
Association of Handgrip Strength with Diabetes Mellitus in Korean Adults According to Sex


Abstract
:1. Introduction
2. Materials and Methods
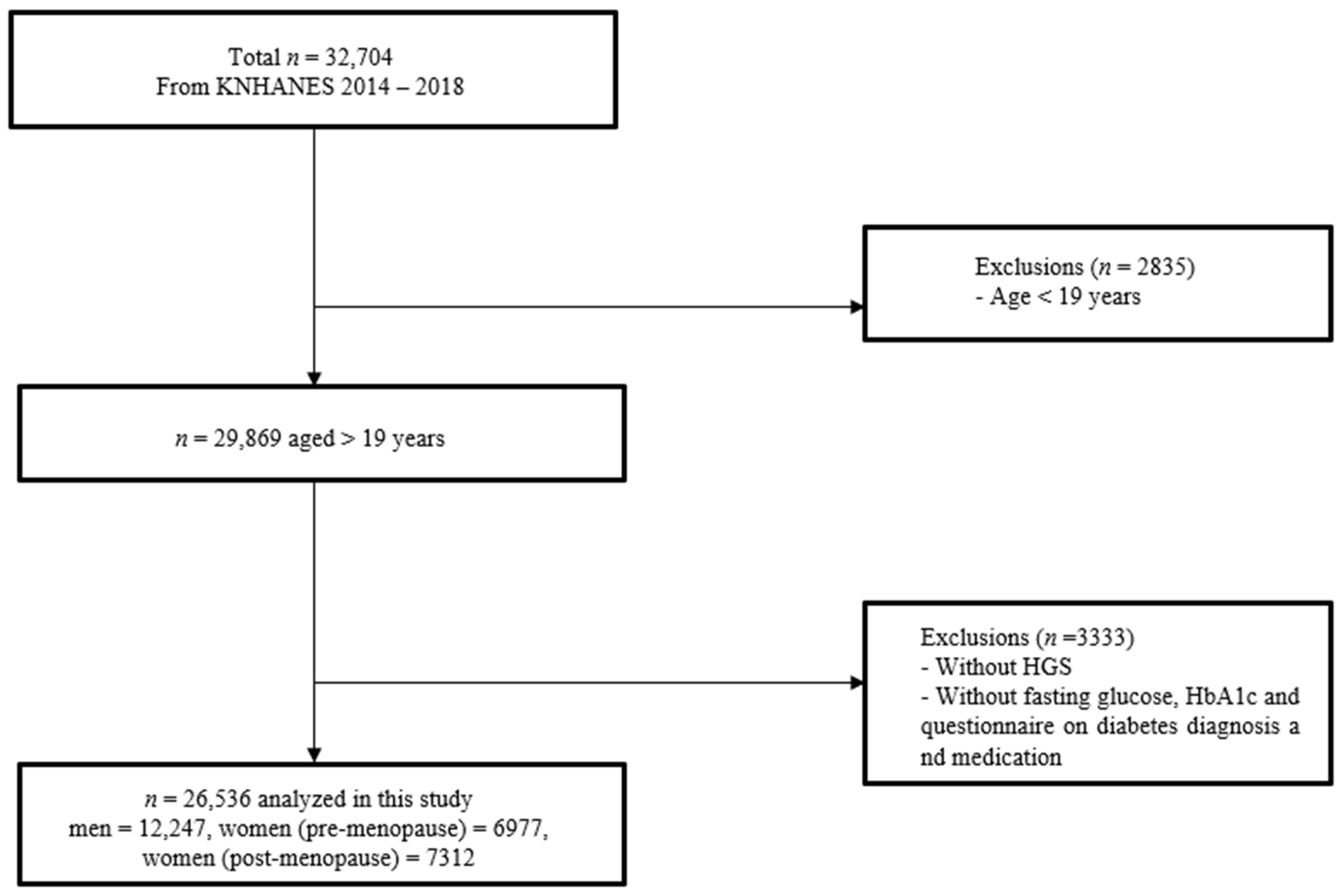
2.1. Study Population
2.2. Measurement of Handgrip Strength
2.3. Anthropometric and Laboratory Measurements and General Data
2.4. Definition of Diabetes Mellitus
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
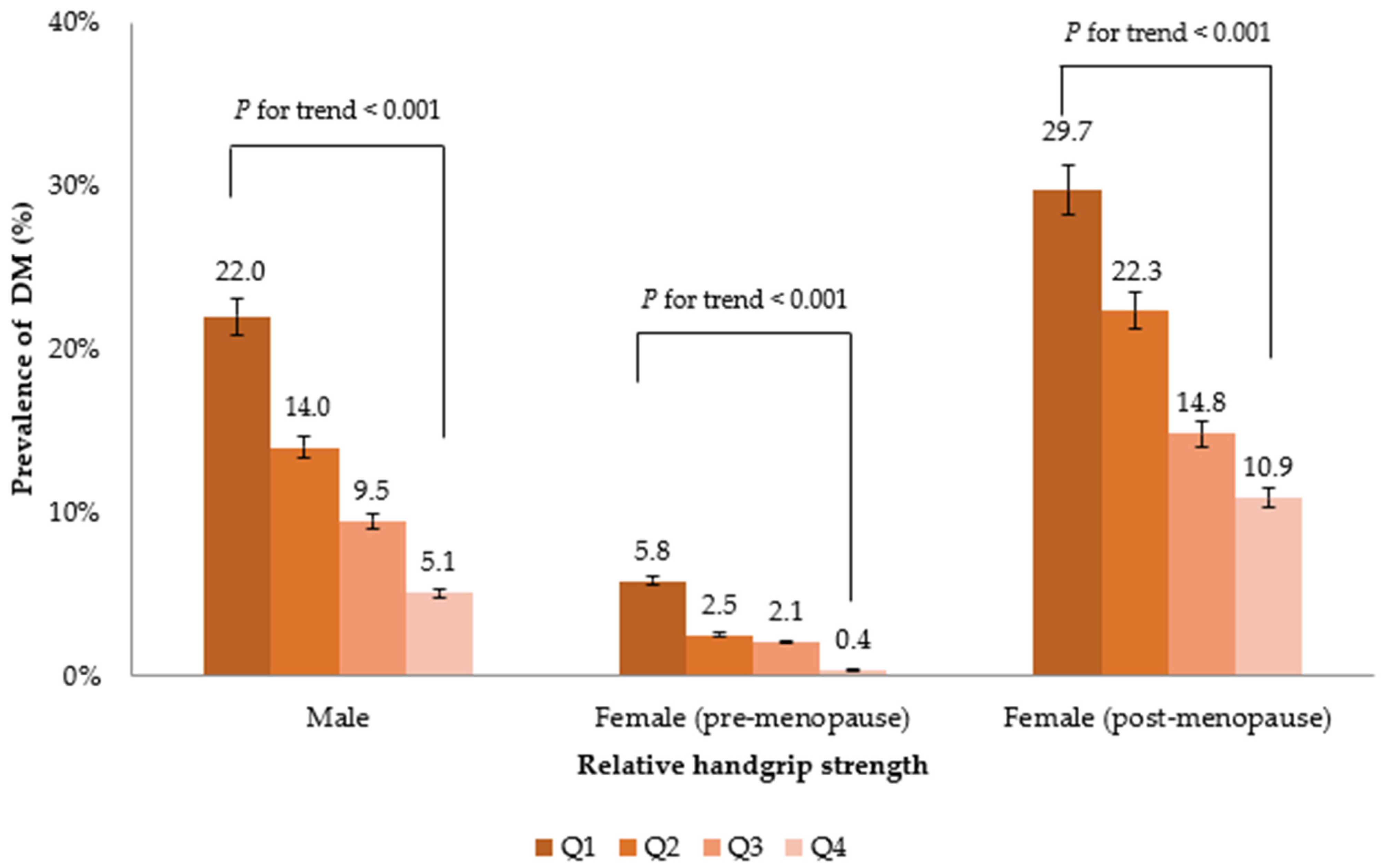
3.2. Association between RGS and the Prevalence of DM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yuen, L.; Saeedi, P.; Riaz, M.; Karuranga, S.; Divakar, H.; Levitt, N.; Yang, X.; Simmons, D. Projections of the prevalence of hyperglycaemia in pregnancy in 2019 and beyond: Results from the international diabetes federation diabetes atlas. Diabetes Res. Clin. Pract. 2019, 157, 107841. [Google Scholar] [CrossRef] [Green Version]
- Zelnick, L.R.; Weiss, N.S.; Kestenbaum, B.R.; Robinson-Cohen, C.; Heagerty, P.J.; Tuttle, K.; Hall, Y.N.; Hirsch, I.B.; de Boer, I.H. Diabetes and ckd in the united states population, 2009–2014. Clin. J. Am. Soc. Nephrol. 2017, 12, 1984–1990. [Google Scholar] [CrossRef] [Green Version]
- Nowakowska, M.; Zghebi, S.S.; Ashcroft, D.M.; Buchan, I.; Chew-Graham, C.; Holt, T.; Mallen, C.; Van Marwijk, H.; Peek, N.; Perera-Salazar, R. The comorbidity burden of type 2 diabetes mellitus: Patterns, clusters and predictions from a large english primary care cohort. BMC Med. 2019, 17, 145. [Google Scholar] [CrossRef]
- Mayhew, A.; Amog, K.; Phillips, S.; Parise, G.; McNicholas, P.; De Souza, R.; Thabane, L.; Raina, P. The prevalence of sarcopenia in community-dwelling older adults, an exploration of differences between studies and within definitions: A systematic review and meta-analyses. Age Ageing 2019, 48, 48–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atlantis, E.; Martin, S.A.; Haren, M.T.; Taylor, A.W.; Wittert, G.A. Inverse associations between muscle mass, strength, and the metabolic syndrome. Metabolism 2009, 58, 1013–1022. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, W.; Liu, T.; Zhang, D. Association of grip strength with risk of all-cause mortality, cardiovascular diseases, and cancer in community-dwelling populations: A meta-analysis of prospective cohort studies. J. Am. Med. Dir. Assoc. 2017, 18, 551.e17–551.e35. