
Smartphone-Enabled versus Conventional Otoscopy in Detecting Middle Ear Disease: A Meta-Analysis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Eligibility Criteria and Study Inclusion
2.4. Data Management
2.5. Risk of Bias Assessment
2.6. Statistical Analysis
3. Results
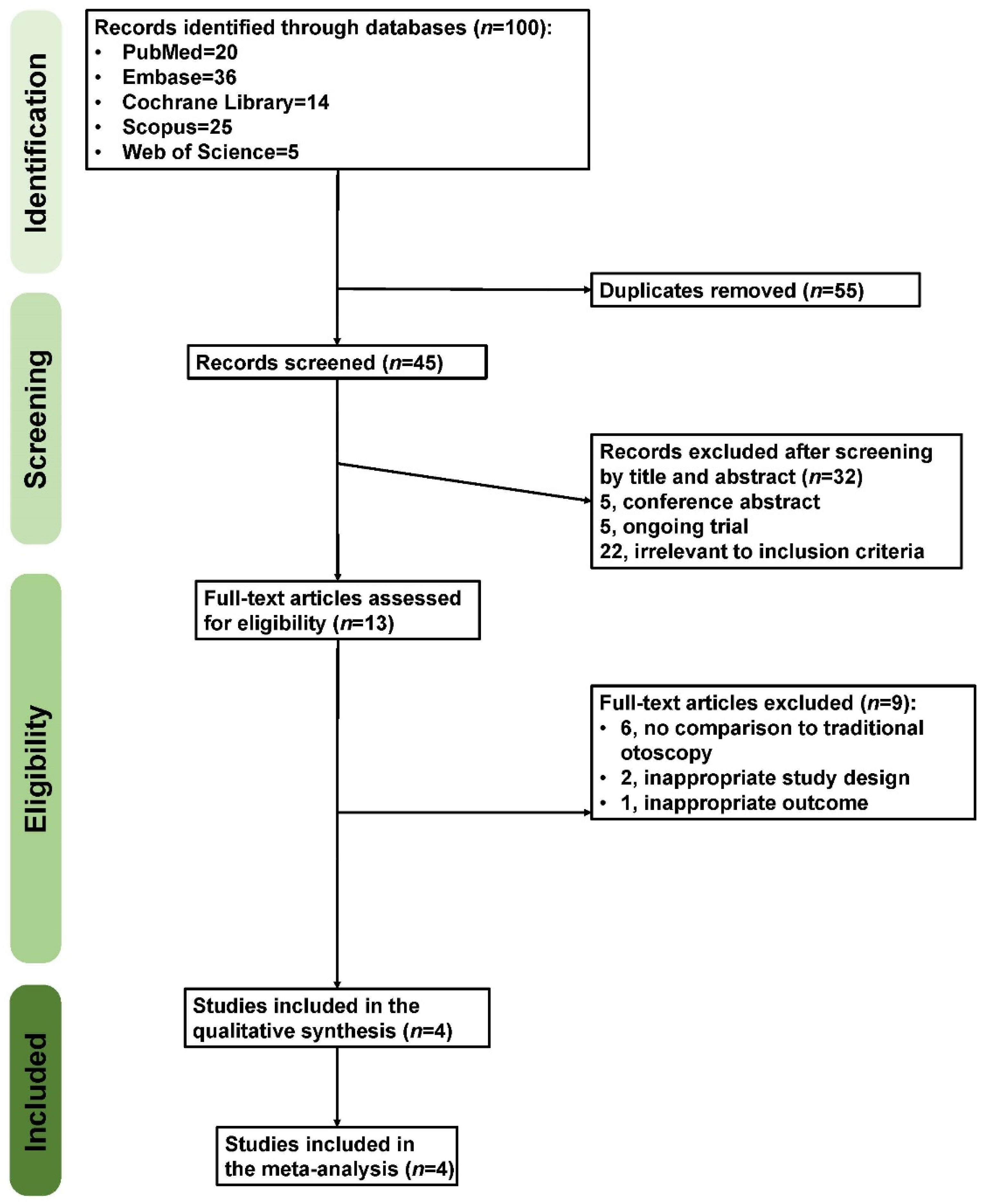
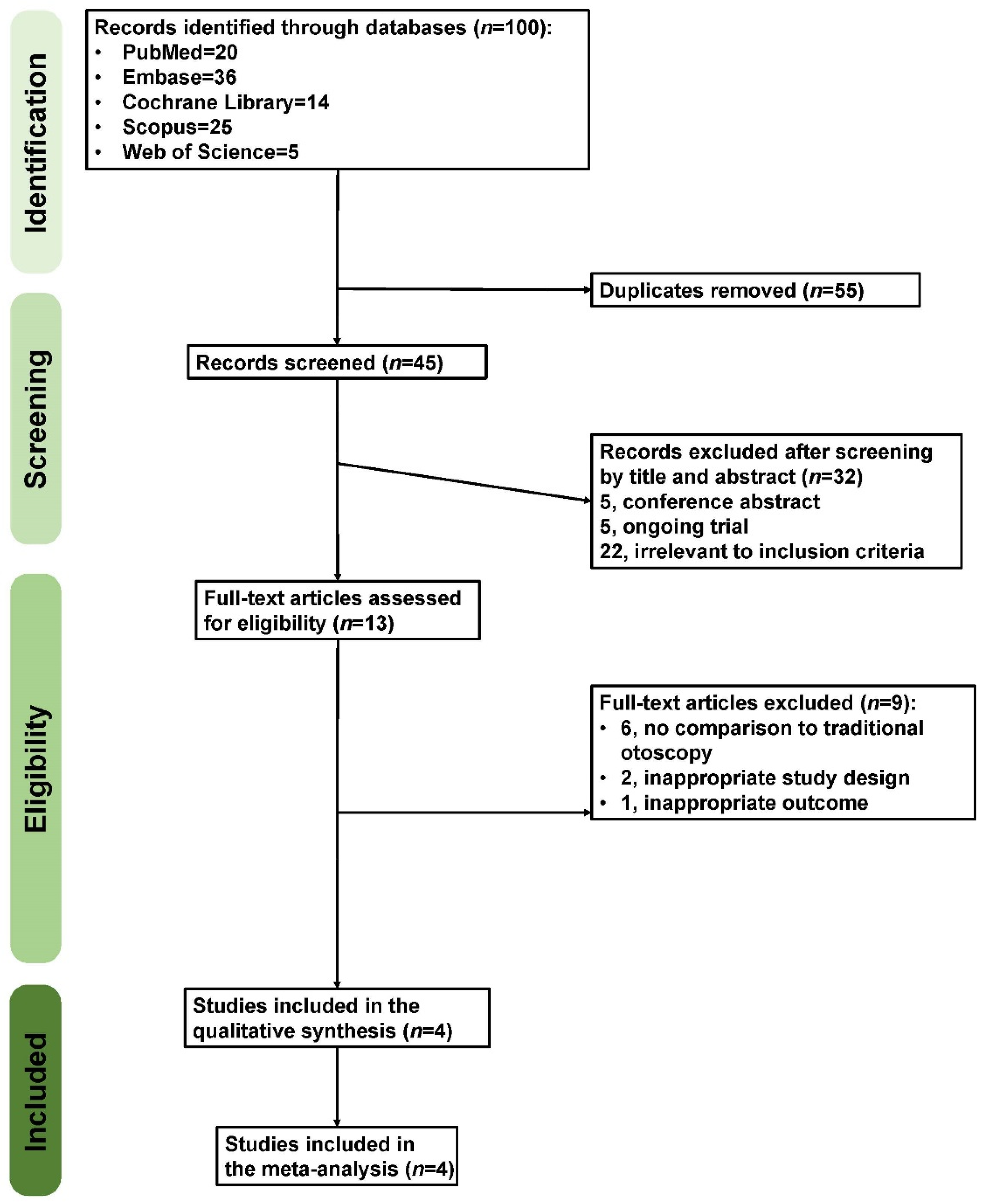
3.1. Study Identification and Selection
