
Plasmodium malariae Detected by Microscopy in the International Bordering Area of Mizoram, a Northeastern State of India

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
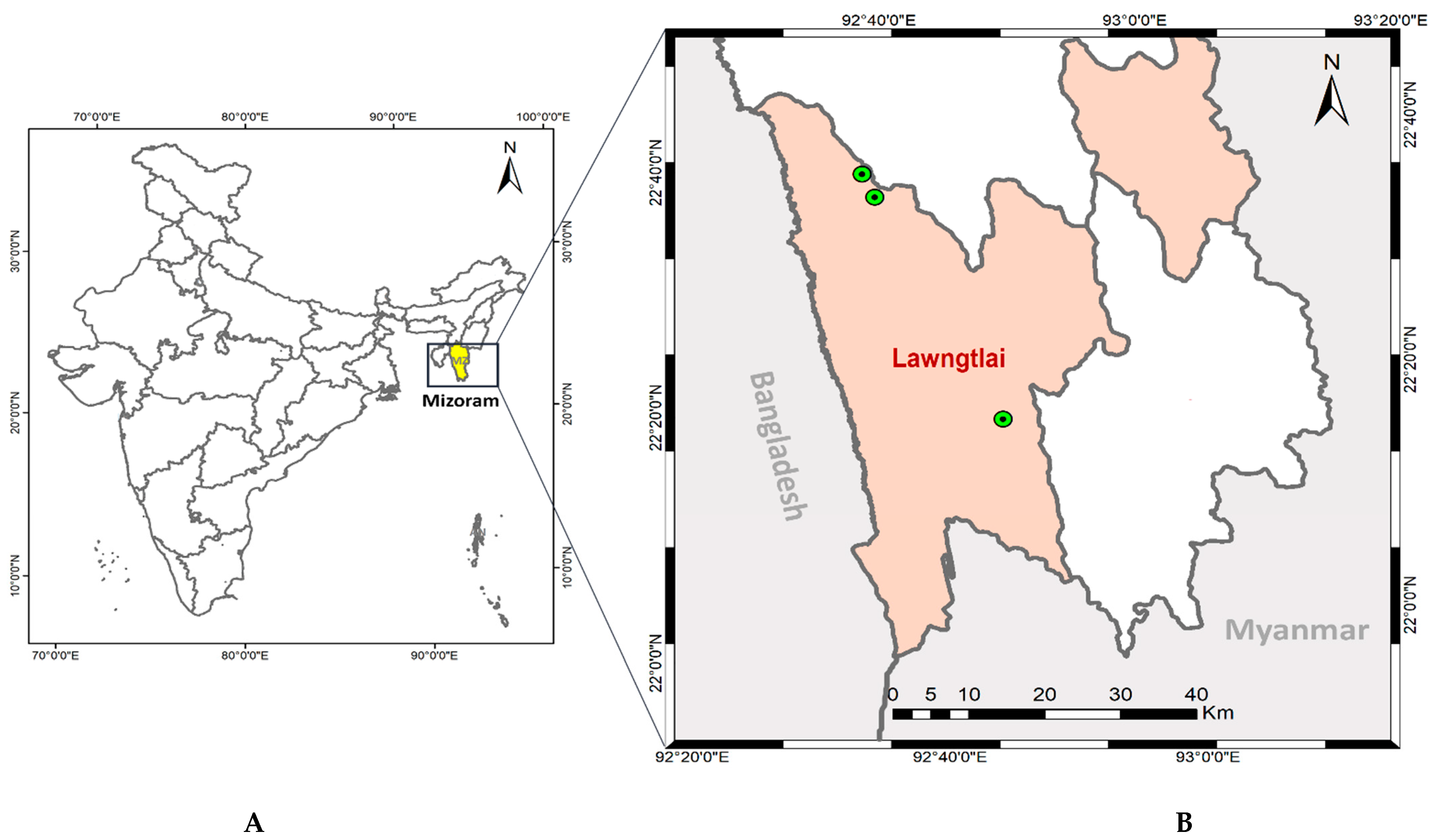
2.1. Description of the Study Area
2.2. Study Population and Malaria Diagnosis
2.3. Estimation of Parasitemia
2.4. Quality Control
2.5. Data Analysis
3. Results
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- World Health Organization. World Malaria Report 2021; World Health Organization: Geneva, Switzerland, 2021; Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2021 (accessed on 3 March 2022).