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Rantanen, T.; Guralnik, J.M.; Foley, D.; Masaki, K.; Leveille, S.; Curb, J.D.; White, L. Midlife hand grip strength as a predictor of old age disability. JAMA 1999, 281, 558–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.-B.; Kwon, Y.-J.; Jung, D.-H.; Kim, J.-K. Association of muscle strength with non-alcoholic fatty liver disease in korean adults. Int. J. Environ. Res. Public Health 2022, 19, 1675. [Google Scholar] [CrossRef]
- Peterson, M.D.; Zhang, P.; Choksi, P.; Markides, K.S.; Al Snih, S. Muscle weakness thresholds for prediction of diabetes in adults. Sports Med. 2016, 46, 619–628. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.-R.; Jung, S.M.; Bang, H.; Kim, H.S.; Kim, Y.B. Association between muscle strength and type 2 diabetes mellitus in adults in korea: Data from the korea national health and nutrition examination survey (knhanes) vi. Medicine 2018, 97, e10984. [Google Scholar] [CrossRef] [PubMed]
- Leong, D.; Teo, K.; Rangarajan, S.; Lopez-Jaramillo, P.; Avezum, A., Jr.; Orlandini, A.; Seron, P.; Ahmed, S.; Rosengren, A.; Kelishadi, R. Prospective urban rural epidemiology (pure) study investigators. Prognostic value of grip strength: Findings from the prospective urban rural epidemiology (pure) study. Lancet 2015, 386, 266–273. [Google Scholar] [CrossRef]
- Xu, L.; Hao, Y.T. Effect of handgrip on coronary artery disease and myocardial infarction: A mendelian randomization study. Sci. Rep. 2017, 7, 954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Studenski, S.A.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M. The fnih sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Choquette, S.; Bouchard, D.; Doyon, C.; Sénéchal, M.; Brochu, M.; Dionne, I.J. Relative strength as a determinant of mobility in elders 67–84 years of age. A nuage study: Nutrition as a determinant of successful aging. J. Nutr. Health Aging 2010, 14, 190–195. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.-j.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The korea national health and nutrition examination survey (knhanes). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Koo, B.K. The differential association between muscle strength and diabetes mellitus according to the presence or absence of obesity. J. Obes. Metab. Syndr. 2019, 28, 46. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.; Lee, I.; Park, D.-H.; Kwak, H.-B.; Min, K. Relationships between socioeconomic status, handgrip strength, and non-alcoholic fatty liver disease in middle-aged adults. Int. J. Environ. Res. Public Health 2021, 18, 1892. [Google Scholar] [CrossRef]
