
Episodic Memory in Amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease Dementia (ADD): Using the “Doors and People” Tool to Differentiate between Early aMCI—Late aMCI—Mild ADD Diagnostic Groups

 ,
,  ,
,  , ,
, ,  ,
, 
 and
and
Abstract
:1. Introduction
1.1. Amnestic Mild Cognitive Impairment and Alzheimer’s Disease Dementia
1.2. Episodic Memory
1.3. The Role of Episodic Memory in the Diagnosis of ADD
1.4. Measures of Episodic Memory—The Doors and People Tool
1.5. Aim and Hypotheses of the Study
2. Methods
2.1. Participants
2.2. Procedure
2.3. Ethics
2.4. Measure
2.5. Statistics
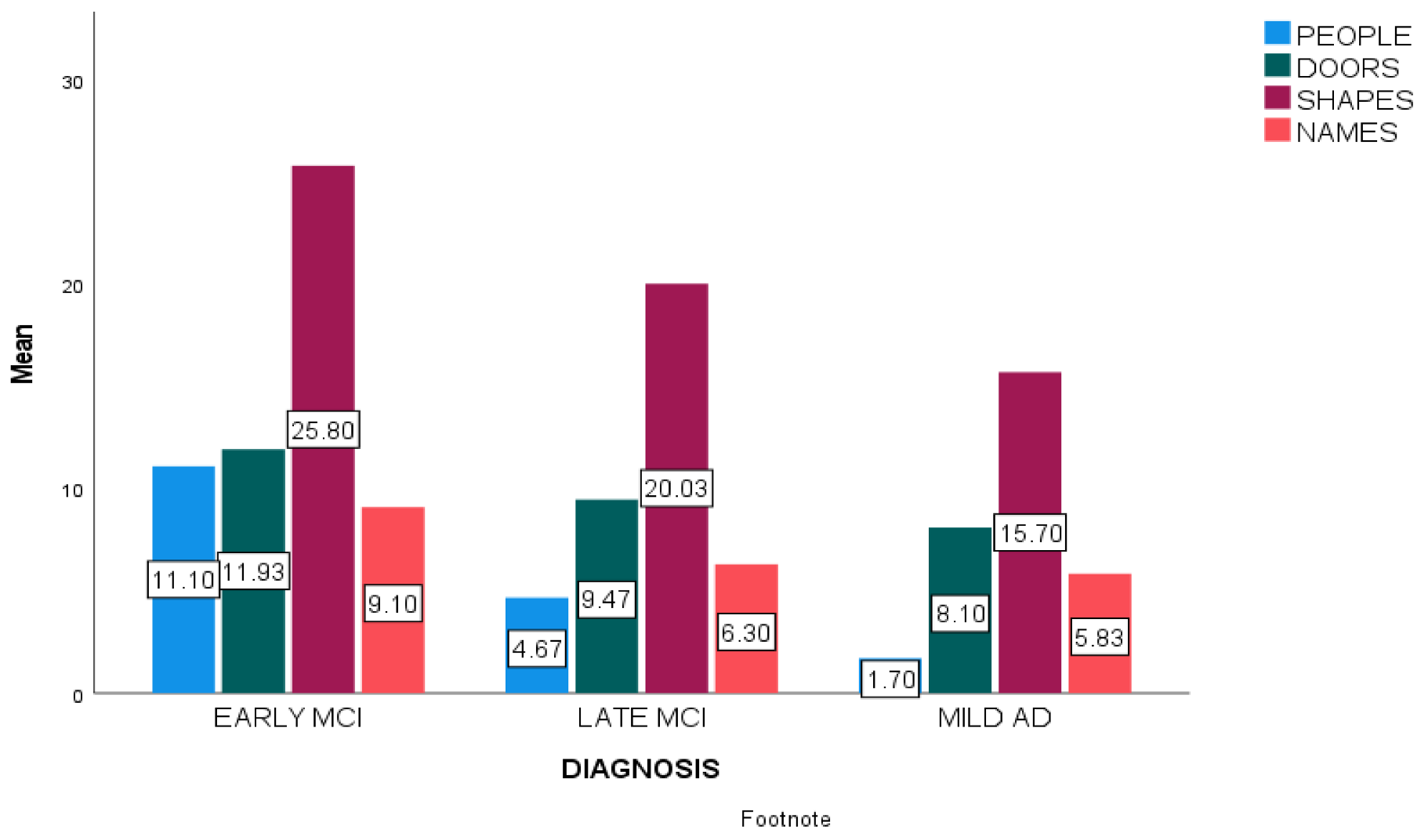
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association, Washington American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA; Washington American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Vermunt, L.; Sikkes, S.A.; Van Den Hout, A.; Handels, R.; Bos, I.; Van Der Flier, W.M.; Kern, S.; Ousset, P.J.; Maruff, P.; Skoog, I.; et al. Duration of preclinical, prodromal, and dementia stages of Alzheimer’s disease in relation to age, sex, and APOE genotype. Alzheimer’s Dement. 2019, 15, 888–898. [Google Scholar] [CrossRef] [PubMed]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.O.; Petersen, R.C.; Nordberg, A.; Bäckman, L.; Albert, M.; et al. Mild cognitive impairment—Beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, E.C.; McDonald, C.R.; Marshall, A.; Thomas, K.R.; Eppig, J.; Weigand, A.J.; Delano-Wood, L.; Galasko, D.R.; Salmon, D.P.; Alzheimer’s Disease Neuroimaging Initiative; et al. Early versus late MCI: Improved MCI staging using a neuropsychological approach. Alzheimer’s Dement. 2019, 15, 699–708. [Google Scholar] [CrossRef]
- Tulving, E. Episodic Memory: From Mind to Brain. Annu. Rev. Psychol. 2002, 53, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Irish, M.; A Lawlor, B.; Coen, R.F.; O’Mara, S.M. Everyday episodic memory in amnestic mild cognitive impairment: A preliminary investigation. BMC Neurosci. 2011, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Pennanen, C.; Kivipelto, M.; Tuomainen, S.; Hartikainen, P.; Hänninen, T.; Laakso, M.P.; Hallikainen, M.; Vanhanen, M.; Nissinen, A.; Soininen, H.; et al. Hippocampus and entorhinal cortex in mild cognitive impairment and early AD. Neurobiol. Aging 2004, 25, 303–310. [Google Scholar] [CrossRef]
- Moffat, S.D.; Resnick, S.M. Effects of age on virtual environment place navigation and allocentric cognitive mapping. Behav. Neurosci. 2002, 116, 851. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, B.C.; Eichenbaum, H. The episodic memory system: Neurocircuitry and disorders. Neuropsychopharmacology 2010, 35, 86–104. [Google Scholar] [CrossRef]
