
Prediction of Cognitive Decline in Parkinson’s Disease Using Clinical and DAT SPECT Imaging Features, and Hybrid Machine Learning Systems

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Method and Martial
2.1. Patient Data and Data Processing Steps
2.1.1. CF Collection
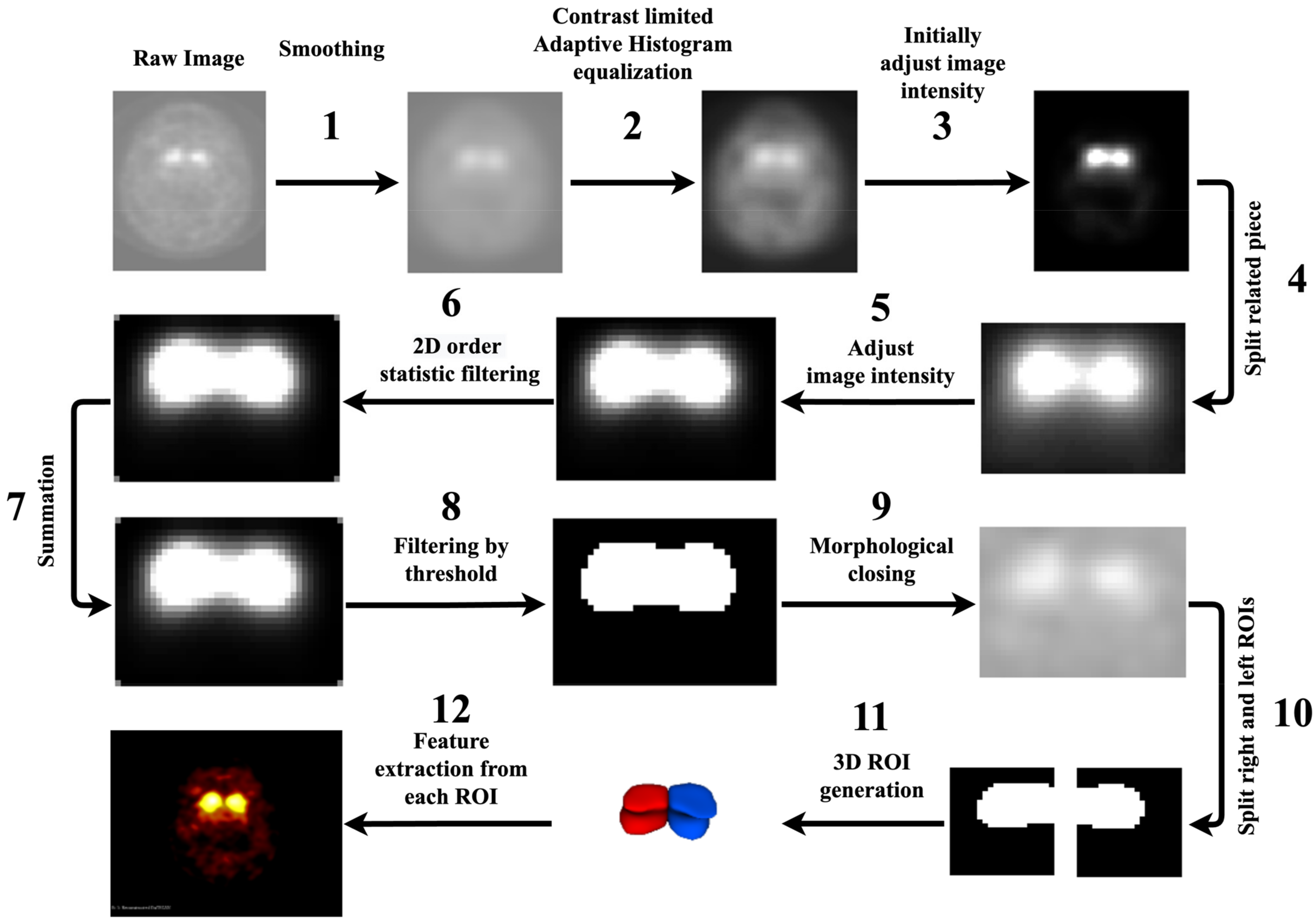
2.1.2. RF Extraction
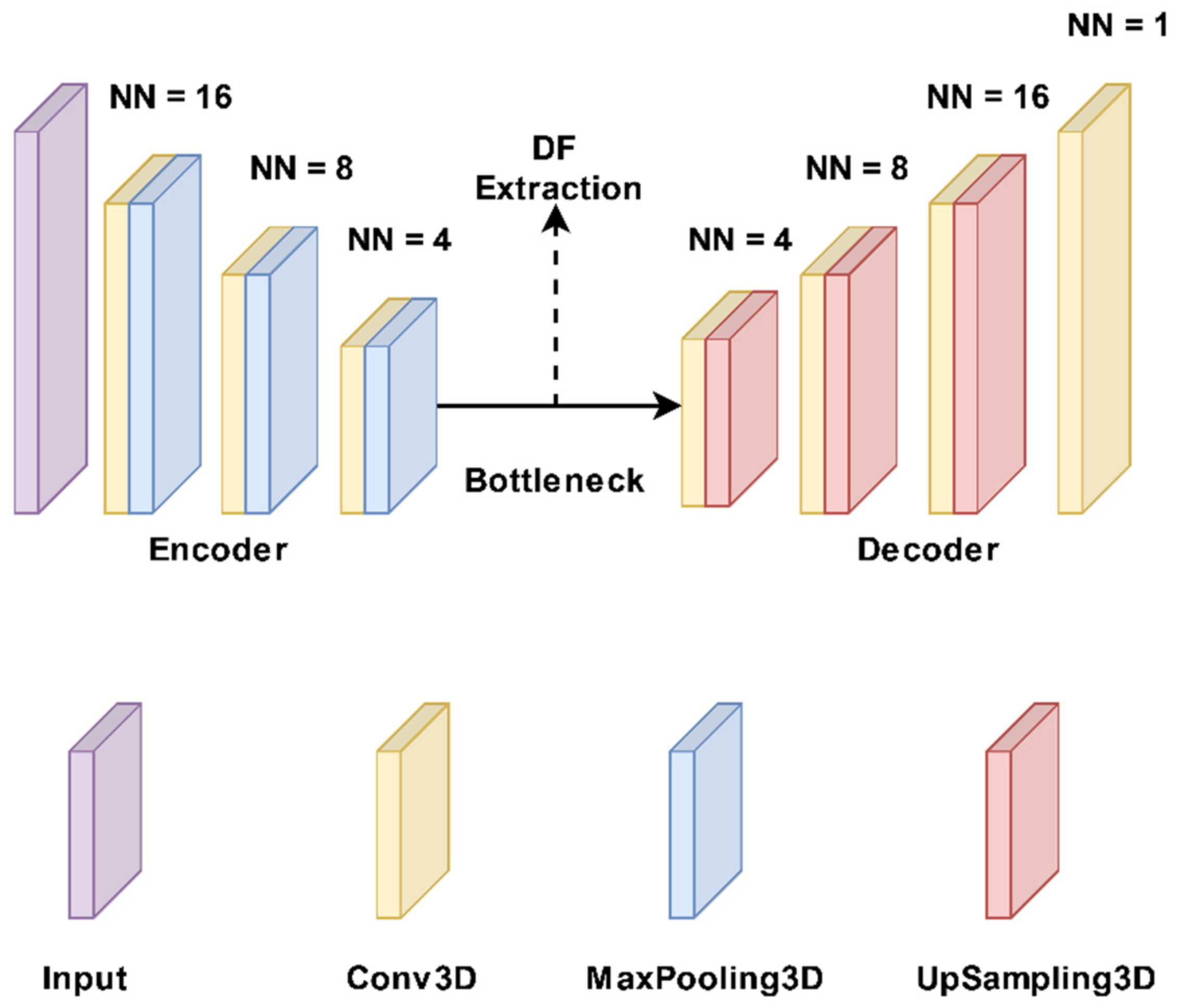
2.1.3. DF Extraction
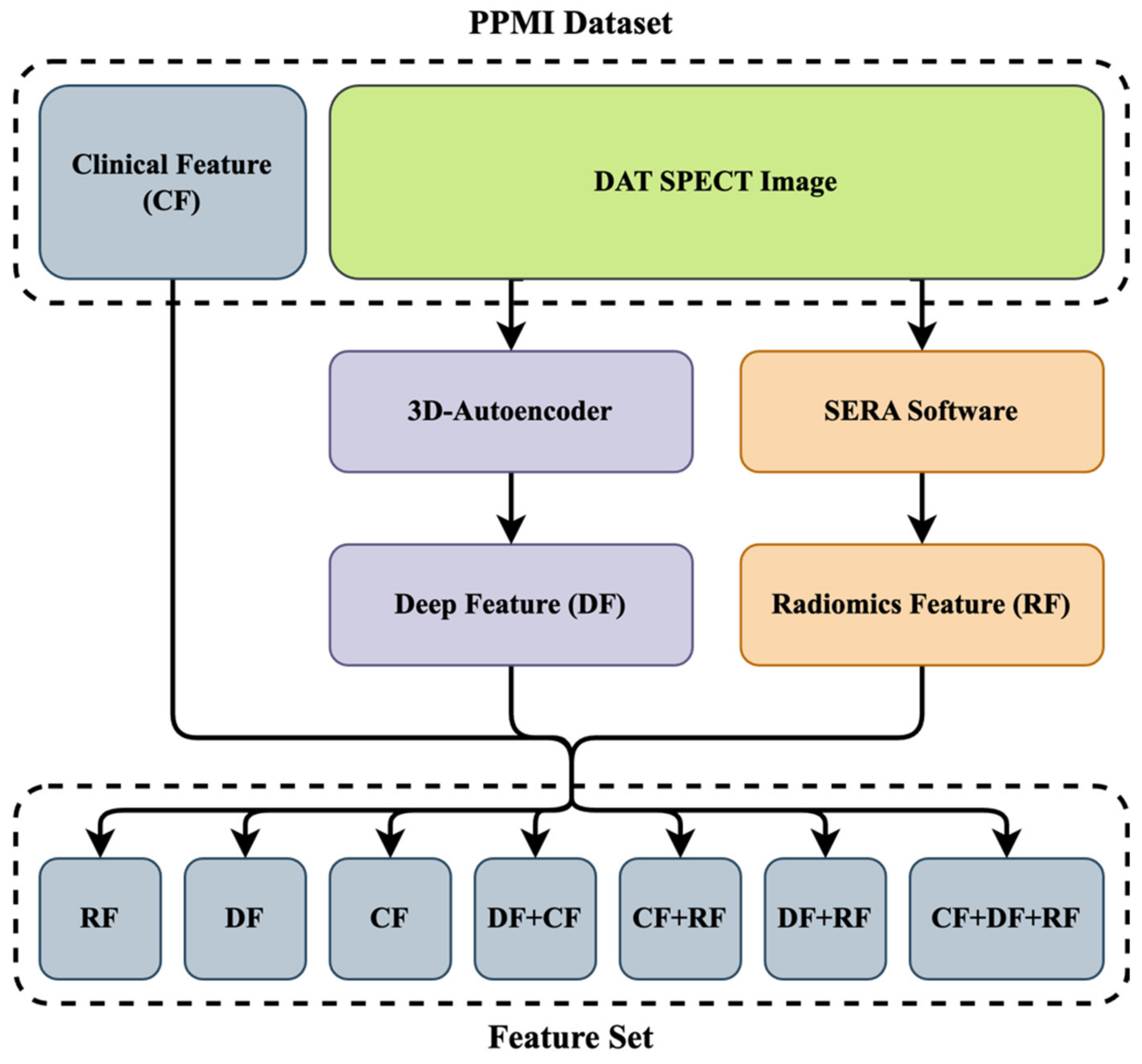
2.1.4. Dataset Preparation
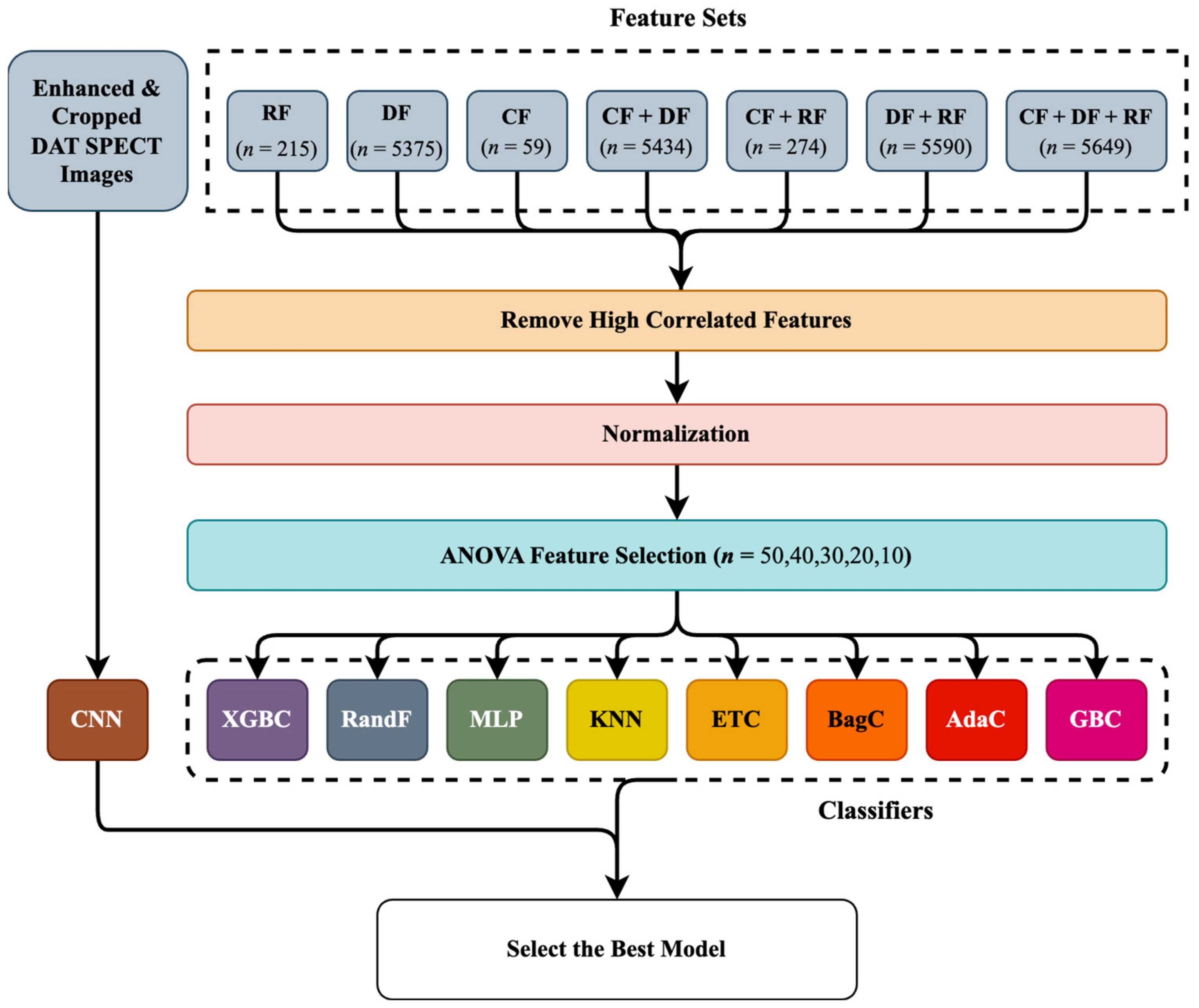
2.2. ML Algorithms
2.2.1. Hybrid Machine Learning Systems (HMLSs)
ANOVA (Analysis of Variance) Feature Selection Algorithm
Classifiers
2.2.2. End-to-End CNN Learning Classifier
2.3. Analysis Procedure
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aarsland, D.; Creese, B.; Politis, M.; Chaudhuri, K.R.; Ffytche, D.H.; Weintraub, D.; Ballard, C. Cognitive Decline in Parkinson Disease. Nat. Rev. Neurol. 2017, 13, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s Disease: Clinical Features and Diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed]
- GBD 2016 Parkinson’s Disease Collaborators. Global, Regional, and National Burden of Parkinson’s Disease, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef]
- Salmanpour, M.; Shamsaei, M.; Saberi Manesh, A.; Klyuzhin, I.; Tang, J.; Sossi, V.; Rahmim, A. Machine Learning Methods for Optimal Prediction of Motor Outcome in Parkinson’s Disease. Phys. Med. 2020, 69, 233–240. [Google Scholar] [CrossRef]
- Chen, F.; Li, Y.; Ye, G.; Zhou, L.; Bian, X.; Liu, J. Development and Validation of a Prognostic Model for Cognitive Impairment in Parkinson’s Disease With REM Sleep Behavior Disorder. Front. Aging Neurosci. 2021, 13, 703158. [Google Scholar] [CrossRef] [PubMed]
- Langston, J.W. The Parkinson’s Complex: Parkinsonism Is Just the Tip of the Iceberg. Ann. Neurol. 2006, 59, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Camargo, C.H.F.; Tolentino, E.D.S.; Bronzini, A.; Ladeira, M.D.A.; Lima, R.; Schultz-Pereira, G.L.; Young-Blood, M.R. Comparison of the Use of Screening Tools for Evaluating Cognitive Impairment in Patients with Parkinson’s Disease. Dement. Neuropsychol. 2016, 10, 344–350. [Google Scholar] [CrossRef]
