
Unravelling Peritoneal Carcinomatosis Using Cross-Sectional Imaging Modalities
 ,
,
Abstract
:1. Introduction
2. Diagnostic Modalities
3. Many Places and Many Faces
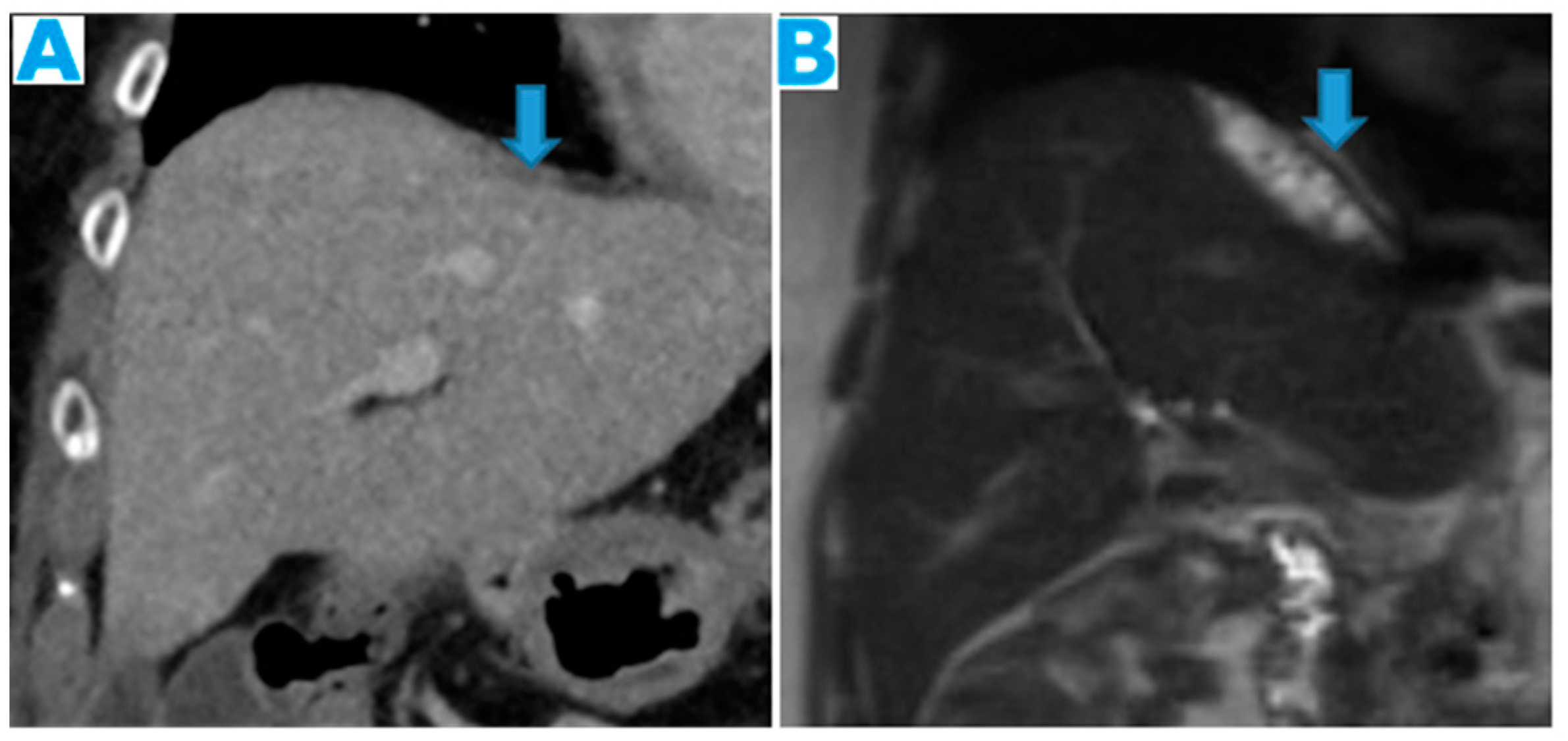
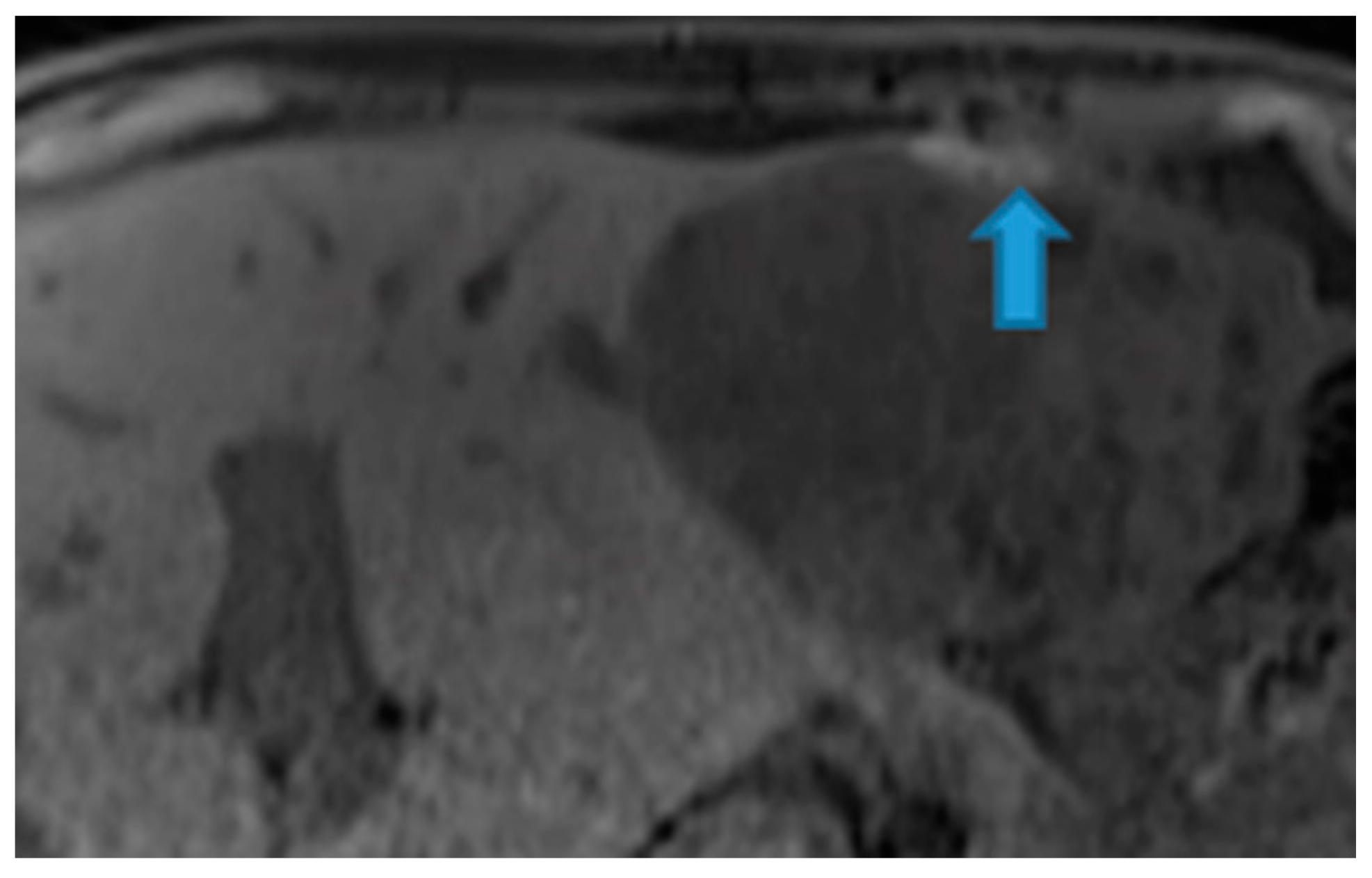
- Cranially, it covers the diaphragm (except for the bare area of the liver, the insertion of the ligaments, and along its posterior margin, where it is in contact with retroperitoneal fat) (Figure 1).
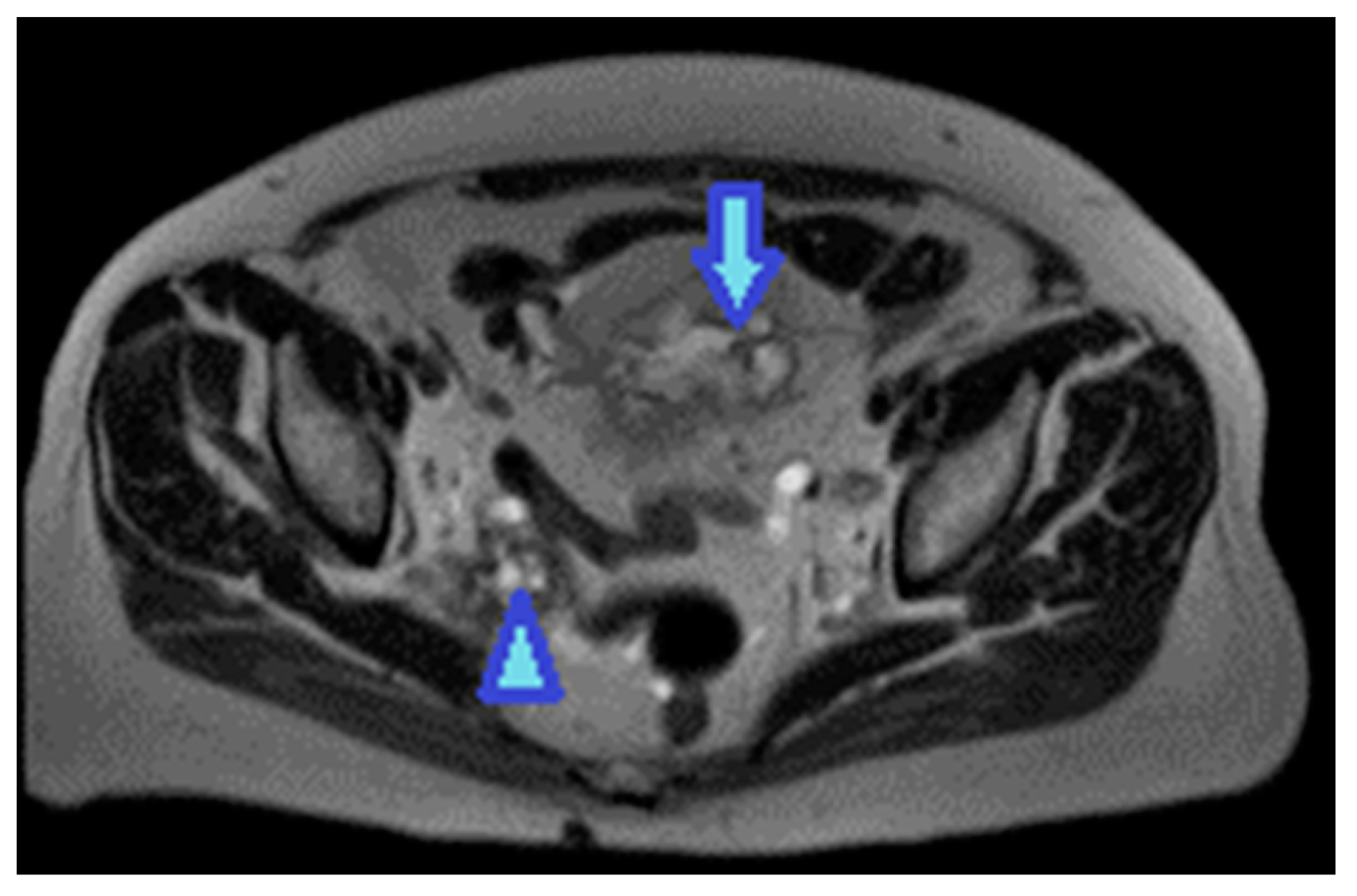
- Caudally, it descends into the pelvis. Its complex anatomy in this location is shown in more detail later.
