
Influence of Prior Imaging Information on Diagnostic Accuracy for Focal Skeletal Processes—A Retrospective Analysis of the Consistency between Biopsy-Verified Imaging Diagnoses

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
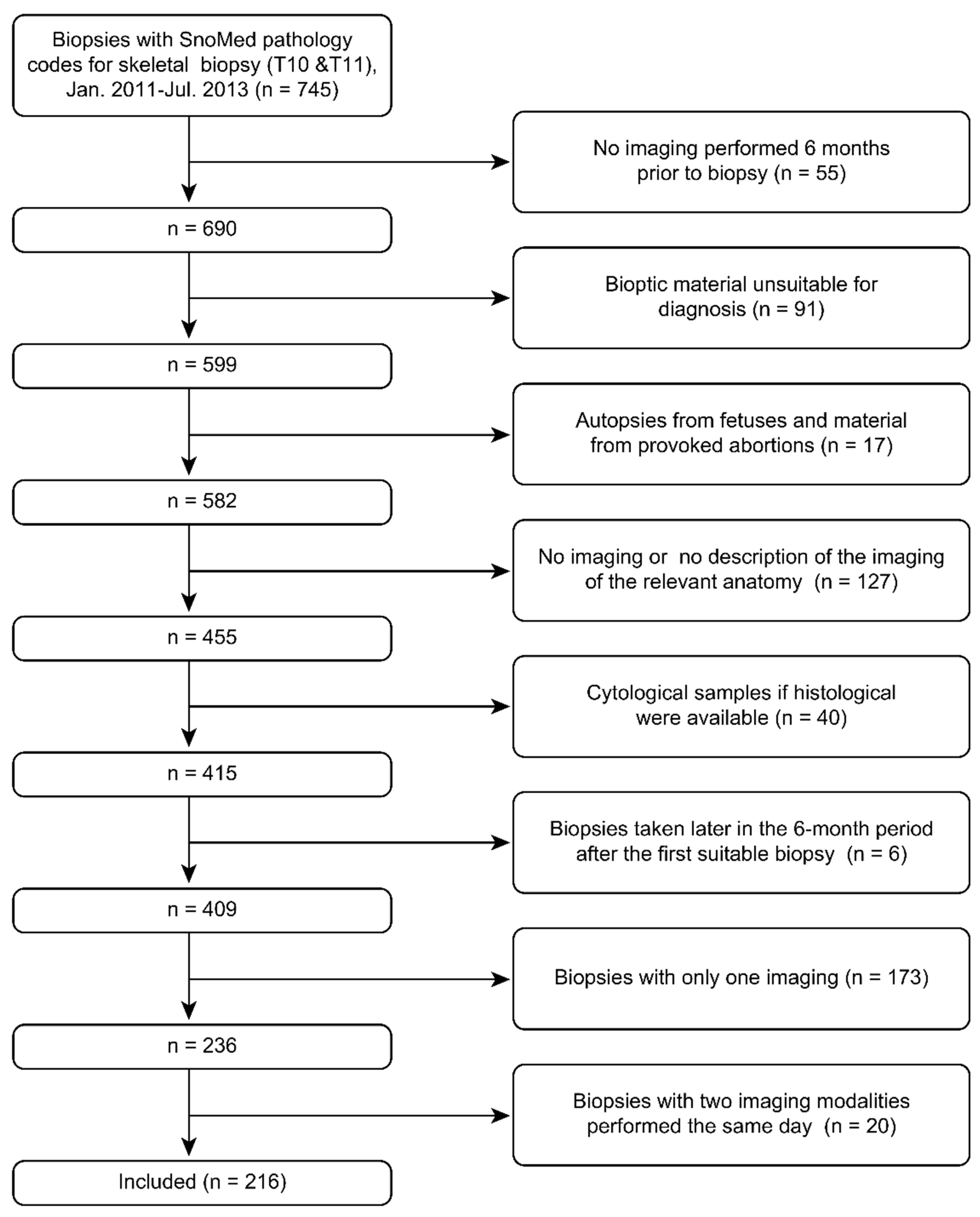
2.1. Collection of Skeletal Biopsies
2.2. Imaging
All radiology imaging procedures were performed in accordance with institutional guidelines (no experimental imaging investigations were included in the analysis), and the written reports were reviewed by two independent reviewers who, based upon the description and conclusions in the original text, classified the described lesion as malignant, benign, or inconclusive. In cases of disagreement after individual reading, the readers reached consensus for each imaging report without the need for a third-party arbitrator. The radiologists had access to an Electronical Patient Journal charts (EPJ—Clinical Suite, CSC Scandihealth A/S) for any relevant journal notes in case they needed more information than was stated in the referral.