- Marek, K.; Chowdhury, S.; Siderowf, A.; Lasch, S.; Coffey, C.S.; Caspell-Garcia, C.; Simuni, T.; Jennings, D.; Tanner, C.M.; Trojanowski, J.Q.; et al. The Parkinson’s Progression Markers Initiative (PPMI)–Establishing a PD Biomarker Cohort. Ann. Clin. Transl. Neurol. 2018, 5, 1460–1477. [Google Scholar] [CrossRef]
- Wojtowicz, A.; Larner, A.J. Diagnostic Test Accuracy of Cognitive Screeners in Older People. Prog. Neurol. Psychiatry 2017, 21, 17–21. [Google Scholar] [CrossRef]
- Hely, M.A.; Morris, J.G.; Traficante, R.; Reid, W.G.; O’Sullivan, D.J.; Williamson, P.M. The Sydney Multicentre Study of Parkinson’s Disease: Progression and Mortality at 10 Years. J. Neurol. Neurosurg. Psychiatry 1999, 67, 300–307. Available online: https://pubmed.ncbi.nlm.nih.gov/10449550/ (accessed on 25 April 2023). [CrossRef] [PubMed]
- De Lau, L.M.; Breteler, M.M. Epidemiology of Parkinson’s Disease. Lancet Neurol. 2006, 5, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Bertrand, J.-A.; Montplaisir, J.; Desjardins, C.; Vendette, M.; Rios Romenets, S.; Panisset, M.; Gagnon, J.-F. Rapid Eye Movement Sleep Behavior Disorder and Risk of Dementia in Parkinson’s Disease: A Prospective Study. Mov. Disord. Off. J. Mov. Disord. Soc. 2012, 27, 720–726. [Google Scholar] [CrossRef] [PubMed]
- Krüger, R.; Klucken, J.; Weiss, D.; Tönges, L.; Kolber, P.; Unterecker, S.; Lorrain, M.; Baas, H.; Müller, T.; Riederer, P. Classification of Advanced Stages of Parkinson’s Disease: Translation into Stratified Treatments. J. Neural Transm. 2017, 124, 1015–1027. [Google Scholar] [CrossRef] [PubMed]
- Javanmardi, A.; Salmanpour, M.R.; Rahmim, A. Do DTI Features Add Value to Clinical and SPECT Imaging Features for Outcome Prediction in Parkinson’s Disease? J. Nucl. Med. 2021, 62 (Suppl. S1), 1414. Available online: https://jnm.snmjournals.org/content/62/supplement_1/1414.abstract (accessed on 26 October 2022).
- Hajianfar, G.; Kalayinia, S.; Hosseinzadeh, M.; Samanian, S.; Maleki, M.; Rezaeijo, S.M.; Sossi, V.; Rahmim, A.; Salmanpour, M.R. Hybrid Machine Learning Systems for Prediction of Parkinson’s Disease Pathogenic Variants Using Clinical Information and Radiomics Features. J. Nucl. Med. 2022, 63 (Suppl. S2), 2508. Available online: https://jnm.snmjournals.org/content/63/supplement_2/2508.abstract (accessed on 26 October 2022).