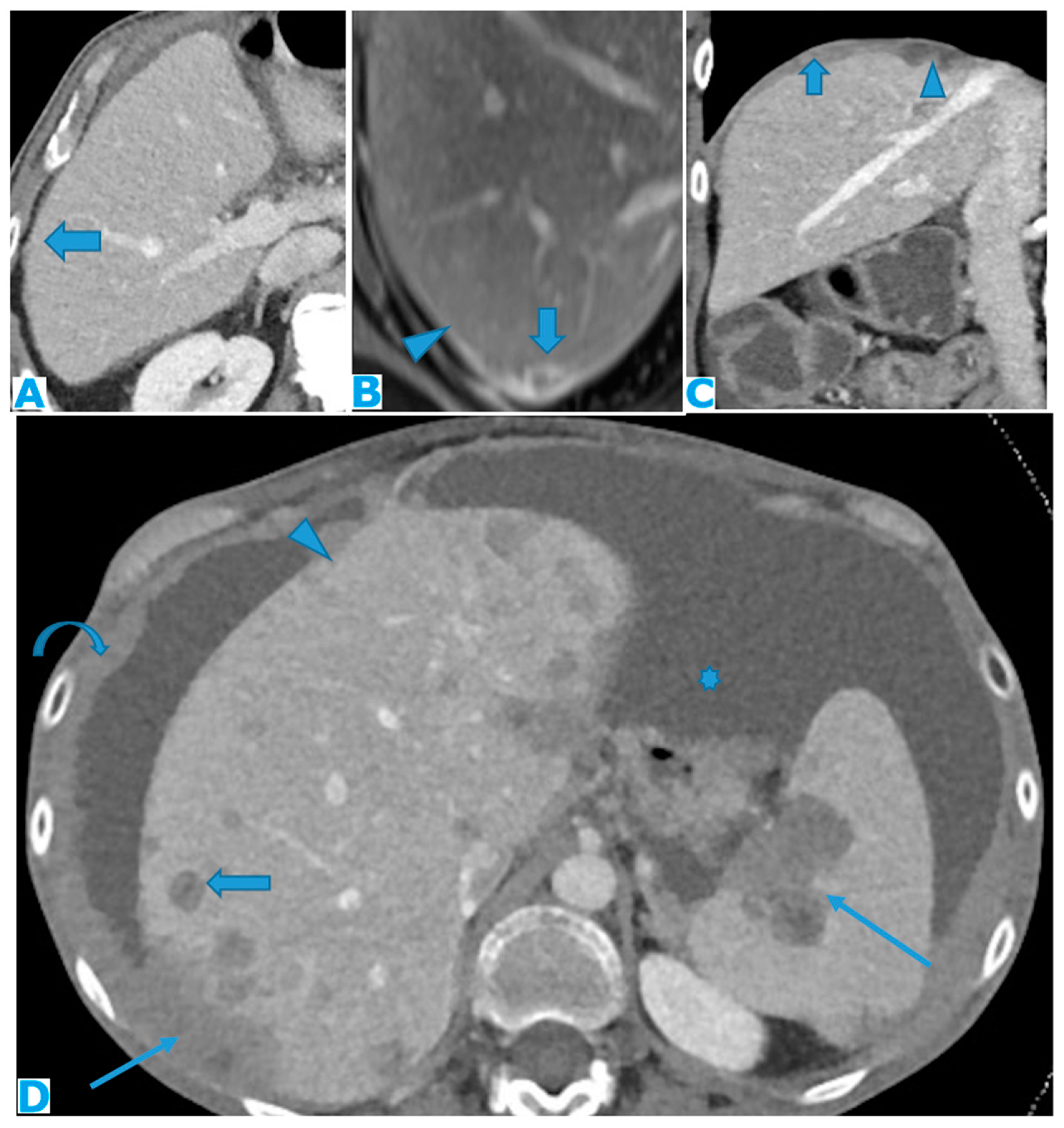
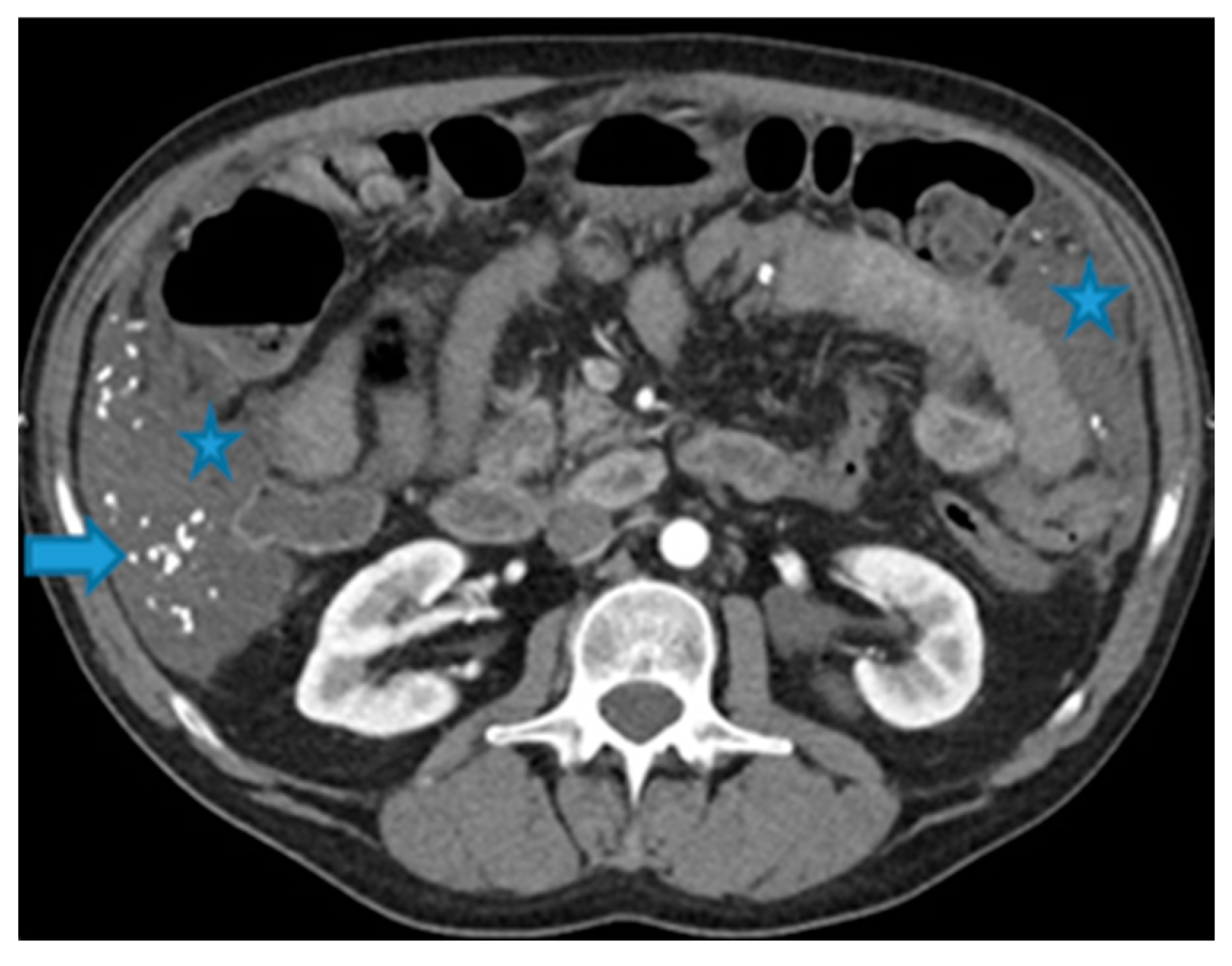
- Anterolaterally, it is separated from the abdominal wall by the fat from the preperitoneal space, that is, the space between the peritoneum and the transversalis fascia (Figure 2).
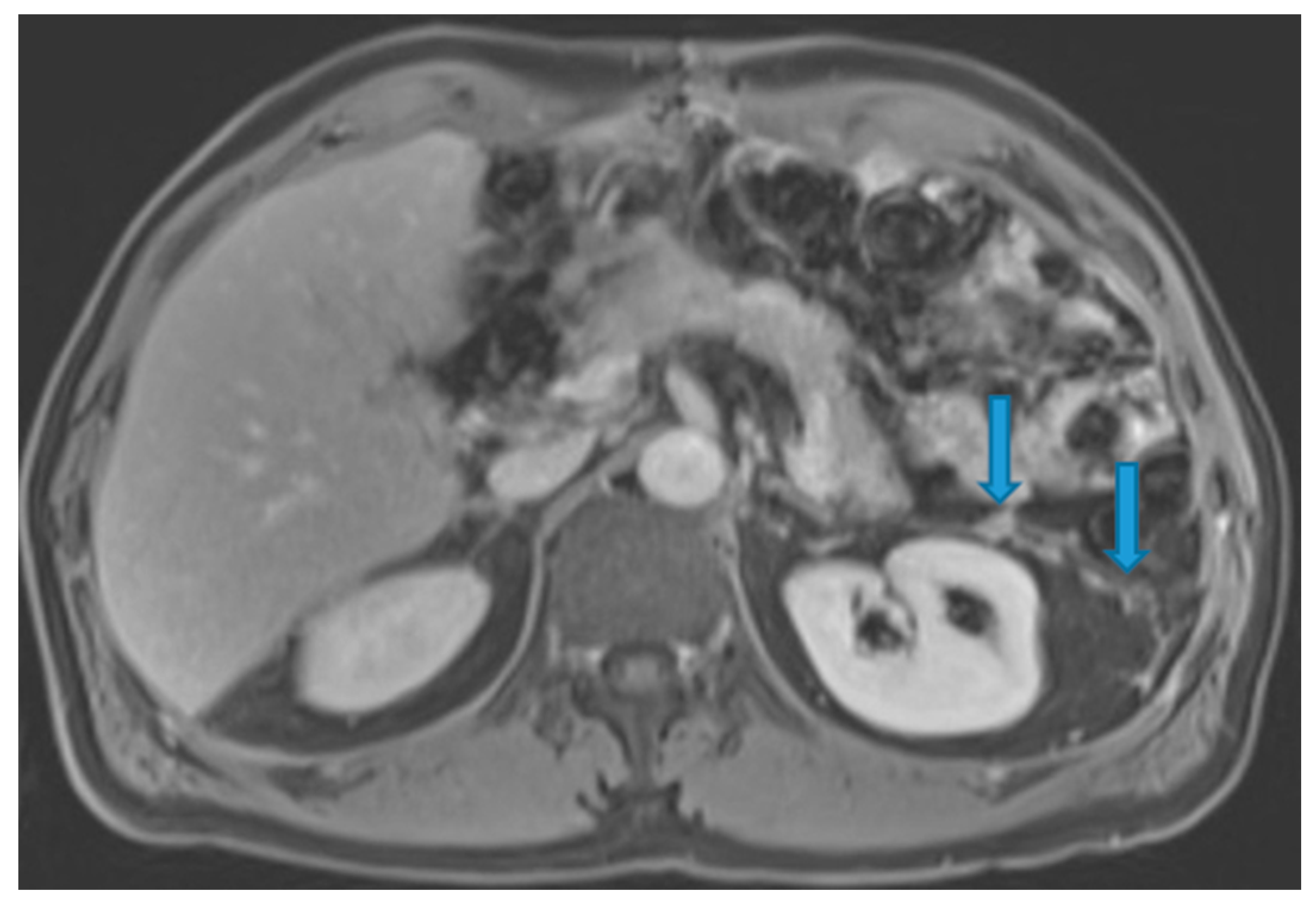
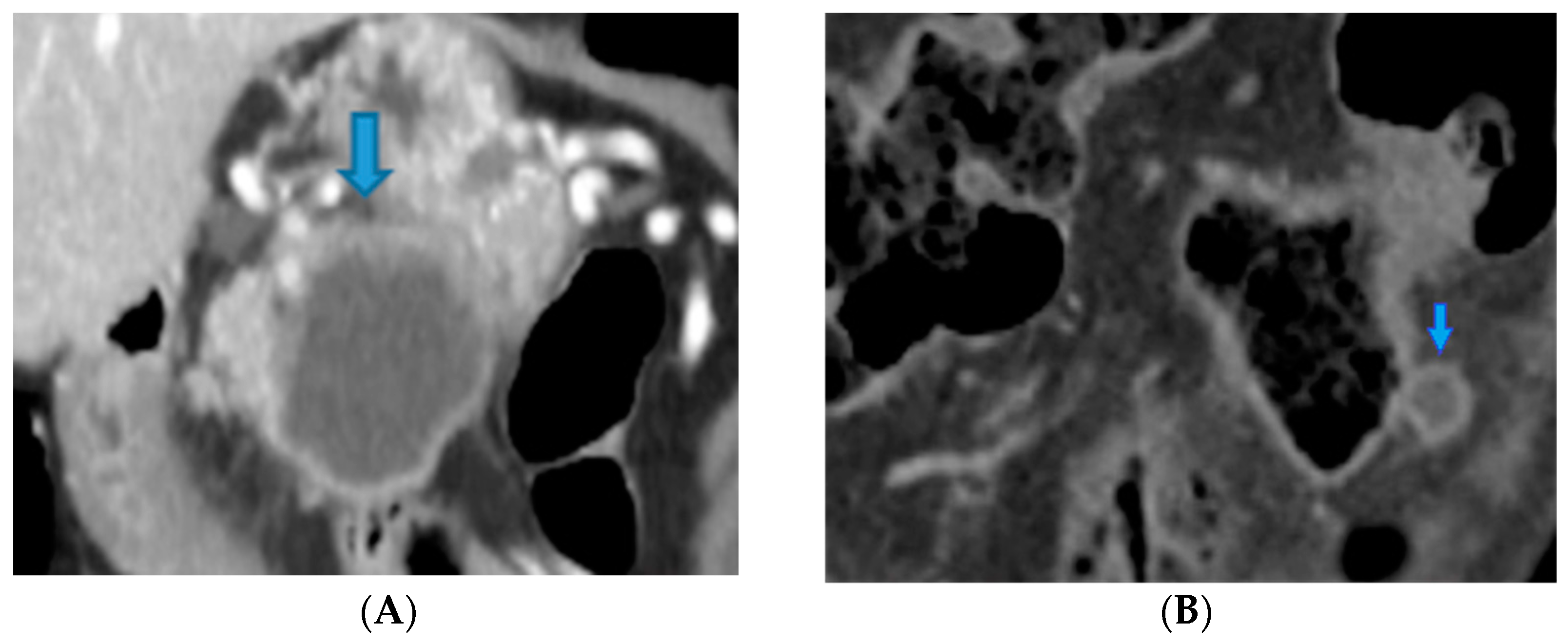
- Posteriorly, it is distanced from the posterior abdominal wall by the retroperitoneal space. It forms the anterior boundary of the retroperitoneal space (Figure 3).
