
Identification of Histopathological Biomarkers in Fatal Cases of Coronavirus Disease: A Study on Lung Tissue

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Settings and Design
2.2. Histological Processing and Staining
2.3. Microscopic Examination
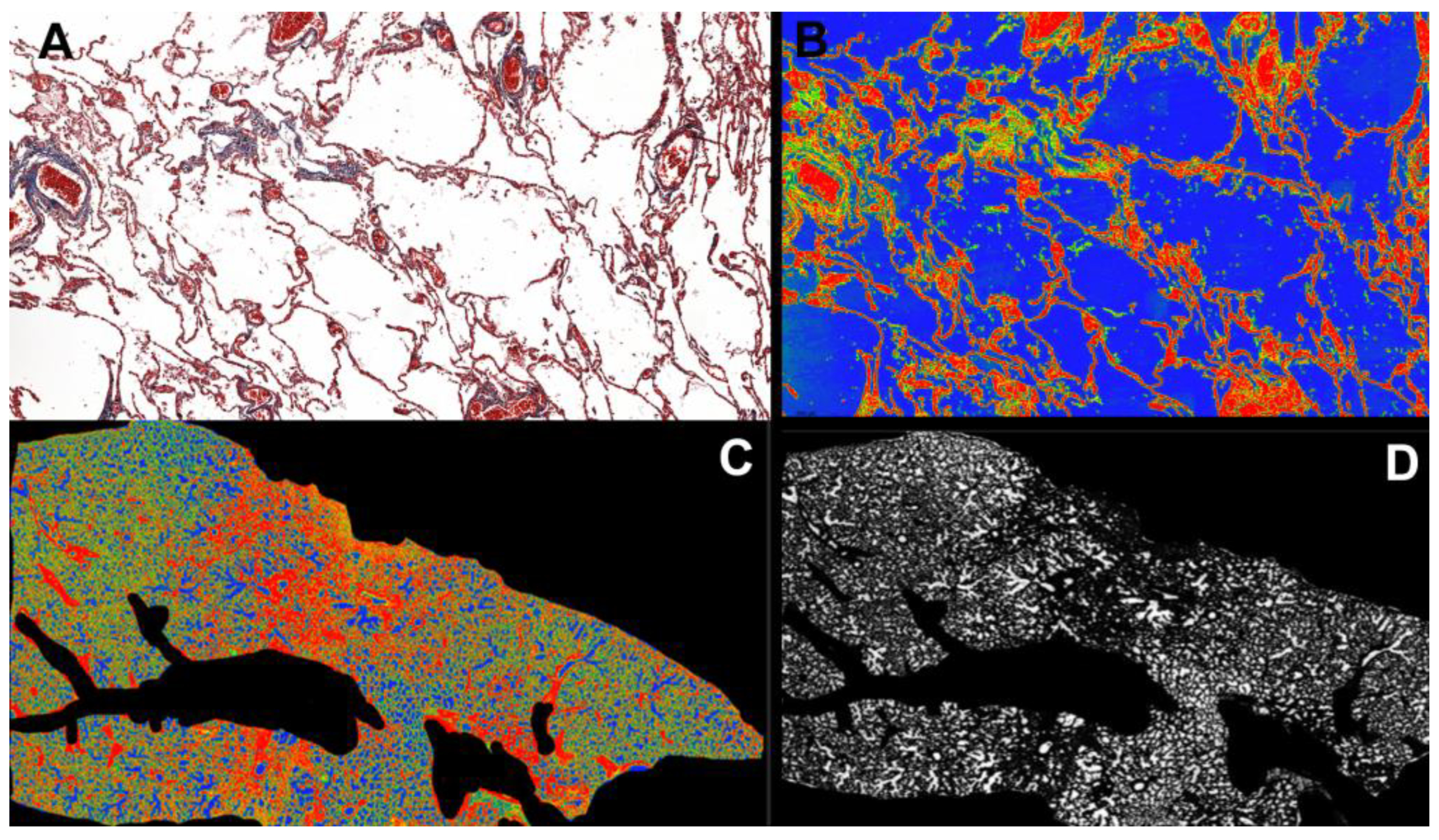
2.4. Morphometric Analysis
2.5. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Macroscopic Findings
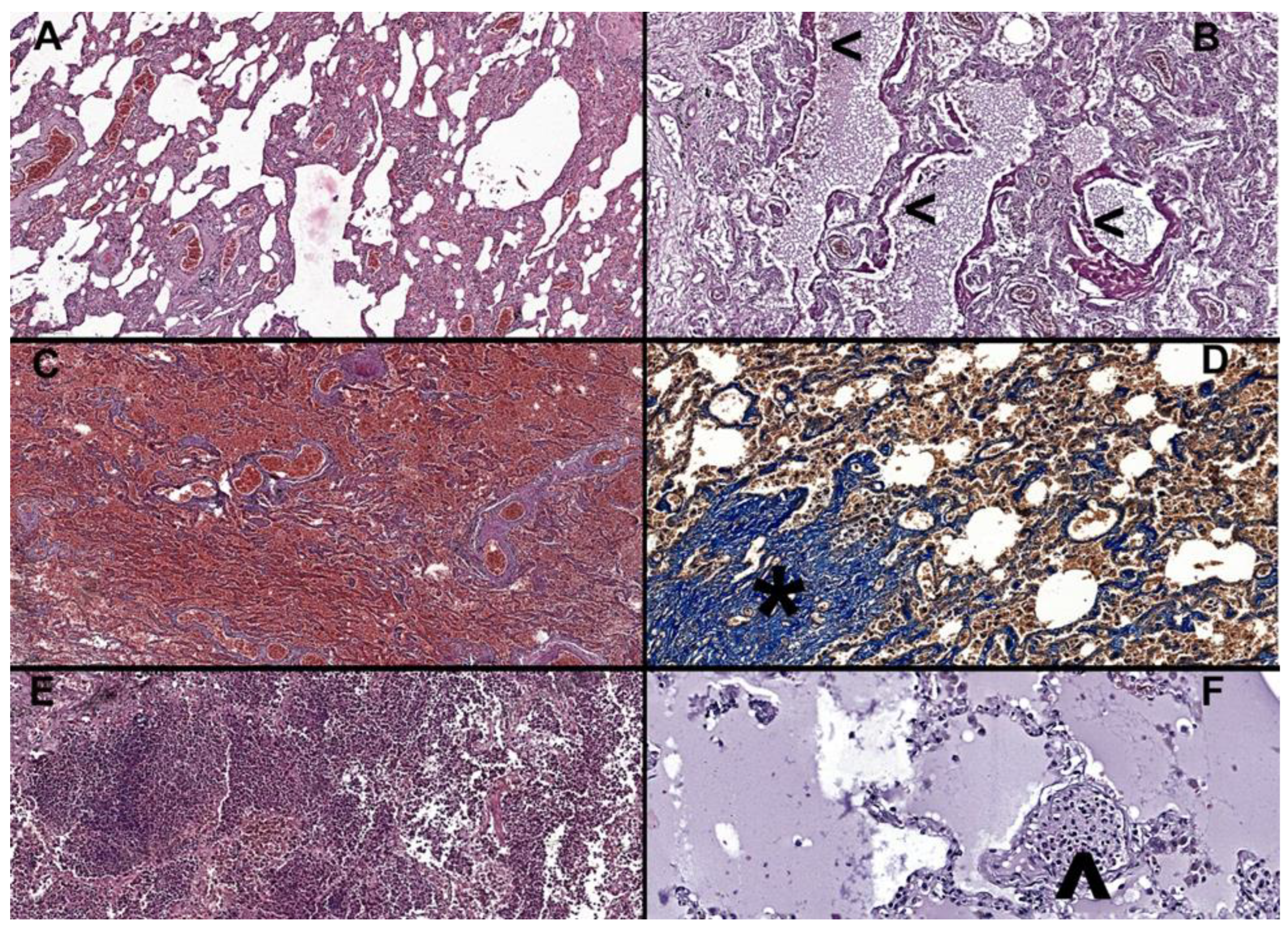
3.3. Microscopic Findings
3.4. Factors Associated with Diffuse Alveolar Damage
4. Discussion
Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Temgoua, M.N.; Endomba, F.T.; Nkeck, J.R.; Kenfack, G.U.; Tochie, J.N.; Essouma, M. Coronavirus Disease 2019 (COVID-19) as a Multi-Systemic Disease and its Impact in Low- and Middle-Income Countries (LMICs). SN Compr. Clin. Med. 2020, 2, 1377–1387. [Google Scholar] [CrossRef] [PubMed]
- Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causesit#:~:text=Human%20disease%20preparedness%20and%20response,virus%20on%2011%20February%202020 (accessed on 7 March 2023).