- Mu, J.; Chaudhuri, K.R.; Bielza, C.; de Pedro-Cuesta, J.; Larrañaga, P.; Martinez-Martin, P. Parkinson’s Disease Subtypes Identified from Cluster Analysis of Motor and Non-Motor Symptoms. Front. Aging Neurosci. 2017, 9, 301. [Google Scholar] [CrossRef]
- Guo, Y.; Liu, F.-T.; Hou, X.-H.; Li, J.-Q.; Cao, X.-P.; Tan, L.; Wang, J.; Yu, J.-T. Predictors of Cognitive Impairment in Parkinson’s Disease: A Systematic Review and Meta-Analysis of Prospective Cohort Studies. J. Neurol. 2021, 268, 2713–2722. [Google Scholar] [CrossRef]
- Schrag, A.; Siddiqui, U.F.; Anastasiou, Z.; Weintraub, D.; Schott, J.M. Clinical Variables and Biomarkers in Prediction of Cognitive Impairment in Patients with Newly Diagnosed Parkinson’s Disease: A Cohort Study. Lancet Neurol. 2017, 16, 66–75. [Google Scholar] [CrossRef]
- Mazancova, A.F.; Růžička, E.; Jech, R.; Bezdicek, O. Test the Best: Classification Accuracies of Four Cognitive Rating Scales for Parkinson’s Disease Mild Cognitive Impairment. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2020, 35, acaa039. [Google Scholar] [CrossRef]
- Pellecchia, M.T.; Picillo, M.; Santangelo, G.; Longo, K.; Moccia, M.; Erro, R.; Amboni, M.; Vitale, C.; Vicidomini, C.; Salvatore, M.; et al. Cognitive Performances and DAT Imaging in Early Parkinson’s Disease with Mild Cognitive Impairment: A Preliminary Study. Acta Neurol. Scand. 2015, 131, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Andersson, S.; Josefsson, M.; Stiernman, L.J.; Rieckmann, A. Cognitive Decline in Parkinson’s Disease: A Subgroup of Extreme Decliners Revealed by a Data-Driven Analysis of Longitudinal Progression. Front. Psychol. 2021, 12, 729755. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Oh, M.; Oh, J.S.; Moon, H.; Chung, S.J.; Lee, C.S.; Kim, J.S. Association of Striatal Dopaminergic Neuronal Integrity with Cognitive Dysfunction and Cerebral Cortical Metabolism in Parkinson’s Disease with Mild Cognitive Impairment. Nucl. Med. Commun. 2019, 40, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Sarker, I.H. Machine Learning: Algorithms, Real-World Applications and Research Directions. SN Comput. Sci. 2021, 2, 160. [Google Scholar] [CrossRef] [PubMed]