3.1. Supramesocolic Spaces
3.1.1. Subphrenic Spaces
3.1.2. Perihepatic and Perisplenic Spaces
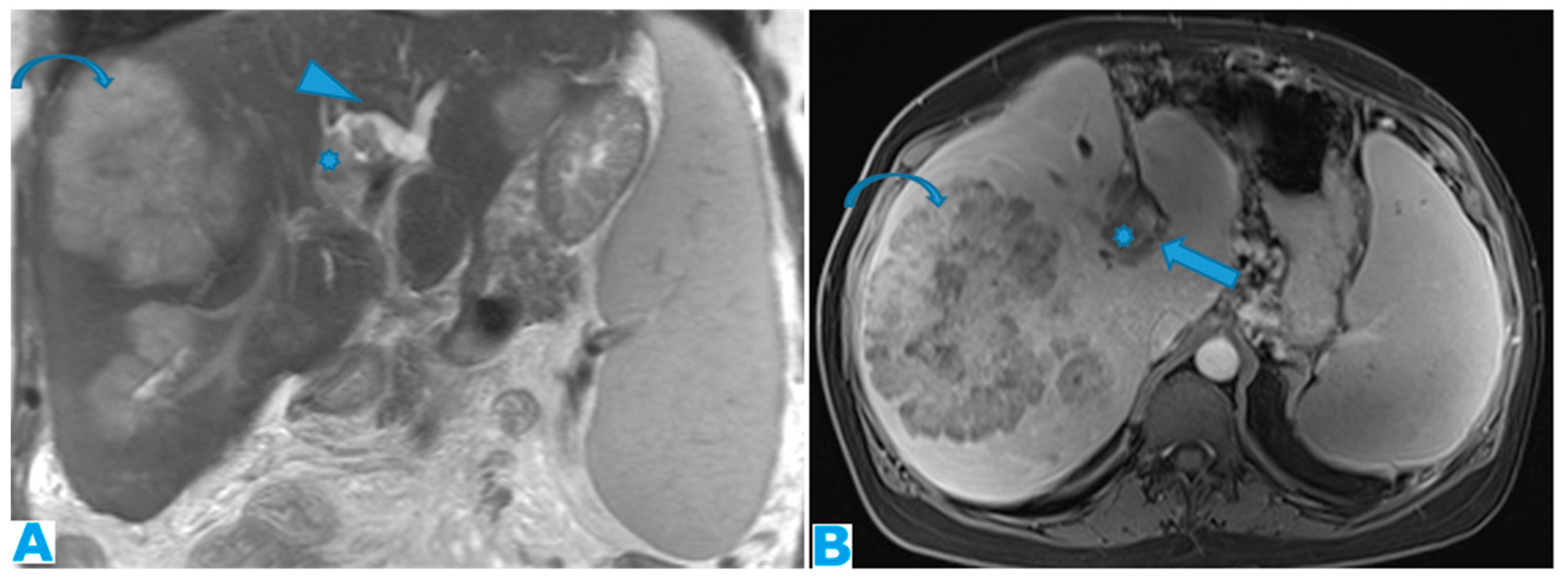
3.1.3. Periportal Space
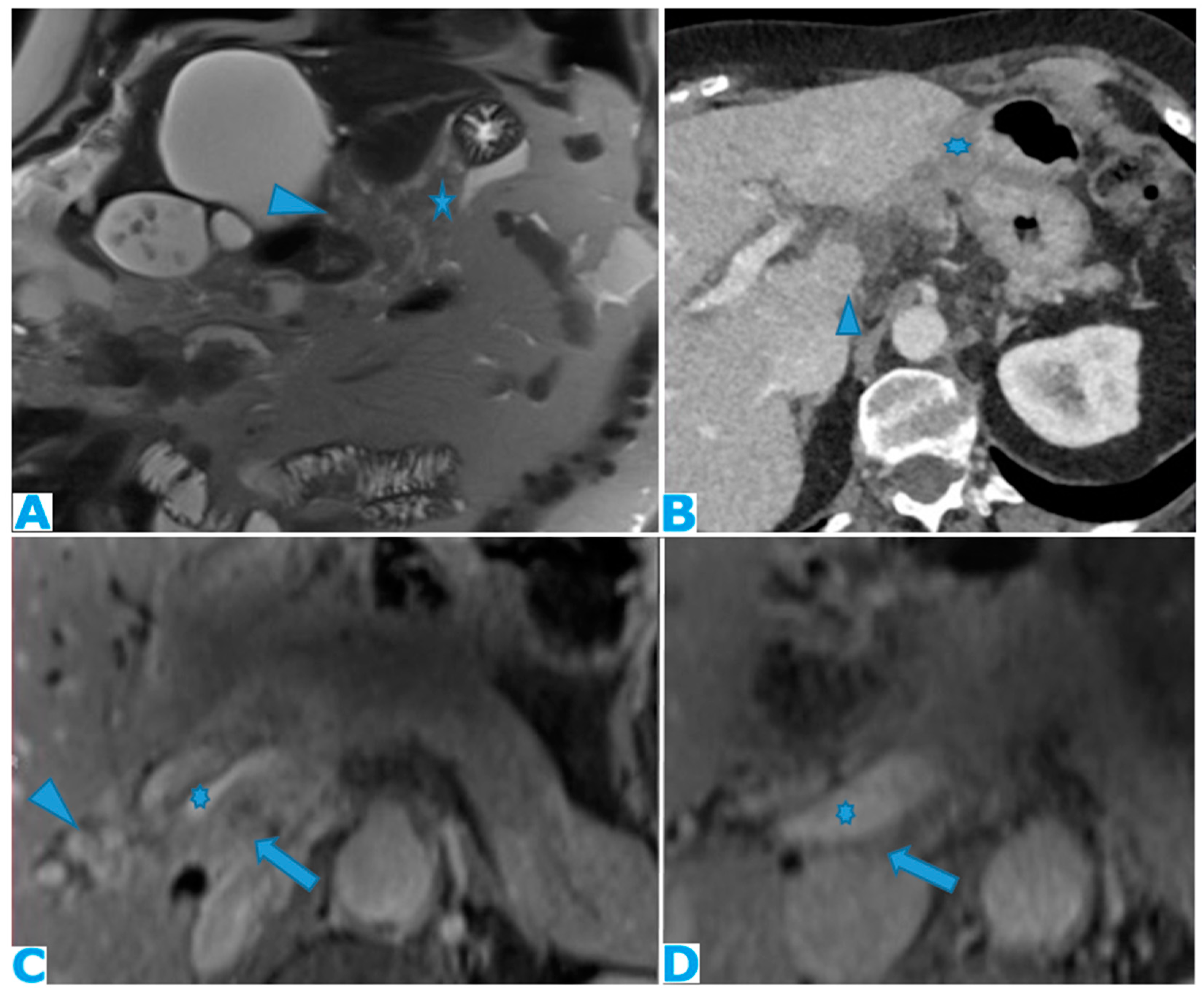
3.1.4. Lesser Omentum
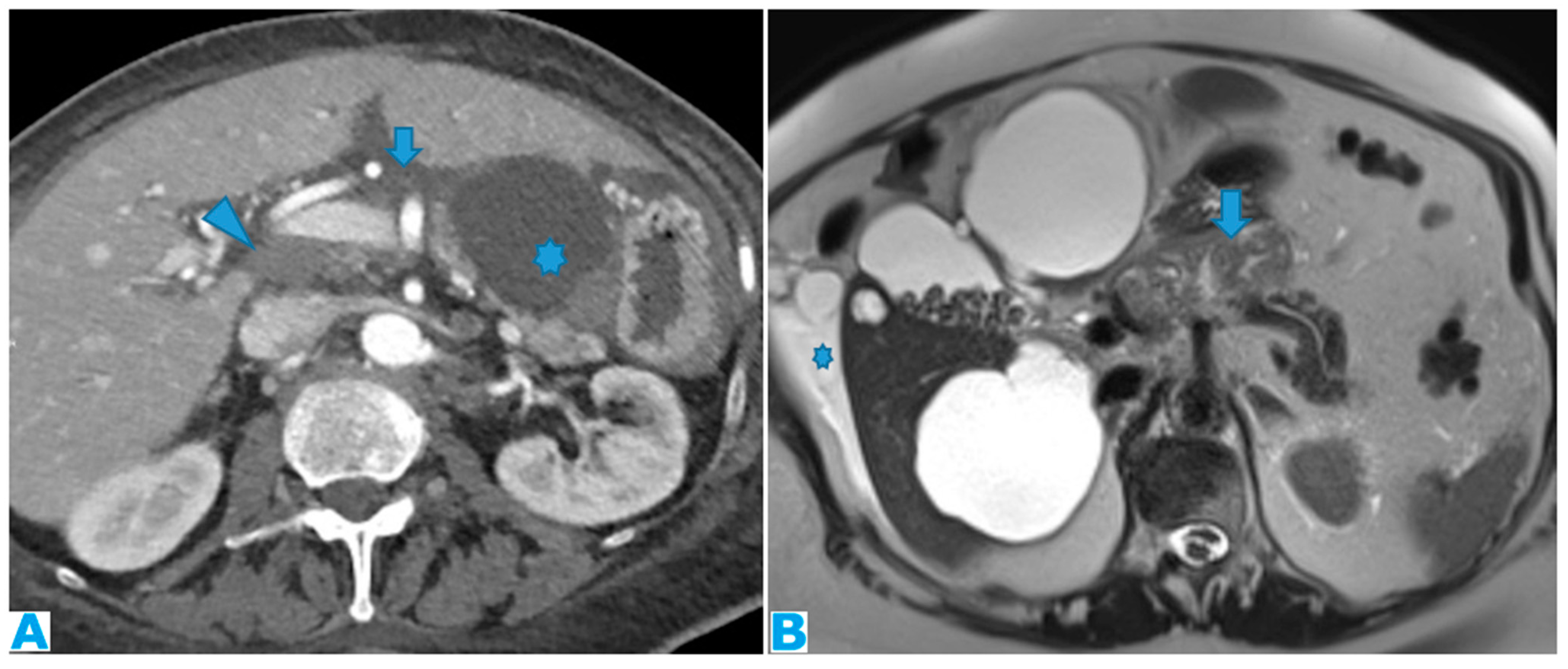
3.1.5. Lesser Sac
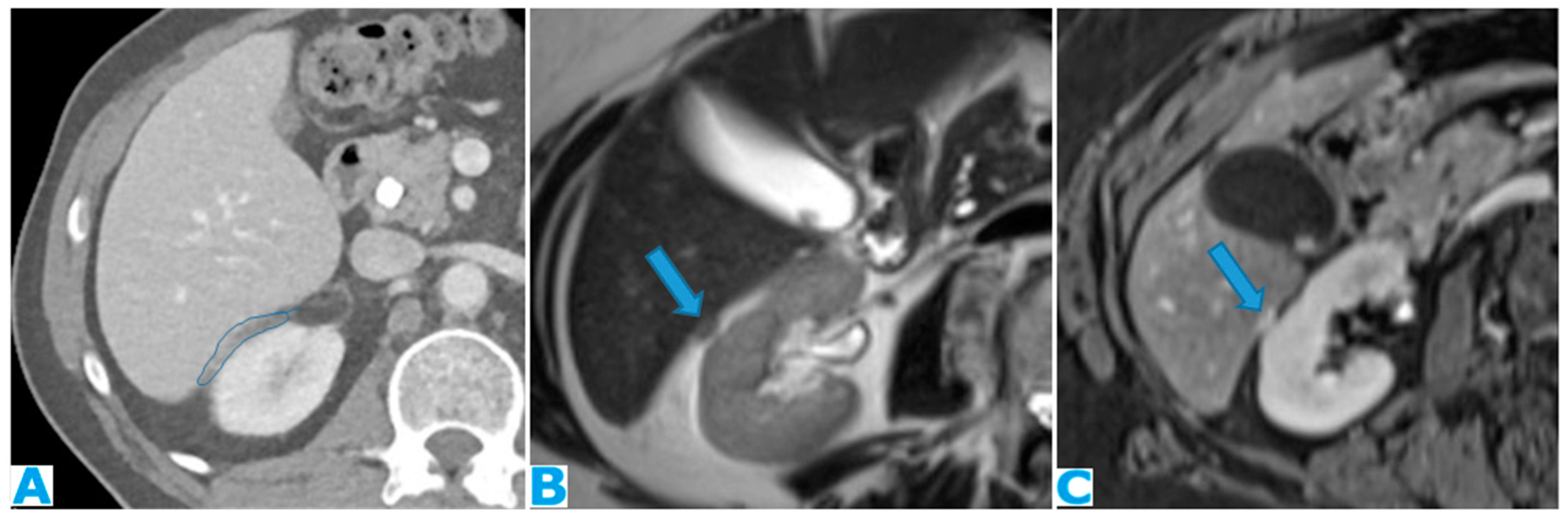
3.1.6. Right Subhepatic Space
3.2. Inframesocolic Spaces