- Moscovitch, M.; Cabeza, R.; Winocur, G.; Nadel, L. Episodic Memory and Beyond: The Hippocampus and Neocortex in Transformation. Annu. Rev. Psychol. 2016, 67, 105–134. [Google Scholar] [CrossRef] [Green Version]
- Geib, B.R.; Stanley, M.L.; Dennis, N.A.; Woldorff, M.; Cabeza, R. From hippocampus to whole-brain: The role of integrative processing in episodic memory retrieval. Hum. Brain Mapp. 2017, 38, 2242–2259. [Google Scholar] [CrossRef] [Green Version]
- Bai, F.; Zhang, Z.; Watson, D.R.; Yu, H.; Shi, Y.; Yuan, Y.; Zang, Y.; Zhu, C.; Qian, Y. Abnormal functional connectivity of hippocampus during episodic memory retrieval processing network in amnestic mild cognitive impairment. Biol. Psychiatry 2009, 65, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Nellessen, N.; Rottschy, C.; Eickhoff, S.B.; Ketteler, S.T.; Kuhn, H.; Shah, N.J.; Schulz, J.B.; Reske, M.; Reetz, K. Specific and disease stage-dependent episodic memory-related brain activation patterns in Alzheimer’s disease: A coordinate-based meta-analysis. Brain Struct. Funct. 2015, 220, 1555–1571. [Google Scholar] [CrossRef] [PubMed]
- Economou, A.; Routsis, C.; Papageorgiou, S.G. Episodic Memory in Alzheimer Disease, Frontotemporal Dementia, and Dementia with Lewy Bodies/Parkinson Disease Dementia. Alzheimer Dis. Assoc. Disord. 2016, 30, 47–52. [Google Scholar] [CrossRef]
- Aslaksen, P.M.; Bystad, M.K.; Ørbo, M.C.; Vangberg, T.R. The relation of hippocampal subfield volumes to verbal episodic memory measured by the California Verbal Learning Test II in healthy adults. Behav. Brain Res. 2018, 351, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolk, D.A.; Dickerson, B.C.; Alzheimer’s Disease Neuroimaging Initiative. Fractionating verbal episodic memory in Alzheimer’s disease. Neuroimage 2011, 54, 1530–1539. [Google Scholar] [CrossRef] [Green Version]
- Juncos-Rabadán, O.; Pereiro, A.X.; Facal, D.; Reboredo, A.; Lojo-Seoane, C. Do the Cambridge Neuropsychological Test Automated Battery episodic memory measures discriminate amnestic mild cognitive impairment? Int. J. Geriatr. Psychiatry 2014, 29, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Robinson, A.C.; McNamee, R.; Davidson, Y.S.; Horan, M.A.; Snowden, J.S.; McInnes, L.; Pendleton, N.; Mann, D.M. Scores obtained from a simple cognitive test of visuospatial episodic memory performed decades before death are associated with the ultimate presence of Alzheimer disease pathology. Dement. Geriatr. Cogn. Disord. 2018, 45, 79–90. [Google Scholar] [CrossRef]
- Quaranta, D.; Gainotti, G.; Di Giuda, D.; Vita, M.G.; Cocciolillo, F.; Lacidogna, G.; Guglielmi, V.; Masullo, C.; Giordano, A.; Marra, C. Predicting progression of amnestic MCI: The integration of episodic memory impairment with perfusion SPECT. Psychiatry Res. Neuroimaging 2018, 271, 43–49. [Google Scholar] [CrossRef]