2.3. Statistics
2.4. Approval
3. Results
3.1. Baseline Data
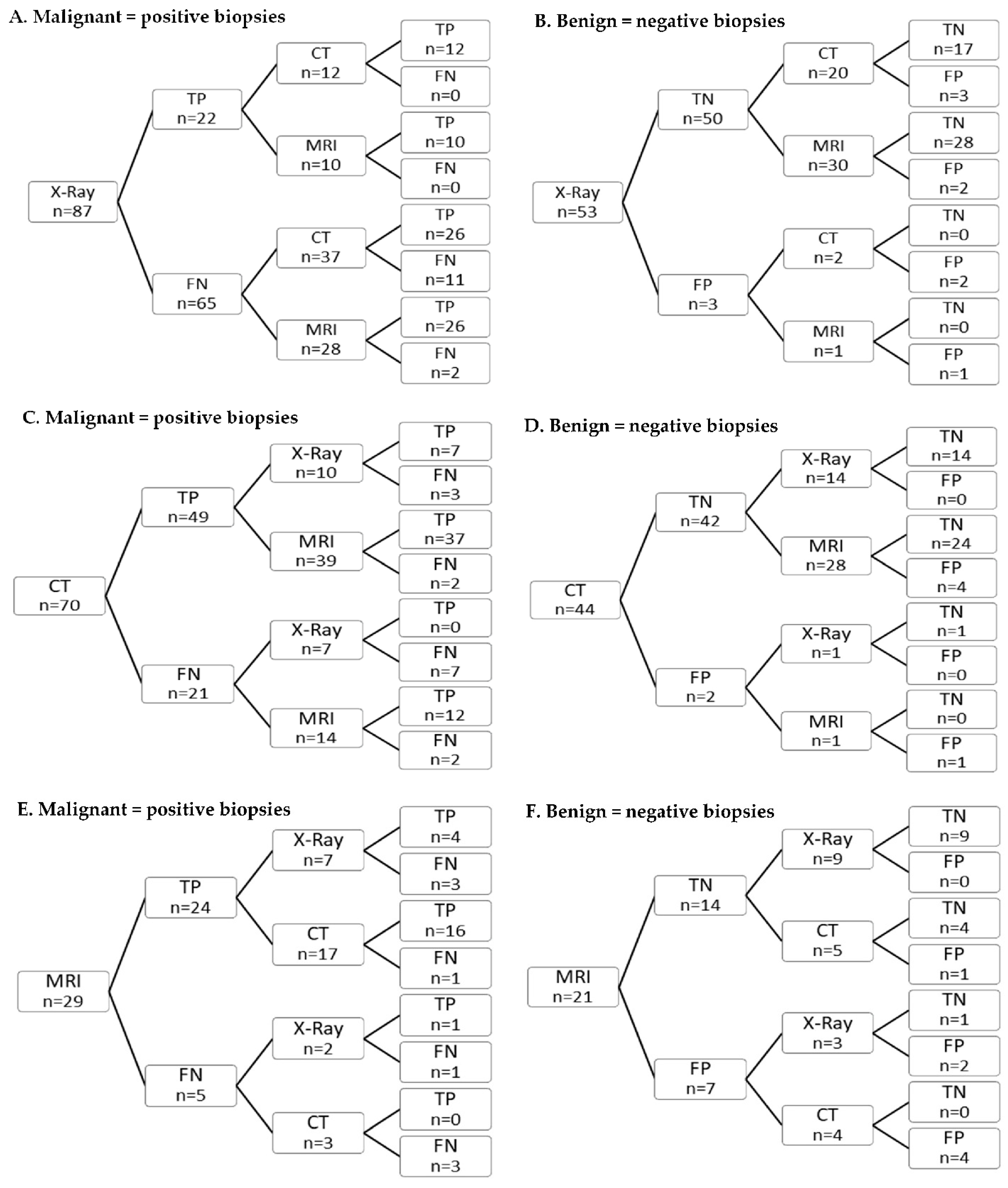
3.2. Sequence Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Busby, L.P.; Courtier, J.L.; Glastonbury, C.M. Bias in radiology: The how and why of misses and misinterpretations. Radiographics 2018, 38, 236–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, A.; Brunese, L.; Pinto, F.; Reali, R.; Daniele, S.; Romano, L. The concept of error and malpractice in radiology. Semin. Ultrasound CT MRI 2012, 33, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Robinson, J.D.; Hippe, D.S.; Deconde, R.P.; Zecevic, M.; Mehta, N. Emergency radiology: An underappreciated source of liability risk. J. Am. Coll. Radiol. 2020, 17, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Hong, G.-S.; Park, K.J.; Lee, C.W.; Lee, J.H.; Kim, S.-O. Impact of diagnostic errors on adverse outcomes: Learning from emergency department revisits with repeat CT or MRI. Insights Imaging 2021, 12, 160. [Google Scholar] [CrossRef] [PubMed]
- Raskin, M.M. Survival strategies for radiology: Some practical tips on how to reduce the risk of being sued and losing. J. Am. Coll. Radiol. 2006, 3, 689–693. [Google Scholar] [CrossRef] [PubMed]