3.2.1. Greater Omentum
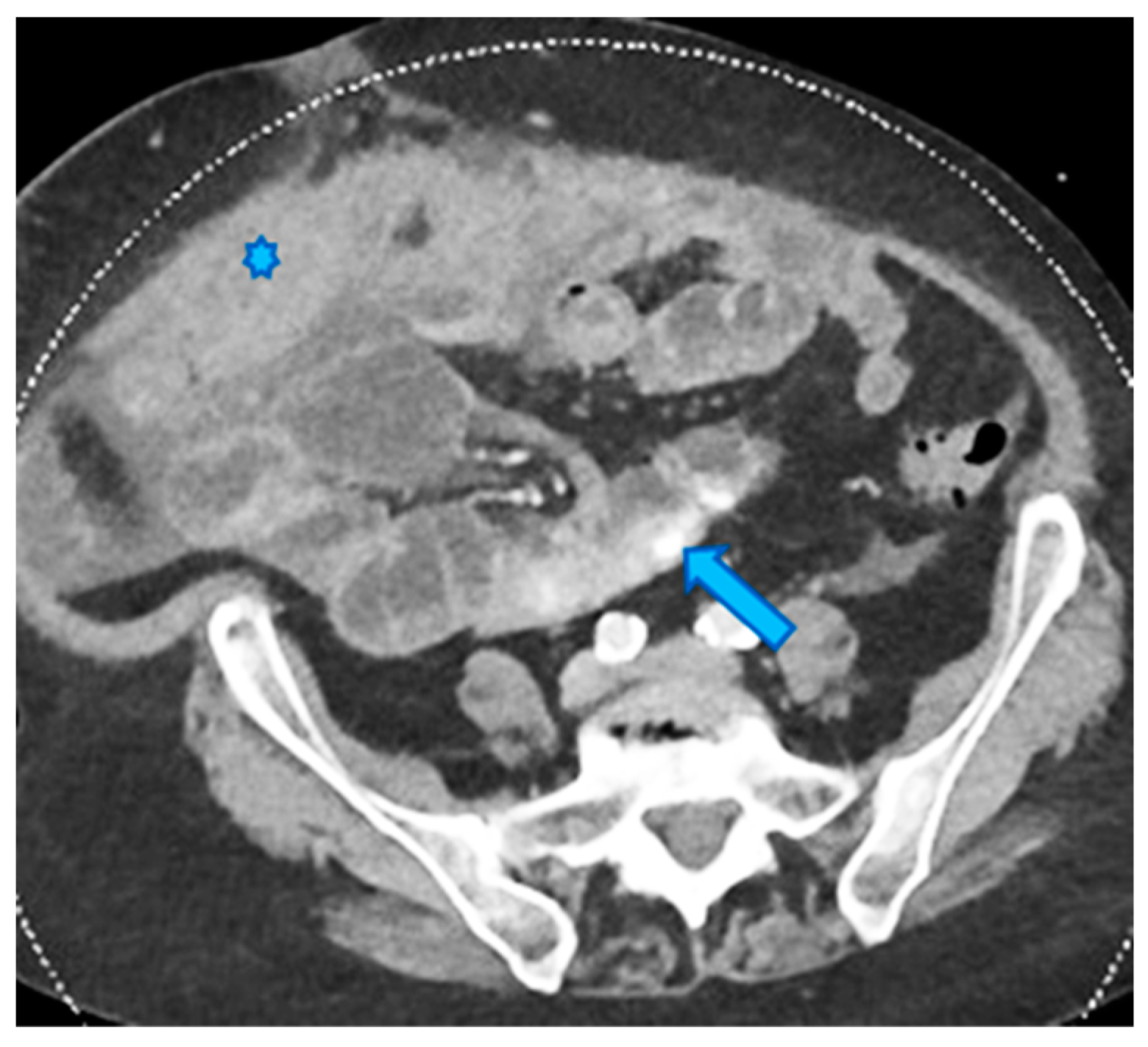
3.2.2. Small Bowel Mesentery
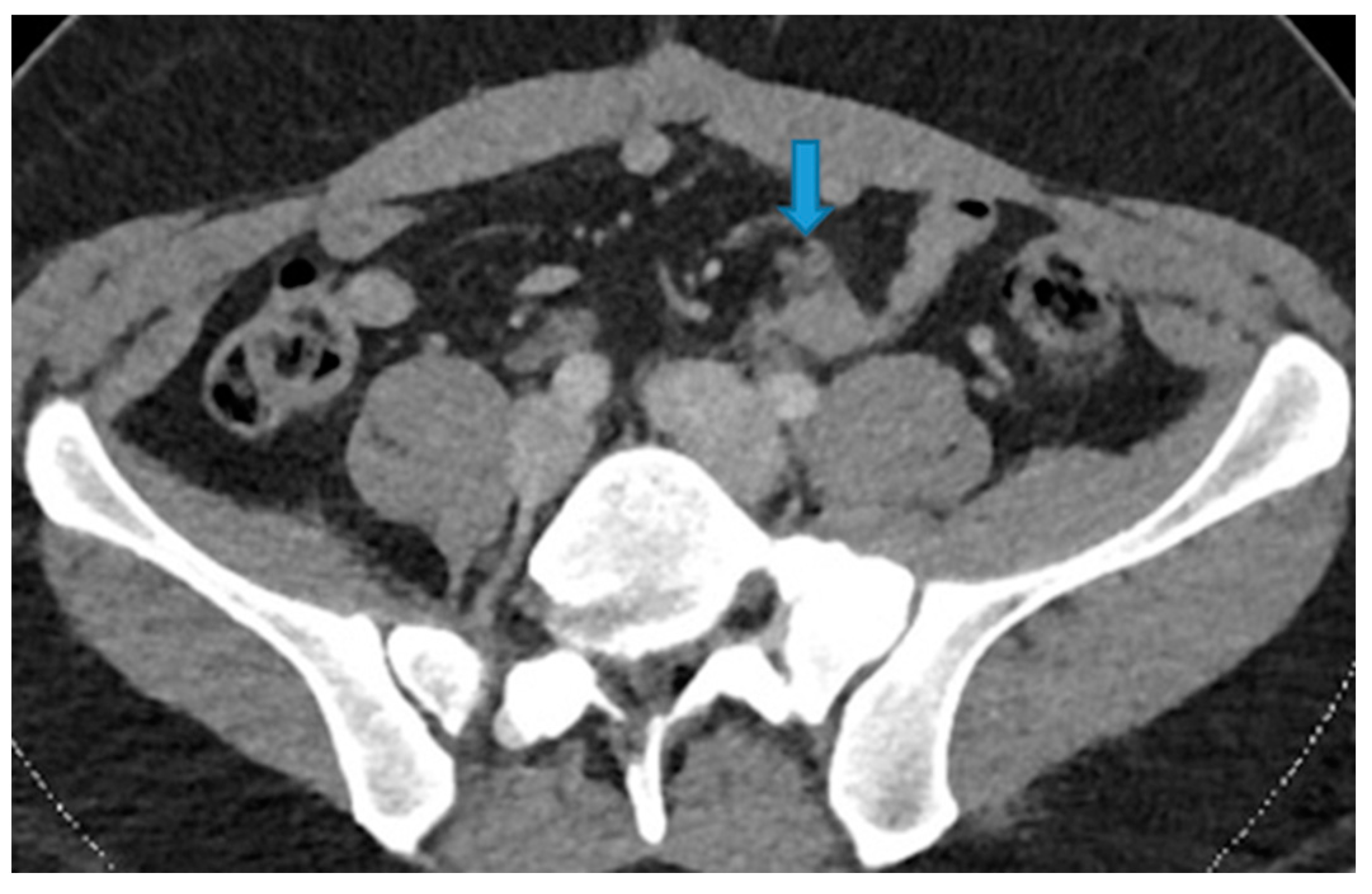
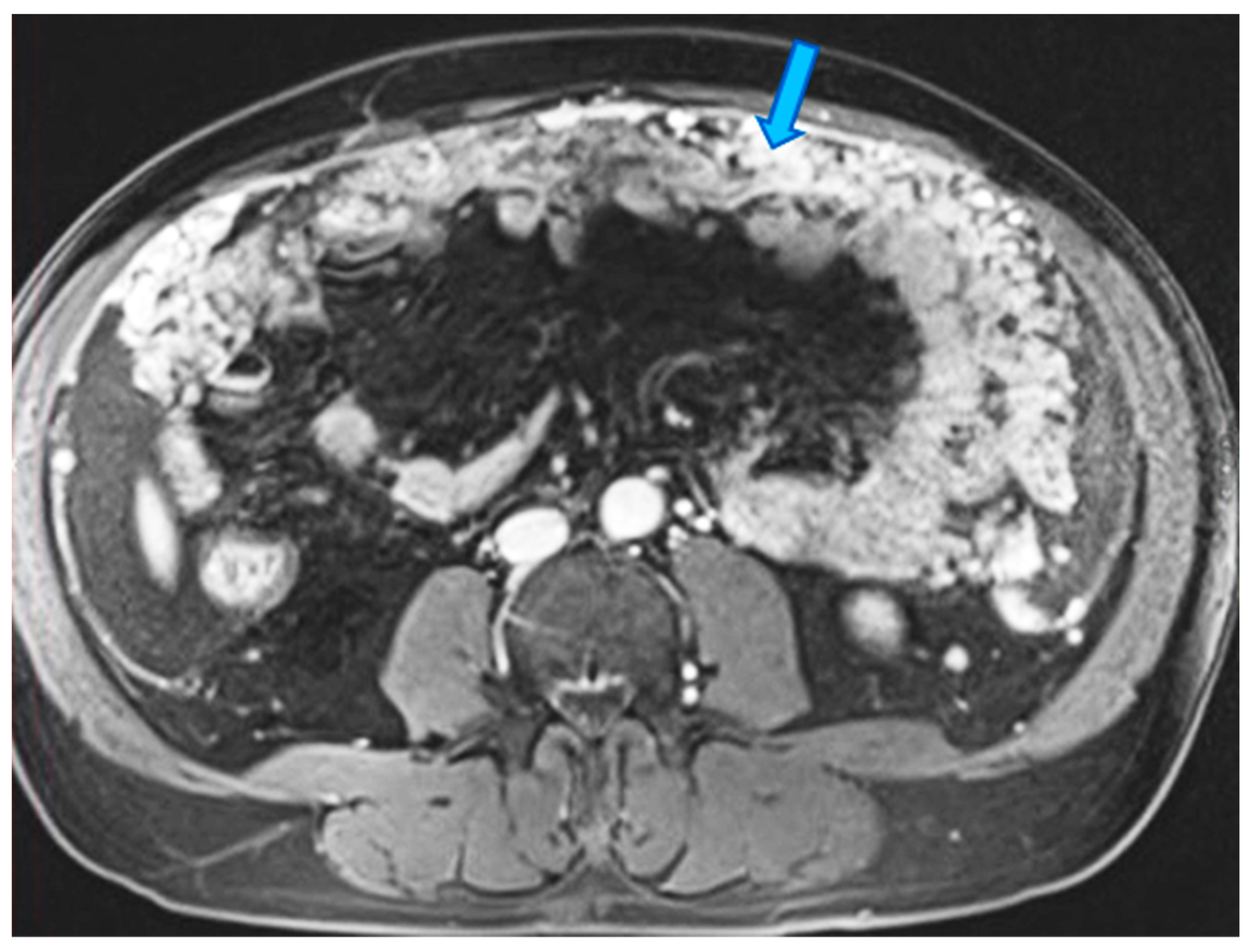
- Within the mesenteric fat: as in the rest of the fat-containing peritoneal spaces, they may range from focal nodular fat stranding to irregular haziness to nodules and masses (Figure 21).
