
Genetic Testing at Diagnosis Has Prognostic Value in Patients with Chronic Lymphocytic Leukemia including at Early Stages

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials & Methods
2.1. Ethics
2.2. Patients
2.3. Statistical Methods
3. Results
3.1. Characteristics of the Study Population
3.2. Molecular Variables
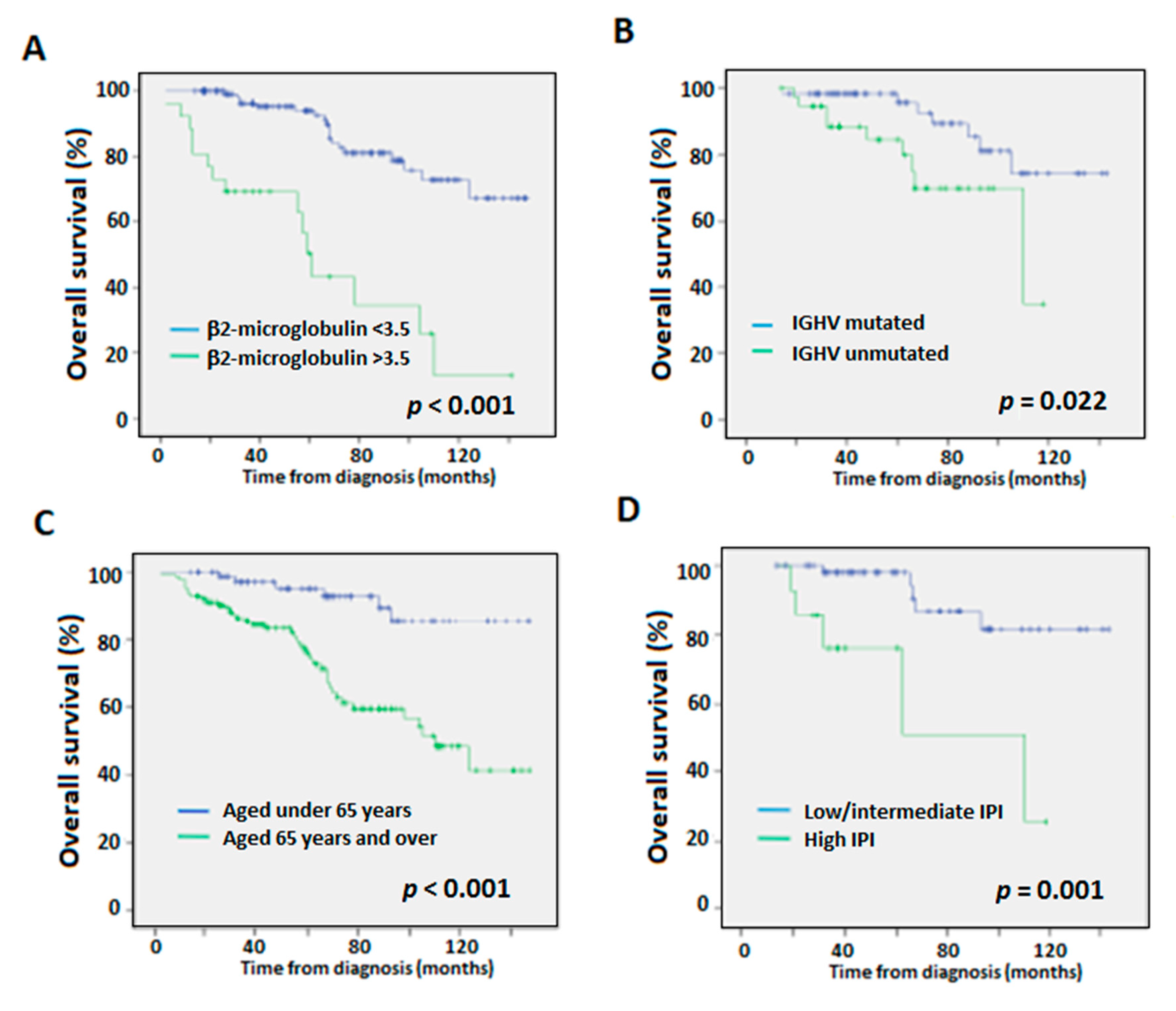
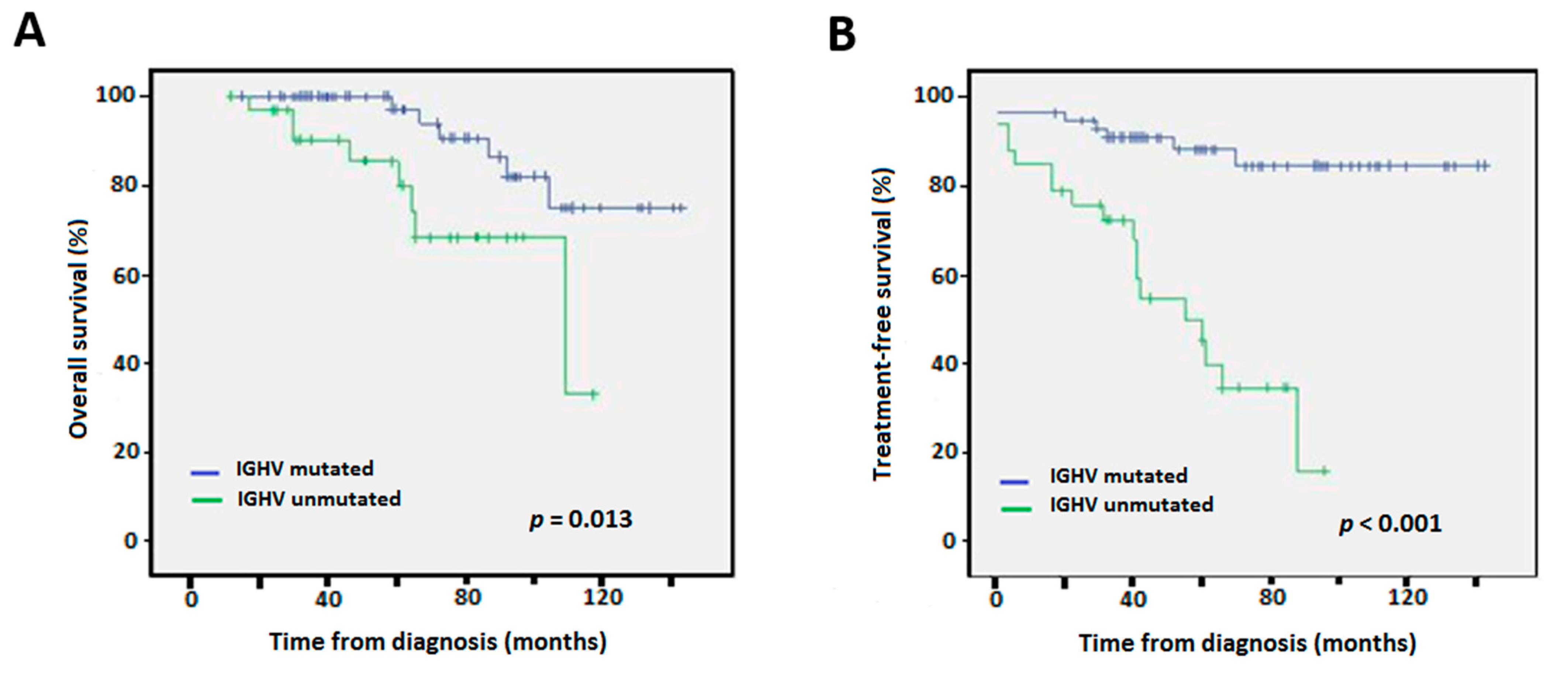
3.3. Overall Survival (OS)
3.4. Time to First Treatment (TTFT)
3.5. Associations between Molecular Variables and Clinical Staging
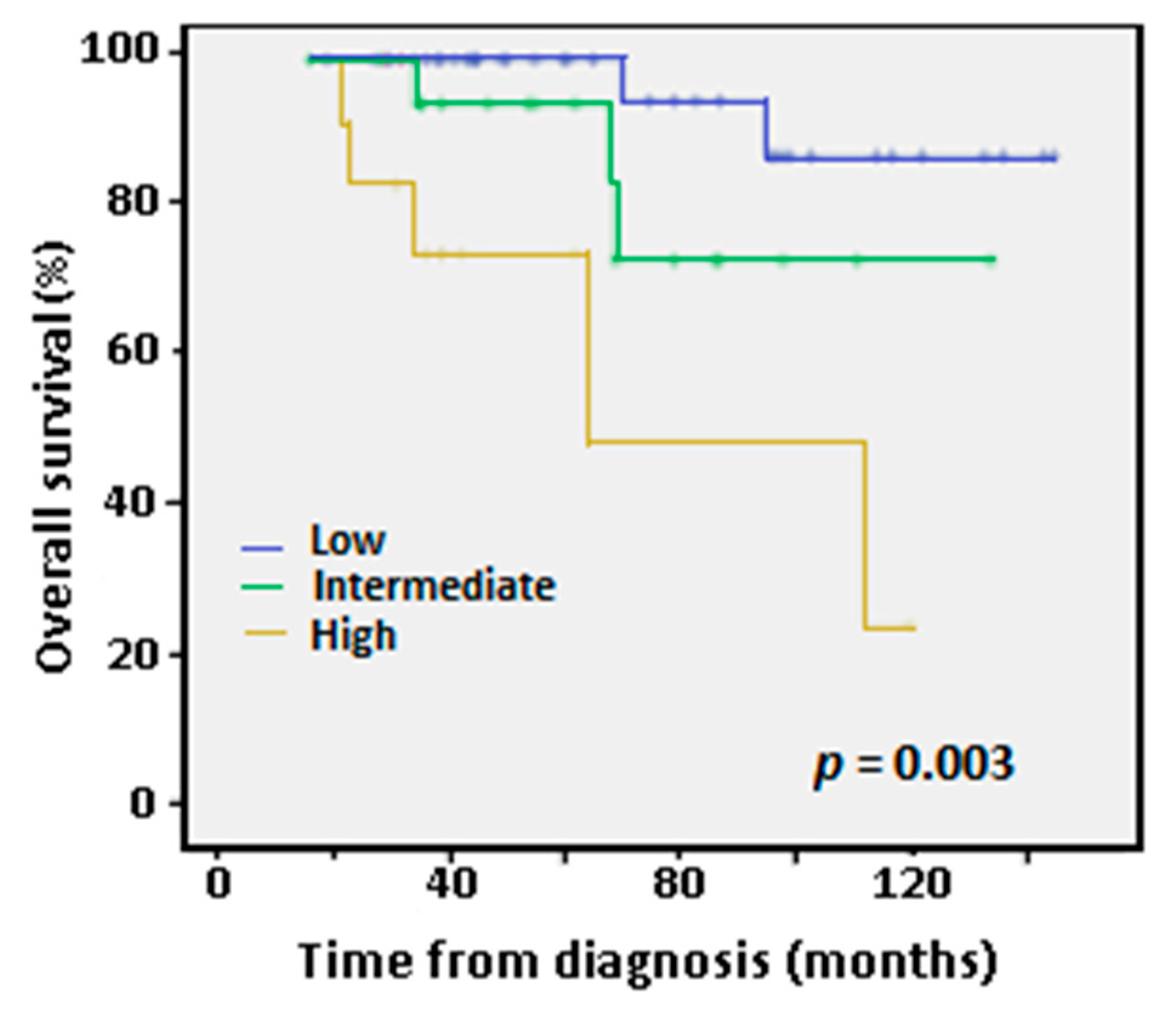
3.6. Validation of the IPS-E Prognostic Score
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sant, M.; Allemani, C.; Tereanu, C.; De Angelis, R.; Capocaccia, R.; Visser, O.; Marcos-Gragera, R.; Maynadié, M.; Simonetti, A.; Lutz, J.-M.; et al. Incidence of hematologic malignancies in Europe by morphologic subtype: Results of the HAEMACARE project. Blood 2010, 116, 3724–3734. [Google Scholar] [CrossRef] [PubMed]
- Hallek, M. Chronic lymphocytic leukemia: 2015 Update on diagnosis, risk stratification, and treatment. Am. J. Hematol. 2015, 90, 446–460. [Google Scholar] [CrossRef] [PubMed]
- Rai, K.R.; Sawitsky, A.; Cronkite, E.P.; Chanana, A.D.; Levy, R.N.; Pasternack, B.S. Clinical staging of chronic lymphocytic leukemia. Blood 1975, 46, 219–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binet, J.L.; Auquier, A.; Dighiero, G.; Chastang, C.; Piguet, H.; Goasguen, J.; Vaugier, G.; Potron, G.; Colona, P.; Oberling, F.; et al. A new prognostic classification of chronic lymphocytic leukemia derived from a multivariate survival analysis. Cancer 1981, 48, 198–206. [Google Scholar] [CrossRef]
