
Emulating Clinical Diagnostic Reasoning for Jaw Cysts with Machine Learning

 , ,
, ,  , , , ,
, , , ,  , , , , , , ,
, , , , , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Image Data
2.1.1. Data Collection
2.1.2. Data Preparation
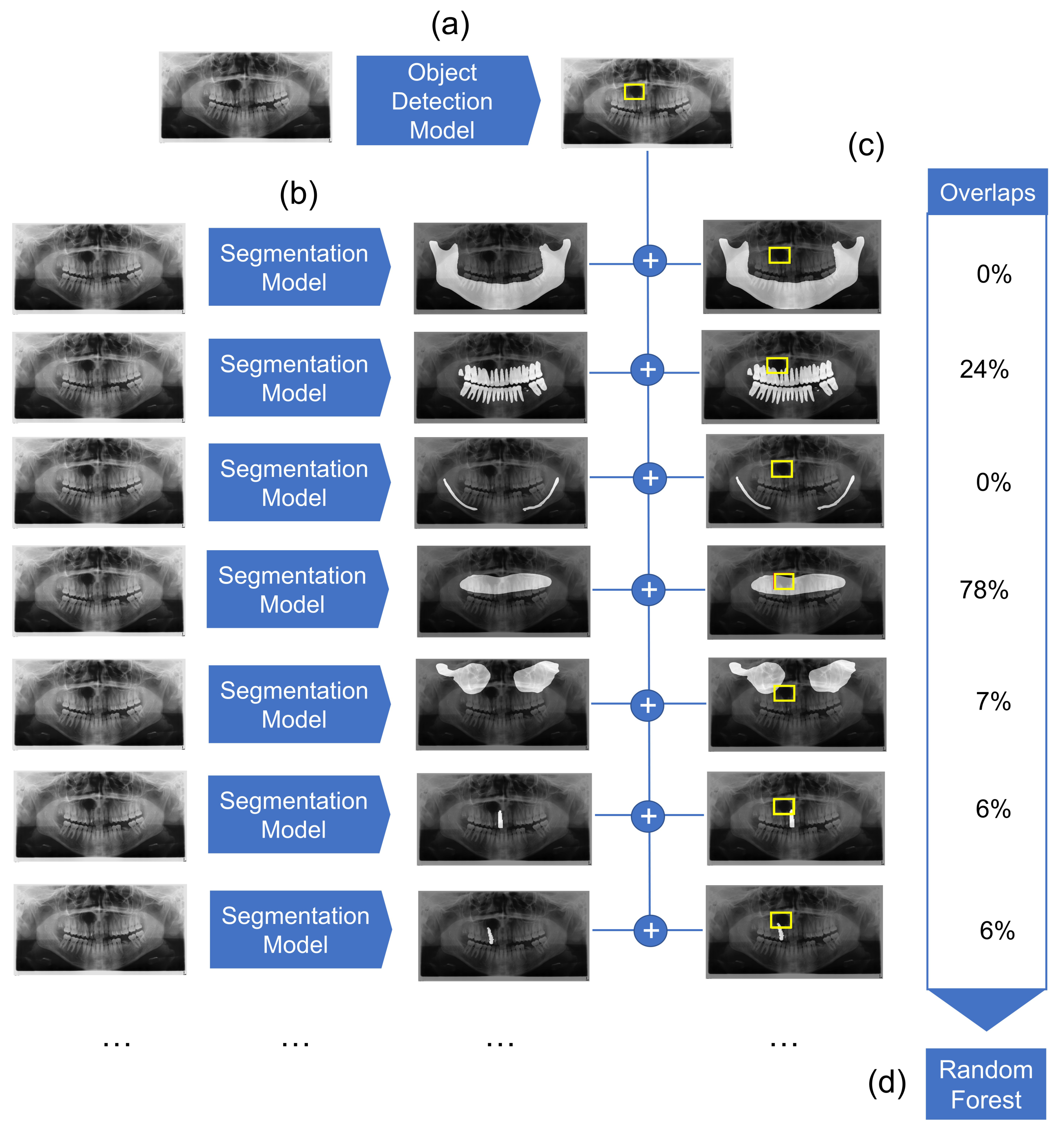
2.2. Modeling
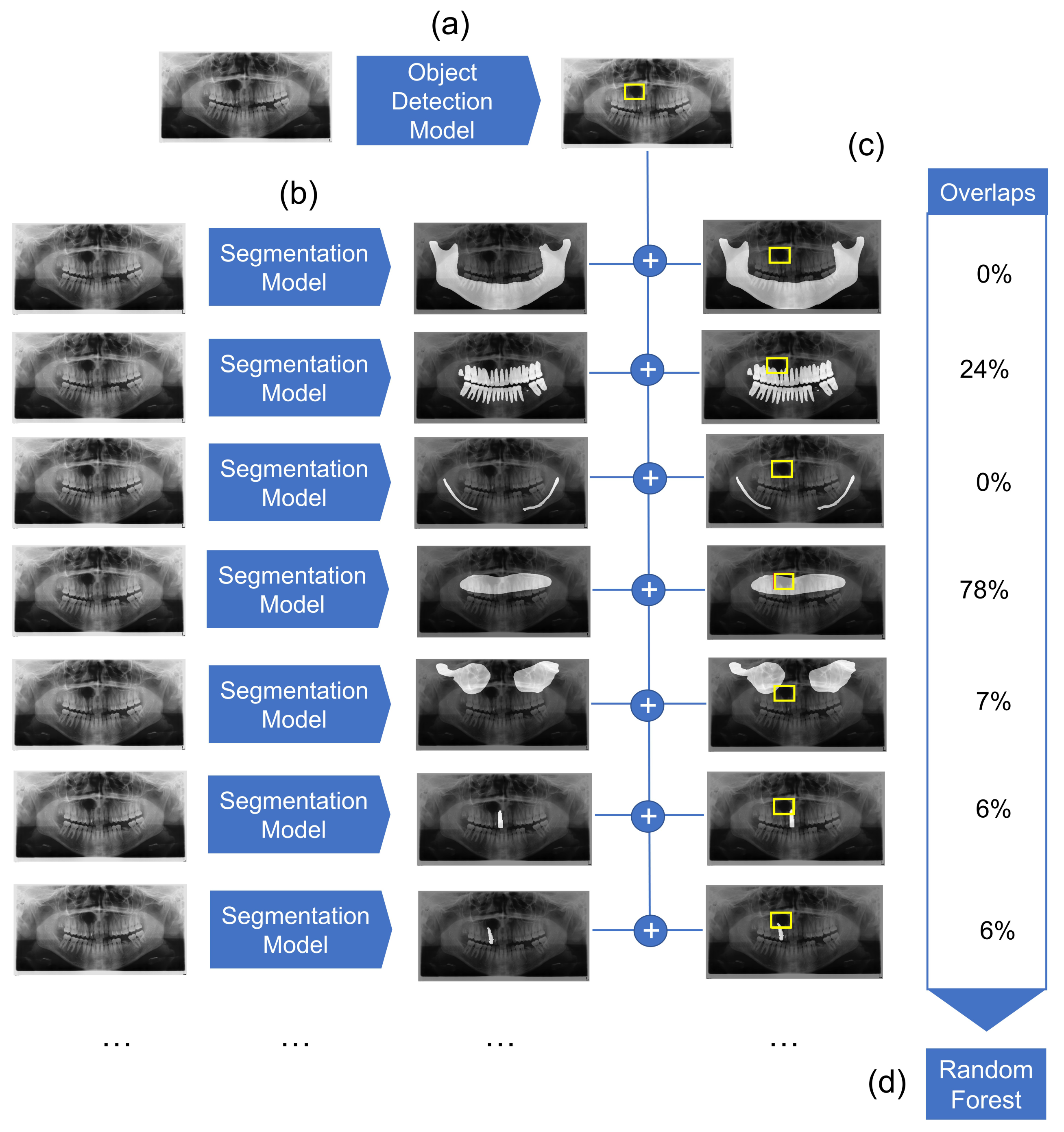
2.2.1. Object Detection Modeling
2.2.2. Segmentation Models
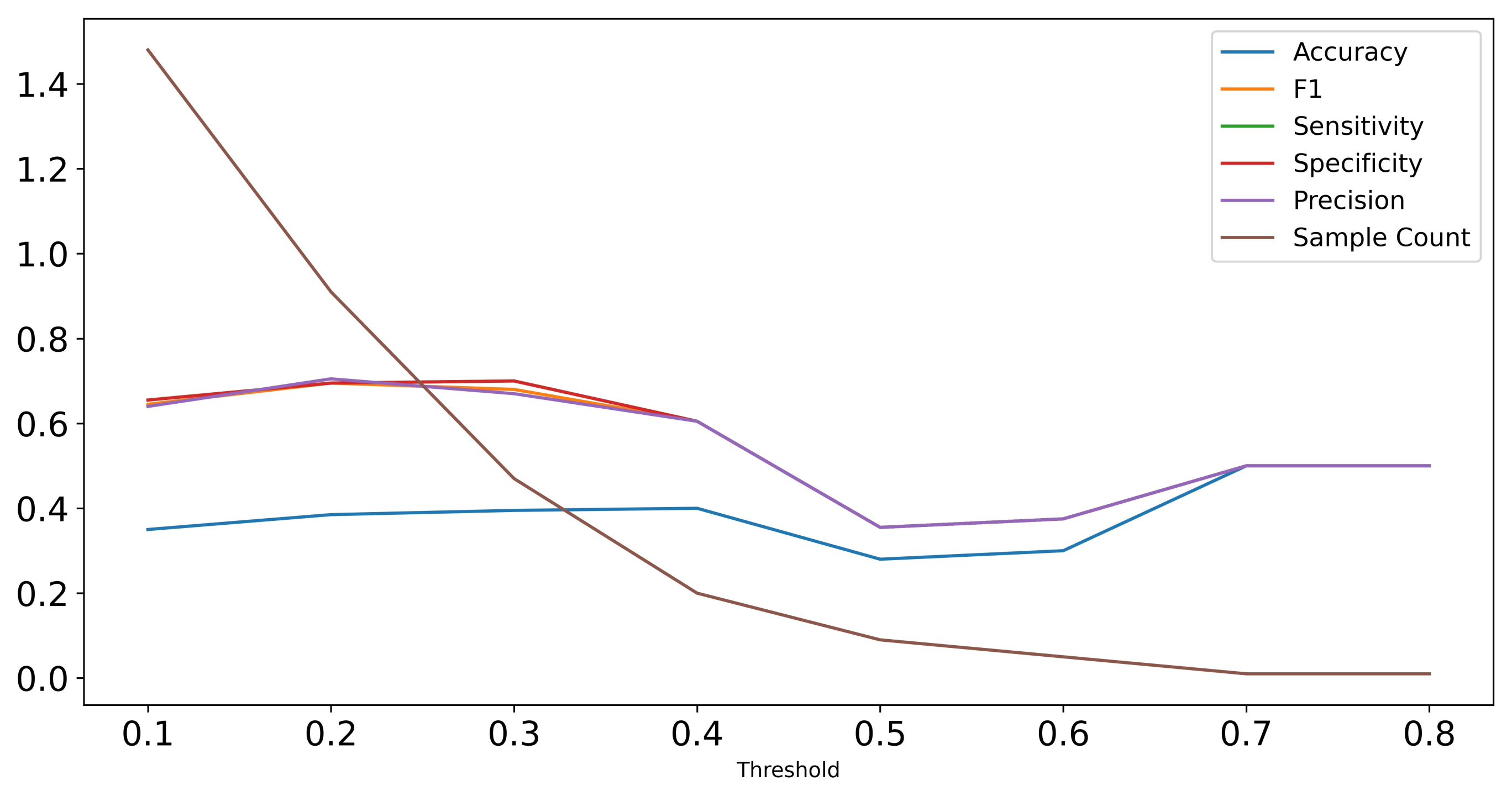
2.2.3. Mask Overlap
2.2.4. Random Forest Classifier
2.3. Human Control Group
3. Results
3.1. Dataset Characteristics
3.2. Detection and Segmentation Performance
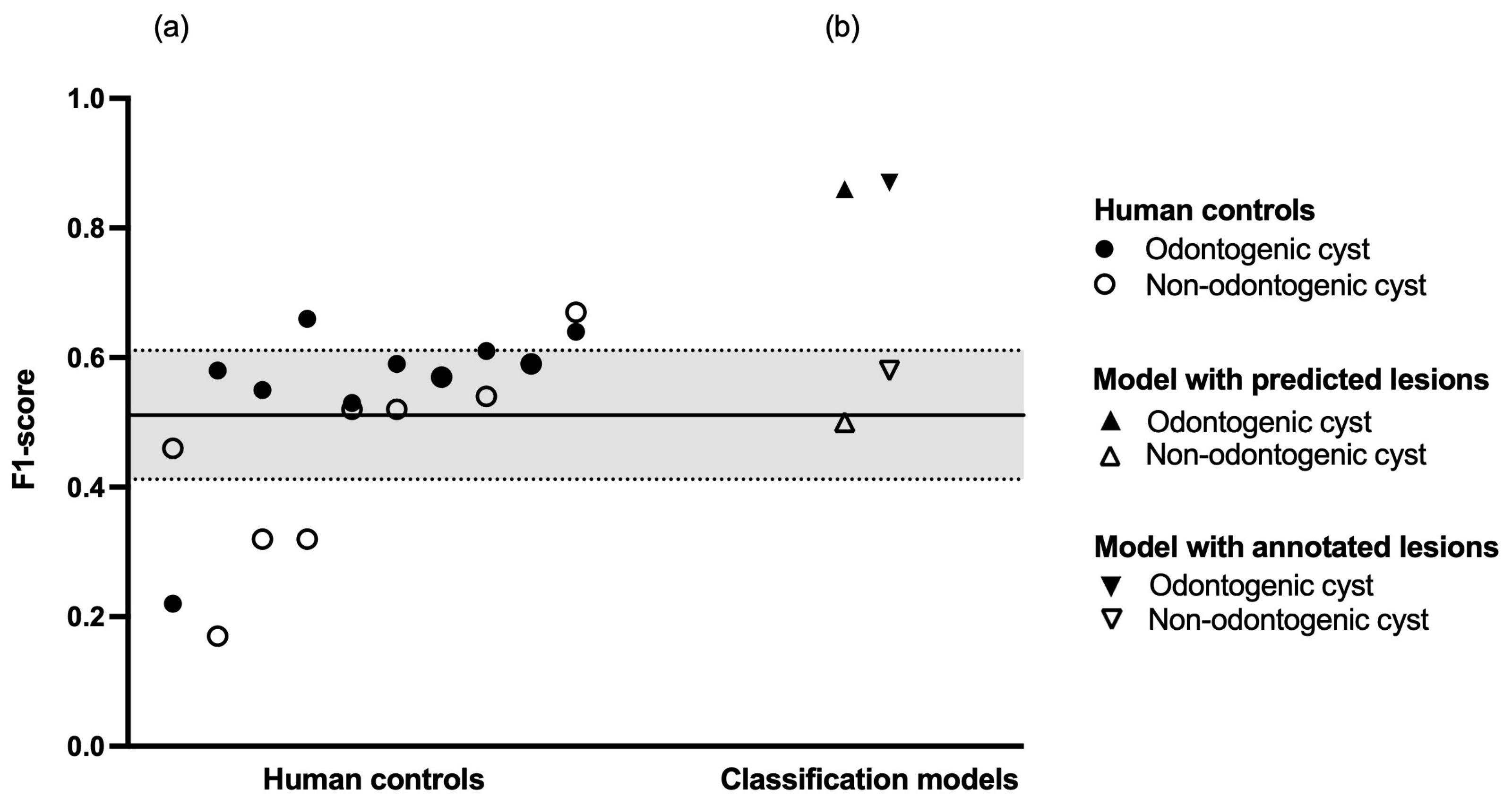
3.3. Random Forest Classifier
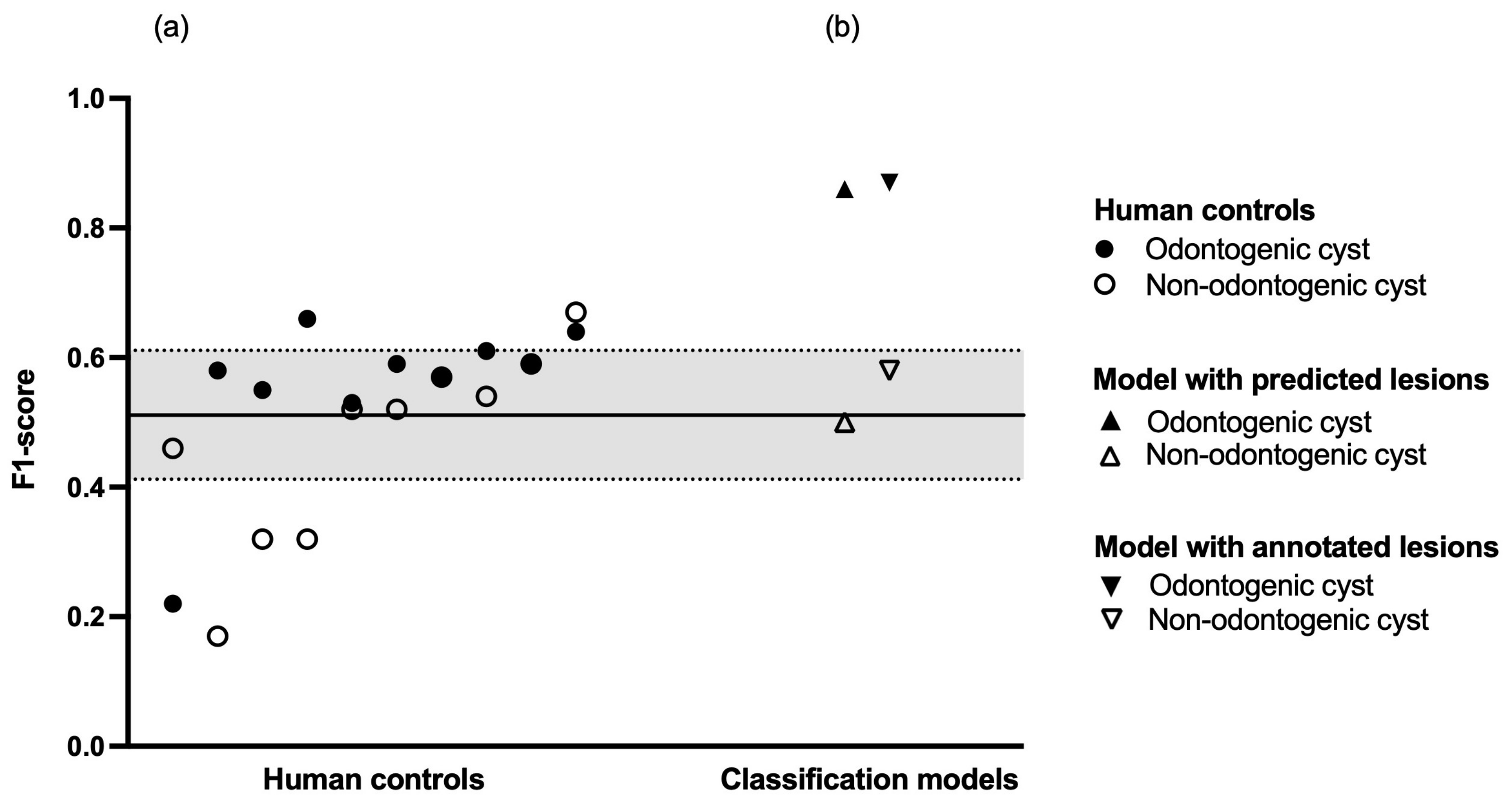
3.4. Human Diagnostic Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CCD | charge-coupled device |
| DICOM | digital imaging and communications in medicine |
| FPN | feature pyramid network |
| IoU | intersection over union |
| IQR | interquartile range |
| OPG | panoramic radiograph |
| R-CNN | region-based convolutional neural network |
| VRAM | video random access memory |
| YOLO | you only look once |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IoU | MD | Value | |
|---|---|---|---|
| Average precision | 0.50–0.95 | 100 | 0.213 |
| 0.50 | 100 | 0.424 | |
| 0.75 | 100 | 0.203 | |
| Average recall | 0.50–0.95 | 1 | 0.244 |
| 0.50–0.95 | 10 | 0.331 | |
| 0.50–0.95 | 100 | 0.394 |
| PPV (Precision) | Sensitivity (Recall) | F1-Score | |
|---|---|---|---|
| Human control 1 | |||
| Odontogenic cyst | 0.49 | 0.92 | 0.64 |
| Non-odontogenic cyst | 0.65 | 0.69 | 0.67 |
| No cyst | 0.91 | 0.41 | 0.56 |