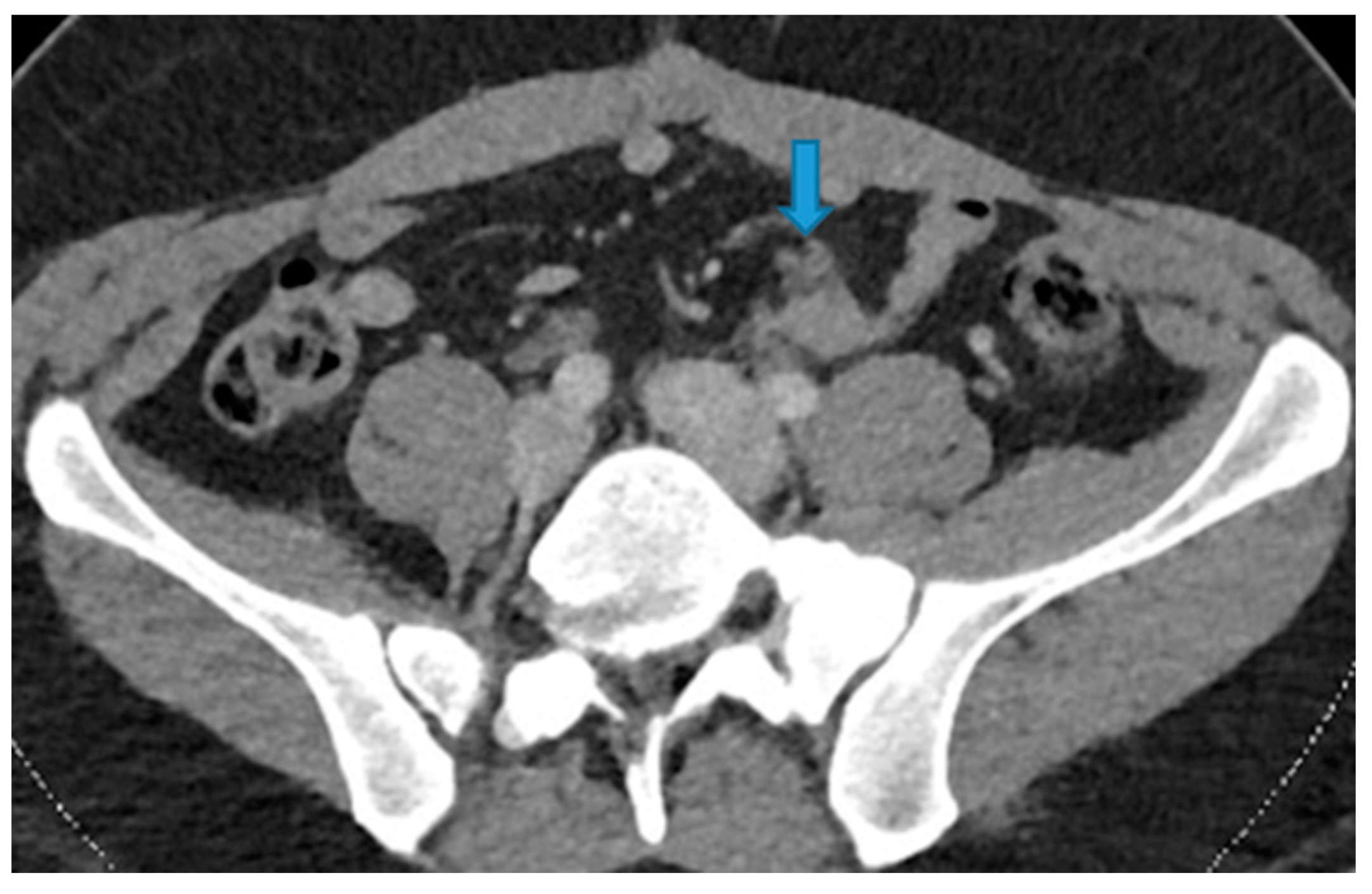
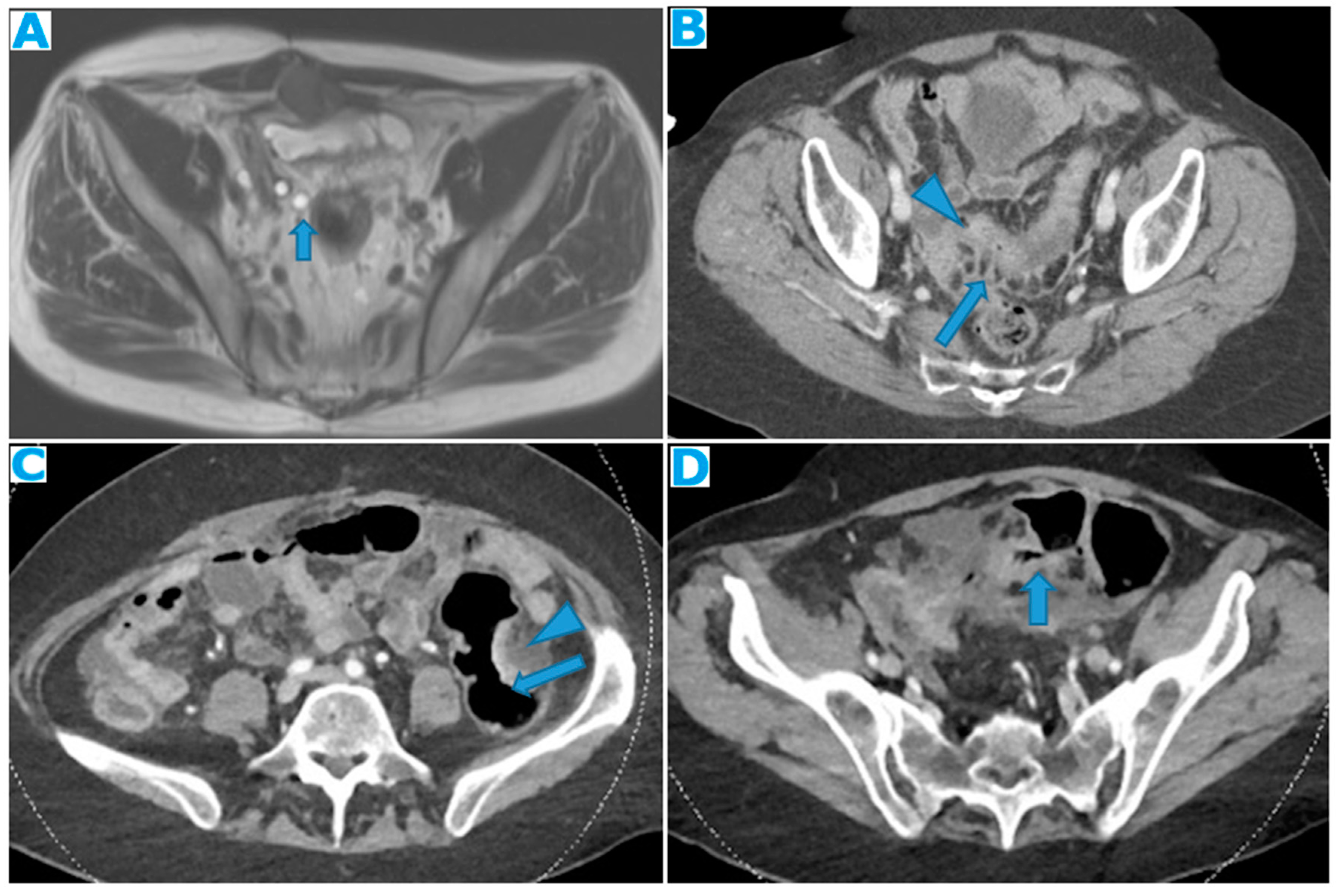
- Within the SB and caecal serosa: deposits may also lie within the serosa covering the small bowel and the caecum (Figure 22).

- Involving both the mesentery and the serosa: as in the transverse mesocolon, deposits may appear both within the mesentery and the serosa covering the small bowel loops and the caecum (Figure 23).

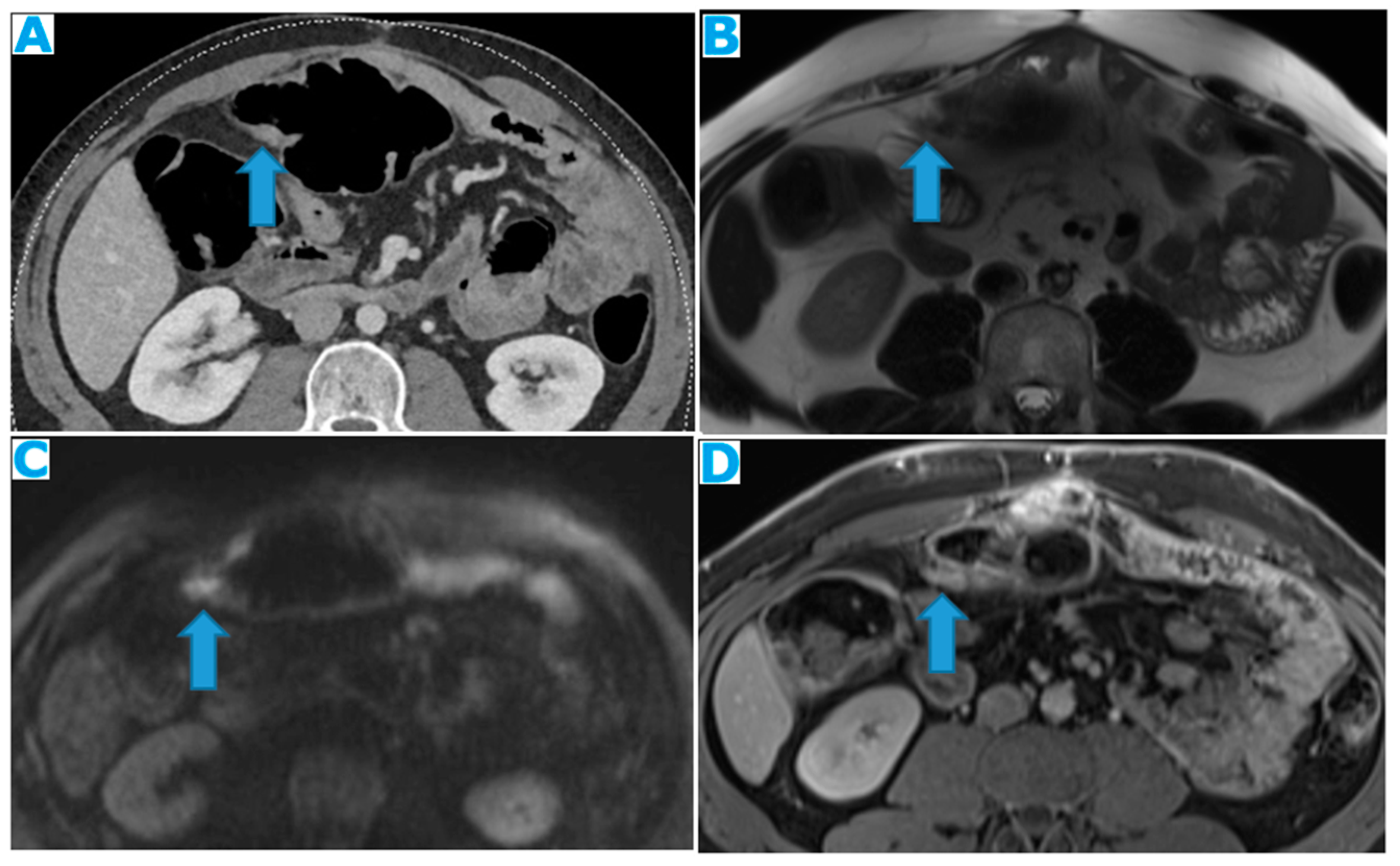
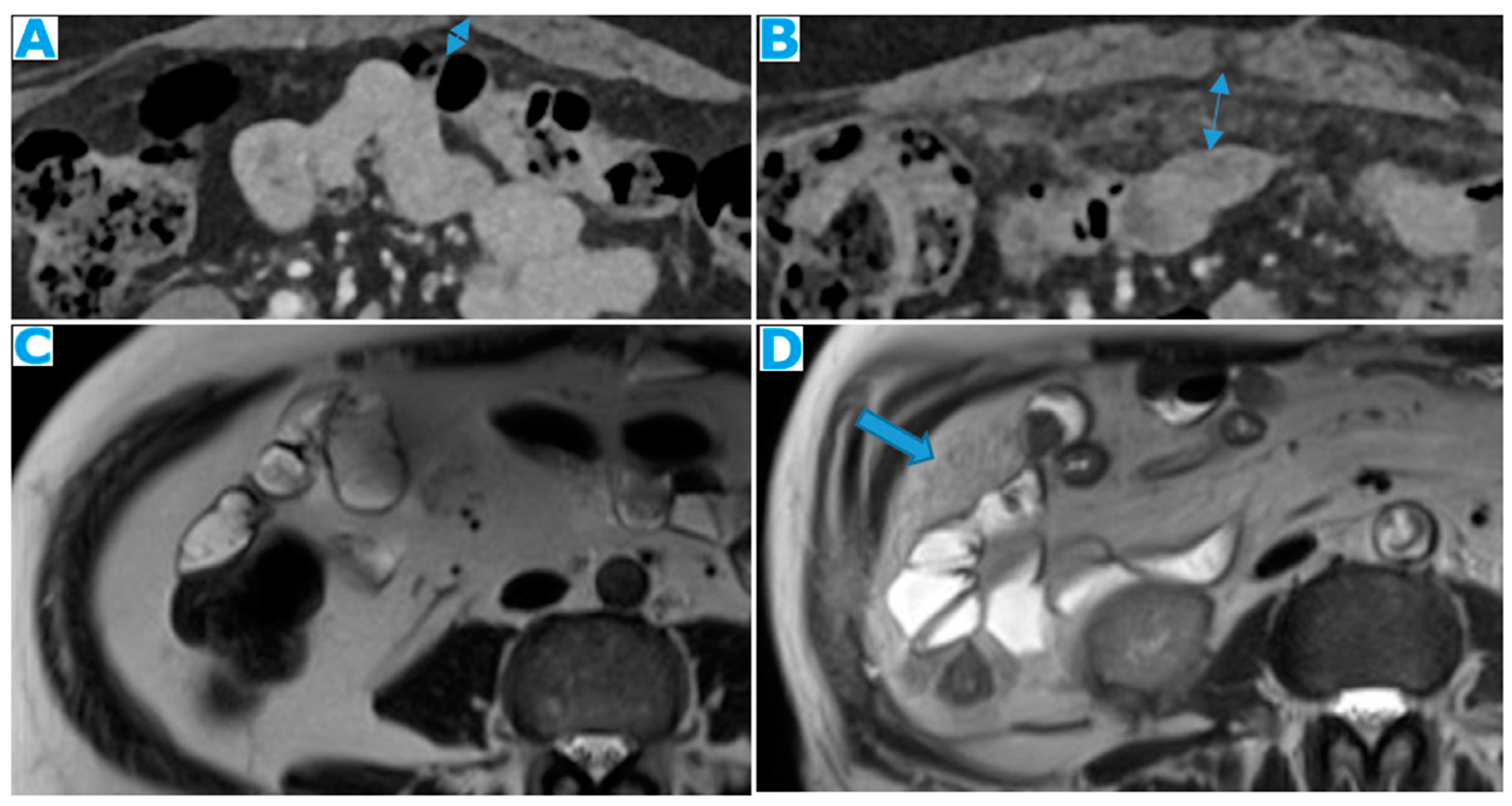
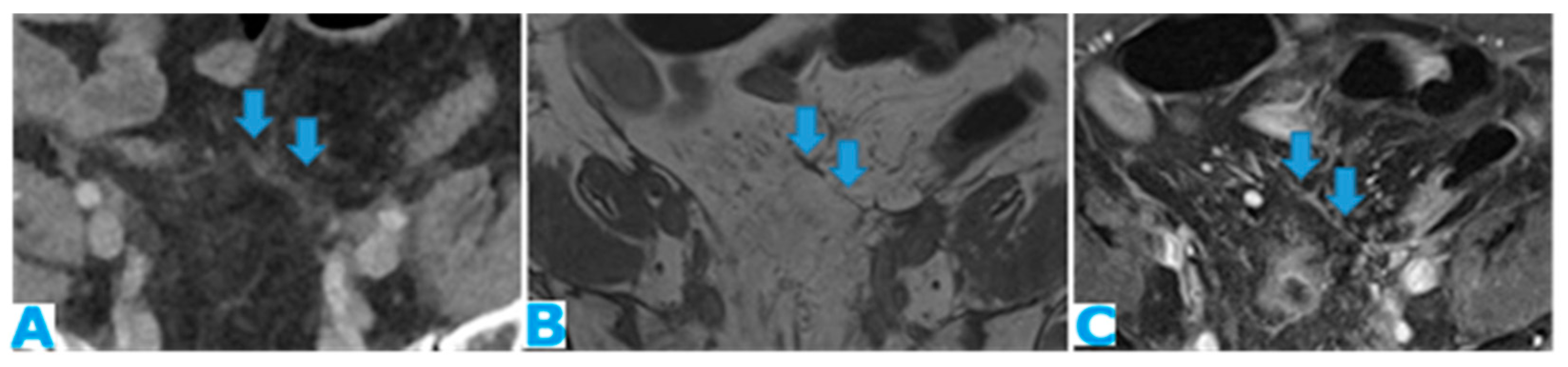
- Within the mesenteric leaves: Deposits within the mesenteric leaves may go unperceived. The nodular thickening and enhancement of the mesenteric leaves is usually more conspicuous using MR but can be also spotted using CT and becomes more noticeable when accompanied by ascites (Figure 24 and Figure 25).