- Pinto, L.B.A.; Brunese, L. Spectrum of diagnostic errors in radiology. World J. Radiol. 2010, 2, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Bruno, M.A.; Walker, E.A.; Abujudeh, H.H. Understanding and confronting our mistakes: The epidemiology of error in radiology and strategies for error reduction. Radiographics 2015, 35, 1668–1676. [Google Scholar] [CrossRef]
- Degnan, A.J.; Ghobadi, E.H.; Hardy, P.; Krupinski, E.; Scali, E.P.; Stratchko, L.; Ulano, A.; Walker, E.; Wasnik, A.P.; Auffermann, W.F. Perceptual and interpretive error in diagnostic radiology—Causes and potential solutions. Acad. Radiol. 2019, 26, 833–845. [Google Scholar] [CrossRef]
- Abujudeh, H.H.; Boland, G.W.; Kaewlai, R.; Rabiner, P.; Halpern, E.F.; Gazelle, G.S.; Thrall, J.H. Abdominal and pelvic computed tomography (CT) interpretation: Discrepancy rates among experienced radiologists. Eur. Radiol. 2010, 20, 1952–1957. [Google Scholar] [CrossRef]
- Kahn, C.E.; Langlotz, C.P.; Burnside, E.S.; Carrino, J.A.; Channin, D.S.; Hovsepian, D.M.; Rubin, D.L. Toward best practices in radiology reporting. Radiology 2009, 252, 852–856. [Google Scholar] [CrossRef]
- Standards for Interpretation and Reporting of Imaging Investigations, 2nd ed.; The Royal College of Radiologists: London, UK, 2008; Available online: https://www.rcr.ac.uk/publication/standards-interpretation-and-reporting-imaging-investigations-second-edition (accessed on 22 October 2021).