- Dias, B.F.; Bicalho, M.A.C.; Costa, M.V.; de Ávila, R.T.; Malloy-Diniz, L.F.; Romano-Silva, M.A.; de Paula, J.J. Episodic memory in normal and pathological aging at the RAVLT Test: Comparisons of immediate and delayed recall. Psychol. Neurosci. 2021, 14, 388. [Google Scholar] [CrossRef]
- Moscoso, A.; Silva-Rodriguez, J.; Aldrey, J.M.; Cortes, J.; Fernandez-Ferreiro, A.; Gomez-Lado, N.; Ruibal, A.; Aguiar, P.; Alzheimer’s Disease Neuroimaging Initiative. Staging the cognitive continuum in prodromal Alzheimer’s disease with episodic memory. Neurobiol. Aging 2019, 84, 1–8. [Google Scholar] [CrossRef]
- Nakhla, M.Z.; Banuelos, D.; Pagán, C.; Olvera, A.G.; Razani, J. Differences between episodic and semantic memory in predicting observation-based activities of daily living in mild cognitive impairment and Alzheimer’s disease. Appl. Neuropsychol. Adult 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Berna, F.; Schönknecht, P.; Seidl, U.; Toro, P.; Schröder, J. Episodic autobiographical memory in normal aging and mild cognitive impairment: A population-based study. Psychiatry Res. 2012, 200, 807–812. [Google Scholar] [CrossRef]
- Tromp, D.; Dufour, A.; Lithfous, S.; Pebayle, T.; Després, O. Episodic memory in normal aging and Alzheimer disease: Insights from imaging and behavioral studies. Ageing Res. Rev. 2015, 24, 232–262. [Google Scholar] [CrossRef] [PubMed]
- Yonelinas, A.P.; Ranganath, C.; Ekstrom, A.D.; Wiltgen, B.J. A contextual binding theory of episodic memory: Systems consolidation reconsidered. Nat. Rev. Neurosci. 2019, 20, 364–375. [Google Scholar] [CrossRef] [PubMed]
- Baddeley, A.D. The psychology of memory. In The Essential Handbook of Memory Disorders for Clinicians; Baddeley, A.D., Kopelman, M.D., Wilson, B.A., Eds.; John Wiley & Sons Ltd.: Oxford, UK, 2004; pp. 1–13. [Google Scholar]
- Chaytor, N.; Schmitter-Edgecombe, M. The ecological validity of neuropsychological tests: A review of the literature on everyday cognitive skills. Neuropsychol. Rev. 2003, 13, 181–197. [Google Scholar] [CrossRef]
- Baddeley, A.D.; Emslie, H.; Nimmo-Smith, I. The Doors and People Test: A Test of visual and Verbal Recall and Recognition; Thames Valley Test Company: Bury St Edmunds, UK, 1994. [Google Scholar]
- Hess, R.S.; D’Amato, R.C. Book Review: Doors and People: A Test of Visual and Verbal Recall and Recognition. J. Psychoeduc. Assess. 1999, 17, 175–180. [Google Scholar] [CrossRef]
- Arabatzi, X.; Masoura, E. Episodic Memory and Norms’ Development for the Battery “Doors and People” in the Greek Population; No. GRI-2021-9114; Aristotle University of Thessaloniki: Thessaloniki, Greece, 2012; Unpublished Dissertation. [Google Scholar]