- Solomon, M.; Liang, C. Human coronaviruses: The emergence of SARS-CoV-2 and management of COVID-19. Virus Res. 2022, 319, 198882. [Google Scholar] [CrossRef] [PubMed]
- Beyerstedt, S.; Casaro, E.B.; Rangel, É.B. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. Eur. J. Clin. Microbiol. Infect Dis. 2021, 40, 905–919. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, Z.; Li, M.; Wang, X. Comparative Review of SARS-CoV-2, SARS-CoV, MERS-CoV, and Influenza A Respiratory Viruses. Front. Immunol. 2020, 11, 552909. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Montero, M.T.V.; Rowe, K.; Kirton, R.; Kunik, F., Jr. Epidemiology, pathogenesis, clinical presentations, diagnosis and treatment of COVID-19: A review of current evidence. Expert. Rev. Clin. Pharmacol. 2021, 14, 601–621. [Google Scholar] [CrossRef]
- Borczuk, A.C. Pulmonary pathology of COVID-19: A review of autopsy studies. Curr. Opin. Pulm. Med. 2021, 27, 184–192. [Google Scholar] [CrossRef]
- Baj, J.; Ciesielka, M.; Buszewicz, G.; Maciejewski, R.; Budzyńska, B.; Listos, P.; Teresiński, G. COVID-19 in the autopsy room-requirements, safety, recommendations, and pathological findings. Forensic. Sci. Med. Pathol. 2021, 17, 101–113. [Google Scholar] [CrossRef]
- Pagani, I.; Ghezzi, S.; Alberti, S.; Poli, G.; Vicenzi, E. Origin and evolution of SARS-CoV-2. Eur. Phys. J. Plus 2023, 138, 157. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Roden, A.C.; Bois, M.C.; Johnson, T.F.; Aubry, M.C.; Alexander, M.P.; Hagen, C.E.; Lin, P.T.; Quinton, R.A.; Maleszewski, J.J.; Boland, J.M. The Spectrum of Histopathologic Findings in Lungs of Patients With Fatal Coronavirus Disease 2019 (COVID-19) Infection. Arch. Pathol. Lab. Med. 2021, 145, 11–21. [Google Scholar] [CrossRef]
- Edler, C.; Schröder, A.S.; Aepfelbacher, M.; Fitzek, A.; Heinemann, A.; Heinrich, F.; Klein, A.; Langenwalder, F.; Lütgehetmann, M.; Meißner, K.; et al. Dying with SARS-CoV-2 infection-an autopsy study of the first consecutive 80 cases in Hamburg, Germany. Int. J. Leg. Med. 2020, 134, 1275–1284. [Google Scholar] [CrossRef] [PubMed]
- Menter, T.; Haslbauer, J.D.; Nienhold, R.; Savic, S.; Hopfer, H.; Deigendesch, N.; Frank, S.; Turek, D.; Willi, N.; Pargger, H.; et al. Postmortem examination of COVID-19 patients reveals diffuse alveolar damage with severe capillary congestion and variegated findings in lungs and other organs suggesting vascular dysfunction. Histopathology 2020, 77, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef]
- Lax, S.F.; Skok, K.; Zechner, P.; Kessler, H.H.; Kaufmann, N.; Koelblinger, C.; Vander, K.; Bargfrieder, U.; Trauner, M. Pulmonary Arterial Thrombosis in COVID-19 With Fatal Outcome: Results From a Prospective, Single-Center, Clinicopathologic Case Series. Ann. Intern. Med. 2020, 173, 350–361. [Google Scholar] [CrossRef]
