
Identifying Obstructive Sleep Apnoea in Patients with Empty Nose Syndrome

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Total Nasal Resistance (TNR)
2.3. Polysomnography
2.4. Subjective Evaluation
2.5. Statistical Analyses
3. Results
3.1. Clinical Characteristics of the Study Population
3.2. PSG Results
3.3. Regression Analyses for AHI
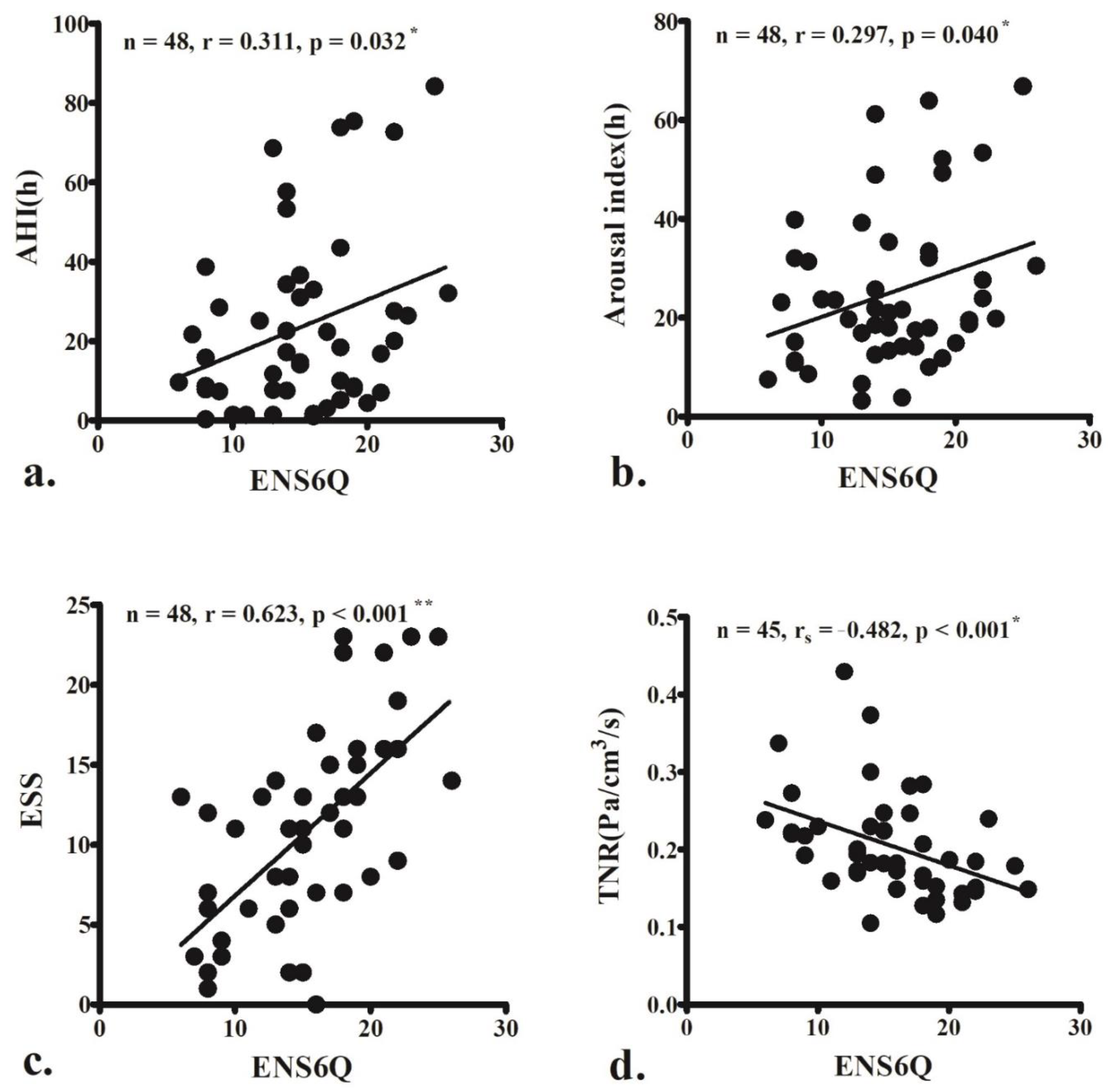
3.4. Correlation Analyses of ENS6Q
3.5. Using Clinical Metrics to Detect Moderate-to-Severe OSA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Veasey, S.C.; Rosen, I.M. Obstructive sleep apnea in adults. N. Engl. J. Med. 2019, 380, 1442–1449. [Google Scholar] [CrossRef]
- McEvoy, R.D.; Antic, N.A.; Heeley, E.; Luo, Y.; Ou, Q.; Zhang, X.; Mediano, O.; Chen, R.; Drager, L.F.; Liu, Z.; et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N. Engl. J. Med. 2016, 375, 919–931. [Google Scholar] [CrossRef]
- Houser, S.M. Empty nose syndrome associated with middle turbinate resection. Otolaryngol.-Head Neck Surg. 2006, 135, 972–973. [Google Scholar] [CrossRef]
- Sozansky, J.; Houser, S.M. Pathophysiology of empty nose syndrome. Laryngoscope 2015, 125, 70–74. [Google Scholar] [CrossRef]
- Zhao, K.; Blacker, K.; Luo, Y.; Bryant, B.; Jiang, J. Perceiving nasal patency through mucosal cooling rather than air temperature or nasal resistance. PLoS ONE 2011, 6, e24618. [Google Scholar] [CrossRef]
- Chen, X.B.; Leong, S.C.; Lee, H.P.; Chong, V.F.; Wang, D.Y. Aerodynamic effects of inferior turbinate surgery on nasal airflow—A computational fluid dynamics model. Rhinol. J. 2010, 48, 394–400. [Google Scholar] [CrossRef]
- Konstantinidis, I.; Tsakiropoulou, E.; Chatziavramidis, A.; Ikonomidis, C.; Markou, K. Intranasal trigeminal function in patients with empty nose syndrome. Laryngoscope 2017, 127, 1263–1267. [Google Scholar] [CrossRef]
- Wu, C.L.; Fu, C.H.; Lee, T.J. Distinct histopathology characteristics in empty nose syndrome. Laryngoscope 2021, 131, E14–E18. [Google Scholar]
- Chhabra, N.; Houser, S.M. The diagnosis and management of empty nose syndrome. Otolaryngol. Clin. N. Am. 2009, 42, 311–330. [Google Scholar] [CrossRef]
- Jiang, C.; Wang, F.; Chen, K.; Shi, R. Assessment of surgical results in patients with empty nose syndrome using the 25-item sino-nasal outcome test evaluation. JAMA Otolaryngol.-Head Neck Surg. 2014, 140, 453–458. [Google Scholar] [CrossRef]
- Manji, J.; Nayak, J.V.; Thamboo, A. The functional and psychological burden of empty nose syndrome. Int. Forum Allergy Rhinol. 2018, 8, 707–712. [Google Scholar] [CrossRef]