- Morris, R.G.; Abrahams, S.; Baddeley, A.D.; Polkey, C.E. Doors and People: Visual and verbal memory after unilateral temporal lobectomy. Neuropsychology 1995, 9, 464. [Google Scholar] [CrossRef]
- MacPherson, S.E.; Turner, M.S.; Bozzali, M.; Cipolotti, L.; Shallice, T. The Doors and People Test: The effect of frontal lobe lesions on recall and recognition memory performance. Neuropsychology 2016, 30, 332–337. [Google Scholar] [CrossRef]
- Prokasheva, S.; Faran, Y.; Cwikel, J.; Geffen, D.B. Analysis of Memory Deficits Following Chemotherapy in Breast Cancer Survivors: Evidence from the Doors and People Test. J. Psychosoc. Oncol. 2011, 29, 499–514. [Google Scholar] [CrossRef]
- Barbeau, E.J.; Pariente, J.; Felician, O.; Puel, M. Visual recognition memory: A double anatomo-functional dissociation. Hippocampus 2010, 21, 929–934. [Google Scholar] [CrossRef]
- Nestor, P.J.; Fryer, T.D.; Smielewski, P.; Hodges, J.R. Limbic hypometabolism in Alzheimer’s disease and mild cognitive impairment. Ann. Neurol. 2003, 54, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.D.; Baddeley, A.D.; Hodges, J.R. Analysis of the episodic memory deficit in early Alzheimer’s disease: Evidence from the doors and people test. Neuropsychologia 1996, 34, 537–551. [Google Scholar] [CrossRef]
- Fitzsimmons, J.; Kubicki, M.; Smith, K.; Bushell, G.; Estepar, R.S.J.; Westin, C.F.; Nestor, P.G.; Niznikiewicz, M.A.; Kikinis, R.; Shenton, M.E. Diffusion tractography of the fornix in schizophrenia. Schizophr. Res. 2009, 107, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramoni, E.; Felician, O.; Barbeau, E.J.; Guedj, E.; Guye, M.; Bartolomei, F.; Ceccaldi, M. Long-term consolidation of declarative memory: Insight from temporal lobe epilepsy. Brain 2011, 134, 816–831. [Google Scholar] [CrossRef] [PubMed]
- Towgood, K.J.; Meuwese, J.D.; Gilbert, S.J.; Turner, M.S.; Burgess, P.W. Advantages of the multiple case series approach to the study of cognitive deficits in autism spectrum disorder. Neuropsychologia 2009, 47, 2981–2988. [Google Scholar] [CrossRef] [Green Version]
- Ambery, F.Z.; Russell, A.J.; Perry, K.; Morris, R.; Murphy, D.G. Neuropsychological functioning in adults with Asperger syndrome. Autism 2006, 10, 551–564. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Tsolaki, M.; Chantzi, H.; Kazis, A. Mini mental state examination (MMSE): A validation study in Greece. Am. J. Alzheimer’s Dis. Other Dement. 2000, 15, 342–345. [Google Scholar] [CrossRef]