- Dhiman, S.; Veer, V.; Dev, V. Declining Transmission of Malaria in India: Accelerating towards Elimination. In Towards Malaria Elimination—A Leap Forward; Manguin, S., Dev, V., Eds.; IntechOpen: London, UK, 2018; Available online: https://www.intechopen.com/chapters/61663 (accessed on 29 April 2022).
- World Malaria Day Observed within Lawngtlai District. Available online: https://lawngtlai.nic.in/world-malaria-day-observed-within-lawngtlai-district/ (accessed on 29 April 2022).
- Bharti, P.K.; Chand, S.K.; Singh, M.P.; Mishra, S.; Shukla, M.M.; Singh, R.; Singh, N. Emergence of a new focus of Plasmodium malariae in forest villages of district Balaghat, Central India: Implications for the diagnosis of malaria and its control. Trop. Med. Int. Health 2013, 18, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, R.; Deora, N.; Bhandari, D.; Parvez, S.; Sinha, A.; Sharma, A. Trends of neglected Plasmodium species infection in humans over the past century in India. One Health 2020, 11, 100190. [Google Scholar] [CrossRef]
- Nema, S.; Singh, A.; Krishna, S.; Poriya, R.; Dubey, S.; Ali, N.A.; Singh, M.P.; Verma, A.K.; Das, A.; Bharti, P.K. Unreported mixed Plasmodium species infection may increase vivax malaria in India: A challenge for malaria elimination. Trans. R. Soc. Trop. Med. Hyg. 2022; ahead to print. [Google Scholar] [CrossRef] [PubMed]
- Gupta, B.; Gupta, P.; Sharma, A.; Singh, V.; Dash, A.P.; Das, A. High proportion of mixed-species Plasmodium infections in India revealed by PCR diagnostic assay. Trop. Med. Int. Health 2010, 15, 819–824. [Google Scholar] [CrossRef] [PubMed]
- Lover, A.A.; Baird, J.K.; Gosling, R.; Price, R.N. Malaria elimination: Time to target all species. Am. J. Trop. Med. Hyg. 2018, 99, 17–23. [Google Scholar] [CrossRef]
- Collins, W.E.; Jeffery, G.M. Plasmodium malariae: Parasite and disease. Clin. Microbiol. Rev. 2007, 20, 579–592. [Google Scholar] [CrossRef] [Green Version]
- Ashraf, S.; Kao, A.; Hugo, C.; Christophel, E.M.; Fatunmbi, B.; Luchavez, J.; Lilley, K.; Bell, D. Developing standards for malaria microscopy: External competency assessment for malaria microscopists in the Asia-Pacific. Malar. J. 2012, 11, 352. [Google Scholar] [CrossRef] [Green Version]
- Bharti, P.K.; Silawat, N.; Singh, P.P.; Singh, M.P.; Shukla, M.; Chand, G.; Dash, A.P.; Singh, N. The usefulness of a new rapid diagnostic test, the First Response® Malaria Combo (pLDH/HRP2) card test, for malaria diagnosis in the forested belt of central India. Malar. J. 2008, 7, 126. [Google Scholar] [CrossRef] [Green Version]
- Singh, N.; Shukla, M.M.; Shukla, M.K.; Mehra, R.K.; Sharma, S.; Bharti, P.K.; Singh, M.P.; Singh, A.; Gunasekar, A. Field and laboratory comparative evaluation of rapid malaria diagnostic tests versus traditional and molecular techniques in India. Malar. J. 2010, 9, 191. [Google Scholar] [CrossRef] [Green Version]
- Bharti, P.K.; Chandel, H.S.; Ahmad, A.; Krishna, S.; Udhayakumar, V.; Singh, N. Prevalence of pfhrp2 and/or pfhrp3 gene deletion in Plasmodium falciparum population in eight highly endemic states in India. PLoS ONE 2016, 11, e0157949. [Google Scholar] [CrossRef]
- Ishengoma, D.S.; Lwitiho, S.; Madebe, R.A.; Nyagonde, N.; Persson, O.; Vestergaard, L.S.; Bygbjerg, I.C.; Lemnge, M.M.; Alifrangis, M. Using rapid diagnostic tests as source of malaria parasite DNA for molecular analyses in the era of declining malaria prevalence. Malar. J. 2011, 10, 6. [Google Scholar] [CrossRef] [Green Version]