3.2. Study Characteristics
3.3. Risk of Bias Assessment
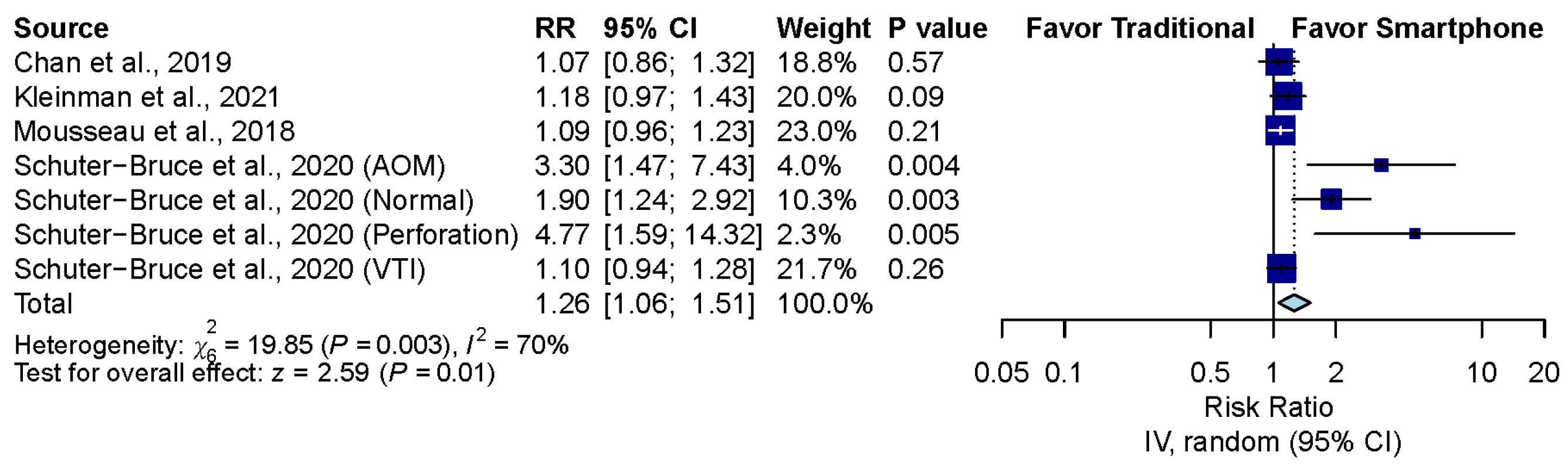