- Hallek, M.; Cheson, B.D.; Catovsky, D.; Caligaris-Cappio, F.; Dighiero, G.; Döhner, H.; Hillmen, P.; Keating, M.J.; Montserrat, E.; Rai, K.R.; et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: A report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute–Working Group 1996 guidelines. Blood 2008, 111, 5446–5456. [Google Scholar] [CrossRef] [Green Version]
- Hallek, M.; Cheson, B.D.; Catovsky, D.; Caligaris-Cappio, F.; Dighiero, G.; Döhner, H.; Hillmen, P.; Keating, M.; Montserrat, E.; Chiorazzi, N.; et al. iwCLL guidelines for diagnosis, indications for treatment, response assessment, and supportive management of CLL. Blood 2018, 131, 2745–2760. [Google Scholar] [CrossRef] [Green Version]
- Hamblin, T.J.; Davis, Z.; Gardiner, A.; Oscier, D.G.; Stevenson, F. Unmutated Ig V(H) genes are associated with a more aggressive form of chronic lymphocytic leukemia. Blood 1999, 94, 1848–1854. [Google Scholar] [CrossRef]
- Damle, R.N.; Wasil, T.; Fais, F.; Ghiotto, F.; Valetto, A.; Allen, S.L.; Buchbinder, A.; Budman, D.; Dittmar, K.; Kolitz, J.; et al. Ig V gene mutation status and CD38 expression as novel prognostic indicators in chronic lymphocytic leukemia. Blood 1999, 94, 1840–1847. [Google Scholar] [CrossRef]
- Thompson, P.A.; Tam, C.S.; O’Brien, S.M.; Wierda, W.G.; Stingo, F.C.; Plunkett, W.; Smith, S.C.; Kantarjian, H.M.; Freireich, E.J.; Keating, M.J. Fludarabine, cyclophosphamide, and rituximab treatment achieves long-term disease-free survival in IGHV-mutated chronic lymphocytic leukemia. Blood 2016, 127, 303–309. [Google Scholar] [CrossRef]
- Rossi, D.; Terzi-Di-Bergamo, L.; De Paoli, L.; Cerri, M.; Ghilardi, G.; Chiarenza, A.; Bulian, P.; Visco, C.; Mauro, F.R.; Morabito, F.; et al. Molecular prediction of durable remission after first-line fludarabine-cyclophosphamide-rituximab in chronic lymphocytic leukemia. Blood 2015, 126, 1921–1924. [Google Scholar] [CrossRef]