- Suzuki, H.; Muramatsu, H.; Hayashi, K. Causes of death of forensic autopsy cases tested positive for COVID-19 in Tokyo Metropolis. Japan. Leg. Med. 2023, 62, 102222. [Google Scholar] [CrossRef] [PubMed]
- Viksne, V.; Strumfa, I.; Sperga, M.; Ziemelis, J.; Abolins, J. Pathological Changes in the Lungs of Patients with a Lethal COVID-19 Clinical Course. Diagnostics 2022, 12, 2808. [Google Scholar] [CrossRef]
- Nur Urer, H.; Ersoy, G.; Yılmazbayhan, E.D. Diffuse alveolar damage of the lungs in forensic autopsies: Assessment of histopathological stages and causes of death. Sci. World J. 2012, 2012, 657316. [Google Scholar] [CrossRef]
- Panchabhai, T.S.; Farver, C.; Highland, K.B. Lymphocytic Interstitial Pneumonia. Clin. Chest Med. 2016, 37, 463–474. [Google Scholar] [CrossRef]
- Corrin, B.; Nicholson, A. Pathology of the Lungs, 3rd ed.; Churchill Livingstone Elsevier: London, UK, 2011; pp. 1–39. [Google Scholar]
- Ashcroft, T.; Simpson, J.M.; Timbrell, V. Simple method of estimating the severity of pulmonary fibrosis on a numerical scale. J. Clin. Pathol. 1988, 41, 467–470. [Google Scholar] [CrossRef]
- Tracking of hCoV-19 Variants. Available online: https://gisaid.org/hcov19-variants/ (accessed on 7 March 2023).
- Bendel, R.B.; Afifi, A.A. Comparison of stopping rules in forward regression. J. Am. Stat. Assoc. 1977, 72, 46–53. [Google Scholar] [CrossRef]
- Crapo, J.D.; Morris, A.H.; Gardner, R.M. Reference spirometric values using techniques and equipment that meet ATS recommendations. Am. Rev. Respir. Dis. 1981, 123, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Weibel, E.R. Lung morphometry: The link between structure and function. Cell Tissue Res. 2017, 367, 413–426. [Google Scholar] [CrossRef] [PubMed]
- Niknam, Z.; Jafari, A.; Golchin, A.; Danesh Pouya, F.; Nemati, M.; Rezaei-Tavirani, M.; Rasmi, Y. Potential therapeutic options for COVID-19: An update on current evidence. Eur. J. Med. Res. 2022, 27, 6. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Yang, L.; Pan, J.; Xu, X.; Peng, R. Correlation between vaccine coverage and the COVID-19 pandemic throughout the world: Based on real-world data. J. Med. Virol. 2022, 94, 2181–2187. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.M.; Bai, P.; He, W.; Wu, F.; Liu, X.F.; Han, D.M.; Liu, S.; Yang, J.K. Gender Differences in Patients With COVID-19: Focus on Severity and Mortality. Front. Public Health 2020, 8, 152. [Google Scholar] [CrossRef]
- Yeap, B.B.; Marriott, R.J.; Manning, L.; Dwivedi, G.; Hankey, G.J.; Wu, F.C.W.; Nicholson, J.K.; Murray, K. Higher premorbid serum testosterone predicts COVID-19-related mortality risk in men. Eur. J. Endocrinol. 2022, 187, 159–170. [Google Scholar] [CrossRef]
- Viveiros, A.; Rasmuson, J.; Vu, J.; Mulvagh, S.L.; Yip, C.Y.Y.; Norris, C.M.; Oudit, G.Y. Sex differences in COVID-19: Candidate pathways, genetics of ACE2, and sex hormones. Am. J. Physiol. Heart Circ. Physiol. 2021, 320, H296–H304. [Google Scholar] [CrossRef]