| Accuracy | 0.61 | ||
| Macro average | 0.68 | 0.67 | 0.62 |
| Weighted average | 0.74 | 0.61 | 0.60 |
| Human control 2 | |||
| Odontogenic cyst | 0.55 | 0.64 | 0.59 |
| Non-odontogenic cyst | 0.86 | 0.38 | 0.52 |
| No cyst | 0.71 | 0.71 | 0.71 |
| Accuracy | 0.65 | ||
| Macro average | 0.70 | 0.57 | 0.61 |
| Weighted average | 0.67 | 0.65 | 0.65 |
| Human control 3 | |||
| Odontogenic cyst | 0.57 | 0.80 | 0.66 |
| Non-odontogenic cyst | 0.58 | 0.22 | 0.32 |
| No cyst | 0.82 | 0.71 | 0.76 |
| Accuracy | 0.69 | ||
| Macro average | 0.66 | 0.58 | 0.58 |
| Weighted average | 0.71 | 0.69 | 0.68 |
| Human control 4 | |||
| Odontogenic cyst | 0.56 | 0.62 | 0.59 |
| Non-odontogenic cyst | 0.47 | 0.69 | 0.56 |
| No cyst | 0.79 | 0.67 | 0.72 |
| Accuracy | 0.65 | ||
| Macro average | 0.61 | 0.66 | 0.62 |
| Weighted average | 0.68 | 0.65 | 0.66 |
| Human control 5 | |||
| Odontogenic cyst | 0.53 | 0.73 | 0.61 |
| Non-odontogenic cyst | 0.62 | 0.47 | 0.54 |
| No cyst | 0.78 | 0.64 | 0.70 |
| Accuracy | 0.65 | ||
| Macro average | 0.64 | 0.61 | 0.62 |
| Weighted average | 0.68 | 0.65 | 0.65 |
| Human control 6 | |||
| Odontogenic cyst | 0.57 | 0.50 | 0.53 |
| Non-odontogenic cyst | 0.66 | 0.59 | 0.62 |
| No cyst | 0.68 | 0.75 | 0.71 |
| Accuracy | 0.65 | ||
| Macro average | 0.64 | 0.61 | 0.62 |
| Weighted average | 0.64 | 0.65 | 0.64 |
| Human control 7 | |||
| Odontogenic cyst | 0.46 | 0.67 | 0.55 |
| Non-odontogenic cyst | 0.31 | 0.34 | 0.32 |
| No cyst | 0.75 | 0.53 | 0.62 |
| Accuracy | 0.55 | ||
| Macro average | 0.50 | 0.51 | 0.50 |
| Weighted average | 0.60 | 0.55 | 0.56 |
| Human control 8 | |||