- Fischer, K.; Bahlo, J.; Fink, A.M.; Goede, V.; Herling, C.D.; Cramer, P.; Langerbeins, P.; von Tresckow, J.; Engelke, A.; Maurer, C.; et al. Long-term remissions after FCR chemoimmunotherapy in previously untreated patients with CLL: Updated results of the CLL8 trial. Blood 2016, 127, 208–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Döhner, H.; Stilgenbauer, S.; Benner, A.; Leupolt, E.; Kröber, A.; Bullinger, L.; Döhner, K.; Bentz, M.; Lichter, P. Genomic Aberrations and Survival in Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2000, 343, 1910–1916. [Google Scholar] [CrossRef] [Green Version]
- Campo, E.; Cymbalista, F.; Ghia, P.; Jäger, U.; Pospisilova, S.; Rosenquist, R.; Schuh, A.; Stilgenbauer, S. TP53 aberrations in chronic lymphocytic leukemia: An overview of the clinical implications of improved diagnostics. Haematologica 2018, 103, 1956–1968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zenz, T.; Vollmer, D.; Trbusek, M.; Smardova, J.; Benner, A.; Soussi, T.; Helfrich, H.; Heuberger, M.; Hoth, P.; Fuge, M.; et al. TP53 mutation profile in chronic lymphocytic leukemia: Evidence for a disease specific profile from a comprehensive analysis of 268 mutations. Leukemia 2010, 24, 2072–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seiffert, M.; Dietrich, S.; Jethwa, A.; Glimm, H.; Lichter, P.; Zenz, T. Exploiting biological diversity and genomic aberrations in chronic lymphocytic leukemia. Leuk. Lymphoma 2011, 53, 1023–1031. [Google Scholar] [CrossRef] [PubMed]
- Wierda, W.G.; O’Brien, S.; Wang, X.; Faderl, S.; Ferrajoli, A.; Do, K.-A.; Cortes, J.; Thomas, D.; Garcia-Manero, G.; Koller, C.; et al. Prognostic nomogram and index for overall survival in previously untreated patients with chronic lymphocytic leukemia. Blood 2007, 109, 4679–4685. [Google Scholar] [CrossRef]