- Salmanpour, M.; Hosseinzadeh, M.; Rezaeijo, S.; Maghsudi, M.; Rahmim, A. Reliable and Reproducible Tensor Radiomics Features in Prediction of Survival in Head and Neck Cancer. E. J. Nucl. Med. Mol. Imag. 2022, 49 (Suppl. S1), S20. [Google Scholar]
- Salmanpour, M.; Hosseinzadeh, M.; Rezaeijo, S.; Ramezani, M.; Marandi, S.; Einy, M.; Rahmim, A. Deep versus Handcrafted Tensor Radiomics Features: Application to Survival Prediction in Head and Neck Cancer. E. J. Nucl. Med. Mol. Imag. 2022, 49 (Suppl. S1), S245–S246. [Google Scholar]
- Salmanpour, M.R.; Hajianfar, G.; Rezaeijo, S.M.; Ghaemi, M.; Rahmim, A. Advanced Automatic Segmentation of Tumors and Survival Prediction in Head and Neck Cancer. In 3D Head and Neck Tumor Segmentation in PET/CT Challenge; Springer: Cham, Switzerland, 2021; pp. 202–210. [Google Scholar]
- Fatan, M.; Hosseinzadeh, M.; Askari, D.; Sheikhi, H.; Rezaeijo, S.M.; Salmanpour, M.R. Fusion-Based Head and Neck Tumor Segmentation and Survival Prediction Using Robust Deep Learning Techniques and Advanced Hybrid Machine Learning Systems. In 3D Head and Neck Tumor Segmentation in PET/CT Challenge; Springer: Cham, Switzerland, 2021; pp. 211–223. [Google Scholar]
- Parekh, V.S.; Jacobs, M.A. Deep Learning and Radiomics in Precision Medicine. Expert Rev. Precis. Med. Drug Dev. 2019, 4, 59–72. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6508888/ (accessed on 26 October 2022). [CrossRef]
- Hassanpour, S.; Langlotz, C.P. Information Extraction from Multi-Institutional Radiology Reports. Artif. Intell. Med. 2016, 66, 29–39. [Google Scholar] [CrossRef]
- Jouzdani, A.F.; Gorji, A.; Hosseinzadeh, M.; Rahmim, A.; Salmanpour, M.R. Prediction of Cognitive Decline in Parkinson’s Disease Using Deep and Handcrafted Radiomics Features. E. J. Nucl. Med. Mol. Imag. 2022, 49 (Suppl. S1), S195–S196. [Google Scholar]
- Salmanpour, M.R.; Hosseinzadeh, M.; Bakhtiari, M.; Gholami, A.R.; Ghaemi, M.M.; Nabizadeh, A.H.; Rezaeijo, S.M.; Rahmim, A. Drug Amount Prediction in Parkinson’s Disease Using Hybrid Machine Learning Systems and Radiomics Features. J. Nucl. Med. 2022, 63 (Suppl. S2), 2256. Available online: https://jnm.snmjournals.org/content/63/supplement_2/2256.abstract (accessed on 26 October 2022). [CrossRef]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Lin, X.; Zhao, Y.; Li, L.; Yan, K.; Liang, D.; Li, Z.C. Deep Learning vs. Radiomics for Predicting Axillary Lymph Node Metastasis of Breast Cancer Using Ultrasound Images: Don’t Forget the Peritumoral Region. Front. Oncol. 