| Odontogenic cyst | 0.87 | 0.13 | 0.22 |
| Non-odontogenic cyst | 0.69 | 0.34 | 0.46 |
| No cyst | 0.60 | 0.97 | 0.74 |
| Accuracy | 0.62 | ||
| Macro average | 0.72 | 0.48 | 0.47 |
| Weighted average | 0.70 | 0.62 | 0.54 |
| Human control 9 | |||
| Odontogenic cyst | 0.42 | 0.97 | 0.58 |
| Non-odontogenic cyst | 0.75 | 0.09 | 0.17 |
| No cyst | 0.90 | 0.32 | 0.47 |
| Accuracy | 0.51 | ||
| Macro average | 0.69 | 0.46 | 0.41 |
| Weighted average | 0.72 | 0.51 | 0.48 |
| Human control 10 | |||
| Odontogenic cyst | 0.42 | 0.89 | 0.57 |
| Non-odontogenic cyst | 0.44 | 0.81 | 0.57 |
| No cyst | 0.79 | 0.11 | 0.20 |
| Accuracy | 0.45 | ||
| Macro average | n/a | ||
| Weighted average | n/a |

References
- Yu, D.; Hu, J.; Feng, Z.; Song, M.; Zhu, H. Deep learning based diagnosis for cysts and tumors of jaw with massive healthy samples. Sci. Rep. 2022, 12, 1855. [Google Scholar] [CrossRef] [PubMed]
- González-Alva, P.; Tanaka, A.; Oku, Y.; Yoshizawa, D.; Itoh, S.; Sakashita, H.; Ide, F.; Tajima, Y.; Kusama, K. Keratocystic odontogenic tumor: A retrospective study of 183 cases. J. Oral Sci. 2008, 50, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Meara, J.G.; Shah, S.; Li, K.K.; Cunningham, M.J. The odontogenic keratocyst: A 20-year clinicopathologic review. Laryngoscope 1998, 108, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Wakolbinger, R.; Beck-Mannagetta, J. Long-term results after treatment of extensive odontogenic cysts of the jaws: A review. Clin. Oral Investig. 2016, 20, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Feher, B.; Frommlet, F.; Lettner, S.; Gruber, R.; Nemeth, L.E.; Ulm, C.; Kuchler, U. A volumetric prediction model for postoperative cyst shrinkage. Clin. Oral Investig. 