- Lee, J.S.; Song, Y.H. Relationship between waist circumference and cardiovascular risk factors in adolescents: Analysis of the korea national health and nutrition examination survey data. Korean Circ. J. 2020, 50, 723–732. [Google Scholar] [CrossRef]
- Kang, M.G.; Kim, K.H.; Koh, J.S.; Park, J.R.; Hwang, S.J.; Hwang, J.Y.; Ahn, J.H.; Jang, J.Y.; Jeong, Y.H.; Kwak, C.H. Association between pulse pressure and body mass index in hypertensive and normotensive populations in the korea national health and nutrition examination survey v, 2010–2012. J. Clin. Hypertens. 2017, 19, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Chobanian, A.V. National heart, lung, and blood institute joint national committee on prevention, detection, evaluation, and treatment of high blood pressure; national high blood pressure education program coordinating committee: The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The jnc 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [PubMed]
- Kang, K.-W.; Sung, J.-H.; Kim, C.-y. High risk groups in health behavior defined by clustering of smoking, alcohol, and exercise habits: National heath and nutrition examination survey. J. Prev. Med. Public Health 2010, 43, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.-J.; Lee, J.-w.; Kang, H.-T.; Cho, M.-C.; Lim, H.-J.; Kim, J.-Y.; Bae, J.-W.; Lee, Y.-J.; Lee, S.-H.; Linton, J.A. Trends in blood pressure and prevalence of hypertension in korean adults based on the 1998–2014 knhanes. Yonsei Med. J. 2018, 59, 356–365. [Google Scholar] [CrossRef]
- Kim, S.; Choi, S.; Kim, J.; Park, S.; Kim, Y.; Park, O.; Oh, K. Trends in health behaviors over 20 years: Findings from the 1998–2018 korea national health and nutrition examination survey. Epidemiol. Health 2021, 43, e2021026. [Google Scholar] [CrossRef]
- Oh, I.H.; Park, J.H.; Lee, C.H.; Park, J.-S. The association of normal range glycated hemoglobin with restrictive lung pattern in the general population. PLoS ONE 2015, 10, e0117725. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Classification of Diabetes Mellitus; WHO: Geneva, Switzerland, 2019.