2020, 10, 53. Available online: https://www.frontiersin.org/articles/10.3389/fonc.2020.00053/full (accessed on 26 October 2022). [CrossRef] [PubMed]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.W.L.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The Process and the Challenges. Magn. Reson. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [PubMed]
- Rahmim, A.; Toosi, A.; Salmanpour, M.R.; Dubljevic, N.; Janzen, I.; Shiri, I.; Ramezani, M.A.; Yuan, R.; Ho, C.; Zaidi, H.; et al. Tensor Radiomics: Paradigm for Systematic Incorporation of Multi-Flavoured Radiomics Features. arXiv 2022, arXiv:2203.06314. [Google Scholar]
- Eroglu, Y.; Yildirim, M.; Cinar, A. MRMR-based Hybrid Convolutional Neural Network Model for Classification of Alzheimer’s Disease on Brain Magnetic Resonance Images. Int. J. Imaging Syst. Technol. 2022, 32, 517–527. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1002/ima.22632 (accessed on 5 April 2023). [CrossRef]
- Salmanpour, M.R.; Shamsaei, M.; Saberi, A.; Setayeshi, S.; Klyuzhin, I.S.; Sossi, V.; Rahmim, A. Optimized Machine Learning Methods for Prediction of Cognitive Outcome in Parkinson’s Disease. Comput. Biol. Med. 2019, 111, 103347. [Google Scholar] [CrossRef]
- Salmapour, M.; Bakhtiary, M.; HosseinZadeh, M.; Maghsudi, M.; Yousefirizi, F.; Ghaemi, M.M.; Rahmim, A. Application of Novel Hybrid Machine Learning Systems and Radiomics Features for Non-Motor Outcome Prediction in Parkinson’s Disease. Phys. Med. Biol. 2022, 63, 3233. Available online: https://iopscience.iop.org/article/10.1088/1361-6560/acaba6 (accessed on 5 April 2023).
- Salmanpour, M.R.; Hosseinzadeh, M.; Bakhtiari, M.; Ghaemi, M.M.; Rezaeijo, S.M.; Nabizadeh, A.H.; Rahmim, A. Cognitive Outcome Prediction in Parkinson’s Disease Using Hybrid Machine Learning Systems and Radiomics Features. J. Nucl. Med. 2022, 63 (Suppl. S2), 3233. Available online: https://jnm.snmjournals.org/content/63/supplement_2/3233.abstract (accessed on 26 October 2022).