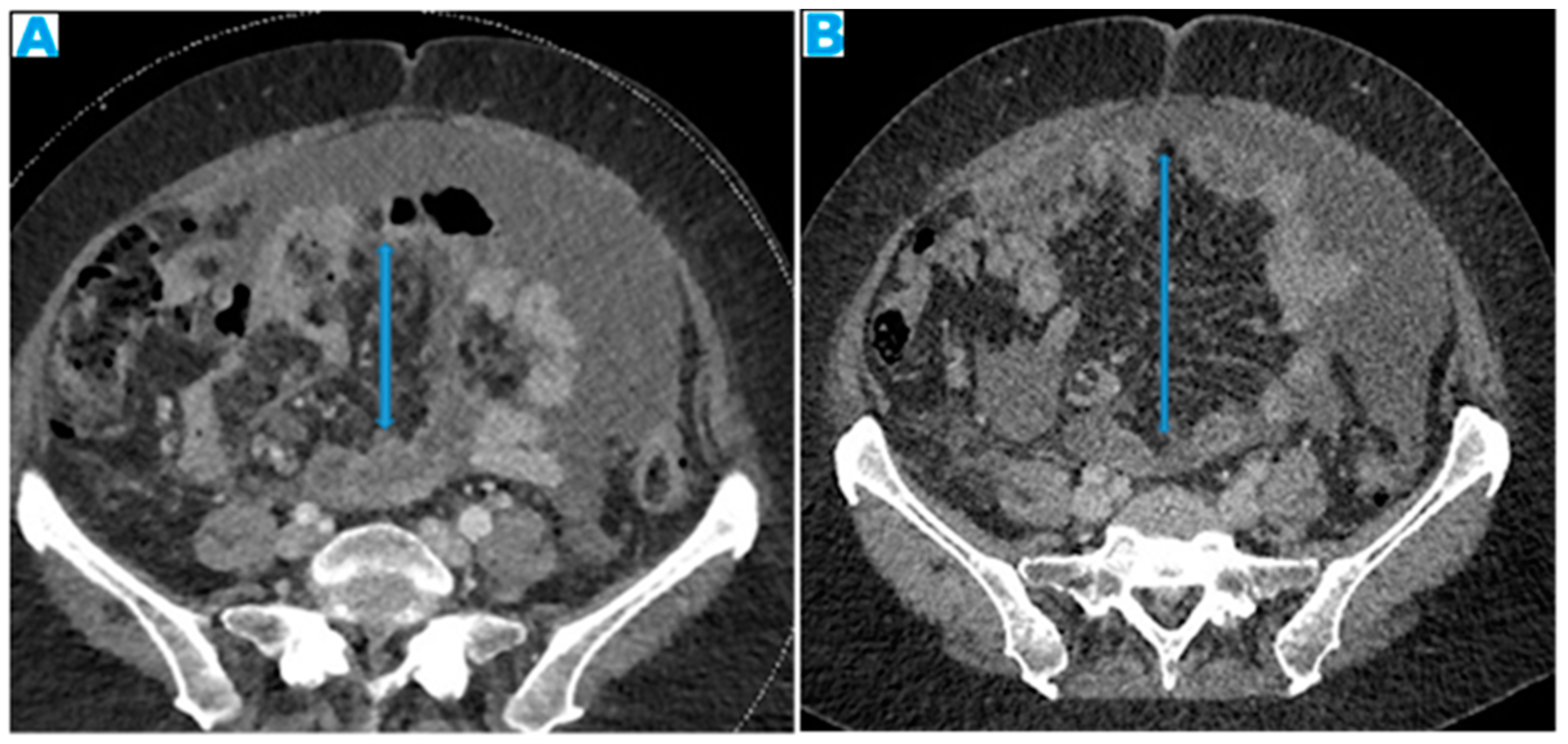
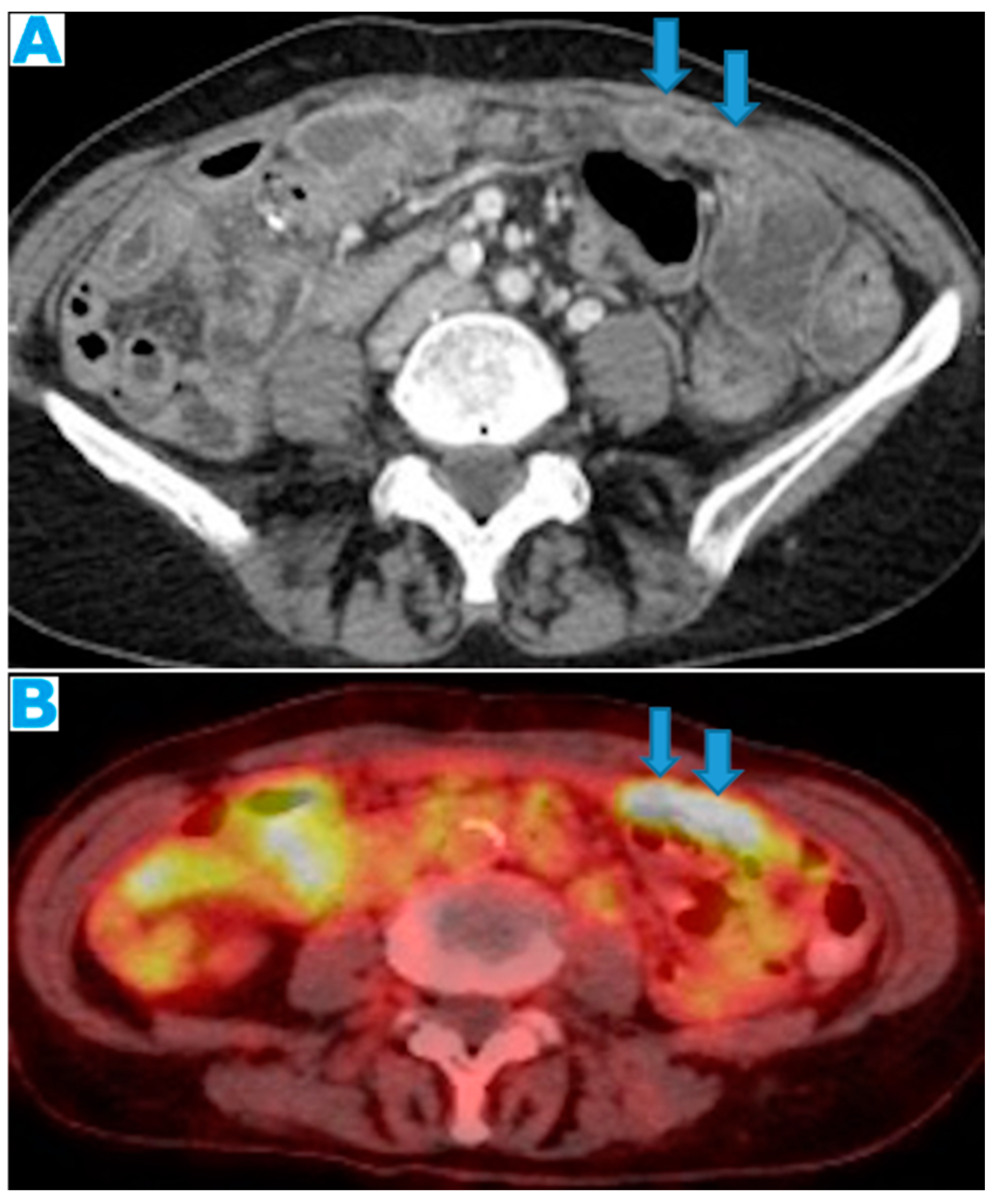
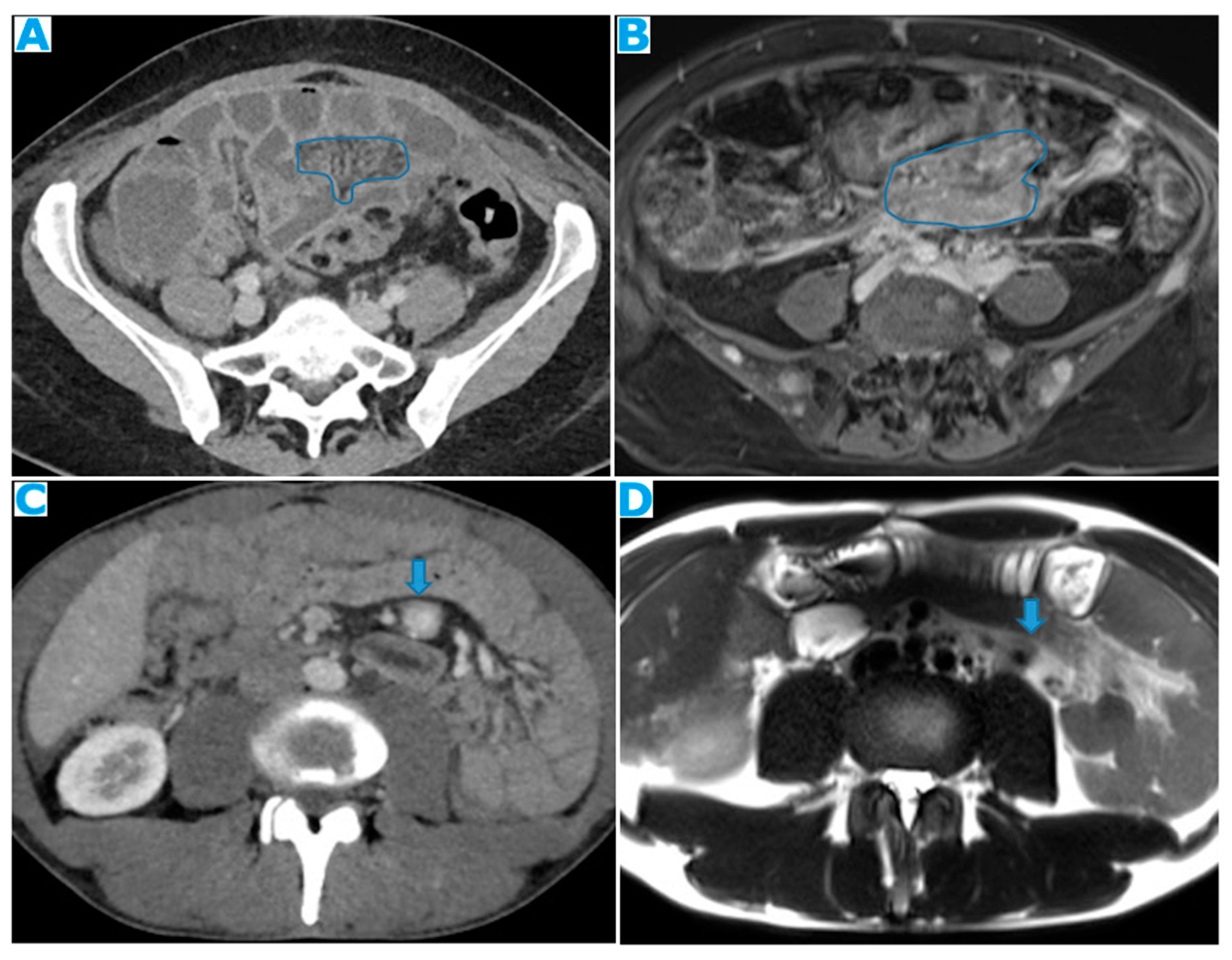
- Stellate mesentery: Diffuse mesenteric infiltration leads to a stellate appearance, which is commonly associated with breast (especially lobular carcinoma) [32], gastric, pancreatic, and ovarian tumours [33]. This deposition pattern follows the distribution of the mesenteric vessels, causing the thickening and rigidity of perivascular bundles (Figure 26).