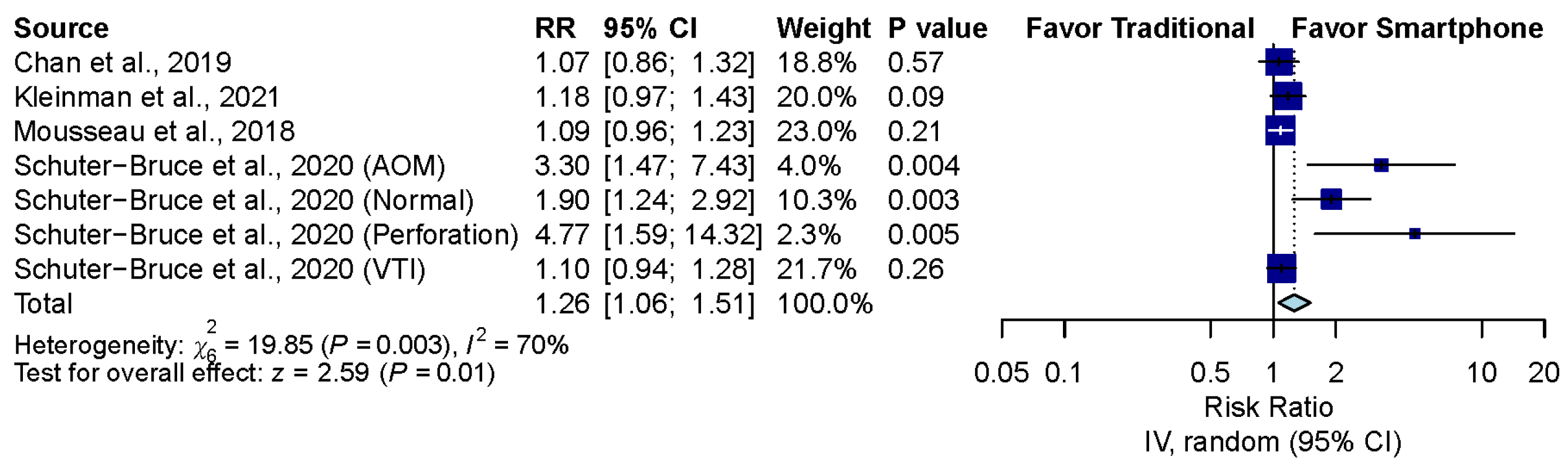
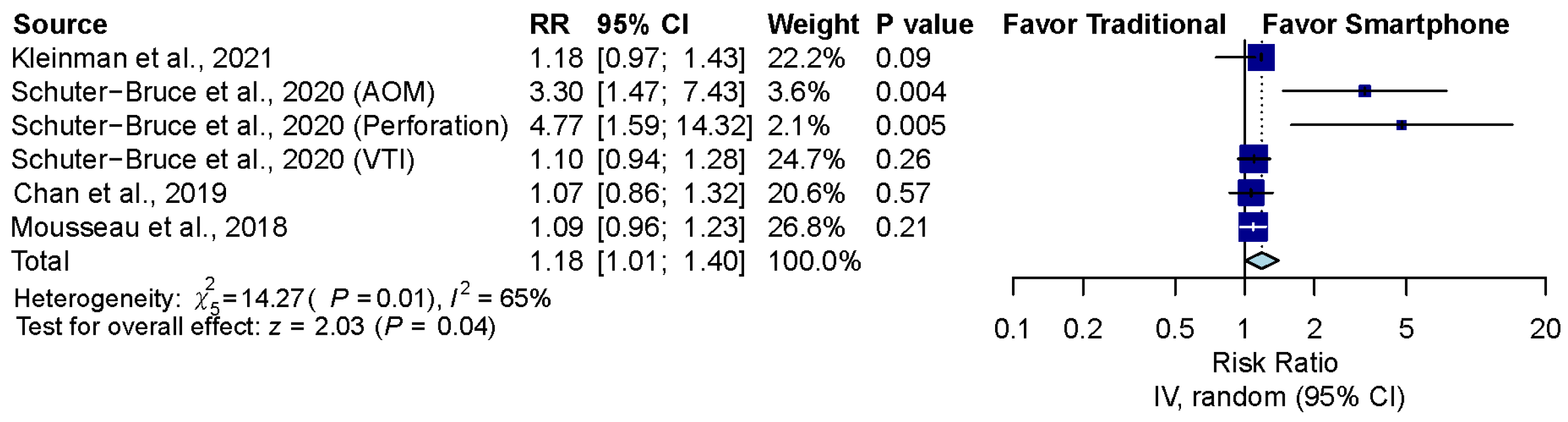
3.4. Overall Comparison between Smartphone-Enabled Otoscopy