- Li, D.; Guo, G.; Xia, L.; Yang, X.; Zhang, B.; Liu, F.; Ma, J.; Hu, Z.; Li, Y.; Li, W. Relative handgrip strength is inversely associated with metabolic profile and metabolic disease in the general population in china. Front. Physiol. 2018, 9, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A. Sarcopenia: Revised european consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Schaap, L.A.; Van Schoor, N.M.; Lips, P.; Visser, M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: The longitudinal aging study amsterdam. J. Gerontol. Ser. A 2018, 73, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Agostinis-Sobrinho, C.A.; Moreira, C.; Abreu, S.; Lopes, L.; Sardinha, L.B.; Oliveira-Santos, J.; Oliveira, A.; Mota, J.; Santos, R. Muscular fitness and metabolic and inflammatory biomarkers in adolescents: Results from labmed physical activity study. Scand. J. Med. Sci. Sports 2017, 27, 1873–1880. [Google Scholar] [CrossRef] [Green Version]
- Schaap, L.A.; Pluijm, S.M.; Deeg, D.J.; Harris, T.B.; Kritchevsky, S.B.; Newman, A.B.; Colbert, L.H.; Pahor, M.; Rubin, S.M.; Tylavsky, F.A. Higher inflammatory marker levels in older persons: Associations with 5-year change in muscle mass and muscle strength. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2009, 64, 1183–1189. [Google Scholar] [CrossRef] [Green Version]
- Pradhan, A.D.; Manson, J.E.; Rifai, N.; Buring, J.E.; Ridker, P.M. C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus. JAMA 2001, 286, 327–334. [Google Scholar] [CrossRef]
- Whitcomb, B.W.; Mumford, S.L.; Perkins, N.J.; Wactawski-Wende, J.; Bertone-Johnson, E.R.; Lynch, K.E.; Schisterman, E.F. Urinary cytokine and chemokine profiles across the menstrual cycle in healthy reproductive-aged women. Fertil. Steril. 2014, 101, 1383–1391.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakumoto, R.; Okuda, K. Possible actions of tumor necrosis factor-α in ovarian function. J. Reprod. Dev. 2004, 50, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertone-Johnson, E.R.; Manson, J.E.; Purdue-Smithe, A.C.; Hankinson, S.E.; Rosner, B.A.; Whitcomb, B.W. A prospective study of inflammatory biomarker levels and risk of early menopause. Menopause 2019, 26, 32. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Smith, L.; Hamer, M. Gender-specific risk factors for incident sarcopenia: 8-year follow-up of the english longitudinal study of ageing. J. Epidemiol. Community Health 2019, 73, 86–88. [Google Scholar] [CrossRef] [PubMed]