- Mangin, D.; Bequignon, E.; Zerah-Lancner, F.; Isabey, D.; Louis, B.; Adnot, S.; Papon, J.-F.; Coste, A.; Boyer, L.; Du Mayne, M.D. Investigating hyperventilation syndrome in patients suffering from empty nose syndrome. Laryngoscope 2017, 127, 1983–1988. [Google Scholar] [CrossRef]
- Lee, T.-J.; Fu, C.-H.; Wu, C.-L.; Tam, Y.-Y.; Huang, C.-C.; Chang, P.-H.; Chen, Y.-W.; Wu, M.-H. Evaluation of depression and anxiety in empty nose syndrome after surgical treatment. Laryngoscope 2016, 126, 1284–1289. [Google Scholar] [CrossRef]
- Huang, C.-C.; Wu, P.-W.; Fu, C.-H.; Chang, P.-H.; Wu, C.-L.; Lee, T.-J. What drives depression in empty nose syndrome? A sinonasal outcome test-25 subdomain analysis. Rhinol. J. 2019, 57, 469–476. [Google Scholar] [CrossRef]
- Huang, C.C.; Wu, P.W.; Fu, C.H.; Huang, C.C.; Chang, P.H.; Lee, T.J. Impact of psychologic burden on surgical outcome in empty nose syndrome. Laryngoscope 2021, 131, E694–E701. [Google Scholar] [CrossRef]
- Amanian, A.; Hari, K.; Habib, A.; Dholakia, S.S.; Nayak, J.; Thamboo, A. The empty nose syndrome 6-item questionnaire (ENS6Q): A diagnostic tool to distinguish empty nose syndrome from primary nasal obstruction. Int. Forum Allergy Rhinol. 2021, 11, 1113–1115. [Google Scholar] [CrossRef]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the sleep apnea definitions task force of the american academy of sleep medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Velasquez, N.; Thamboo, A.; Habib, A.-R.R.; Huang, Z.; Nayak, J.V. The empty nose syndrome 6-item questionnaire (ENS6Q): A validated 6-item questionnaire as a diagnostic aid for empty nose syndrome patients. Int. Forum Allergy Rhinol. 2016, 7, 64–71. [Google Scholar] [CrossRef]
- Thamboo, A.; Velasquez, N.; Habib, A.R.R.; Zarabanda, D.; Paknezhad, H.; Nayak, J.V. Defining surgical criteria for empty nose syndrome: Validation of the office-based cotton test and clinical interpretability of the validated empty nose syndrome 6-item questionnaire. Laryngoscope 2017, 127, 1746–1752. [Google Scholar] [CrossRef]
- Toma, S.; Hopkins, C. Stratification of SNOT-22 scores into mild, moderate or severe and relationship with other subjective instruments. Rhinology 2016, 54, 129–133. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Conradt, R.; Redhardt, F.; Beutel, B.; Hildebrandt, O.; Cassel, W.; Kesper, K.; Koehler, J.; Hildebrandt, W.; Koehler, U. Predisposing factors of daytime sleepiness in obese OSA patients. J. Sleep Res. 2021, 31, e13458. [Google Scholar] [CrossRef]