2021, 25, 6093–6099. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Kwak, E.J.; You, K.S.; Jung, Y.S.; Jung, H.D. Volume change pattern of decompression of mandibular odontogenic keratocyst. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 2. [Google Scholar] [CrossRef] [PubMed]
- Altaf, F.; Islam, S.M.S.; Akhtar, N.; Janjua, N.K. Going Deep in Medical Image Analysis: Concepts, Methods, Challenges, and Future Directions. IEEE Access 2019, 7, 99540–99572. [Google Scholar] [CrossRef]
- Pauwels, R.; Araki, K.; Siewerdsen, J.H.; Thongvigitmanee, S.S. Technical aspects of dental CBCT: State of the art. Dentomaxillofac. Radiol. 2015, 44, 20140224. [Google Scholar] [CrossRef]
- Kwon, O.; Yong, T.H.; Kang, S.R.; Kim, J.E.; Huh, K.H.; Heo, M.S.; Lee, S.S.; Choi, S.C.; Yi, W.J. Automatic diagnosis for cysts and tumors of both jaws on panoramic radiographs using a deep convolution neural network. Dentomaxillofac. Radiol. 2020, 49, 20200185. [Google Scholar] [CrossRef]
- Ariji, Y.; Yanashita, Y.; Kutsuna, S.; Muramatsu, C.; Fukuda, M.; Kise, Y.; Nozawa, M.; Kuwada, C.; Fujita, H.; Katsumata, A.; et al. Automatic detection and classification of radiolucent lesions in the mandible on panoramic radiographs using a deep learning object detection technique. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 424–430. [Google Scholar] [CrossRef]
- Poedjiastoeti, W.; Suebnukarn, S. Application of Convolutional Neural Network in the Diagnosis of Jaw Tumors. Healthc. Inform. Res. 2018, 24, 236–241. [Google Scholar] [CrossRef]