- Pflug, N.; Bahlo, J.; Shanafelt, T.D.; Eichhorst, B.F.; Bergmann, M.A.; Elter, T.; Bauer, K.; Malchau, G.; Rabe, K.G.; Stilgenbauer, S.; et al. Development of a comprehensive prognostic index for patients with chronic lymphocytic leukemia. Blood 2014, 124, 49–62. [Google Scholar] [CrossRef]
- International CLL-IPI working group. An international prognostic index for patients with chronic lymphocytic leukaemia (CLL-IPI): A meta-analysis of individual patient data. Lancet Oncol. 2016, 17, 779–790. [Google Scholar] [CrossRef]
- Condoluci, A.; Di Bergamo, L.T.; Langerbeins, P.; Hoechstetter, M.A.; Herling, C.D.; De Paoli, L.; Delgado, J.; Rabe, K.G.; Gentile, M.; Doubek, M.; et al. International prognostic score for asymptomatic early-stage chronic lymphocytic leukemia. Blood 2020, 135, 1859–1869. [Google Scholar] [CrossRef]
- Cohen, J.A.; Rossi, F.M.; Zucchetto, A.; Bomben, R.; Terzi-Di-Bergamo, L.; Rabe, K.G.; Degan, M.; Steffan, A.; Polesel, J.; Santinelli, E.; et al. A laboratory-based scoring system predicts early treatment in Rai 0 chronic lymphocytic leukemia. Haematologica 2019, 105, 1613–1620. [Google Scholar] [CrossRef] [Green Version]
- Malcikova, J.; Tausch, E.; Rossi, D.; Sutton, L.A.; Soussi, T.; Zenz, T.; Kater, A.P.; Niemann, C.U.; Gonzalez, D.; Davi, F.; et al. ERIC recommendations for TP53 mutation analysis in chronic lymphocytic leukemia—Update on methodological approaches and results interpretation. Leukemia 2018, 32, 1070–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenquist, R.; Ghia, P.; Hadzidimitriou, A.; Sutton, L.-A.; Agathangelidis, A.; Baliakas, P.; Darzentas, N.; Giudicelli, V.; Lefranc, M.