- Pressman, M.R. Primer of Polysomnogram Interpretation; Butterworth Heinemann: Boston, MA, USA, 2002. [Google Scholar]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.; Quan, S.F. The AASM manual for the scoring of sleep and associated events: Rules. In Terminology and Technical Specifications; American Academy of Sleep Medicine: Westchester, NY, USA, 2007. [Google Scholar]
- Shrivastava, D.; Jung, S.; Saadat, M.; Sirohi, R.; Crewson, K. How to interpret the results of a sleep study. J. Community Hosp. Intern. Med. Perspect. 2014, 4, 24983. [Google Scholar] [CrossRef]
- Wu, J.; He, S.; Li, Y.; Wang, T.; Zhao, G.; Pan, Y.; Zang, H.; Han, D. Evaluation of the clinical efficacy of nasal surgery in the treatment of obstructive sleep apnoea. Am. J. Otolaryngol. 2021, 43, 103158. [Google Scholar] [CrossRef]
- Huang, C.-C.; Cheng, P.-W.; Liao, L.-J.; Huang, T.-W. Reduction of postural nasal resistance following oropharyngeal surgery in patients with moderate-severe obstructive sleep apnea. Rhinol. J. 2021, 59, 75–80. [Google Scholar] [CrossRef]
- Dayal, A.; Rhee, J.S.; Garcia, G.J.M. Impact of middle versus inferior total turbinectomy on nasal aerodynamics. Otolaryngol.-Head Neck Surg. 2016, 155, 18–525. [Google Scholar] [CrossRef]
- Malik, J.; Li, C.; Maza, G.; Farag, A.A.; Krebs, J.P.; McGhee, S.; Zappitelli, G.; Deshpande, B.; Otto, B.A.; Zhao, K. Computational fluid dynamic analysis of aggressive turbinate reductions: Is it a culprit of empty nose syndrome? Int. Forum Allergy Rhinol. 2019, 9, 891–899. [Google Scholar] [CrossRef]
- Yosunkaya, S.; Kutlu, R.; Cihan, F.G. Evaluation of depression and quality of life in patients with obstructive sleep apnea syndrome. Niger. J. Clin. Pract. 2016, 19, 573–579. [Google Scholar] [CrossRef]
- Saunamäki, T.; Jehkonen, M. Depression and anxiety in obstructive sleep apnea syndrome: A review. Acta Neurol. Scand. 2007, 116, 277–288. [Google Scholar] [CrossRef]
- Stubbs, B.; Vancampfort, D.; Veronese, N.; Solmi, M.; Gaughran, F.; Manu, P.; Rosenbaum, S.; De Hert, M.; Fornaro, M. The prevalence and predictors of obstructive sleep apnea in major depressive disorder, bipolar disorder and schizophrenia: A systematic review and meta-analysis. J. Affect. Disord. 2016, 197, 259–267. [Google Scholar] [CrossRef]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of obstructive sleep apnea: A population health perspective. Am. J. Respir. Crit. Care Med. 2002, 165, 1217–1239. [Google Scholar] [CrossRef]