- Lemes, R.M.R.; Costa, A.J.; Bartolomeo, C.S.; Bassani, T.B.; Nishino, M.S.; Pereira, G.J.D.S.; Smaili, S.S.; Maciel, R.M.B.; Braconi, C.T.; da Cruz, E.F.; et al. 17β-estradiol reduces SARS-CoV-2 infection in vitro. Physiol. Rep. 2021, 9, e14707. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Grandmaison, G.L.; Clairand, I.; Durigon, M. Organ weight in 684 adult autopsies: New tables for a Caucasoid population. Forensic. Sci. Int. 2001, 119, 149–154. [Google Scholar] [CrossRef]
- Matoba, K.; Hyodoh, H.; Murakami, M.; Saito, A.; Matoba, T.; Ishida, L.; Fujita, E.; Yamase, M.; Jin, S. Estimating normal lung weight measurement using postmortem CT in forensic cases. Leg. Med. 2017, 29, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, F.; Pezzuto, F.; Fortarezza, F.; Hofman, P.; Kern, I.; Panizo, A.; von der Thüsen, J.; Timofeev, S.; Gorkiewicz, G.; Lunardi, F. Pulmonary pathology and COVID-19: Lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch. 2020, 477, 359–372. [Google Scholar] [CrossRef]
- Valdebenito, S.; Bessis, S.; Annane, D.; Lorin de la Grandmaison, G.; Cramer-Bordé, E.; Prideaux, B.; Eugenin, E.A.; Bomsel, M. COVID-19 Lung Pathogenesis in SARS-CoV-2 Autopsy Cases. Front. Immunol. 2021, 12, 735922. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Ballotta, A.; Di Dedda, U.; Baryshnikova, E.; Dei Poli, M.; Resta, M.; Falco, M.; Albano, G.; Menicanti, L. The procoagulant pattern of patients with COVID-19 acute respiratory distress syndrome. J. Thromb. Haemost. 2020, 18, 1747–1751. [Google Scholar] [CrossRef]
- Ebner, J.; Van den Nest, M.; Bouvier-Azula, L.; Füszl, A.; Gabler, C.; Willinger, B.; Diab-Elschahawi, M.; Presterl, E. Routine Surveillance of Healthcare-Associated Infections Misses a Significant Proportion of Invasive Aspergillosis in Patients with Severe COVID-19. J. Fungi 2022, 8, 273. [Google Scholar] [CrossRef] [PubMed]
- Kurra, N.; Woodard, P.I.; Gandrakota, N.; Gandhi, H.; Polisetty, S.R.; Ang, S.P.; Patel, K.P.; Chitimalla, V.; Ali Baig, M.M.; Samudrala, G. Opportunistic Infections in COVID-19: A Systematic Review and Meta-Analysis. Cureus 2022, 14, e23687. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Trias-Sabrià, P.; Dorca Duch, E.; Molina-Molina, M.; Aso, S.; Díez-Ferrer, M.; Marín Muñiz, A.; Bordas-Martínez, J.; Sabater, J.; Luburich, P.; Del Rio, B.; et al. Radio-Histological Correlation of Lung Features in Severe COVID-19 Through CT-Scan and Lung Ultrasound Evaluation. Front. Med. 2022, 9, 820661. [Google Scholar] [CrossRef]
- George, P.M.; Wells, A.U.; Jenkins, R.G. Pulmonary fibrosis and COVID-19: The potential role for antifibrotic therapy. Lancet Respir. Med. 2020, 8, 807–815. [Google Scholar] [CrossRef]