-P.; Langerak, A.W.; et al. Immunoglobulin gene sequence analysis in chronic lymphocytic leukemia: Updated ERIC recommendations. Leukemia 2017, 31, 1477–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wierda, W.G.; O’Brien, S.; Wang, X.; Faderl, S.; Ferrajoli, A.; Do, K.-A.; Garcia-Manero, G.; Cortes, J.; Thomas, D.; Koller, C.A.; et al. Multivariable Model for Time to First Treatment in Patients With Chronic Lymphocytic Leukemia. J. Clin. Oncol. 2011, 29, 4088–4095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentile, M.; Cutrona, G.; Neri, A.; Molica, S.; Ferrarini, M.; Morabito, F. Predictive value of beta2-microglobulin (beta2-m) levels in chronic lymphocytic leukemia since Binet A stages. Haematologica 2009, 94, 887–888. [Google Scholar] [CrossRef]
- Chiorazzi, N.; Rai, K.R.; Ferrarini, M. Chronic lymphocytic leukemia. N. Engl. J. Med. 2005, 352, 804–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCCN Guidelines Version 3.2022. Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. Available online: https://www.nccn.org/guidelines (accessed on 3 June 2022).
- Eichhorst, B.; Robak, T.; Montserrat, E.; Ghia, P.; Niemann, C.; Kater, A.; Gregor, M.; Cymbalista, F.; Buske, C.; Hillmen, P.; et al. Chronic lymphocytic leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 32, 23–33. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | OS | TTFT | ||||||
|---|---|---|---|---|---|---|---|---|
| n | p-Value | HR | 95% CI | p-Value | HR | 95% CI | ||
| Whole series | β2-microglobulin (mg/L) | 167 | 0.729 | 0.73 | 0.12–4.30 | 0.421 | 1.75 | 0.45–6.89 |
| IGHV unmutated | 109 | 0.01 | 6.16 | 1.56–24.37 | 0.001 | 13.58 | 2.91–63.29 | |
| Age > 65 years | 217 | 0.072 | 3.57 | 0.89–14.31 | ||||
| Rai 3–4 | 217 | 0.033 | 27.22 | 1.30–572.00 | 0.081 | 9.67 | 0.76–123.70 | |
| Rai 0–2 | β2-microglobulin (mg/L) | 157 | 0.72 | 0.72 | 0.12–4.26 | 0.42 | 1.75 | 0.45–6.89 |