- Geraci, A.; Calvani, R.; Ferri, E.; Marzetti, E.; Arosio, B.; Cesari, M. Sarcopenia and menopause: The role of estradiol. Front. Endocrinol. 2021, 12, 588. [Google Scholar] [CrossRef] [PubMed]
- Paschou, S.A.; Anagnostis, P.; Pavlou, D.I.; Vryonidou, A.; Goulis, D.G.; Lambrinoudaki, I. Diabetes in menopause: Risks and management. Curr. Vasc. Pharmacol. 2019, 17, 556–563. [Google Scholar] [CrossRef]
- Lambrinoudaki, I.; Brincat, M.; Erel, C.T.; Gambacciani, M.; Moen, M.H.; Schenck-Gustafsson, K.; Tremollieres, F.; Vujovic, S.; Rees, M.; Rozenberg, S. Emas position statement: Managing obese postmenopausal women. Maturitas 2010, 66, 323–326. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F.; Manson, J.E.; Stevenson, J.C.; Fonseca, V.A. Menopausal hormone therapy and type 2 diabetes prevention: Evidence, mechanisms, and clinical implications. Endocr. Rev. 2017, 38, 173–188. [Google Scholar] [CrossRef] [Green Version]
- Alley, D.E.; Shardell, M.D.; Peters, K.W.; McLean, R.R.; Dam, T.-T.L.; Kenny, A.M.; Fragala, M.S.; Harris, T.B.; Kiel, D.P.; Guralnik, J.M. Grip strength cutpoints for the identification of clinically relevant weakness. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2014, 69, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; Maggi, S.; Dennison, E.; Al-Daghri, N.M.; Allepaerts, S. Pitfalls in the measurement of muscle mass: A need for a reference standard. J. Cachexia Sarcopenia Muscle 2018, 9, 269–278. [Google Scholar] [CrossRef]
- Nevill, A.M.; Tomkinson, G.R.; Lang, J.J.; Wutz, W.; Myers, T.D. How should adult handgrip strength be normalized? Allometry reveals new insights and associated reference curves. Med. Sci. Sports Exerc. 2021, 54, 162–168. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Men | Q1 | Q2 | Q3 | Q4 | |
| ≤2.84 | 2.85–3.30 | 3.31–3.75 | >3.75 | ||
| n | 12,247 | 3721 | 3170 | 2809 | 2547 |
| Age (years) | 45.7 ± 0.2 | 52.6 ± 0.4 | 47.2 ± 0.4 | 43.7 ± 0.3 | 39.3 ± 0.3 |
| Waist circumference (cm) | 85.8 ± 0.2 | 91.0 ± 0.2 | 87.3 ± 0.2 | 84.6 ± 0.2 | 80.5 ± 0.2 |