- Hunter, T.B.; Boyle, R.R. The value of reading the previous radiology report. AJR Am. J. Roentgenol. 1988, 150, 697–698. [Google Scholar] [CrossRef] [PubMed]
- Berbaum, K.S.; Smith, W.L. Use of reports of previous radiologic studies. Acad. Radiol. 1998, 5, 111–114. [Google Scholar] [CrossRef]
- Berlin, L. Comparing new radiographs with those obtained previously. AJR Am. J. Roentgenol. 1999, 172, 3–6. [Google Scholar] [CrossRef] [PubMed]
- European Society of Radiology. Good practice for radiological reporting. Guidelines from the European Society of Radiology (ESR). Insights Imaging 2011, 2, 93–96. [Google Scholar] [CrossRef] [Green Version]
- Brady, A.; Laoide, R.; McCarthy, P.; McDermott, R. Discrepancy and error in radiology: Concepts, causes and consequences. Ulst. Med. J. 2012, 81, 3–9. [Google Scholar]
- Berlin, L. Malpractice issues in radiology. Alliterative errors. AJR Am. J. Roentgenol. 2000, 174, 925–931. [Google Scholar] [CrossRef]
- White, K.; Berbaum, K.; Smith, W.L. The role of previous radiographs and reports in the interpretation of current radiographs. Investig. Radiol. 1994, 29, 263–265. [Google Scholar] [CrossRef]
- Aideyan, U.O.; Berbaum, K.; Smith, W.L. Influence of prior radiologic information on the interpretation of radiographic examinations. Acad. Radiol. 1995, 2, 205–208. [Google Scholar] [CrossRef]
- Hattori, S.; Yokota, H.; Takada, T.; Horikoshi, T.; Takishima, H.; Mikami, W.; Mukai, H.; Funakoshi, H.; Naganuma, T.; Yano, T.; et al. Impact of clinical information on CT diagnosis by radiologist and subsequent clinical management by physician in acute abdominal pain. Eur. Radiol. 2021, 31, 5454–5463. [Google Scholar] [CrossRef]
- Berbaum, K.S.; Franken, E.A. Commentary: Does clinical history affect perception? Acad. Radiol. 2006, 13, 402–403. [Google Scholar] [CrossRef]
- Doubilet, P.; Herman, P.G. Interpretation of radiographs: Effect of clinical history. AJR Am. J. Roentgenol. 1981, 137, 1055–1058. [Google Scholar] [CrossRef] [PubMed]
- Loy, C.T.; Irwig, L. Accuracy of diagnostic tests read with and without clinical information: A systematic review. JAMA 2004, 292, 1602–1609. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.B.; Nielsen, M.L.; Andersen, J.D.; Lilholt, H.J.; Vyberg, M.; Petersen, L.J. Diagnostic accuracy of imaging methods for the diagnosis of skeletal malignancies: A retrospective analysis against a pathology-proven reference. Eur. J. Radiol. 2016, 85, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.B.; Petersen, L.J.; Nielsen, M.B.; Zacho, H.D. Validity of negative bone biopsy in suspicious bone lesions. Acta Radiol. Open 2021, 10, 20584601211030662. [Google Scholar] [CrossRef] [PubMed]
- Bruun, N. Stata Module to Build, Present and Style Stata Matrices, Statistical Software Components S458201. Available online: https://ideas.repec.org/c/boc/bocode/s458201.html (accessed on 21 October 2021).