and Traditional Otoscopy
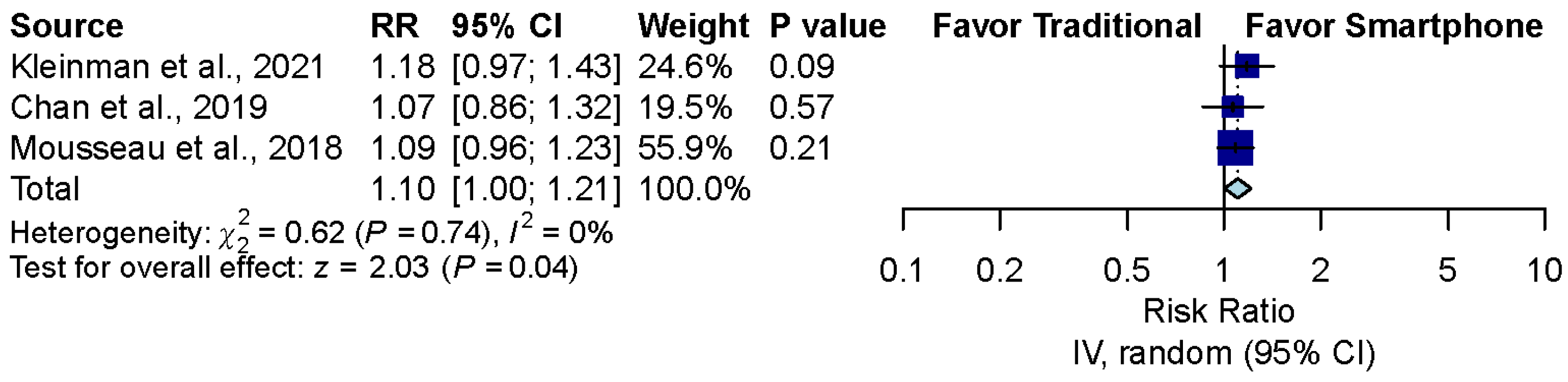
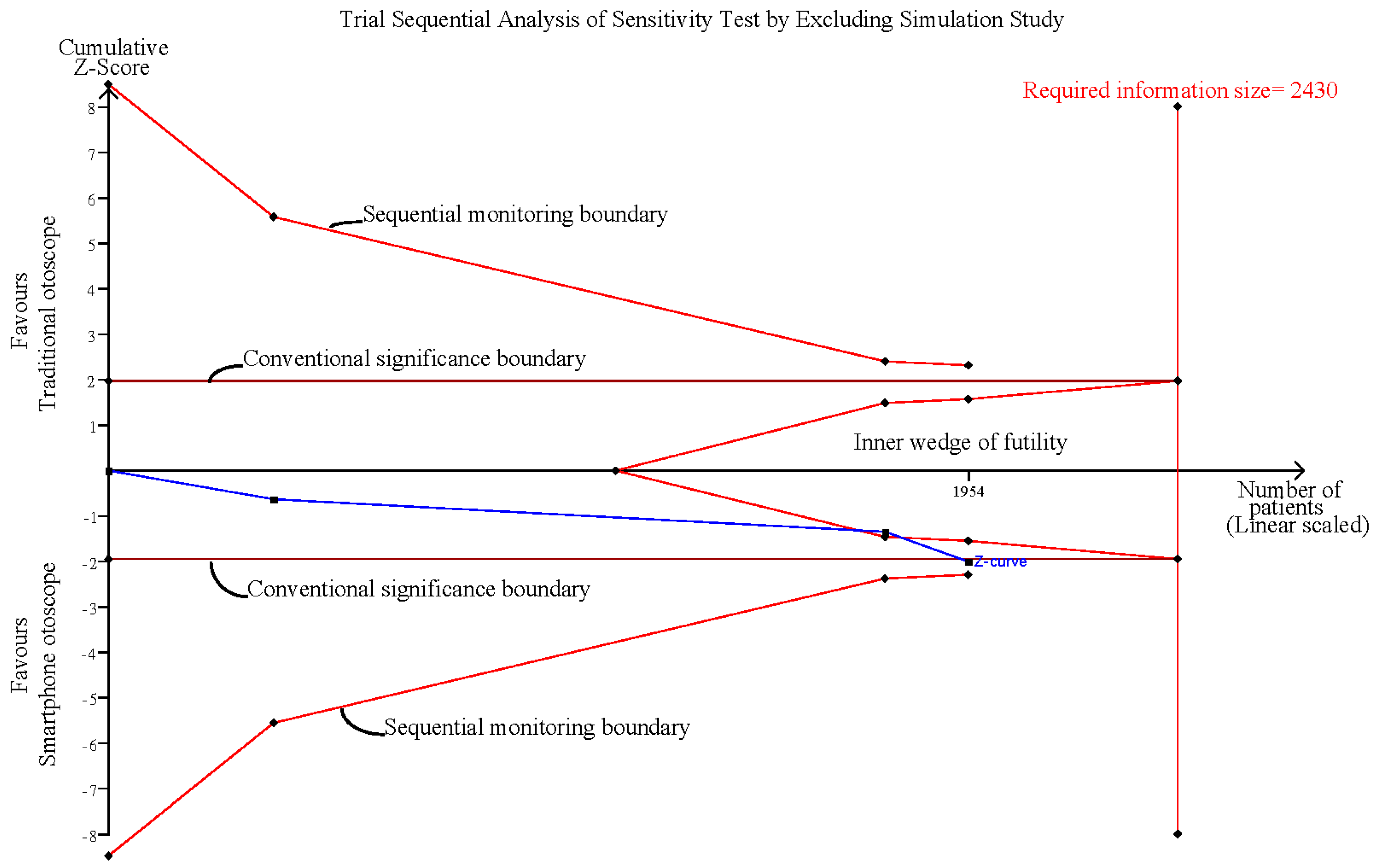