- Hein, M.; Lanquart, J.-P.; Loas, G.; Hubain, P.; Linkowski, P. Prevalence and risk factors of moderate to severe obstructive sleep apnea syndrome in major depression: A observational and retrospective study on 703 subjects. BMC Pulm. Med. 2017, 17, 165. [Google Scholar] [CrossRef]
- Ong, J.C.; Gress, J.L.; Pedro-Salcedo, M.G.S.; Manber, R. Frequency and predictors of obstructive sleep apnea among individuals with major depressive disorder and insomnia. J. Psychosom. Res. 2009, 67, 135–141. [Google Scholar] [CrossRef]
- Mulgrew, A.T.; Nasvadi, G.; Butt, A.; Cheema, R.; Fox, N.; Fleetham, J.A.; Ryan, C.F.; Cooper, P.; Ayas, N.T. Risk and severity of motor vehicle crashes in patients with obstructive sleep apnoea/hypopnoea. Thorax 2008, 63, 536–541. [Google Scholar] [CrossRef]
- Kent, B.D.; Grote, L.; Ryan, S.; Pépin, J.L.; Bonsignore, M.R.; Tkacova, R.; Saaresranta, T.; Verbraecken, J.; Lévy, P.; Hedner, J.; et al. Diabetes mellitus prevalence and control in sleep-disordered breathing: The European sleep apnea cohort (ESADA) study. Chest 2014, 146, 982–990. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Bonsignore, M.R.; Management Committee of EU Cost Action B26. Sleep apnoea as an independent risk factor for cardiovascular disease: Current evidence, basic mechanisms and research priorities. Eur. Respir. J. 2007, 29, 156–178. [Google Scholar] [CrossRef]
- Young, T.; Shahar, E.; Nieto, F.J.; Redline, S.; Newman, A.B.; Gottlieb, D.J.; Walsleben, J.A.; Finn, L.; Enright, P.; Samet, J.M. Predictors of sleep-disordered breathing in community-dwelling adults the sleep heart health study. Arch. Intern. Med. 2002, 162, 893–900. [Google Scholar] [CrossRef]
- Lavigne, F.; Petrof, B.J.; Johnson, J.R.; Lavigne, P.; Binothman, N.; Kassissia, G.O.; Al Samri, M.; Giordano, C.; Dubé, N.; Hercz, D.; et al. Effect of topical corticosteroids on allergic airway inflammation and disease severity in obstructive sleep apnoea. Clin. Exp. Allergy 2013, 43, 1124–1133. [Google Scholar]
- Gadi, G.; Wali, S.; Koshak, E.; Albar, M.; Fida, A.; Abdelaziz, M.; Alnoury, K.; Alama, N. The prevalence of allergic rhinitis and atopic markers in obstructive sleep apnea. J. Epidemiol. Glob. Health 2017, 7, 37–44. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Mean ± SD | Range |
|---|---|---|
| Age (year) | 44.5 ± 11.7 | 24–67 |
| Female:male, n | 7:41 | |
| Smoking, n | 11 | |
| BMI (kg/m2) | 24.0 ± 3.1 | 17.5–31.6 |
| NC (cm) | 37.3 ± 3.1 | 31–44 |
| sIgE (IU/mL) | 278.6 ± 546.1 | 2–2403 |
| TNR (Pa/cm3/s) | 0.20 ± 0.07 | 0.11–0.43 |
| ESS | 10.8 ± 6.1 | 1–23 |
| SNOT-22 | 63.9 ± 18.1 | 33–108 |
| ENS6Q | 15.2 ± 5.0 | 6–26 |