- Kandiah, N.; Zhang, A.; Cenina, A.R.; Au, W.L.; Nadkarni, N.; Tan, L.C. Montreal Cognitive Assessment for the Screening and Prediction of Cognitive Decline in Early Parkinson’s Disease. Parkinsonism Relat. Disord. 2014, 20, 1145–1148. [Google Scholar] [CrossRef]
- Salmanpour, M.R.; Shamsaei, M.; Saberi, A.; Hajianfar, G.; Soltanian-Zadeh, H.; Rahmim, A. Robust Identification of Parkinson’s Disease Subtypes Using Radiomics and Hybrid Machine Learning. Comput. Biol. Med. 2021, 129, 104142. [Google Scholar] [CrossRef]
- Salmanpour, M.R.; Shamsaei, M.; Hajianfar, G.; Soltanian-Zadeh, H.; Rahmim, A. Longitudinal Clustering Analysis and Prediction of Parkinson’s Disease Progression Using Radiomics and Hybrid Machine Learning. Quant. Imaging Med. Surg. 2022, 12, 906. [Google Scholar] [CrossRef] [PubMed]
- Salmanpour, M.R.; Saberi, A.; Hajianfar, G.; Rahmim, A. Hybrid Machine Learning Methods and Ensemble Voting for Identification of Parkinson’s Disease Subtypes. J. Nucl. Med. 2021, 62 (Suppl. S1), 107. Available online: https://jnm.snmjournals.org/content/62/supplement_1/107 (accessed on 6 April 2023).
- Salmanpour, M.; Shamsaei, M.; Saberi, A.; Hajianfar, G.; Ashrafinia, S.; Davoodi-Bojd, E.; Rahmim, A. Hybrid Machine Learning Methods for Robust Identification of Parkinson’s Disease Subtypes. J. Nucl. Med. 2020, 61 (Suppl. S1), 1429. Available online: https://jnm.snmjournals.org/content/61/supplement_1/1429 (accessed on 6 April 2023).
- Salmanpour, M.R.; Shamsaei, M.; Rahmim, A. Feature Selection and Machine Learning Methods for Optimal Identification and Prediction of Subtypes in Parkinson’s Disease. Comput. Methods Programs Biomed. 2021, 206, 106131. [Google Scholar] [CrossRef]
- Salmanpour, M.; Saberi, A.; Shamsaei, M.; Rahmim, A. Optimal Feature Selection and Machine Learning for Prediction of Outcome in Parkinson’s Disease. J. Nucl. Med. 2020, 61 (Suppl. S1), 524. [Google Scholar]
- Leung, K.H.; Salmanpour, M.R.; Saberi, A.; Klyuzhin, I.S.; Sossi, V.; Jha, A.K.; Rahmim, A. Using Deep-Learning to Predict Outcome of Patients with Parkinson’s Disease. In Proceedings of the 2018 IEEE Nuclear Science Symposium and Medical Imaging Conference Proceedings (NSS/MIC), Sydney, Australia, 10–17 November 2018; Available online: https://ieeexplore.ieee.org/document/8824432 (accessed on 6 April 2023).
- Koza, J.R.; Bennett, F.H.; Andre, D.; Keane, M.A. Automated Design of Both the Topology and Sizing of Analog Electrical Circuits Using Genetic Programming. In Artificial Intelligence in Design ’96; Gero, J.S., Sudweeks, F., Eds.; Springer: Dordrecht, The Netherlands, 1996; pp. 151–170. ISBN 978-94-010-6610-5. [Google Scholar]
- Ashrafinia, S. Quantitative Nuclear Medicine Imaging Using Advanced Image Reconstruction and Radiomics. Ph.D. Thesis, The Johns Hopkins University, Baltim, Egypt, 2019. [Google Scholar]
- Zwanenburg, A.; Leger, S.; Vallières, M.; Löck, S. Image Biomarker Standardisation Initiative. arXiv 2019, arXiv:1612.07003. [Google Scholar]
- McNitt-Gray, M.; Napel, S.; Jaggi, A.; Mattonen, S.A.; Hadjiiski, L.; Muzi, M.; Goldgof, D.; Balagurunathan, Y.; Pierce, L.A.; Kinahan, P.E.; et al. Standardization in Quantitative Imaging: A Multicenter Comparison of Radiomic Features from Different Software Packages on Digital Reference Objects and Patient Data Sets. Tomography 2020, 6, 118–128. [Google Scholar] [CrossRef]
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of Deep Learning: Concepts, CNN Architectures, Challenges, Applications, Future Directions. J. Big Data 2021, 8, 53. [Google Scholar] [CrossRef]
- Bashir, K.; Li, T.; Yahaya, M. A Novel Feature Selection Method Based on Maximum Likelihood Logistic Regression for Imbalanced Learning in Software Defect Prediction. Int. Arab J. Inf. Technol. 2020, 17, 721–730. Available online: https://www.researchgate.net/publication/344028578_A_Novel_Feature_Selection_Method_Based_on_Maximum_Likelihood_Logistic_Regression_for_Imbalanced_Learning_in_Software_Defect_Prediction (accessed on 26 April 2023). [CrossRef]
- Comparison of Feature Selection Methods for Sentiment Analysis. Available online: https://link.springer.com/chapter/10.1007/978-3-642-13059-5_30 (accessed on 26 April 2023).