- Komaki-Yasuda, K.; Vincent, J.P.; Nakatsu, M.; Kato, Y.; Ohmagari, N.; Kano, S. A novel PCR-based system for the detection of four species of human malaria parasites and Plasmodium knowlesi. PLoS ONE 2018, 13, e0191886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahar, R.; Ringwald, P.; Basco, L.K. Diagnosis of Plasmodium malariae infection by the polymerase chain reaction. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 410–411. [Google Scholar] [CrossRef]
- Fitri, L.E.; Widaningrum, T.; Endharti, A.T.; Prabowo, M.H.; Winaris, N.; Nugraha, R.Y.B. Malaria diagnostic update: From conventional to advanced method. J. Clin. Lab. Anal. 2022, 36, e24314. [Google Scholar] [CrossRef] [PubMed]
- Dev, V.; Manguin, S. Defeating malaria in the North-East region: The forerunner for malaria elimination in India. Acta Trop. 2021, 222, 106040. [Google Scholar] [CrossRef] [PubMed]
- Subbarao, S.K.; Nanda, N.; Rahi, M.; Raghavendra, K. Biology and bionomics of malaria vectors in India: Existing information and what more needs to be known for strategizing elimination of malaria. Malar. J. 2019, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lalchhuanawma, R.; Murhekar, M.V. Health-seeking behaviour for febrile illness in malaria-endemic Kolasib district, Mizoram, India. Int. Health 2012, 4, 314–319. [Google Scholar] [CrossRef]
- National Drug Policy on Malaria. 2013. Available online: https://nvbdcp.gov.in/Doc/National-Drug-Policy-2013.pdf (accessed on 25 April 2022).
- Prajapati, S.K.; Singh, O.P. Insights into the invasion biology of Plasmodium vivax. Front. Cell. Infect. Microbiol. 2013, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Kerlin, D.H.; Gatton, M.L. Preferential invasion by Plasmodium merozoites and the self-regulation of parasite burden. PLoS ONE 2013, 8, e57434. [Google Scholar] [CrossRef] [Green Version]
- Roucher, C.; Rogier, C.; Sokhna, C.; Tall, A.; Trape, J.-F. A 20-year longitudinal study of Plasmodium ovale and Plasmodium malariae prevalence and morbidity in a West African population. PLoS ONE 2014, 9, e87169. [Google Scholar] [CrossRef] [Green Version]
- Yman, V.; Wandell, G.; Mutemi, D.D.; Miglar, A.; Asghar, M.; Hammar, U.; Karlsson, M.; Lind, I.; Nordfjell, C.; Rooth, I. Persistent transmission of Plasmodium malariae and Plasmodium ovale species in an area of declining Plasmodium falciparum transmission in eastern Tanzania. PLoS Negl. Trop. Dis. 2019, 13, e0007414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, N.; Chang, Q.; Sun, X.; Lu, H.; Yin, J.; Zhang, Z.; Wahlgren, M.; Chen, Q. Co-infections with Plasmodium knowlesi and other malaria parasites, Myanmar. Emerg. Infect. Dis. 2010, 16, 1476–1478. [Google Scholar] [CrossRef]
- Han, T.Z.; Han, K.T.; Aye, K.H.; Hlaing, T.; Thant, K.Z.; Vythilingam, I. Comparison of microscopy and PCR for the detection of human Plasmodium species and Plasmodium knowlesi in southern Myanmar. Asian Pac. J. Trop. Biomed. 2017, 7, 680–685. [Google Scholar] [CrossRef]
