The prognostic impact of downgrading and upgrading from biopsy to radical prostatectomy among men with Gleason score 7 prostate cancer. Prostate 2019, 79, 1805–1810. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.M.; Rais-Bahrami, S.; Truong, H.; Stamatakis, L.; Vourganti, S.; Nix, J.; Hoang, A.N.; Walton-Diaz, A.; Shuch, B.; Weintraub, M.; et al. Magnetic resonance imaging/ultrasound-fusion biopsy significantly upgrades prostate cancer versus systematic 12-core transrectal ultrasound biopsy. Eur. Urol. 2013, 64, 713–719. [Google Scholar] [CrossRef]
- Le, J.D.; Tan, N.; Shkolyar, E.; Lu, D.Y.; Kwan, L.; Marks, L.S.; Huang, J.; Margolis, D.J.; Raman, S.S.; Reiter, R.E. Multifocality and prostate cancer detection by multiparametric magnetic resonance imaging: Correlation with whole-mount histopathology. Eur. Urol. 2015, 67, 569–576. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PI-RADS 3 | PI-RADS 4 | PI-RADS 5 | p | |
|---|---|---|---|---|
| Number of patients (%) | 77 (47.5) | 72 (44.4) | 13 (8.0) | |
| Age (years, median, interquartile range) | 70 (65–75.5) | 71.5 (67–76.75) | 72 (70–76) | 0.326 |
| PSA (ng/mL, median, interquartile range) | 7.44 (4.97–10.39) | 6.56 (5.19–9.67) | 6.35 (5.34–16.15) | 0.689 |
| PV (mL, median, interquartile range) | 45.8 (30.55–64.2) | 32.75 (27.25–44.125) | 35 (26.8–48) | 0.0027 |
| Biopsy core (median, min., max.) | 14 (12, 18) | 14 (11, 16) | 14 (11, 16) | 0.065 |
| Targeted biopsy core (median, min., max.) | 2 (2, 4) | 2 (2, 4) | 2 (2, 4) | 0.650 |
| Perilesional target core (median, min., max.) | 2 (2, 6) | 2 (1, 6) | 2 (2, 3) | 0.258 |
| Systematic biopsy core (median, min., max.) | 10 (5, 12) | 10 (5, 12) | 10 (7, 12) | 0.148 |
| Number of csPC cases (%) | 31 (40.3) | 61 (84.7) | 10 (76.9) | <0.0001 |
| Number pf cisPC cases (%) | 8 (10.4) | 8 (11.1) | 3 (23.1) | 0.413 |
| Number of negative cases (%) | 38 (49.3) | 3 (4.2) | 0 (0) | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomioka, M.; Seike, K.; Uno, H.; Asano, N.; Watanabe, H.; Tomioka-Inagawa, R.; Kawase, M.; Kato, D.; Takai, M.; Iinuma, K.; et al. Perilesional Targeted Biopsy Combined with MRI-TRUS Image Fusion-Guided Targeted Prostate Biopsy: An Analysis According to PI-RADS Scores. Diagnostics 2023, 13, 2608. https://doi.org/10.3390/diagnostics13152608
Tomioka M, Seike K, Uno H, Asano N, Watanabe H, Tomioka-Inagawa R, Kawase M, Kato D, Takai M, Iinuma K, et al. Perilesional Targeted Biopsy Combined with MRI-TRUS Image Fusion-Guided Targeted Prostate Biopsy: An Analysis According to PI-RADS Scores. Diagnostics. 2023; 13(15):2608. https://doi.org/10.3390/diagnostics13152608
Chicago/Turabian StyleTomioka, Masayuki, Kensaku Seike, Hiromi Uno, Nami Asano, Haruo Watanabe, Risa Tomioka-Inagawa, Makoto Kawase, Daiki Kato, Manabu Takai, Koji Iinuma, and et al. 2023. "Perilesional Targeted Biopsy Combined with MRI-TRUS Image Fusion-Guided Targeted Prostate Biopsy: An Analysis According to PI-RADS Scores" Diagnostics 13, no. 15: 2608. https://doi.org/10.3390/diagnostics13152608
APA StyleTomioka, M., Seike, K., Uno, H., Asano, N., Watanabe, H., Tomioka-Inagawa, R., Kawase, M., Kato, D., Takai, M., Iinuma, K., Tobisawa, Y., Nakane, K., Tsuchiya, K., Ito, T., & Koie, T. (2023). Perilesional Targeted Biopsy Combined with MRI-TRUS Image Fusion-Guided Targeted Prostate Biopsy: An Analysis According to PI-RADS Scores. Diagnostics, 13(15), 2608. https://doi.org/10.3390/diagnostics13152608