- Fraiman, D.; Fraiman, R. An ANOVA Approach for Statistical Comparisons of Brain Networks. Sci. Rep. 2018, 8, 4746. Available online: https://www.nature.com/articles/s41598-018-23152-5 (accessed on 14 November 2022). [CrossRef]
- Roy, S.; Meena, T.; Lim, S.-J. Demystifying Supervised Learning in Healthcare 4.0: A New Reality of Transforming Diagnostic Medicine. Diagnostics 2022, 12, 2549. [Google Scholar] [CrossRef] [PubMed]
- Freund, Y.; Schapire, R.E. A Decision-Theoretic Generalization of On-Line Learning and an Application to Boosting. J. Comput. Syst. Sci. 1997, 55, 119–139. Available online: https://www.sciencedirect.com/science/article/pii/S002200009791504X (accessed on 13 October 2022). [CrossRef]
- Breiman, L. Bagging Predictors. Mach. Learn. 1996, 24, 123–140. [Google Scholar] [CrossRef]
- Friedman, J.H. Greedy Function Approximation: A Gradient Boosting Machine. Ann. Stat. 2001, 29, 1189–1232. Available online: https://projecteuclid.org/journals/annals-of-statistics/volume-29/issue-5/Greedy-function-approximation-A-gradient-boostingmachine/10.1214/aos/1013203451.full (accessed on 13 October 2022). [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. Sci. Res. Publ. 2001, 45, 5–32. Available online: https://www.scirp.org/(S(czeh2tfqw2orz553k1w0r45))/reference/referencespapers.aspx?referenceid=1734556 (accessed on 13 October 2022). [CrossRef]
- Chen, T.; Guestrin, C. XGBoost: A Scalable Tree Boosting System. arXiv 2016, arXiv:1603.02754. Available online: https://arxiv.org/abs/1603.02754 (accessed on 13 October 2022).
- Hinton, G.E. Connectionist Learning Procedures. In Machine Learning; Elsevier: Amsterdam, The Netherlands, 1990; pp. 555–610. [Google Scholar]
- Fix, E.; Hodges, J.L. Discriminatory Analysis. Nonparametric Discrimination: Consistency Properties. Int. Stat. Rev. Int. Stat. 1989, 57, 238–247. [Google Scholar] [CrossRef]
- Geurts, P.; Ernst, D.; Wehenkel, L. Extremely Randomized Trees. Mach. Lang. 2006, 63, 3–42. [Google Scholar] [CrossRef]
- Feng, X.; Jiang, Y.; Yang, X.; Du, M.; Li, X. Computer Vision Algorithms and Hardware Implementations: A Survey. Integration 2019, 69, 309–320. [Google Scholar] [CrossRef]
- Brahim, A.; Górriz, J.M.; Ramírez, J.; Khedher, L. Intensity Normalization of DaTSCAN SPECT Imaging Using a Model-Based Clustering Approach. Appl. Soft Comput. 2015, 37, 234–244. [Google Scholar] [CrossRef]
- Biundo, R.; Weis, L.; Pilleri, M.; Facchini, S.; Formento-Dojot, P.; Vallelunga, A.; Antonini, A. Diagnostic and Screening Power of Neuropsychological Testing in Detecting Mild Cognitive Impairment in Parkinson’s Disease. J. Neural Transm. 2013, 120, 627–633. [Google Scholar] [CrossRef]
- Bradshaw, T.J.; McCradden, M.D.; Jha, A.K.; Dutta, J.; Saboury, B.; Siegel, E.L.; Rahmim, A. Artificial Intelligence Algorithms Need to Be Explainable—Or Do They? J. Nucl. Med. 2023, in press. Available online: https://jnm.snmjournals.org/content/early/2023/04/27/jnumed.122.264949 (accessed on 5 April 2023).
- Gunning, D.; Stefik, M.; Choi, J.; Miller, T.; Stumpf, S.; Yang, G.-Z. XAI—Explainable Artificial Intelligence. Sci. Robot. 2019, 4, eaay7120. [Google Scholar] [CrossRef]
- Samek, W.; Müller, K.R. Towards Explainable Artificial Intelligence. In Explainable AI: Interpreting, Explaining and Visualizing Deep Learning; Springer: Cham, Switzerland, 2019; pp. 5–22. Available online: https://link.springer.com/chapter/10.1007/978-3-030-28954-6_1 (accessed on 5 April 2023).
- Rudin, C. Stop Explaining Black Box Machine Learning Models for High Stakes Decisions and Use Interpretable Models Instead. Nat. Mach. Intell. 2019, 1, 206–215. [Google Scholar] [CrossRef]
- Murdoch, W.J.; Singh, C.; Kumbier, K.; Abbasi-Asl, R.; Yu, B. Definitions, Methods, and Applications in Interpretable Machine Learning. Proc. Natl. Acad. Sci. USA 2019, 116, 22071–22080. [Google Scholar] [CrossRef] [PubMed]
- Izumo, T.; Weng, Y.-H. Coarse Ethics: How to Ethically Assess Explainable Artificial Intelligence. AI Ethics 2021, 2, 449–461. [Google Scholar] [CrossRef]
- Erro, R.; Schneider, S.A.; Stamelou, M.; Quinn, N.P.; Bhatia, K.P. What Do Patients with Scans without Evidence of Dopaminergic Deficit (SWEDD) Have? New Evidence and Continuing Controversies. J. Neurol. Neurosurg. Psychiatry 2016, 87, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Utiumi, M.A.; Felício, A.C.; Borges, C.R.; Braatz, V.L.; Rezende, S.A.; Munhoz, R.P.; Bressan, R.A.; Ferraz, H.B.; Teive, H.A. Dopamine Transporter Imaging in Clinically Unclear Cases of Parkinsonism and the Importance of Scans without Evidence of Dopaminergic Deficit (SWEDDs). Arq. Neuropsiquiatr. 2012, 70, 667–673. [Google Scholar] [CrossRef]
- Rahmim, A.; Huang, P.; Shenkov, N.; Fotouhi, S.; Davoodi-Bojd, E.; Lu, L.; Mari, Z.; Soltanian-Zadeh, H.; Sossi, V. Improved Prediction of Outcome in Parkinson’s Disease Using Radiomics Analysis of Longitudinal DAT SPECT Images. NeuroImage Clin. 2017, 16, 539–544. [Google Scholar] [CrossRef]