- Fuehrer, H.-P.; Starzengruber, P.; Swoboda, P.; Khan, W.A.; Matt, J.; Ley, B.; Thriemer, K.; Haque, R.; Yunus, E.B.; Hossain, S.M. Indigenous Plasmodium ovale malaria in Bangladesh. Am. J. Trop. Med. Hyg. 2010, 83, 75–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuehrer, H.-P.; Swoboda, P.; Harl, J.; Starzengruber, P.; Habler, V.E.; Bloeschl, I.; Haque, R.; Matt, J.; Khan, W.A.; Noedl, H. High prevalence and genetic diversity of Plasmodium malariae and no evidence of Plasmodium knowlesi in Bangladesh. Parasitol. Res. 2014, 113, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- Jambulingam, P.; Mohapatra, S.; Das, L.; Das, P.; Rajagopalan, P. Detection of Plasmodium ovale in Koraput district, Orissa state. Indian J. Med. Res. 1989, 89, 115–116. [Google Scholar] [PubMed]
- Prakash, A.; Mohapatra, P.; Bhattacharyya, D.; Goswami, B.; Mahanta, J. Plasmodium ovale: First case report from Assam, India. Curr. Sci. 2003, 84, 1187–1188. [Google Scholar]
- Singh, R.; Jain, V.; Singh, P.; Bharti, P.; Thomas, T.; Basak, S.; Singh, N. First report of detection and molecular confirmation of Plasmodium ovale from severe malaria cases in central India. Trop. Med. Int. Health 2013, 18, 1416–1420. [Google Scholar] [CrossRef]
- Krishna, S.; Bharti, P.K.; Chandel, H.S.; Ahmad, A.; Kumar, R.; Singh, P.P.; Singh, M.P.; Singh, N. Detection of mixed infections with Plasmodium spp. by PCR, India, 2014. Emerg. Infect. Dis. 2015, 21, 1853–1857. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, N.; Bhandari, S.; Bharti, P.K.; Basak, S.K.; Singh, M.P.; Singh, N. Sympatric distribution of Plasmodium ovale curtisi and P. ovale wallikeri in India: Implication for the diagnosis of malaria and its control. Trans. R. Soc. Trop. Med. Hyg. 2015, 109, 352–354. [Google Scholar] [CrossRef]
- Mohapatra, P.K.; Prakash, A.; Bhattacharyya, D.R.; Goswami, B.; Ahmed, A.; Sarmah, B.; Mahanta, J. Detection & molecular confirmation of a focus of Plasmodium malariae in Arunachal Pradesh, India. Indian J. Med. Res. 2008, 128, 52–60. [Google Scholar] [PubMed]
- Dhangadamajhi, G.; Kar SK, K.; Ranjit, M.R. High prevalence and gender bias in distribution of Plasmodium malariae infection in central east-coast India. Trop. Biomed. 2009, 26, 326–333. [Google Scholar] [PubMed]
- Fançony, C.; Sebastião, Y.V.; Pires, J.E.; Gamboa, D.; Nery, S.V. Performance of microscopy and RDTs in the context of a malaria prevalence survey in Angola: A comparison using PCR as the gold standard. Malar. J. 2013, 12, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age | Number of Fever Cases: 948 | Rapid Diagnostic Test, n (%) | Malaria Microscopy, n (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender (n) | Malaria-Positive (%) | Pf (%) | Pv (%) | Pm (%) | Mix (%) | Malaria-Positive (%) | Pf (%) | Pv (%) | Pm (%) | Mix (%) | |
| Under-5 years | Male (86) | 8 (9.30) | 7(8.14) | 1 (1.16) | 0 | 0 | 9 (10.47) | 7 (8.14) | 2 (2.33) | 0 | 0 |
| Female (64) | 8 (12.50) | 6(9.38) | 2 (3.13) | 0 | 0 | 9 (14.06) | 7 (10.94) | 2 (3.13) | 0 | 0 | |
| 5–15 years | Male (164) | 22 (13.41) | 21(12.80) | 1 (0.61) | 0 | 0 | 30 (18.29) | 27 (16.46) | 1 (0.61) | 2 (1.22) | 0 |
| Female (111) | 22 (19.81) | 22 (19.82) | 0 | 0 | 0 | 25 (22.52) | 24 (21.62) | 0 | 0 | 1 (0.90) | |
| ≥15 years | Male (262) | 55 (20.99) | 49 (18.70) | 6 (2.29) | 0 | 0 | 65 (24.81) | 55 (20.99) | 7 (2.67) | 1 (0.38) | 2 (0.76) |
| Female (261) | 36 (13.79) | 31 (11.88) | 5 (1.92) | 0 | 0 | 41 (15.71) | 34 (13.03) | 5 (1.92) | 2 (0.77) | 0 (0.00) | |
| Total | Male (512) | 85 (16.60) | 77 (15.34) | 8 (1.56) | 0 | 0 | 104 (20.31) | 89 (17.38) | 10 (1.953) | 3 (0.58) | 2 (0.39) |
| Female (436) | 66 (15.14) | 59 (13.53) | 7 (1.60) | 0 | 0 | 75 (17.20) | 65 (14.91) | 7 (1.61) | 2 (0.46) | 1 (0.23) | |