- Jia, X.; Ren, L.; Cai, J. Clinical implementation of AI technologies will require interpretable AI models. Med. Phys. 2020, 47, 1–4. [Google Scholar] [CrossRef]
- Meijering, E. A bird’s-eye view of deep learning in bioimage analysis. Comput. Struct. Biotechnol. J. 2020, 18, 2312–2325. [Google Scholar] [CrossRef]
- Jiang, Z.Y.; Lan, T.J.; Cai, W.X.; Tao, Q. Primary clinical study of radiomics for diagnosing simple bone cyst of the jaw. Dentomaxillofac. Radiol. 2021, 50, 20200384. [Google Scholar] [CrossRef]
- Oda, M.; Staziaki, P.V.; Qureshi, M.M.; Andreu-Arasa, V.C.; Li, B.; Takumi, K.; Chapman, M.N.; Wang, A.; Salama, A.R.; Sakai, O. Using CT texture analysis to differentiate cystic and cystic-appearing odontogenic lesions. Eur. J. Radiol. 2019, 120, 108654. [Google Scholar] [CrossRef]
- Bowen, J.L. Educational strategies to promote clinical diagnostic reasoning. N. Engl. J. Med. 2006, 355, 2217–2225. [Google Scholar] [CrossRef]
- Lawson, A.E.; Daniel, E.S. Inferences of clinical diagnostic reasoning and diagnostic error. J. Biomed. Inform. 2011, 44, 402–412. [Google Scholar] [CrossRef]
- Monteiro, S.M.; Norman, G. Diagnostic reasoning: Where we’ve been, where we’re going. Teach. Learn. Med. 2013, 25 (Suppl. 1), S26–S32. [Google Scholar] [CrossRef]
- Lin, T.; Dollár, P.; Girshick, R.B.; He, K.; Hariharan, B.; Belongie, S.J. Feature Pyramid Networks for Object Detection. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–16 July 2017. [Google Scholar]