- Francone, M.; Iafrate, F.; Masci, G.M.; Coco, S.; Cilia, F.; Manganaro, L.; Panebianco, V.; Andreoli, C.; Colaiacomo, M.C.; Zingaropoli, M.A.; et al. Chest CT score in COVID-19 patients: Correlation with disease severity and short-term prognosis. Eur. Radiol. 2020, 30, 6808–6817. [Google Scholar] [CrossRef]
- Pan, F.; Ye, T.; Sun, P.; Gui, S.; Liang, B.; Li, L.; Zheng, D.; Wang, J.; Hesketh, R.L.; Yang, L.; et al. Time Course of Lung Changes at Chest CT during Recovery from Coronavirus Disease 2019 (COVID-19). Radiology 2020, 295, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Barton, L.M.; Duval, E.J.; Stroberg, E.; Ghosh, S.; Mukhopadhyay, S. COVID-19 Autopsies, Oklahoma, USA. Am. J. Clin. Pathol. 2020, 153, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Borczuk, A.C.; Salvatore, S.P.; Seshan, S.V.; Patel, S.S.; Bussel, J.B.; Mostyka, M.; Elsoukkary, S.; He, B.; Del Vecchio, C.; Fortarezza, F.; et al. COVID-19 pulmonary pathology: A multi-institutional autopsy cohort from Italy and New York City. Mod. Pathol. 2020, 33, 2156–2168. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors | Year * | Country | Age Range (Years) | Sample Size | Macroscopic Findings | Microscopic Findings |
|---|---|---|---|---|---|---|
| Fox et al. [10] | 2020 | US | 44–78 | 10 | (a) Pleurisy; (b) patchy pattern edema; (c) pulmonary infarction | (a) DAD; (b) microthrombi |
| Roden et al. [11] | 2020 | US | 69–94 | 8 | (a) Consolidation; (b) pleurisy; (c) patchy pattern; (d) fibrosis; (e) pulmonary embolism | (a) DAD; (b) squamous metaplasia; (c) bronchopneumonia; (d) pulmonary embolism |
| Edler et al. [12] | 2020 | Germany | 52–96 | 80 | (a) Congestion; (b) pleurisy; (c) patchy pattern; (d) tracheobronchitis; (e) bronchopneumonia | (a) DAD; (b) squamous metaplasia; (c) bronchopneumonia; (d) fibrosis |
| Menter et al. [13] | 2020 | Switzerland | 53–96 | 21 | (a) Severe congestion; (b) consolidation; (c) bronchopneumonia | (a) DAD; (b) capillary stasis; (c) bronchopneumonia; (d) interstitial pneumonia; (e) edema; (f) microthrombi; (g) pulmonary embolism |
| Carsana et al. [14] | 2020 | Italy | 32–86 | 38 | (a) Congestion; (b) edema; (c) patchy pattern | (a) DAD; (b) capillary stasis; (c) bronchopneumonia; (d) interstitial pneumonia; (e) edema; (f) microthrombi; (g) atypical pneumocytes; (h) fibrosis |
| Lax et al. [15] | 2020 | Austria | 75–91 | 11 | (a) Congestion; (b) emphysema; (c) pulmonary embolism; (d) pulmonary infarction | (a) DAD; (b) bronchopneumonia; (c) interstitial pneumonia; (d) edema; (e) microthrombi; (f) fibrosis; |
| Suzuki et al. [16] | 2022 | Japan | 28–96 | 41 | (a) Consolidation; (b) tracheobronchitis; (c) pulmonary embolism | (a) DAD; (b) bronchopneumonia; (c) tracheobronchitis; (d) microthrombi |
| Viksne et al. [17] | 2022 | Latvia | 22–94 | 88 | No data | (a) DAD; (b) microthrombi; (c) pulmonary embolism; (d) fibrosis |