| Variables | Mean ± SD | Range |
|---|---|---|
| AHI (/h) | 23.8 ± 22.4 | 0.3–84.2 |
| Mild OSA, n (%) | 14 (29.2) | |
| Moderate OSA, n (%) | 12 (25.0) | |
| Severe OSA, n (%) | 14 (29.2) | |
| Arousal Index (/h) | 25.1 ± 15.9 | 3.2–66.8 |
| Snore index (/h) | 266.5 ± 162.9 | 2.6–593.6 |
| Lowest SpO2 (%) | 85.9 ± 11.1 | 45–98 |
| Mean SpO2 (%) | 96.6 ± 1.8 | 91–99 |
| Efficiency (%) | 73.4 ± 15.3 | 25.8–96.1 |
| Stage A (%) | 20.9 ± 13.8 | 3.5–73.5 |
| Stage REM (%) | 20.0 ± 8.1 | 2.2–36.2 |
| Stage N1 (%) | 30.2 ± 16.9 | 6.7–78.6 |
| Stage N2 (%) | 47.3 ± 15.5 | 5.0–75.5 |
| Stage N3 (%) | 2.1 ± 5.4 | 0.0–27.1 |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | B (95% CI) | β | p | B (95% CI) | β | p | VIF |
| Age(year) | 0.44 (−0.11–0.99) | 0.23 | 0.115 | ||||
| BMI(kg/m2) | 3.71 (1.19–5.52) | 0.52 | <0.001 ** | 3.44 (1.58–5.30) | 0.48 | <0.001 ** | 1.166 |
| NC(cm) | 3.83 (1.96–5.69) | 0.52 | <0.001 ** | 0.23 (−0.66–1.12) | 0.03 | 0.601 | 1.036 |
| sIgE(IU/mL) | 0.01 (0.002–0.025) | 0.32 | 0.026 * | 0.01 (0.003–0.023) | 0.32 | 0.01 * | 1.032 |
| TNR(Pa/cm3/s) | −44.61 (−148.08–58.85) | −0.13 | 0.389 | ||||
| ESS | 0.98 (−0.06–2.02) | 0.27 | 0.065 | 0.07 (−1.10–1.25) | 0.02 | 0.903 | 1.790 |
| SNOT-22 | 0.34 (−0.02–0.69) | 0.27 | 0.063 | −0.12 (−0.53–0.29) | −0.10 | 0.547 | 1.879 |
| ENS6Q | 1.40 (0.13–2.67) | 0.31 | 0.032 * | 1.13 (−0.41–2.68) | 0.25 | 0.147 | 2.042 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-C.; Wu, P.-W.; Chuang, C.-C.; Lee, C.-C.; Lee, Y.-S.; Chang, P.-H.; Fu, C.-H.; Huang, C.-C.; Lee, T.-J. Identifying Obstructive Sleep Apnoea in Patients with Empty Nose Syndrome. Diagnostics 2022, 12, 1720. https://doi.org/10.3390/diagnostics12071720
Huang C-C, Wu P-W, Chuang C-C, Lee C-C, Lee Y-S, Chang P-H, Fu C-H, Huang C-C, Lee T-J. Identifying Obstructive Sleep Apnoea in Patients with Empty Nose Syndrome. Diagnostics. 2022; 12(7):1720. https://doi.org/10.3390/diagnostics12071720
Chicago/Turabian StyleHuang, Chien-Chia, Pei-Wen Wu, Chi-Cheng Chuang, Cheng-Chi Lee, Yun-Shien Lee, Po-Hung Chang, Chia-Hsiang Fu, Chi-Che Huang, and Ta-Jen Lee. 2022. "Identifying Obstructive Sleep Apnoea in Patients with Empty Nose Syndrome" Diagnostics 12, no. 7: 1720. https://doi.org/10.3390/diagnostics12071720
APA StyleHuang, C.-C., Wu, P.-W., Chuang, C.-C., Lee, C.-C., Lee, Y.-S., Chang, P.-H., Fu, C.-H., Huang, C.-C., & Lee, T.-J. (2022). Identifying Obstructive Sleep Apnoea in Patients with Empty Nose Syndrome. Diagnostics, 12(7), 1720. https://doi.org/10.3390/diagnostics12071720