| BMI (kg/m2) | 24.5 ± 0.1 | 26.3 ± 0.1 | 25.0 ± 0.1 | 24.0 ± 0.1 | 22.6 ± 0.1 |
| Fasting glucose (mg/dL) | 102.1 ± 0.3 | 108.3 ± 0.6 | 103.7 ± 0.5 | 100.7 ± 0.6 | 95.9 ± 0.4 |
| Total cholesterol (mg/dL) | 190.6 ± 0.4 | 189.1 ± 0.8 | 193.1 ± 0.8 | 192.3 ± 0.8 | 187.9 ± 0.8 |
| Triglyceride (mg/dL) | 164.4 ± 1.7 | 167.9 ± 2.7 | 181.1 ± 3.3 | 163.4 ± 3.3 | 145.5 ± 3.6 |
| AST (IU/L) | 24.9 ± 0.3 | 27.4 ± 0.4 | 25.6 ± 0.3 | 24.1 0.2 | 22.5 ± 0.3 |
| ALT (IU/L) | 27.6 ± 0.4 | 32.6 ± 0.6 | 29.7 ± 0.5 | 26.1 ± 0.4 | 22.4 ± 0.3 |
| Systolic BP (mmHg) | 119.8 ± 0.2 | 122.9 ± 0.3 | 120.9 ± 0.3 | 119.2 ± 0.3 | 116.3 ± 0.3 |
| Diastolic BP (mmHg) | 78.1 ± 0.2 | 77.7 ± 0.2 | 78.9 ± 0.2 | 78.8 ± 0.2 | 77.2 ± 0.2 |
| Smoking status, n (%) | |||||
| Never smoker | 2776 (25.3) | 871 (26.8) | 705 (25.1) | 635 (25.4) | 565 (23.9) |
| Ex-smoker | 4882 (36.1) | 1720 (41.9) | 1341 (38.6) | 1019 (33.7) | 802 (30.4) |
| Current smoker | 4248 (38.6) | 1011 (31.3) | 1054 (36.3) | 1071 (40.9) | 1112 (45.7) |
| Alcohol uptake, n (%) | 3816 (33.9) | 923 (27.8) | 1028 (35.6) | 988 (36.4) | 880 (35.9) |
| Regular exercise, n (%) | 3386 (32.7) | 736 (24.3) | 869 (31.0) | 890 (35.9) | 891 (39.8) |
| Hypertension, n (%) | 4178 (29.4) | 1813 (43.4) | 1154 (32.7) | 747 (24.5) | 464 (16.8) |
| Women (premenopause) | Q1 | Q2 | Q3 | Q4 | |
| ≤1.90 | 1.91–2.22 | 2.23–2.53 | >2.53 | ||
| N | 6977 | 1757 | 1749 | 1765 | 1706 |
| Age (years) | 35.4 ± 0.1 | 36.1 ± 0.3 | 35.6 ± 0.3 | 35.5 ± 0.3 | 34.5 ± 0.3 |
| Waist circumference (cm) | 75.4 ± 0.3 | 81.3 ± 0.3 | 76.4 ± 0.3 | 73.3 ± 0.2 | 70.1 ± 0.2 |
| BMI (kg/m2) | 22.6 ± 0.1 | 25.3 ± 0.1 | 23.1 ± 0.1 | 21.7 ± 0.1 | 20.4 ± 0.1 |
| Fasting glucose (mg/dL) | 92.3 ± 0.2 | 95.8 ± 0.6 | 92.7 ± 0.5 | 90.8 ± 0.3 | 89.8 ± 0.2 |
| Total cholesterol (mg/dL) | 186.8 ± 0.5 | 193.4 ± 1.1 | 187.8 ± 0.8 | 185.7 ± 0.9 | 180.1 ± 0.8 |
| Triglyceride (mg/dL) | 96.6 ± 0.9 | 115.3 ± 2.2 | 99.3 ± 1.9 | 92.1 ± 1.7 | 80.2 ± 1.3 |
| AST (IU/L) | 18.7 ± 0.2 | 20.3 ± 0.3 | 18.3 ± 0.2 | 18.2 ± 0.2 | 17.8 ± 0.2 |
| ALT (IU/L) | 15.4 ± 0.3 | 19.0 ± 0.5 | 15.1 ± 0.3 | 14.3 ± 0.3 | 13.2 ± 0.2 |
| Systolic BP (mmHg) | 107.6 ± 0.2 | 109.7 ± 0.4 | 107.8 ± 0.3 | 106.6 ± 0.3 | 106.1 ± 0.3 |
| Diastolic BP (mmHg) | 71.6 ± 0.3 | 73.2 ± 0.2 | 71.7 ± 0.3 | 70.9 ± 0.3 | 70.7 ± 0.3 |
| Smoking status, n (%) | |||||