- Konstantopoulos, K.; Vogazianos, P.; Doskas, T. Normative data of the Montreal Cognitive Assessment in the Greek population and parkinsonian dementia. Arch. Clin. Neuropsychol. 2016, 31, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Zalonis, I.; Kararizou, E.; Triantafyllou, N.; Kapaki, E.; Papageorgiou, S.; Sgouropoulos, P.E.E.A.; Vassilopoulos, D. A Normative Study of the Trail Making Test A and B in Greek Adults. Clin. Neuropsychol. 2008, 22, 842–850. [Google Scholar] [CrossRef]
- Messinis, L.; Tsakona, I.; Malefaki, S.; Papathanasopoulos, P. Normative data and discriminant validity of Rey’s Verbal Learning Test for the Greek adult population. Arch. Clin. Neuropsychol. 2007, 22, 739–752. [Google Scholar] [CrossRef] [Green Version]
- Efklides, A.; Yiultsi, E.; Kangellidou, T.; Kounti, F.; Dina, F.; Tsolaki, M. Wechsler Memory Scale, Rivermead Behavioral Memory Test, and Everyday Memory Questionnaire in healthy adults and Alzheimer’s patients. Eur. J. Psychol. Assess. 2002, 18, 63. [Google Scholar] [CrossRef]
- Kounti, F.; Tsolaki, M.; Kiosseoglou, G. Functional cognitive assessment scale (FUCAS): A new scale to assess executive cognitive function in daily life activities in patients with dementia and mild cognitive impairment. Hum. Psychopharmacol. Clin. Exp. 2006, 21, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Tsatali, M.; Emmanouel, A.; Gialaouzidis, M.; Avdikou, K.; Stefanatos, C.; Diamantidou, A.; Kouroundi, E.; Messini, C.; Tsolaki, M. Rey Complex Figure Test (RCFT): Norms for the Greek older adult population. Appl. Neuropsychol. Adult 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kosmidis, M.H.; Vlahou, C.H.; Panagiotaki, P.; Kiosseoglou, G. The verbal fluency task in the Greek population: Normative data, and clustering and switching strategies. J. Int. Neuropsychol. Soc. 2004, 10, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Tsolaki, M.; Fountoulakis, K.; Nakopoulou, E.; Kazis, A.; Mohs, R.C. Alzheimer’s Disease Assessment Scale: The validation of the scale in Greece in elderly demented patients and normal subjects. Dement. Geriatr. Cogn. Disord. 1997, 8, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Fountoulakis, K.N.; Tsolaki, M.; Iacovides, A.; Yesavage, J.; O’Hara, R.; Kazis, A.; Ierodiakonou, C. The validation of the short form of the Geriatric Depression Scale (GDS) in Greece. Aging Clin. Exp. Res. 1999, 11, 367–372. [Google Scholar] [CrossRef]
- Grammatikopoulos, I.A.; Sinoff, G.; Alegakis, A.; Kounalakis, D.; Antonopoulou, M.; Lionis, C. The Short Anxiety Screening Test in Greek: Translation and validation. Ann. Gen. Psychiatry 2010, 9, 1. [Google Scholar] [CrossRef] [Green Version]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.; Ryoo, H.; Park, J.; Jeong, Y. Morphological and microstructural changes of the hippocampus in early MCI: A study utilizing the Alzheimer’s disease neuroimaging initiative database. J. Clin. Neurol. 2017, 13, 144–154. [Google Scholar] [CrossRef] [Green Version]