| IGHV unmutated | 96 | 0.01 | 6.16 | 1.56–24.41 | 0.001 | 13.58 | 2.91–63.29 | |
| Age > 65 years | 204 | 0.073 | 3.57 | 0.89–14.32 | ||||
| Binet A | β2-microglobulin (mg/L) | 137 | 0.912 | 1.069 | 0.24–5.03 | 0.219 | 2.19 | 0.63–7.62 |
| IGHV unmutated | 77 | 0.009 | 5.96 | 1.56–22.72 | 0.001 | 14.08 | 3.04–65.28 | |
| Age > 65 years | 176 | 0.066 | 3.59 | 0.92–14.01 | ||||
| Variable | n | N (%) | p-Value | N (%) | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| Rai 0–2 | Rai 3–4 | Binet A | Binet B-C | |||||
| β2-microglobulin (mg/L) | ≤3.5 | 150 | 130 (95.6) | 6 (4.4) | <0.001 | 117 (8.4) | 20 (14.6) | 0.147 |
| >3.5 | 20 (74.1) | 7 (25.9) | 20 (74.1) | 7(25.9) | ||||
| Trisomy 12 | No | 123 | 101 (91) | 10 (9) | 0.155 | 90 (81.1) | 21 (18.9) | 0.005 |
| Yes | 22 (81.5) | 5 (18.5) | 15 (55.6) | 12 (44.4) | ||||
| Del(11q) | No | 122 | 116 (89.9) | 13 (10.1) | 0.19 | 100 (77.5) | 29 (22.5) | 0.077 |
| Yes | 6 (75) | 2 (25) | 4 (50) | 4 (50) | ||||
| Del(17p)/TP53 mutation | No | 123 | 112 (88.9) | 14 (11.1) | 0.768 | 96 (76.2) | 30 (23.8) | 0.926 |
| Yes | 11 (91.7) | 1 (8.3) | 9 (75) | 3 (25) | ||||
| IGHV mutated | No | 90 | 58 (93.5) | 4(6.5) | 0.071 | 53 (84.1) | 10 (15.9) | 0.01 |
| Yes | 32 (82.1) | 7 (17.9) | 24 (61.5) | 15 (38.5) | ||||
| Age | ≤65 years | 192 | 73 (91.3) | 7 (8.8) | 0.397 | 59 (73.8) | 21 (26.3) | 0.069 |
| Rai 0–2 | Binet A | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | n | HR | p-Value | 95% CI | n | HR | p-Value | 95% CI |
| Lymphocytes ≥ 15 × 109/L | 79 | 1.62 | 0.384 | 0.55–4.84 | 67 | 1.85 | 0.40 | 0.45–7.80 |
| IGHV unmutated | 79 | 8.05 | 0.002 | 2.10–30.87 | 67 | 8.05 | 0.013 | 1.54–42.10 |