| Never smoker | 5941 (84.9) | 1490 (84.1) | 1496 (85.5) | 1501 (85.5) | 1454 (84.5) |
| Ex-smoker | 569 (8.1) | 141 (8.2) | 132 (7.3) | 159 (8.4) | 137 (8.4) |
| Current smoker | 458 (7.0) | 124 (7.7) | 119 (7.2) | 101 (6.1) | 114 (7.1) |
| Alcohol uptake, n (%) | 914 (13.5) | 249 (14.5) | 239 (13.6) | 194 (11.4) | 232 (14.5) |
| Regular exercise, n (%) | 2023 (29.6) | 426 (23.8) | 482 (28.7) | 559 (32.3) | 556 (33.4) |
| Hypertension, n (%) | 467 (6.1) | 189 (10.2) | 128 (6.3) | 85 (4.5) | 65 (3.4) |
| Women (postmenopause) | Q1 | Q2 | Q3 | Q4 | |
| ≤1.48 | 1.49–1.81 | 1.82–2.13 | >2.13 | ||
| N | 7312 | 1938 | 1897 | 1787 | 1690 |
| Age (years) | 63.3 ± 0.2 | 69.4 ± 0.3 | 64.5 ± 0.3 | 61.4 ± 0.2 | 57.6 ± 0.2 |
| Waist circumference (cm) | 81.8 ± 0.3 | 86.3 ± 0.3 | 84.0 ± 0.3 | 80.8 ± 0.2 | 76.2 ± 0.2 |
| BMI (kg/m2) | 24.1 ± 0.1 | 25.8 ± 0.1 | 24.9 ± 0.1 | 23.8 ± 0.1 | 22.1 ± 0.1 |
| Fasting glucose (mg/dL) | 103.4 ± 0.4 | 108.0 ± 0.8 | 105.3 ± 0.7 | 101.5 ± 0.6 | 99.3 ± 0.6 |
| Total cholesterol (mg/dL) | 199.5 ± 0.6 | 193.1 ± 1.2 | 198.4 ± 1.2 | 203.5 ± 1.1 | 202.4 ± 1.0 |
| Triglyceride (mg/dL) | 132.0 ± 1.3 | 141.8 ± 2.6 | 138.6 ± 2.6 | 129.7 ± 2.5 | 118.6 ± 2.3 |
| AST (IU/L) | 23.4 ± 0.3 | 23.9 ± 0.3 | 24.2 ± 0.4 | 23.2 ± 0.2 | 22.4 ± 0.2 |
| ALT (IU/L) | 20.4 ± 0.4 | 20.4 ± 0.4 | 21.6 ± 0.5 | 20.8 ± 0.3 | 18.8 ± 0.3 |
| Systolic BP (mmHg) | 123.7 ± 0.3 | 127.8 ± 0.5 | 125.6 ± 0.5 | 122.6 ± 0.5 | 118.8 ± 0.5 |
| Diastolic BP (mmHg) | 74.7 ± 0.3 | 73.4 ± 0.3 | 75.0 ± 0.3 | 75.4 ± 0.3 | 75.0 ± 0.3 |
| Smoking status, n (%) | |||||
| Never smoker | 6749 (92.8) | 1770 (92.3) | 1773 (94.4) | 1646 (92.5) | 1560 (92.1) |
| Ex-smoker | 247 (3.4) | 75 (4.1) | 62 (3.0) | 66 (3.6) | 44 (2.8) |
| Current smoker | 245 (3.8) | 68 (3.6) | 41 (2.6) | 60 (4.0) | 76 (5.1) |
| Alcohol uptake, n (%) | 319 (5.1) | 46 (2.7) | 83 (5.4) | 95 (5.9) | 95 (6.4) |
| Regular exercise, n (%) | 1109 (16.2) | 163 (8.4) | 238 (13.5) | 304 (18.1) | 404 (24.8) |
| Hypertension, n (%) | 3567 (45.6) | 1246 (63.5) | 1038 (50.2) | 775 (40.4) | 508 (28.2) |
| Men | Women (Premenopause) | Women (Postmenopause) | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | p-Value | OR | p-Value | OR | p-Value | |||
| Unadjusted | 0.41 (0.37–0.45) | <0.001 | Unadjusted | 0.21 (0.15–0.28) | <0.001 | Unadjusted | 0.36 (0.31–0.42) | <0.001 |