- Lin, T.Y.; Goyal, P.; Girshick, R.; He, K.; Dollár, P. Focal Loss for Dense Object Detection. IEEE Trans. Pattern Anal. Mach. Intell. 2020, 42, 318–327. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep Residual Learning for Image Recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Las Vegas, NV, USA, 26 June–1 July 2016; IEEE Computer Society: Los Alamitos, CA, USA, 2016; pp. 770–778. [Google Scholar] [CrossRef]
- Deng, J.; Dong, W.; Socher, R.; Li, L.J.; Li, K.; Fei-Fei, L. ImageNet: A large-scale hierarchical image database. In Proceedings of the 2009 IEEE Conference on Computer Vision and Pattern Recognition, Miami, FL, USA, 20–25 June 2009; pp. 248–255. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Schneider, L.; Arsiwala-Scheppach, L.; Krois, J.; Meyer-Lueckel, H.; Bressem, K.; Niehues, S.; Schwendicke, F. Benchmarking Deep Learning Models for Tooth Structure Segmentation. J. Dent. Res. 2022, 00220345221100169. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests–Random Features; University of California: Berkeley, CA, USA, 1999. [Google Scholar]
- Fleiss, J. Measuring nominal scale agreement among many raters. Psychol. Bull. 1971, 76, 378–382. [Google Scholar] [CrossRef]
- Yang, H.; Jo, E.; Kim, H.J.; Cha, I.H.; Jung, Y.S.; Nam, W.; Kim, J.Y.; Kim, J.K.; Kim, Y.H.; Oh, T.G.; et al. Deep Learning for Automated Detection of Cyst and Tumors of the Jaw in Panoramic Radiographs. J. Clin. Med. 2020, 9, 1839. [Google Scholar] [CrossRef]
- Kaczmarzyk, T.; Mojsa, I.; Stypulkowska, J. A systematic review of the recurrence rate for keratocystic odontogenic tumour in relation to treatment modalities. Int. J. Oral Maxillofac. Surg. 2012, 41, 756–767. [Google Scholar] [CrossRef]