- Coleman, R.E.; Croucher, P.I.; Padhani, A.R.; Clézardin, P.; Chow, E.; Fallon, M.; Guise, T.; Colangeli, S.; Capanna, R.; Costa, L. Bone metastases. Nat. Rev. Dis. Prim. 2020, 6, 83. [Google Scholar] [CrossRef] [PubMed]
- Macedo, F.; Ladeira, K.; Pinho, F.; Saraiva, N.; Bonito, N.; Pinto, L.; Gonçalves, F. Bone metastases: An overview. Oncol. Rev. 2017, 11, 321. [Google Scholar] [CrossRef]
- O’Sullivan, G.J.; Carty, F.L.; Cronin, C.G. Imaging of bone metastasis: An update. World J. Radiol. 2015, 7, 202–211. [Google Scholar] [CrossRef]
- Heindel, W.; Gübitz, R.; Vieth, V.; Weckesser, M.; Schober, O.; Schäfers, M. The diagnostic imaging of bone metastases. Dtsch. Arztebl. Int. 2014, 111, 741–747. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Patients (n = 207) | |
| Male, n (%) | 116 (56%) |
| Female, n (%) | 91 (44%) |
| Age, median (range) | 67 (1–93) |
| Biopsies (n = 216) | |
| Malignant, n (%) | 132 (61%) |
| Benign, n (%) | 84 (39%) |
| Biopsy specimen (n = 216) | |
| Cytological, n (%) | 16 (8%) |
| Histological, n (%) | 195 (90%) |
| Dissection, n (%) | 5 (2%) |
| Imaging modalities performed (n = 464) | |
| X-ray, n (% of biopsies) | 143 (66%) |
| CT, n (% of biopsies) | 169 (78%) |
| MRI, n (% of biopsies) | 152 (70%) |
| Localization of bone lesion (n = 216) | |
| Spine, n (%) | 119 (55%) |
| Extremities, n (%) | 39 (18%) |
| Pelvis, n (%) | 36 (17%) |
| Thorax and shoulders, n (%) | 19 (9%) |
| Head, n (%) | 3 (1%) |
| X-ray (n = 143) | CT (n = 169) | MRI (n = 152) | |
|---|---|---|---|
| Sensitivity | 31.3 (21.4–42.6) | 73.5 (64.3–81.3) | 92.1 (84.5–96.8) |
| Specificity | 95.2 (86.7–99.0) | 85.7 (73.8–93.6) | 81.0 (69.1–89.8) |
| Accuracy | 59.4 (50.9–67.6) | 77.5 (70.5–83.6) | 87.5 (81.2–92.3) |
| PPV | 89.3 (71.8–97.7) | 91.2 (83.4–96.1) | 87.2 (78.8–93.2) |
| NPV | 52.2 (42.7–61.6) | 61.5 (49.8–72.3) | 87.9 (76.7–95.01) |
| X-ray | CT | |||||
|---|---|---|---|---|---|---|
| Not Preceded by MRI (n = 122) | Preceded by MRI (n = 21) | p Value | Not Preceded by MRI (n = 140) | Preceded by MRI (n = 29) | p Value | |
| Sensitivity | 28.2 (18.1–40.1) | 55.6 (21.2–86.3) | 0.13 | 72.0 (61.8–80.9) | 80.0 (56.3–94.3) | 0.58 |
| Specificity | 98.0 (89.6–100.0) | 83.3 (51.6–97.9) | 0.09 | 93.6 (82.5–98.7) | 44.4 (13.7–78.8) | 0.00 |
| Accuracy | 70.0 (63.1–76.3) | 65.2 (42.7–83.6) | 0.34 | 79.3 (71.6–85.7) | 69.0 (49.2–84.7) | 0.23 |
| PPV | 95.2 (76.2–99.9) | 71.4 (29.0–96.3) | 0.15 | 95.7 (88.0–99.1) | 76.2 (52.8–91.8) | 0.01 |
| NPV | 49.5 (39.4–59.6) | 71.4 (41.9–91.6) | 0.16 | 62.9 (50.5–74.1) | 50.0 (15.7–84.3) | 0.48 |
| X-ray | MRI | |||||
|---|---|---|---|---|---|---|
| Not Preceded by CT (n = 111) | Preceded by CT (n = 32) | p Value | Not Preceded by CT (n = 70) | Preceded by CT (n = 82) | p Value | |