- Kang, D.W.; Lim, H.K.; Joo, S.H.; Lee, N.R.; Lee, C.U. Differential associations between volumes of atrophic cortical brain regions and memory performances in early and late mild cognitive impairment. Front. Aging Neurosci. 2019, 11, 245. [Google Scholar] [CrossRef] [Green Version]
- Perri, R.; Serra, L.; Carlesimo, G.A.; Caltagirone, C. Amnestic mild cognitive impairment: Difference of memory profile in subjects who converted or did not convert to Alzheimer’s disease. Neuropsychology 2007, 21, 549. [Google Scholar] [CrossRef] [PubMed]
- Boraxbekk, C.-J.; Lundquist, A.; Nordin, A.; Nyberg, L.; Nilsson, L.-G.; Adolfsson, R. Free Recall Episodic Memory Performance Predicts Dementia Ten Years prior to Clinical Diagnosis: Findings from the Betula Longitudinal Study. Dement. Geriatr. Cogn. Disord. Extra 2015, 5, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Bozzali, M.; Filippi, M.; Magnani, G.; Cercignani, M.; Franceschi, M.; Schiatti, E.; Castiglioni, S.; Mossini, R.; Falautano, M.; Scotti, G.; et al. The contribution of voxel-based morphometry in staging patients with mild cognitive impairment. Neurology 2006, 67, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Warren, S.L.; Moustafa, A.A.; Alashwal, H. Harnessing forgetfulness: Can episodic-memory tests predict early Alzheimer’s disease? Exp. Brain Res. 2021, 239, 2925–2937. [Google Scholar] [CrossRef] [PubMed]
- Fleisher, A.S.; Sowell, B.B.; Taylor, C.; Gamst, A.C.; Petersen, R.C.; Thal, L.J. Clinical predictors of progression to Alzheimer disease in amnestic mild cognitive impairment. Neurology 2007, 68, 1588–1595. [Google Scholar] [CrossRef] [PubMed]
- De Simone, M.S.; Perri, R.; Fadda, L.; Caltagirone, C.; Carlesimo, G.A. Predicting progression to Alzheimer’s disease in subjects with amnestic mild cognitive impairment using performance on recall and recognition tests. J. Neurol. 2019, 266, 102–111. [Google Scholar] [CrossRef]
- Marra, C.; Gainotti, G.; Fadda, L.; Perri, R.; Lacidogna, G.; Scaricamazza, E.; Quaranta, D. Usefulness of an integrated analysis of different memory tasks to predict the progression from mild cognitive impairment to Alzheimer’s disease: The episodic memory score (EMS). J. Alzheimer’s Dis. 2016, 50, 61–70. [Google Scholar] [CrossRef]
- Chételat, G.; Landeau, B.; Eustache, F.; Mézenge, F.; Viader, F.; de La Sayette, V.; Baron, J.C. Using voxel-based morphometry to map the structural changes associated with rapid conversion in MCI: A longitudinal MRI study. Neuroimage 2005, 27, 934–946. [Google Scholar] [CrossRef]