- Gulshan, V.; Peng, L.; Coram, M.; Stumpe, M.C.; Wu, D.; Narayanaswamy, A.; Venugopalan, S.; Widner, K.; Madams, T.; Cuadros, J.; et al. Development and validation of a deep learning algorithm for detection of diabetic retinopathy in retinal fundus photographs. JAMA 2016, 316, 2402–2410. [Google Scholar] [CrossRef]
- Kim, J.R.; Shim, W.H.; Yoon, H.M.; Hong, S.H.; Lee, J.S.; Cho, Y.A.; Kim, S. Computerized bone age estimation using deep learning based program: Evaluation of the accuracy and efficiency. Am. J. Roentgenol. 2017, 209, 1374–1380. [Google Scholar] [CrossRef]
| Vienna | Nijmegen | Total | |
|---|---|---|---|
| Demographics | |||
| Age, median (IQR), years | 50 (39–60) | 57 (45–66) | 53.5 (41–63) |
| Female, n (% of total) | 391 (43) | 115 (35) | 506 (41) |
| Male, n (% of total) | 519 (57) | 214 (65) | 733 (59) |
| Diagnosis | |||
| Cysts, n.f.s., n (%) | 215 (23.6) | 0 (0) | 215 (17.3) |
| Odontogenic cysts, n (%) | 485 (53.3) | 102 (31) | 587 (47.3) |
| Non-odontogenic cysts, n (%) | 90 (9.9) | 139 (42.2) | 229 (18.5) |
| Negative controls, n (%) | 120 (13.2) | 88 (26.7) | 208 (16.8) |
| Odontogenic Cyst | Non-Odontogenic Cyst | |
|---|---|---|
| With predictions via object detection (IoU ≥ 0.30) | ||
| Sensitivity (Recall) | 0.84 | 0.56 |
| Specificity | 0.56 | 0.84 |
| PPV (Precision) | 0.89 | 0.45 |
| NPV | 0.45 | 0.89 |
| F1-score | 0.86 | 0.50 |
| With original annotations | ||
| Sensitivity (Recall) | 0.91 | 0.51 |
| Specificity | 0.51 | 0.91 |
| PPV (Precision) | 0.83 | 0.68 |
| NPV | 0.68 | 0.83 |
| F1-score | 0.87 | 0.58 |
| Odontogenic Cyst | Non-Odontogenic Cyst | No Cyst | |
|---|---|---|---|
| Sensitivity (Recall) | 0.70 | 0.44 | 0.56 |