3.2.3. Paracolic Gutters
3.2.4. Peritoneal Recesses of the Pelvis–Ovarian Metastases
4. Peritoneal Fluid Circulation–Ascites
5. Deposit Behaviour in Cross-Sectional Images
- Melanin-containing deposits: from melanoma (Figure 41).

- Calcium-containing deposits: mucinous tumours of different origins (ovary, stomach, colon, pancreas, appendix, gallbladder, urachus) may calcify (Figure 42).

- Blood-containing deposits: blood content is frequently found in peritoneal deposits from hypervascular tumours of different origins (for instance, clear-cell and granulosa ovarian tumours) (Figure 43).

- Myxoid-containing deposits: as in myxoid liposarcoma (Figure 44).

- Non-mineralised cartilage-containing deposits: from chondrosarcoma (Figure 45).

- Mucin-containing deposits: from mucinous tumours arising on different organs, namely ovary, stomach, colon, pancreas, appendix, gallbladder, and the urachus (Figure 46).

- Keratin-containing deposits: from tumours showing squamous differentiation (Figure 47).

6. Differential Diagnosis
6.1. Inflammatory
6.1.1. Omental Infarction—Figure S1
6.1.2. Peritoneal Amyloidosis—Figure S2
6.1.3. Peritoneal Sarcoidosis—Figure S3
6.1.4. Familial Mediterranean Fever—Figure S4
6.1.5. Encapsulating Sclerosing Peritonitis—Figure S5
6.2. Infectious
6.2.1. Peritoneal Tuberculosis—Figure S6
- Wet (the most common), where the salient feature is ascites, either free or loculated, which may show high attenuation on CT due to the high protein contents.
- Dry, where cellular content is predominant.
- Fibrotic fixed, where the main features are fibrotic changes, causing clustered SB loops.
- An in-between state may also be found (fibrotic mixed).
6.2.2. Peritoneal Echinococcosis—Figures S7 and S8
6.3. Benign Noninflammatory/Noninfectious
6.3.1. Splenosis/Accessory Spleen—Figure S9
6.3.2. Foreign Body Bowel Perforation—Figure S10
6.3.3. Encapsulated Omental Fat Necrosis—Figure S11
6.3.4. Endometriosis—Figure S12
6.3.5. Leiomyomatosis Peritonealis—Figure S13
6.3.6. Desmoid Tumours—Figure S14
6.4. Malignant
6.4.1. Primary Peritoneal Serous Carcinoma—Figure S15
6.4.2. Pseudomyxoma Peritonei (PMP)—Figure S16
6.4.3. Peritoneal Malignant Mesothelioma (PMM)—Figure S17
6.4.4. Desmoplastic Small Round Cell Tumour—Figure S18
6.4.5. Peritoneal Lymphomatosis and Peritoneal Sarcomatosis—Figures S19 and S20
7. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flanagan, M.; Solon, J. Peritoneal metastases from extra-abdominal cancer—A population-based study. Eur. J. Surg. Oncol. 2018, 44, 1811–1817. [Google Scholar] [CrossRef] [PubMed]
- Desai, J.P.; Moustarah, F. Peritoneal Metastasis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Pereira, F.; Serrano, A.; Manzanedo, I.; Pérez-Viejo, E.; González-Moreno, S.; González-Bayón, L.; Arjona-Sánchez, A.; Torres, J.; Ramos, I.; Barrios, M.E.; et al. GECOP-MMC: Phase IV randomized clinical trial to evaluate the efficacy of hyperthermic intraperitoneal chemotherapy (HIPEC) with mytomicin-C after complete surgical cytoreduction in patients with colon cancer peritoneal metastases. BMC Cancer 2022, 22, 536. [Google Scholar] [CrossRef] [PubMed]
- van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.H.J.T.; van der Velden, J.; Arts, H.J.; Massuger, L.F.A.G.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef]
- Yang, X.-J.; Huang, C.-Q.; Suo, T.; Mei, L.-J.; Yang, G.-L.; Cheng, F.-L.; Zhou, Y.-F.; Xiong, B.; Yonemura, Y.; Li, Y. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer: Final results of a phase III randomized clinical trial. Ann. Surg. Oncol. 2011, 18, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szadkowska, M.A.; Pałucki, J.; Cieszanowski, A. Diagnosis and treatment of peritoneal carcinomatosis—A comprehensive overview. Pol. J. Radiol. 2023, 88, e89–e97. [Google Scholar] [CrossRef]
- González-Moreno, S.; González-Bayón, L. Imaging of peritoneal carcinomatosis. Cancer J. Sudbury Mass 2009, 15, 184–189. [Google Scholar] [CrossRef]
- Patel, C.M.; Sahdev, A. CT, MRI and PET imaging in peritoneal malignancy. Cancer Imaging 2011, 11, 123–139. [Google Scholar] [CrossRef] [Green Version]
- Van ’t Sant, I.; Engbersen, M.P. Diagnostic performance of imaging for the detection of peritoneal metastases: A meta-analysis. Eur. Radiol. 2020, 30, 3101–3112. [Google Scholar] [CrossRef]
- Cianci, R.; Delli Pizzi, A. Magnetic Resonance Assessment of Peritoneal Carcinomatosis: Is There a True Benefit from Diffusion-Weighted Imaging? Curr. Probl. Diagn. Radiol. 2020, 49, 392–397. [Google Scholar] [CrossRef]
- Low, R.N. Magnetic Resonance Imaging in the Oncology Patient: Evaluation of the Extrahepatic Abdomen. Semin. Ultrasound CT MRI 2005, 26, 224–236. [Google Scholar] [CrossRef]
- Satoh, Y.; Ichikawa, T.; Motosugi, U.; Kimura, K.; Sou, H.; Sano, K.; Araki, T. Diagnosis of peritoneal dissemination: Comparison of 18F-FDG PET/CT, diffusion-weighted MRI, and contrast-enhanced MDCT. AJR Am. J. Roentgenol. 2011, 196, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Low, R.N.; Sebrechts, C.P.; Barone, R.M.; Muller, W. Diffusion-weighted MRI of peritoneal tumors: Comparison with conventional MRI and surgical and histopathologic findings—A feasibility study. AJR Am. J. Roentgenol. 2009, 193, 461–970. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Li, K.; Peng, T. Diagnostic value of diffusion-weighted imaging/magnetic resonance imaging for peritoneal metastasis from malignant tumor: A systematic review and meta-analysis. Medicine 2021, 100, e24251. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.M.; Collins, D.J. Diffusion-weighted MRI in the body: Applications and challenges in oncology. AJR Am. J. Roentgenol. 2007, 188, 1622–1635. [Google Scholar] [CrossRef] [Green Version]
- Sala, E.; Priest, A.N.; Kataoka, M.; Graves, M.J.; McLean, M.A.; Joubert, I.; Lomas, D.J. Apparent diffusion coefficient and vascular signal fraction measurements with magnetic resonance imaging: Feasibility in metastatic ovarian cancer at 3 Tesla: Technical development. Eur. Radiol 2010, 20, 491–496. [Google Scholar] [CrossRef]
- Kyriazi, S.; Collins, D.J.; Messiou, C.; Pennert, K.; Davidson, R.L.; Giles, S.L.; Kaye, S.B.; Desouza, N.M. Metastatic ovarian and primary peritoneal cancer: Assessing chemotherapy response with diffusion-weighted MR imaging--value of histogram analysis of apparent diffusion coefficients. Radiology 2011, 261, 182–192. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Lee, S.W. Diagnostic accuracy of (18)F-FDG PET/CT for detection of peritoneal carcinomatosis; a systematic review and meta-analysis. Br. J. Radiol. 2018, 91, 20170519. [Google Scholar] [CrossRef]
- Bhuyan, P.; Mahapatra, S.; Mahapatra, S.; Sethy, S.; Parida, P.; Satpathy, S. Extraovarian primary peritoneal papillary serous carcinoma. Arch. Gynecol. Obstet. 2010, 281, 561–564. [Google Scholar] [CrossRef]
- Bhatt, A.N.; Mathur, R.; Farooque, A.; Verma, A.; Dwarakanath, B.S. Cancer biomarkers—Current perspectives. Indian J. Med. Res. 2010, 132, 129–149. [Google Scholar]
- Nagpal, M.; Singh, S.; Singh, P.; Chauhan, P.; Zaidi, M.A. Tumor markers: A diagnostic tool. Natl. J. Maxillofac. Surg. 2016, 7, 17–20. [Google Scholar]
- Nougaret, S.; Addley, H.C. Ovarian carcinomatosis: How the radiologist can help plan the surgical approach. Radiographics 2012, 32, 1775–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laghi, A.; Bellini, D.; Rengo, M.; Accarpio, F.; Caruso, D.; Biacchi, D.; Di Giorgio, A.; Sammartino, P. Diagnostic performance of computed tomography and magnetic resonance imaging for detecting peritoneal metastases: Systematic review and meta-analysis. Radiol. Med. 2017, 122, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Rivard, J.D.; Temple, W.J.; McConnell, Y.J.; Sultan, H.; Mack, L.A. Preoperative computed tomography does not predict resectability in peritoneal carcinomatosis. Am. J. Surg. 2014, 207, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Low, R.N.; Barone, R.M.; Rousset, P. Peritoneal MRI in patients undergoing cytoreductive surgery and HIPEC: History, clinical applications, and implementation. Eur. J. Surg. Oncol. 2021, 47, 65–74. [Google Scholar] [CrossRef]
- Cabral, F.C.; Krajewski, K.M. Peritoneal lymphomatosis: CT and PET/CT findings and how to differentiate between carcinomatosis and sarcomatosis. Cancer Imaging 2013, 13, 162–170. [Google Scholar] [CrossRef]
- Low, R.N. MR imaging of the peritoneal spread of malignancy. Abdom. Imaging 2007, 32, 267–283. [Google Scholar] [CrossRef]
- Tirkes, T.; Sandrasegaran, K. Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging. Radiographics 2012, 32, 437–451. [Google Scholar] [CrossRef]
- Gore, R.M.; Levine, L.S. Textbook of Gastrointestinal Radiology, 3rd ed.; Saunders: Philadelphia, PA, USA, 2007; pp. 2071–2097. [Google Scholar]
- Meyers, M.A.; Oliphant, M. The peritoneal ligaments and mesenteries: Pathways of intraabdominal spread of disease. Radiology 1987, 163, 593–604. [Google Scholar] [CrossRef]
- Akin, O.; Sala, E. Perihepatic metastases from ovarian cancer: Sensitivity and specificity of CT for the detection of metastases with and those without liver parenchymal invasion. Radiology 2008, 248, 511–517. [Google Scholar] [CrossRef]
- Winston, C.B.; Hadar, O. Metastatic lobular carcinoma of the breast: Patterns of spread in the chest, abdomen, and pelvis on CT. AJR Am. J. Roentgenol. 2000, 175, 795–800. [Google Scholar] [CrossRef]
- Healy, J.C.; Reznek, R.H. The peritoneum, mesenteries and omenta: Normal anatomy and pathological processes. Eur. Radiol. 1998, 8, 886–900. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Yang, J. MRI for discriminating metastatic ovarian tumors from primary epithelial ovarian cancers. J. Ovarian Res. 2015, 8, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zulfiqar, M.; Koen, J. Krukenberg Tumors: Update on Imaging and Clinical Features. AJR Am. J. Roentgenol. 2020, 215, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Kim, W.H. CT and MR findings of Krukenberg tumors: Comparison with primary ovarian tumors. J. Comput. Assist. Tomogr. 1996, 20, 393–398. [Google Scholar] [CrossRef] [PubMed]
- Saif, M.W.; Siddiqui, I.A. Management of ascites due to gastrointestinal malignancy. Ann. Saudi Med. 2009, 29, 369–377. [Google Scholar] [CrossRef] [Green Version]
- Chang, D.K.; Kim, J.W. Clinical significance of CT-defined minimal ascites in patients with gastric cancer. World J. Gastroenterol. 2005, 11, 6587. [Google Scholar] [CrossRef]
- Meyers, M.A. Intraperitoneal seeding: Pathways of spread and localization. In Meyers’ Dynamic Radiology of the Abdomen, 6th ed.; Meyers, M.A., Charnsangavej, C., Eds.; Springer: New York, NY, USA, 2000; pp. 69–105. [Google Scholar]
- Feldman, G.B.; Knapp, R.C. Lymphatic drainage of the peritoneal cavity and its significance in ovarian cancer. Am. J. Obstet. Gynecol. 1974, 119, 991–994. [Google Scholar] [CrossRef]