- Leube, D.T.; Weis, S.; Freymann, K.; Erb, M.; Jessen, F.; Heun, R.; Kircher, T.T. Neural correlates of verbal episodic memory in patients with MCI and Alzheimer’s disease–a VBM study. Int. J. Geriatr. Psychiatry 2008, 23, 1114–1118. [Google Scholar] [CrossRef]
- Chang, Y.L.; Bondi, M.W.; Fennema-Notestine, C.; McEvoy, L.K.; Hagler, D.J., Jr.; Jacobson, M.W.; Dale, A.M.; Alzheimer’s Disease Neuroimaging Initiative. Brain substrates of learning and retention in mild cognitive impairment diagnosis and progression to Alzheimer’s disease. Neuropsychologia 2010, 48, 1237–1247. [Google Scholar] [CrossRef] [Green Version]
- Gomar, J.J.; Bobes-Bascaran, M.T.; Conejero-Goldberg, C.; Davies, P.; Goldberg, T.E. Utility of combinations of biomarkers, cognitive markers, and risk factors to predict conversion from mild cognitive impairment to Alzheimer disease in patients in the Alzheimer’s disease neuroimaging initiative. Arch. Gen. Psychiatry 2011, 68, 961–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathan, P.J.; Abbott, R.; Lim, Y.Y.; Galluzzi, S.; Marizzoni, M.; Bagnoli, C.; Frisoni, G. PT593. CSF Beta-Amyloid and APOE E4 Related Decline in Episodic Memory over 12 months measured using the CANTAB in individuals with amnestic MCI: Results from the European-ADNI study. Int. J. Neuropsychopharmacol. 2016, 19, 18–19. [Google Scholar]
- Eckerström, C.; Olsson, E.; Bjerke, M.; Malmgren, H.; Edman, Å.; Wallin, A.; Nordlund, A. A combination of neuropsychological, neuroimaging, and cerebrospinal fluid markers predicts conversion from mild cognitive impairment to dementia. J. Alzheimer’s Dis. 2013, 36, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Prull, M.W.; Gabrieli, J.D.E.; Bunge, S.A. Age-related changes in memory: A cognitive neuroscience perspective. In the Handbook of Aging and Cognition; Craik, F.I.M., Salthouse, T.A., Eds.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2000; pp. 91–153. [Google Scholar]
- Guerreiro, R.; Bras, J. The age factor in Alzheimer’s disease. Genome Med. 2015, 7, 106. [Google Scholar] [CrossRef] [Green Version]
- DeTure, M.; Dickson, D. The neuropathological diagnosis of Alzheimer’s disease. Mol. Neurodegener. 2019, 14, 32. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Age | Education | ||||
|---|---|---|---|---|---|---|
| % Male | % Female | M | SD | M | SD | |
| Early aMCI | 46.66 | 53.34 | 71.87 | 5.002 | 10.57 | 3.785 |
| Late aMCI | 50 | 50 | 78.93 | 3.073 | 8.53 | 2.763 |
| Mild ADD | 46.66 | 53.34 | 80.40 | 2.978 | 9.33 | 3.055 |
| Value | F | Df | p | |
|---|---|---|---|---|
| Age-group | 0.954 | 0.970 | 4 | 0.428 |
| Diagnostic group | 0.703 | 3.907 | 8 | <0.001 ** |
| Age-group × Diagnostic group | 0.887 | 1.254 | 8 | 0.271 |