| Sensitivity | 28.6 (17.9–41.3) | 41.2 (18.4–67.1) | 0.38 | 91.7 (77.5–98.2) | 92.5 (81.8–97.9) | 1.00 |
| Specificity | 93.8 (82.8–98.7) | 100.0 (78.2–100.0) | 1.00 | 79.4 (62.1–91.3) | 82.8 (64.2–94.2) | 1.00 |
| Accuracy | 56.8 (47.0–66.1) | 68.8 (50.0–83.9) | 0.84 | 85.7 (75.3–92.9) | 89.0 (80.2–94.9) | 0.63 |
| PPV | 85.7 (63.7–97.0) | 100.0 (59.0–100.0) | 0.55 | 82.5 (67.2–92.7) | 90.7 (79.7–96.9) | 0.35 |
| NPV | 50.0 (39.9–60.7) | 60.0 (38.7–78.9) | 0.50 | 90.0 (73.5–97.9) | 85.7 (67.3–96.0) | 0.70 |
| CT | MRI | |||||
|---|---|---|---|---|---|---|
| Not Preceded by X-ray (n = 98) | Preceded by X-ray (n = 71) | p Value | Not Preceded by X-ray (n = 83) | Preceded by X-ray (n = 69) | p Value | |
| Sensitivity | 70.3 (57.6–88.1) | 77.6 (63.4–88.2) | 0.52 | 90.2 (78.6–96.7) | 94.7 (82.3–99.4) | 0.69 |
| Specificity | 91.2 (76.3–98.1) | 77.3 (54.6–92.2) | 0.24 | 71.9 (53.3–86.3) | 90.3 (74.2–98.0) | 0.11 |
| Accuracy | 77.6 (68.0–65.4) | 77.5 (66.0–86.5) | 1.00 | 83.1 (73.3–90.5) | 92.8 (83.9–97.6) | 0.09 |
| PPV | 93.8 (82.8–98.7) | 88.4 (74.9–96.1) | 0.47 | 83.6 (71.2–92.2) | 92.3 (79.1–98.4) | 0.35 |
| NPV | 62.0 (47.2–75.3) | 60.7 (40.6–78.5) | 1.00 | 82.1 (63.1–93.9) | 93.3 (77.9–99.2) | 0.25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lange, M.B.; Petersen, L.J.; Lausen, M.; Bruun, N.H.; Nielsen, M.B.; Zacho, H.D. Influence of Prior Imaging Information on Diagnostic Accuracy for Focal Skeletal Processes—A Retrospective Analysis of the Consistency between Biopsy-Verified Imaging Diagnoses. Diagnostics 2022, 12, 1735. https://doi.org/10.3390/diagnostics12071735
Lange MB, Petersen LJ, Lausen M, Bruun NH, Nielsen MB, Zacho HD. Influence of Prior Imaging Information on Diagnostic Accuracy for Focal Skeletal Processes—A Retrospective Analysis of the Consistency between Biopsy-Verified Imaging Diagnoses. Diagnostics. 2022; 12(7):1735. https://doi.org/10.3390/diagnostics12071735
Chicago/Turabian StyleLange, Mine Benedicte, Lars J. Petersen, Mads Lausen, Niels Henrik Bruun, Michael Bachmann Nielsen, and Helle D. Zacho. 2022. "Influence of Prior Imaging Information on Diagnostic Accuracy for Focal Skeletal Processes—A Retrospective Analysis of the Consistency between Biopsy-Verified Imaging Diagnoses" Diagnostics 12, no. 7: 1735. https://doi.org/10.3390/diagnostics12071735
APA StyleLange, M. B., Petersen, L. J., Lausen, M., Bruun, N. H., Nielsen, M. B., & Zacho, H. D. (2022). Influence of Prior Imaging Information on Diagnostic Accuracy for Focal Skeletal Processes—A Retrospective Analysis of the Consistency between Biopsy-Verified Imaging Diagnoses. Diagnostics, 12(7), 1735. https://doi.org/10.3390/diagnostics12071735