| Age Group | BSE | Risk of Malaria Infection | Risk of P. Falciparum * Infection | Risk of Non-P. falciparum ** Infection | |||
|---|---|---|---|---|---|---|---|
| +ve | Odds Ratio (95% CI), p-Value | Pf | Odds Ratio (95% CI), p-Value | Non-Pf | Odds Ratio (95% CI), p-Value | ||
| Under-5 years | 150 | 18 | – | 14 | – | 4 | – |
| 5–15 years | 275 | 55 | 1.67 (0.94–2.94), p = 0.078 | 51 | 1.99 (1.06–3.71), p = 0.03 | 4 | 0.55 (0.13 to 2.21), p = 0.39 |
| ≥15 years | 523 | 106 | 1.69 (0.99–2.87), p = 0.053 | 89 | 1.82 (1.01–3.29), p = 0.046 | 17 | 1.22 (0.40 to 3.67), p = 0.73 |
| Country | Plasmodium Species | Study Site | Positivity | Remarks | Reference |
|---|---|---|---|---|---|
| Myanmar | P. knowlesi | Southern Myanmar near Yunnan Province of China | Pk: 4 Pk + Pf: 13 Pk + Pv: 13 Pk + Pf + Pv: 2 | M. nemestrina as reservoir host | [26] |
| P. malariae | Ranong province border | Pm: 1 | Both microscopy and PCR were capable to identify | [27] | |
| Bangladesh | P. malariae | Chittagong Hill Tracts in southeastern Bangladesh | Pm: 60 | P. malariae is highly underestimated in rural Bangladesh | [29] |
| P. malariae and P. ovale | Chittagong Hill Tracts | Pm: 3 Po: 3 | Both microscopy and PCR were capable to identify | [28] | |
| India | P. ovale | Koraput District, Orissa state. | Po: 3 | – | [30] |
| P. ovale | Titabor PHC, Jorhat (Assam) | Po: 1 | – | [31] | |
| P. falciparum + P. ovale | Orissa, Jharkhand, Chhattisgarh, Madhya Pradesh | Pf + Po: 6 | Mixed infection | [33] | |
| P. falciparum + P. malariae + P. ovale | Jharkhand | Pf + Pm + P: 01 | Mixed infection | [33] | |
| P. falciparum + P. malariae | Orissa, Chhattisgarh, Maharashtra, Madhya Pradesh, Tripura, Gujarat, and Rajasthan | Pf + Pm: 19 | Mixed infection | [33] | |
| P. ovale curtisi and P. ovale wallikeri | Bastar, State of Chhattisgarh | Po: 2 Pv + Pf + Po: 1 | Mono- and mixed infection of P. ovale curtisi | [34] | |
| P. ovale | Jagdalpur (Chhattisgarh) | Po: 3 | – | [32] | |
| P. malariae (mono- and mixed infections) | Balaghat District | Pm: 14 Pm + Pv: 2 Pm + Pf: 3 | Existence in forest villages of central India | [4] | |
| P. malariae | Lohit (Arunachal Pradesh) | Pm: 9 | Confirmed by nested PCR | [35] | |
| P. malariae | Orissa | Pm: 108 | High prevalence | [36] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Singh, K.; Bharti, P.K.; Devi, N.C.; Ahmed, N.; Sharma, A. Plasmodium malariae Detected by Microscopy in the International Bordering Area of Mizoram, a Northeastern State of India. Diagnostics 2022, 12, 2015. https://doi.org/10.3390/diagnostics12082015
Singh K, Bharti PK, Devi NC, Ahmed N, Sharma A. Plasmodium malariae Detected by Microscopy in the International Bordering Area of Mizoram, a Northeastern State of India. Diagnostics. 2022; 12(8):2015. https://doi.org/10.3390/diagnostics12082015
Chicago/Turabian StyleSingh, Kuldeep, Praveen Kumar Bharti, Naorem Chaoba Devi, Naseem Ahmed, and Amit Sharma. 2022. "Plasmodium malariae Detected by Microscopy in the International Bordering Area of Mizoram, a Northeastern State of India" Diagnostics 12, no. 8: 2015. https://doi.org/10.3390/diagnostics12082015
APA StyleSingh, K., Bharti, P. K., Devi, N. C., Ahmed, N., & Sharma, A. (2022). Plasmodium malariae Detected by Microscopy in the International Bordering Area of Mizoram, a Northeastern State of India. Diagnostics, 12(8), 2015. https://doi.org/10.3390/diagnostics12082015