| F | Df | p | Partial n2 | |
|---|---|---|---|---|
| People | 12.616 | 2 | <0.001 ** | 0.231 |
| Doors | 5.694 | 2 | 0.005 ** | 0.119 |
| Shapes | 9.323 | 2 | <0.001 ** | 0.182 |
| Names | 4.834 | 2 | 0.010 * | 0.103 |
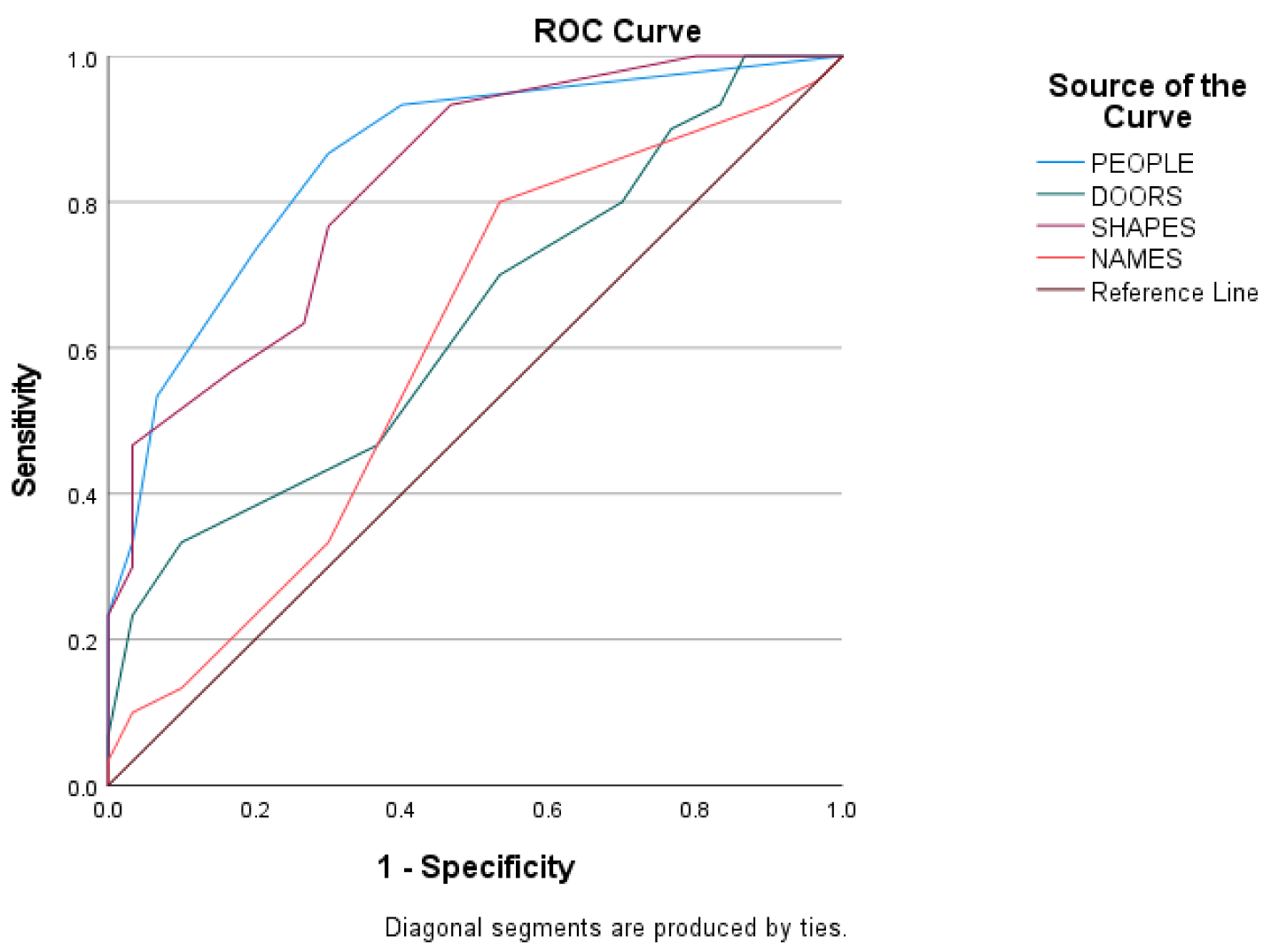
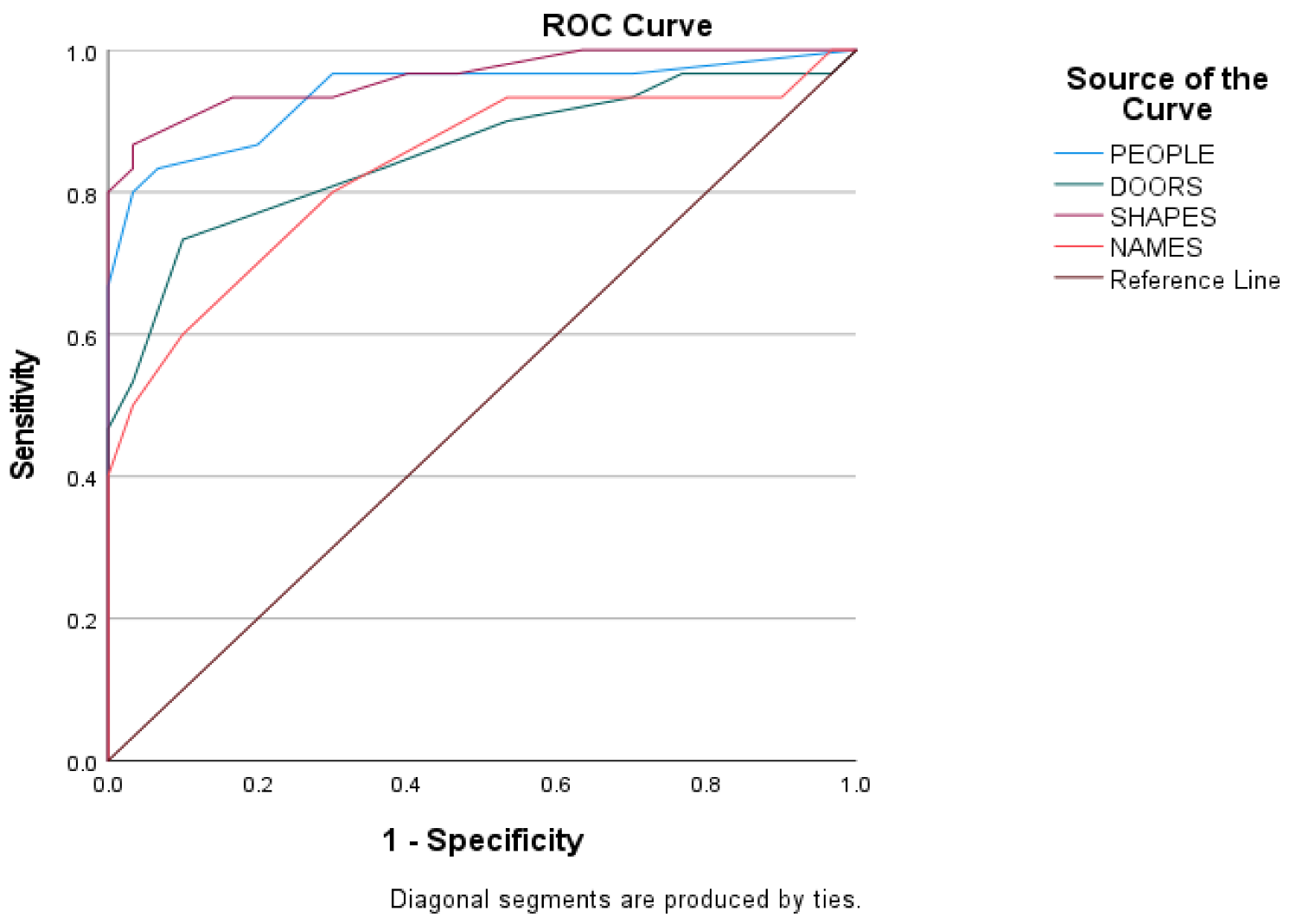
| Cut-Offs | Sensitivity % | Specificity % | p | ||
|---|---|---|---|---|---|
| Early MCI-Late MCI | People | 5.5 | 80 | 66.7 | <0.01 ** |
| Doors | 10.5 | 73.3 | 77.7 | <0.01 ** | |
| Shapes | 21.5 | 83.3 | 70 | <0.01 ** | |
| Names | 6.5 | 80 | 66.7 | <0.01 ** | |
| Late MCI-Mild AD | People | 2.5 | 86.7 | 70 | <0.01 ** |
| Doors | _ | _ | _ | ||
| Shapes | 17.5 | 76.7 | 70 | <0.01 ** | |
| Names | _ | _ | _ | ||
| Early MCI-Mild AD | People | 4.5 | 83.3 | 93.3 | <0.01 ** |
| Doors | 9.5 | 83.3 | 63.3 | <0.01 ** | |
| Shapes | 19.5 | 93.3 | 83.3 | <0.01 ** | |
| Names | 6.5 | 80 | 70 | <0.01 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatzikostopoulos, A.; Moraitou, D.; Tsolaki, M.; Masoura, E.; Papantoniou, G.; Sofologi, M.; Papaliagkas, V.; Kougioumtzis, G.; Papatzikis, E. Episodic Memory in Amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease Dementia (ADD): Using the “Doors and People” Tool to Differentiate between Early aMCI—Late aMCI—Mild ADD Diagnostic Groups. Diagnostics 2022, 12, 1768. https://doi.org/10.3390/diagnostics12071768
Chatzikostopoulos A, Moraitou D, Tsolaki M, Masoura E, Papantoniou G, Sofologi M, Papaliagkas V, Kougioumtzis G, Papatzikis E. Episodic Memory in Amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease Dementia (ADD): Using the “Doors and People” Tool to Differentiate between Early aMCI—Late aMCI—Mild ADD Diagnostic Groups. Diagnostics. 2022; 12(7):1768. https://doi.org/10.3390/diagnostics12071768
Chicago/Turabian StyleChatzikostopoulos, Athanasios, Despina Moraitou, Magdalini Tsolaki, Elvira Masoura, Georgia Papantoniou, Maria Sofologi, Vasileios Papaliagkas, Georgios Kougioumtzis, and Efthymios Papatzikis. 2022. "Episodic Memory in Amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease Dementia (ADD): Using the “Doors and People” Tool to Differentiate between Early aMCI—Late aMCI—Mild ADD Diagnostic Groups" Diagnostics 12, no. 7: 1768. https://doi.org/10.3390/diagnostics12071768
APA StyleChatzikostopoulos, A., Moraitou, D., Tsolaki, M., Masoura, E., Papantoniou, G., Sofologi, M., Papaliagkas, V., Kougioumtzis, G., & Papatzikis, E. (2022). Episodic Memory in Amnestic Mild Cognitive Impairment (aMCI) and Alzheimer’s Disease Dementia (ADD): Using the “Doors and People” Tool to Differentiate between Early aMCI—Late aMCI—Mild ADD Diagnostic Groups. Diagnostics, 12(7), 1768. https://doi.org/10.3390/diagnostics12071768