| Characteristic | All, n = 79 no. (%) | <70 Years, n = 36 no. (%) | ≥70 Years, n = 43 no. (%) | Stat. (p-Value) |
|---|---|---|---|---|
| Sex | 1.2 (0.2721) | |||
| Female | 20 (25.3) | 7 (19.4) | 13 (30.2) | |
| Male | 59 (74.7) | 29 (80.6) | 30 (69.8) | |
| Living area | 0.5 (0.4988) | |||
| Urban | 54 (68.4) | 26 (72.2) | 28 (65.1) | |
| Rural | 25 (31.6) | 10 (27.8) | 15 (34.9) | |
| Class of BMI | 4.4 (0.2220) | |||
| underweight | 13 (16.5) | 3 (8.3) | 10 (23.3) | |
| normal | 22 (27.8) | 10 (27.8) | 12 (27.9) | |
| obesity grade 1–2 | 35 (44.3) | 17 (47.2) | 18 (41.9) | |
| obesity grade 3 | 9 (11.4) | 6 (16.7) | 3 (7) | |
| Comorbidities | ||||
| Arterial hypertension | 30 (38) | 12 (33.3) | 18 (41.9) | 0.6 (0.4367) |
| Type 2 diabetes mellitus | 15 (19) | 6 (16.7) | 9 (20.9) | 0.2 (0.6304) |
| Congestive heart failure | 10 (12.7) | 4 (11.1) | 5 (11.6) | n.a (0.8622) |
| COPD | 7 (8.9) | 3 (8.3) | 4 (9.3) | n.a (0.8480) |
| Myocardial infarction | 5 (6.3) | 0 (0) | 5 (11.6) | n.a (0.0381) |
| Hepatic steatosis | 6 (7.6) | 2 (5.6) | 4 (9.3) | n.a (0.5431) |
| Malign tumors | 7 (8.9) | 3 (8.3) | 4 (9.3) | n.a (0.8480) |
| Stroke | 6 (7.6) | 1 (2.8) | 5 (11.6) | n.a (0.1496) |
| Characteristic | All, n = 79 | <70 Years, n = 36 | ≥70 Years, n = 43 | Stat. (p-Value) |
|---|---|---|---|---|
| Combined lung weight, g | 1.5 (0.1276) * | |||
| median [Q1 to Q3] | 1748 [1338 to 2090] | 1830 [1505 to 2115] | 1645 [1235 to 1865] | |
| {min to max} | {610 to 3005} | {1225 to 2425} | {610 to 3005} | |
| Patchy pattern, no. (%) | 63 (79.7) | 30 (83.3) | 33 (76.7) | 0.5 (0.468) |
| Bloody exudate, no. (%) | 62 (78.5) | 33 (91.7) | 29 (67.4) | 6.8 (0.0091) |
| Edema exudate, no. (%) | 58 (73.4) | 27 (75) | 31 (72.1) | 0.1 (0.7708) |
| Purulent exudate, no. (%) | 17 (21.5) | 5 (13.9) | 12 (27.9) | 2.3 (0.1311) |
| Pulmonary infarction, no. (%) | 39 (49.4) | 20 (55.6) | 19 (44.2) | 1 (0.3141) |
| Characteristic | All, n = 79 | <70 Years, n = 36 | ≥70 Years, n = 43 | Stat. (p-Value) |
|---|---|---|---|---|
| DAD, no. (%) | n.a. (0.1354) | |||
| Absent | 37 (46.8) | 12 (33.3) | 25 (58.1) | |
| Exudative phase | 22 (27.8) | 13 (36.1) | 9 (20.9) | |
| Organizing phase | 15 (19) | 9 (25) | 6 (14) | |
| Fibrosis phase | 5 (6.3) | 2 (5.6) | 3 (7) | |
| Lung congestion, no. (%) | n.a. (0.9935) | |||
| Absent | 8 (10.1) | 4 (11.1) | 4 (9.3) | |
| Slight | 22 (27.8) | 10 (27.8) | 12 (27.9) | |
| Moderate | 29 (36.7) | 13 (36.1) | 16 (37.2) | |
| Severe | 20 (25.3) | 9 (25) | 11 (25.6) | |
| Microthrombi, no. (%) | 31 (39.2) | 13 (36.1) | 18 (41.9) | 0.3 (0.6022) |
| Epithelial desquamation, no. (%) | n.a. (0.8561) | |||
| Absent | 50 (63.3) | 21 (58.3) | 29 (67.4) | |
| Slight | 15 (19) | 8 (22.2) | 7 (16.3) | |
| Moderate | 10 (12.7) | 5 (13.9) | 5 (11.6) | |
| Severe | 4 (5.1) | 2 (5.6) | 2 (4.7) | |