- Odusami, M.; Maskeliūnas, R.; Damaševičius, R. An Intelligent System for Early Recognition of Alzheimer’s Disease Using Neuroimaging. Sensors 2022, 22, 740. [Google Scholar] [CrossRef]
- Ke, Q.; Zhang, J.; Wei, W.; Damaševičius, R.; Woźniak, M. Adaptive Independent Subspace Analysis of Brain Magnetic Resonance Imaging Data. IEEE J. Mag. 2019, 7, 12252–12261. Available online: https://ieeexplore.ieee.org/abstract/document/8620993 (accessed on 24 April 2023). [CrossRef]
- Yousaf, T.; Pagano, G.; Niccolini, F.; Politis, M. Predicting Cognitive Decline with Non-Clinical Markers in Parkinson’s Disease (PRECODE-2). J. Neurol. 2019, 266, 1203–1210. [Google Scholar] [CrossRef] [PubMed]
- Leung, K.H.; Rowe, S.P.; Pomper, M.G.; Du, Y. A Three-Stage, Deep Learning, Ensemble Approach for Prognosis in Patients with Parkinson’s Disease. EJNMMI Res. 2021, 11, 52. [Google Scholar] [CrossRef] [PubMed]
- Odusami, M.; Maskeliūnas, R.; Damaševičius, R. Pixel-Level Fusion Approach with Vision Transformer for Early Detection of Alzheimer’s Disease. Electronics 2023, 12, 1218. [Google Scholar] [CrossRef]
- Sarangi, S.; Sahidullah, M.; Saha, G. Optimization of Data-Driven Filterbank for Automatic Speaker Verification. Digit. Signal Process. 2020, 104, 102795. Available online: https://www.sciencedirect.com/science/article/abs/pii/S1051200420301408 (accessed on 14 November 2022). [CrossRef]
- Gladkikh, V.; Kim, D.Y.; Hajibabaei, A.; Jana, A.; Myung, C.W.; Kim, K.S. Machine Learning for Predicting the Band Gaps of ABX3 Perovskites from Elemental Properties. J. Phys. Chem. C 2020, 124, 8905–8918. Available online: https://pubs.acs.org/doi/abs/10.1021/acs.jpcc.9b11768 (accessed on 14 November 2022). [CrossRef]
- Skurichina, M.; Duin, R.P. Bagging, Boosting and the Random Subspace Method for Linear Classifiers. Pattern Anal. Appl. 2002, 5, 121–135. Available online: https://link.springer.com/article/10.1007/s100440200011 (accessed on 14 November 2022). [CrossRef]
- Abd Manaf, S.; Mustapha, N.; Sulaiman, M.N.; Husin, N.A.; Shafri, H.Z.M.; Razali, M.N. Hybridization of SLIC and Extra Tree for Object Based Image Analysis in Extracting Shoreline from Medium Resolution Satellite Images. Int. J. Intell. Eng. Syst. 2018, 11, 62–72. Available online: https://www.researchgate.net/publication/322050216_Hybridization_of_SLIC_and_Extra_Tree_for_Object_Based_Image_Analysis_in_Extracting_Shoreline_from_Medium_Resolution_Satellite_Images (accessed on 14 November 2022).
- What is XGBoost? NVIDIA Data Science Glossary. Available online: https://www.nvidia.com/en-us/glossary/data-science/xgboost/ (accessed on 14 November 2022).
- Ray, S. A Quick Review of Machine Learning Algorithms. In Proceedings of the 2019 International Conference on Machine Learning, Big Data, Cloud and Parallel Computing (COMITCon), Faridabad, India, 14–16 February 2019; Available online: https://www.semanticscholar.org/paper/A-Quick-Review-of-Machine-Learning-Algorithms-Ray/8db8166249dfb94dd8d52f88d27917b5755ae049 (accessed on 14 November 2022).
- Gardner, M.W.; Dorling, S.R. Artificial neural networks (the multilayer perceptron)—A review of applications in the atmospheric sciences. Atmos. Environ. 1998, 32, 2627–2636. [Google Scholar] [CrossRef]
- Uddin, S.; Khan, A.; Hossain, M.E.; Moni, M.A. Comparing different supervised machine learning algorithms for disease prediction. BMC Med. Inform. Decis. Mak. 2019, 19, 281. Available online: https://bmcmedinformdecismak.biomedcentral.com/articles/10.1186/s12911-019-1004-8 (accessed on 14 November 2022). [CrossRef]







Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hosseinzadeh, M.; Gorji, A.; Fathi Jouzdani, A.; Rezaeijo, S.M.; Rahmim, A.; Salmanpour, M.R. Prediction of Cognitive Decline in Parkinson’s Disease Using Clinical and DAT SPECT Imaging Features, and Hybrid Machine Learning Systems. Diagnostics 2023, 13, 1691. https://doi.org/10.3390/diagnostics13101691
Hosseinzadeh M, Gorji A, Fathi Jouzdani A, Rezaeijo SM, Rahmim A, Salmanpour MR. Prediction of Cognitive Decline in Parkinson’s Disease Using Clinical and DAT SPECT Imaging Features, and Hybrid Machine Learning Systems. Diagnostics. 2023; 13(10):1691. https://doi.org/10.3390/diagnostics13101691
Chicago/Turabian StyleHosseinzadeh, Mahdi, Arman Gorji, Ali Fathi Jouzdani, Seyed Masoud Rezaeijo, Arman Rahmim, and Mohammad R. Salmanpour. 2023. "Prediction of Cognitive Decline in Parkinson’s Disease Using Clinical and DAT SPECT Imaging Features, and Hybrid Machine Learning Systems" Diagnostics 13, no. 10: 1691. https://doi.org/10.3390/diagnostics13101691
APA StyleHosseinzadeh, M., Gorji, A., Fathi Jouzdani, A., Rezaeijo, S. M., Rahmim, A., & Salmanpour, M. R. (2023). Prediction of Cognitive Decline in Parkinson’s Disease Using Clinical and DAT SPECT Imaging Features, and Hybrid Machine Learning Systems. Diagnostics, 13(10), 1691. https://doi.org/10.3390/diagnostics13101691