| Model 1 | 0.59 (0.53–0.67) | <0.001 | Model 1 | 0.23 (0.17–0.32) | <0.001 | Model 1 | 0.50 (0.42–0.59) | <0.001 |
| Model 2 | 0.79 (0.68–0.91) | 0.001 | Model 2 | 0.65 (0.46–0.93) | 0.018 | Model 2 | 0.80 (0.66–0.98) | 0.027 |
| Model 3 | 0.84 (0.74–0.95) | 0.007 | Model 3 | 0.68 (0.47–0.97) | 0.035 | Model 3 | 0.83 (0.68–1.01) | 0.058 |
| Men | Women (Pre-Menopause) | Women (Post-Menopause) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | Q1 | Q2 | Q3 | Q4 | |
| ≤2.84 | 2.85–3.30 | 3.31–3.75 | >3.75 | ≤1.90 | 1.91–2.22 | 2.22–2.53 | >2.53 | ≤1.48 | 1.48–1.81 | 1.81–2.13 | >2.13 | |
| Unadjusted | 1.00 | 0.56 (0.48–0.66) | 0.39 (0.32–0.46) | 0.16 (0.13–0.21) | 1.00 | 0.42 (0.29–0.62) | 0.35 (0.22–0.54) | 0.07 (0.03–0.15) | 1.00 | 0.68 (0.57–0.81) | 0.41 (0.33–0.50) | 0.29 (0.23–0.36) |
| Model 1 | 1.00 | 0.72 (0.61–0.85) | 0.60 (0.50–0.72) | 0.32 (0.25–0.41) | 1.00 | 0.44 (0.30–0.66) | 0.38 (0.24–0.59) | 0.08 (0.04–0.18) | 1.00 | 0.81 (0.67–0.98) | 0.54 (0.44–0.67) | 0.44 (0.34–0.56) |
| Model 2 | 1.00 | 0.88 (0.75–1.04) | 0.85 (0.70–1.04) | 0.54 (0.42–0.71) | 1.00 | 0.78 (0.50–1.22) | 1.03 (0.62–1.71) | 0.30 (0.14–0.66) | 1.00 | 0.92 (0.75–1.12) | 0.75 (0.60–0.94) | 0.81 (0.62–1.05) |
| Model 3 | 1.00 | 0.87 (0.73–1.04) | 0.90 (0.73–1.10) | 0.57 (0.43–0.75) | 1.00 | 0.82 (0.52–1.30) | 1.10 (0.65–1.86) | 0.33 (0.14–0.75) | 1.00 | 0.91 (0.73–1.12) | 0.77 (0.61–0.97) | 0.82 (0.63–1.07) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.-B.; Moon, J.-E.; Kim, J.-K. Association of Handgrip Strength with Diabetes Mellitus in Korean Adults According to Sex. Diagnostics 2022, 12, 1874. https://doi.org/10.3390/diagnostics12081874
Lee S-B, Moon J-E, Kim J-K. Association of Handgrip Strength with Diabetes Mellitus in Korean Adults According to Sex. Diagnostics. 2022; 12(8):1874. https://doi.org/10.3390/diagnostics12081874
Chicago/Turabian StyleLee, Sung-Bum, Ji-Eun Moon, and Jong-Koo Kim. 2022. "Association of Handgrip Strength with Diabetes Mellitus in Korean Adults According to Sex" Diagnostics 12, no. 8: 1874. https://doi.org/10.3390/diagnostics12081874
APA StyleLee, S.-B., Moon, J.-E., & Kim, J.-K. (2022). Association of Handgrip Strength with Diabetes Mellitus in Korean Adults According to Sex. Diagnostics, 12(8), 1874. https://doi.org/10.3390/diagnostics12081874