| Nodal involvement | 79 | 6.61 | 0.002 | 2.06–21.52 | 67 | 4.85 | 0.028 | 1.18–19.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suárez-Cabrera, A.; Fiallo-Suárez, D.V.; Stuckey, R.; Uroz-de la Iglesia, M.L.; Florido, Y.; Lemes-Castellano, A.; Perera-Álvarez, M.Á.; Luzardo-Henríquez, H.; de la Nuez, H.; Fernández-Caldas, P.; et al. Genetic Testing at Diagnosis Has Prognostic Value in Patients with Chronic Lymphocytic Leukemia including at Early Stages. Diagnostics 2022, 12, 1802. https://doi.org/10.3390/diagnostics12081802
Suárez-Cabrera A, Fiallo-Suárez DV, Stuckey R, Uroz-de la Iglesia ML, Florido Y, Lemes-Castellano A, Perera-Álvarez MÁ, Luzardo-Henríquez H, de la Nuez H, Fernández-Caldas P, et al. Genetic Testing at Diagnosis Has Prognostic Value in Patients with Chronic Lymphocytic Leukemia including at Early Stages. Diagnostics. 2022; 12(8):1802. https://doi.org/10.3390/diagnostics12081802
Chicago/Turabian StyleSuárez-Cabrera, Alexia, Dolly Viviana Fiallo-Suárez, Ruth Stuckey, Marta Luna Uroz-de la Iglesia, Yanira Florido, Angelina Lemes-Castellano, Miguel Ángel Perera-Álvarez, Hugo Luzardo-Henríquez, Haridian de la Nuez, Paula Fernández-Caldas, and et al. 2022. "Genetic Testing at Diagnosis Has Prognostic Value in Patients with Chronic Lymphocytic Leukemia including at Early Stages" Diagnostics 12, no. 8: 1802. https://doi.org/10.3390/diagnostics12081802
APA StyleSuárez-Cabrera, A., Fiallo-Suárez, D. V., Stuckey, R., Uroz-de la Iglesia, M. L., Florido, Y., Lemes-Castellano, A., Perera-Álvarez, M. Á., Luzardo-Henríquez, H., de la Nuez, H., Fernández-Caldas, P., de la Iglesia, S., Gómez-Casares, M. T., & Bilbao-Sieyro, C. (2022). Genetic Testing at Diagnosis Has Prognostic Value in Patients with Chronic Lymphocytic Leukemia including at Early Stages. Diagnostics, 12(8), 1802. https://doi.org/10.3390/diagnostics12081802