- Seltzer, S.E. Analysis of the tethered-bowel sign on abdominal CT as a predictor of malignant ascites. Gastrointest. Radiol. 1987, 12, 245–249. [Google Scholar] [CrossRef]
- Leitner, M.J.; Jordan, C.G. Torsion, infarction and hemorrhage of the omentum as a cause of acute abdominal distress. Ann. Surg. 1952, 135, 103–110. [Google Scholar] [CrossRef]
- Pereira, J.M.; Sirlin, C.B. Disproportionate fat stranding: A helpful CT sign in patients with acute abdominal pain. Radiographics 2004, 24, 703–715. [Google Scholar] [CrossRef]
- Pickhardt, P.J.; Bhalla, S. Unusual nonneoplastic peritoneal and subperitoneal conditions: CT findings. Radiographics 2005, 25, 719–730. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Ryu, J.A. Amyloidosis of the mesentery and small intestine presenting as a mesenteric haematoma. Br. J. Radiol. 2008, 81, e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Iannuzzi, M.C.; Rybicki, B.A. Sarcoidosis. N. Engl. J. Med. 2007, 357, 2153–2165. [Google Scholar] [CrossRef] [PubMed]
- Gezer, N.S.; Basara, I. Abdominal sarcoidosis: Cross-sectional imaging findings. Diagn. Interv. Radiol. 2015, 21, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Zissin, R.; Rathaus, V. CT findings in patients with familial Mediterranean fever during an acute abdominal attack. Br. J. Radiol. 2003, 76, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, H.; Cascella, M. Familial Mediterranean Fever. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Manphool, S.; Satheesh, K. Encapsulating peritoneal sclerosis: The abdominal cocoon. Radiographics 2019, 39, 62–77. [Google Scholar]
- Uygur-Bayramicli, O.; Dabak, G. A clinical dilemma: Abdominal tuberculosis. World J. Gastroenterol. 2003, 9, 1098–1101. [Google Scholar] [CrossRef]
- Burrill, J.; Williams, C.J. Tuberculosis: A radiologic review. Radiographics 2007, 27, 1255–1273. [Google Scholar] [CrossRef] [Green Version]
- Pedrosa, I.; Saíz, A. Hydatid disease: Radiologic and pathologic features and complications. Radiographics 2000, 20, 795–817. [Google Scholar] [CrossRef]
- Moro, P.; Schantz, P.M. Echinococcosis: A review. Int. J. Infect. Dis. 2009, 13, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Zalaquett, E.; Menias, C. Imaging of hydatid disease with a focus on extrahepatic involvement. Radiographics 2007, 37, 901–923. [Google Scholar] [CrossRef] [PubMed]
- McManus, D.P.; Zhang, W. Echinococcosis. Lancet 2003, 362, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Sato, N.; Abe, T. Intrahepatic splenosis in a chronic hepatitis C patient with no history of splenic trauma mimicking hepatocellular carcinoma. Am. J. Case Rep. 2014, 15, 416–420. [Google Scholar]
- Leong, C.W.; Menon, T. Post-Traumatic Intrahepatic Splenosis Mimicking a Neuroendocrine Tumour. BMJ Case Rep. 2013, 2013, bcr2012007885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gruen, D.R.; Gollub, M. Intrahepatic splenosis mimicking hepatic adenoma. AJR Am. J. Roentgenol. 1997, 168, 725–726. [Google Scholar] [CrossRef]
- Drake, A.; Dhundee, J. Disseminated leiomyomatosis peritonealis in association with oestrogen secreting ovarian fibrothecoma. BJOG 2001, 108, 661–664. [Google Scholar]
- Kumar, S.; Sharma, J.B. Disseminated peritoneal leiomyomatosis: An unusual complication of laparoscopic myomectomy. Arch. Gynecol. Obstet. 2008, 278, 93–95. [Google Scholar] [CrossRef]
- Surmacki, P.; Sporny, S. Disseminated peritoneal leiomyomatosis coexisting with leiomyoma of the uterine body. Arch. Gynecol. Obstet. 2006, 273, 301–303. [Google Scholar] [CrossRef]
- Sinha, A.; Hansmann, A. Imaging assessment of desmoid tumours in familial adenomatous polyposis: Is state-of-the-art 1.5 T MRI better than 64-MDCT? Br. J. Radiol. 2012, 85, e254–e261. [Google Scholar] [CrossRef] [Green Version]
- Brooks, A.P.; Reznek, R.H. CT appearances of desmoid tumours in familial adenomatous polyposis: Further observations. Clin. Radiol. 1994, 49, 601–607. [Google Scholar] [CrossRef]
- Robinson, W.A.; McMillan, C. Desmoid tumors in pregnant and postpartum women. Cancers 2012, 4, 184–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Yang, Q. Differences between primary peritoneal serous carcinoma and advanced serous ovarian carcinoma: A study based on the SEER database. J. Ovarian Res. 2021, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Morita, H.; Aoki, J. Serous surface papillary carcinoma of the peritoneum: Clinical, radiologic, and pathologic findings in 11 patients. Am. J. Roentgenol. 2004, 183, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Diop, A.D.; Fontarensky, M. CT imaging of peritoneal carcinomatosis and its mimics. Diagn. Interv. Imaging 2014, 95, 861–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugarbaker, P.H. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution phenomenon. Ann. Surg. 1994, 219, 109–111. [Google Scholar]
- Mittal, R.; Chandramohan, A. Pseudomyxoma peritonei: Natural history and treatment. Int. J. Hyperthermia. 2017, 33, 511–519. [Google Scholar] [CrossRef]
- Ronnett, B.M.; Yan, H. Patients with pseudomyxoma peritonei associated with disseminated peritoneal adenomucinosis have a significantly more favorable prognosis than patients with peritoneal mucinous carcinomatosis. Cancer 2001, 92, 85–91. [Google Scholar] [CrossRef]
- Broeckx, G.; Pauwels, P. Malignant peritoneal mesothelioma: A review. Transl. Lung Cancer Res. 2018, 7, 537–542. [Google Scholar] [CrossRef]
- Chen, J.; Wu, Z. Intra-abdominal desmoplastic small round cell tumors: CT and FDG-PET/CT findings with histopathological association. Oncol. Lett. 2016, 11, 3298–3302. [Google Scholar] [CrossRef] [Green Version]
- Yoo, E.; Kim, J.H. Greater and lesser omenta: Normal anatomy and pathologic processes. Radiographics 2007, 27, 707–720. [Google Scholar] [CrossRef] [Green Version]
- Karaosmanoglu, D.; Karcaaltincaba, M.; Oguz, B.; Akata, D.; Ozmen, M.; Akhan, O. CT findings of lymphoma with peritoneal, omental and mesenteric involvement: Peritoneal lymphomatosis. Eur. J. Radiol. 2009, 71, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Hardy, S.M. Signs in imaging: The sandwich sign. Radiology 2003, 226, 651–652. [Google Scholar] [CrossRef]
- Kim, Y.; Cho, O. Peritoneal lymphomatosis: CT findings. Abdom. Imaging 1998, 23, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.; Sanchez, T.R.S. Diffuse peritoneal lymphomatosis: Atypical presentation of Burkitt lymphoma. Pediatr. Radiol. 2009, 39, 274–276. [Google Scholar] [CrossRef] [PubMed]
- Balthazar, E.J.; Noordhoorn, M. CT of small-bowel lymphoma in immunocompetent patients and patients with AIDS: Comparison of findings. AJR Am. J. Roentgenol. 1997, 168, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Tamara, N.O.; Jyothi, P. Peritoneal sarcomatosis versus peritoneal carcinomatosis: Imaging findings at MDCT. AJR Am. J. Roentgenol. 2010, 195, W229–W235. [Google Scholar]
- Bilimoria, M.M.; Holtz, D.J. Tumor volume as a prognostic factor for sarcomatosis. Cancer 2002, 94, 2441–2446. [Google Scholar] [CrossRef]




































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Favoured PC Sites | Underlying Reason |
|---|---|
| Ileocecal region | Anchor of the small bowel mesentery |
| Sigmoid mesocolon | Area of arrested flow |
| Right paracolic gutter | Major gravity dependent pathway |
| Subhepatic space | Gravity dependence |
| Right subphrenic space and omentum | Resorption sites |
| Content | T1 | T2 | CT | Primary Tumour |
|---|---|---|---|---|
| Melanin | ↑ | ↓ | ↓ | Melanoma |
| Calcium | ↑= | ↓= | ↑ | Mucinous tumors (ovary, stomach, colon, pancreas, appendix, gallbladder, urachus) Serous papillary ovarian tumour |
| Blood | ↑ ↑ | ↓ ↑ | ↑ | Hypervascular tumours. High-grade ovarian tumours (serous and endometrioid adenocarcinoma). Clear cell ovarian carcinoma Granulosa cell tumour. In the subacute stage of a haematoma, the methemoglobin causes a high SI on T1WI, and a variable SI on T2WI (low in early subacute stage, high in late subacute stage). |
| Myxoid | ↓ | ↑ | ↓ | Myxoid tumours |
| Non mineralized cartilage | ↓ | ↑ | ↓ | Condrosarcoma |
| Mucin | ↓ | ↑ | ↓ | Mucinous tumours (ovary, stomach, colon, pancreas, appendix, gallbladder, urachus) |
| Keratin | ↓ | ↑ | ↓ | Squamous differentiation |
| Hypervascular Deposits | Hypovascular Deposits |
|---|---|
| Ovarian (clear cell, granulosa) | Mucinous tumours (ovary, stomach, colon, pancreas, appendix, gallbladder, urachus) |
| Breast carcinoma | Pancreas adenocarcinoma |
| Lung carcinoma | Liposarcoma (myxoid or undifferentiated) |
| Melanoma | |
| Sarcoma: - GIST - Leiomyosarcoma - Fibrous solitary tumour | |
| Renal cell carcinoma | |
| Neuroendocrine tumours | |
| Hepatocellular carcinoma | |
| Thyroid carcinoma | |
| Paraganglioma | |
| Choriocarcinoma |
| Inflammatory | Infectious | Benign Noninflammatory Noninfectious | Malignant |
|---|---|---|---|
| Omental infarction | Peritoneal tuberculosis | Splenosis Accessory spleen | Primary peritoneal serous carcinoma |
| Peritoneal amyloidosis | Peritoneal echinococcosis | Bowel perforation | Pseudomyxoma peritonei |
| Peritoneal sarcoidosis | Encapsulated omental fat necrosis | Peritoneal malignant mesothelioma | |
| Familial Mediterranean fever | Endometriosis | Desmoplastic small round cell tumour | |
| Encapsulated sclerosing peritonitis | Leiomyomatosis peritonealis | Peritoneal lymphomatosis | |
| Desmoid tumours | Peritoneal sarcomatosis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veron Sanchez, A.; Bennouna, I.; Coquelet, N.; Cabo Bolado, J.; Pinilla Fernandez, I.; Mullor Delgado, L.A.; Pezzullo, M.; Liberale, G.; Gomez Galdon, M.; Bali, M.A. Unravelling Peritoneal Carcinomatosis Using Cross-Sectional Imaging Modalities. Diagnostics 2023, 13, 2253. https://doi.org/10.3390/diagnostics13132253
Veron Sanchez A, Bennouna I, Coquelet N, Cabo Bolado J, Pinilla Fernandez I, Mullor Delgado LA, Pezzullo M, Liberale G, Gomez Galdon M, Bali MA. Unravelling Peritoneal Carcinomatosis Using Cross-Sectional Imaging Modalities. Diagnostics. 2023; 13(13):2253. https://doi.org/10.3390/diagnostics13132253
Chicago/Turabian StyleVeron Sanchez, Ana, Ilias Bennouna, Nicolas Coquelet, Jorge Cabo Bolado, Inmaculada Pinilla Fernandez, Luis A. Mullor Delgado, Martina Pezzullo, Gabriel Liberale, Maria Gomez Galdon, and Maria A. Bali. 2023. "Unravelling Peritoneal Carcinomatosis Using Cross-Sectional Imaging Modalities" Diagnostics 13, no. 13: 2253. https://doi.org/10.3390/diagnostics13132253
APA StyleVeron Sanchez, A., Bennouna, I., Coquelet, N., Cabo Bolado, J., Pinilla Fernandez, I., Mullor Delgado, L. A., Pezzullo, M., Liberale, G., Gomez Galdon, M., & Bali, M. A. (2023). Unravelling Peritoneal Carcinomatosis Using Cross-Sectional Imaging Modalities. Diagnostics, 13(13), 2253. https://doi.org/10.3390/diagnostics13132253