| Bronchopneumonia, no. (%) | 14 (17.7) | 3 (8.3) | 11 (25.6) | 4.0 (0.0456) |
| Tracheobronchitis, no. (%) | 12 (15.2) | 3 (8.3) | 9 (20.9) | 2.4 (0.1203) |
| Alveolar edema, no. (%) | 66 (83.5) | 31 (86.1) | 35 (81.4) | 0.3 (0.5734) |
| Interstitial edema, no. (%) | 11 (13.9) | 2 (5.6) | 9 (20.9) | 3.9 (0.0493) |
| Antrachotic pigment, no. (%) | 3.6 (0.1688) | |||
| Absent | 48 (60.8) | 25 (69.4) | 23 (53.5) | |
| Slight | 16 (20.3) | 4 (11.1) | 12 (27.9) | |
| Moderate | 15 (19) | 7 (19.4) | 8 (18.6) | |
| Interstitial pneumonia, no. (%) | 59 (74.7) | 29 (80.6) | 30 (69.8) | 1.2 (0.2721) |
| Emphysema, no. (%) | 40 (50.6) | 17 (47.2) | 23 (53.5) | 0.3 (0.5790) |
| Ashcroft Score | −0.4 (0.6692) | |||
| Median [Q1 to Q3] | 2 [1 to 3] | 2 [1 to 3] | 2 [1 to 3] | |
| {min to max} | {0 to 6} | {0 to 6} | {0 to 6} | |
| Proliferative nodules (no./25 cm2) | −1.2 (0.2348) | |||
| Median [Q1 to Q3] | 2 [0 to 3.3] | 1 [0 to 3] | 2 [0 to 4] | |
| {min to max} | {0 to 11} | {0 to 7} | {0 to 11} | |
| Alveolar air capacity | −0.4 (0.6616) | |||
| Median [Q1 to Q3] | 12.5 [7 to 20.1] | 11.4 [6.8 to 21.5] | 12.8 [7.9 to 17.1] | |
| {min to max} | {1 to 50.5} | {1.8 to 50.5} | {1 to 32.5} |
| Variable | Univariable | Multivariable * | ||
|---|---|---|---|---|
| OR [95%CI] | p-Value | OR [95%CI] | p-Value | |
| Age, years | 0.96 [0.92 to 0.99] | 0.0204 | 0.96 [0.92 to 0.99] | 0.0190 |
| Obesity | 2.12 [0.86 to 5.23] | 0.1036 | ||
| Variant, alpha = reference | 7.00 [1.45 to 33.80] | 0.0154 | 7.59 [1.51 to 38.10] | 0.0138 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gheban-Roșca, I.-A.; Gheban, B.-A.; Pop, B.; Mironescu, D.-C.; Siserman, V.C.; Jianu, E.M.; Drugan, T.; Bolboacă, S.D. Identification of Histopathological Biomarkers in Fatal Cases of Coronavirus Disease: A Study on Lung Tissue. Diagnostics 2023, 13, 2039. https://doi.org/10.3390/diagnostics13122039
Gheban-Roșca I-A, Gheban B-A, Pop B, Mironescu D-C, Siserman VC, Jianu EM, Drugan T, Bolboacă SD. Identification of Histopathological Biomarkers in Fatal Cases of Coronavirus Disease: A Study on Lung Tissue. Diagnostics. 2023; 13(12):2039. https://doi.org/10.3390/diagnostics13122039
Chicago/Turabian StyleGheban-Roșca, Ioana-Andreea, Bogdan-Alexandru Gheban, Bogdan Pop, Daniela-Cristina Mironescu, Vasile Costel Siserman, Elena Mihaela Jianu, Tudor Drugan, and Sorana D. Bolboacă. 2023. "Identification of Histopathological Biomarkers in Fatal Cases of Coronavirus Disease: A Study on Lung Tissue" Diagnostics 13, no. 12: 2039. https://doi.org/10.3390/diagnostics13122039
APA StyleGheban-Roșca, I.-A., Gheban, B.-A., Pop, B., Mironescu, D.-C., Siserman, V. C., Jianu, E. M., Drugan, T., & Bolboacă, S. D. (2023). Identification of Histopathological Biomarkers in Fatal Cases of Coronavirus Disease: A Study on Lung Tissue. Diagnostics, 13(12), 2039. https://doi.org/10.3390/diagnostics13122039