| Specificity | 0.62 | 0.95 | 0.76 |
| PPV (Precision) | 0.53 | 0.58 | 0.78 |
| NPV | 0.83 | 0.94 | 0.62 |
| F1-score | 0.56 | 0.45 | 0.61 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feher, B.; Kuchler, U.; Schwendicke, F.; Schneider, L.; Cejudo Grano de Oro, J.E.; Xi, T.; Vinayahalingam, S.; Hsu, T.-M.H.; Brinz, J.; Chaurasia, A.; et al. Emulating Clinical Diagnostic Reasoning for Jaw Cysts with Machine Learning. Diagnostics 2022, 12, 1968. https://doi.org/10.3390/diagnostics12081968
Feher B, Kuchler U, Schwendicke F, Schneider L, Cejudo Grano de Oro JE, Xi T, Vinayahalingam S, Hsu T-MH, Brinz J, Chaurasia A, et al. Emulating Clinical Diagnostic Reasoning for Jaw Cysts with Machine Learning. Diagnostics. 2022; 12(8):1968. https://doi.org/10.3390/diagnostics12081968
Chicago/Turabian StyleFeher, Balazs, Ulrike Kuchler, Falk Schwendicke, Lisa Schneider, Jose Eduardo Cejudo Grano de Oro, Tong Xi, Shankeeth Vinayahalingam, Tzu-Ming Harry Hsu, Janet Brinz, Akhilanand Chaurasia, and et al. 2022. "Emulating Clinical Diagnostic Reasoning for Jaw Cysts with Machine Learning" Diagnostics 12, no. 8: 1968. https://doi.org/10.3390/diagnostics12081968
APA StyleFeher, B., Kuchler, U., Schwendicke, F., Schneider, L., Cejudo Grano de Oro, J. E., Xi, T., Vinayahalingam, S., Hsu, T.-M. H., Brinz, J., Chaurasia, A., Dhingra, K., Gaudin, R. A., Mohammad-Rahimi, H., Pereira, N., Perez-Pastor, F., Tryfonos, O., Uribe, S. E., Hanisch, M., & Krois, J. (2022). Emulating Clinical Diagnostic Reasoning for Jaw Cysts with Machine Learning. Diagnostics, 12(8), 1968. https://doi.org/10.3390/diagnostics12081968