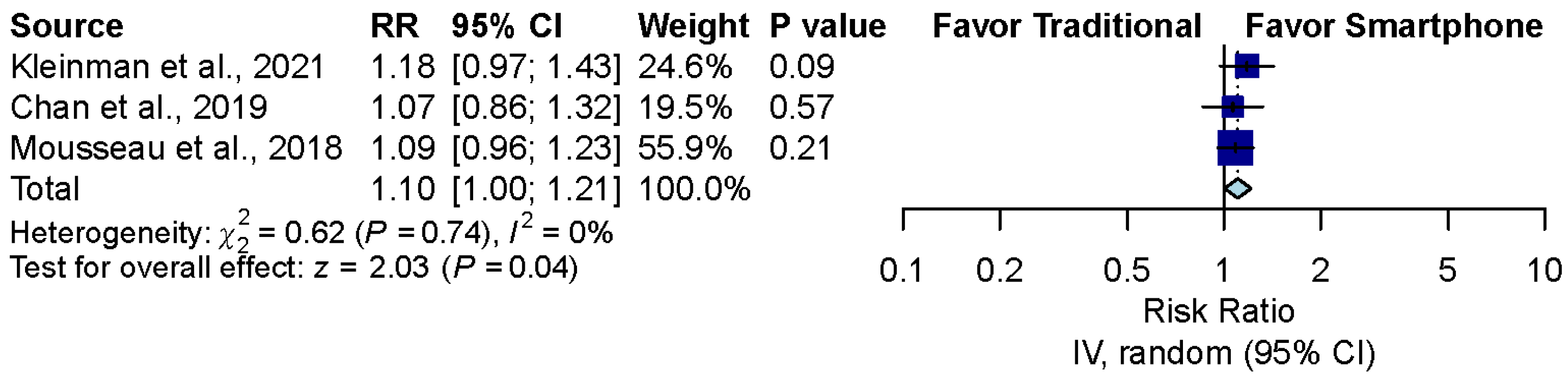
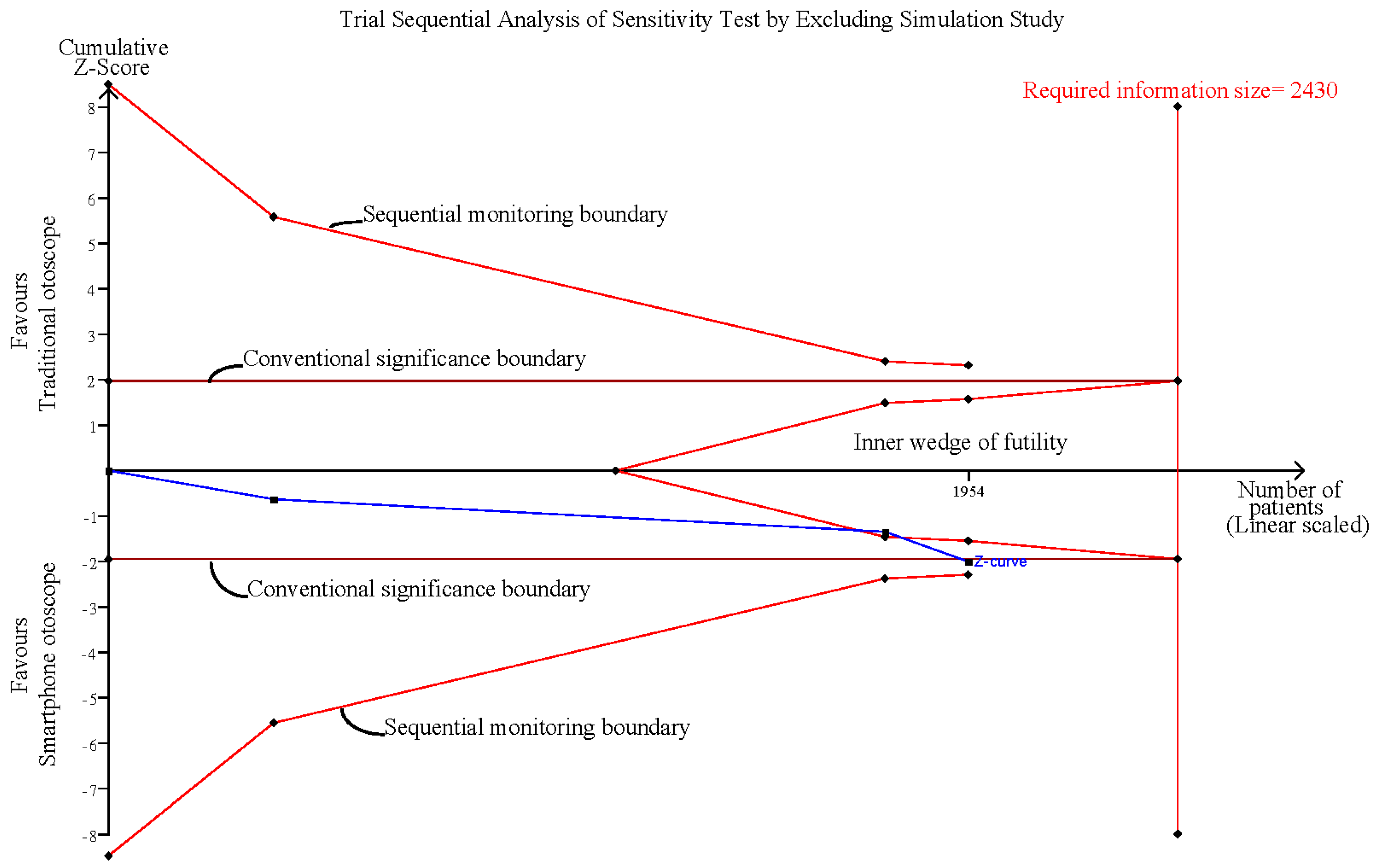
3.5. Sensitivity Analysis after Excluding the Simulation Study
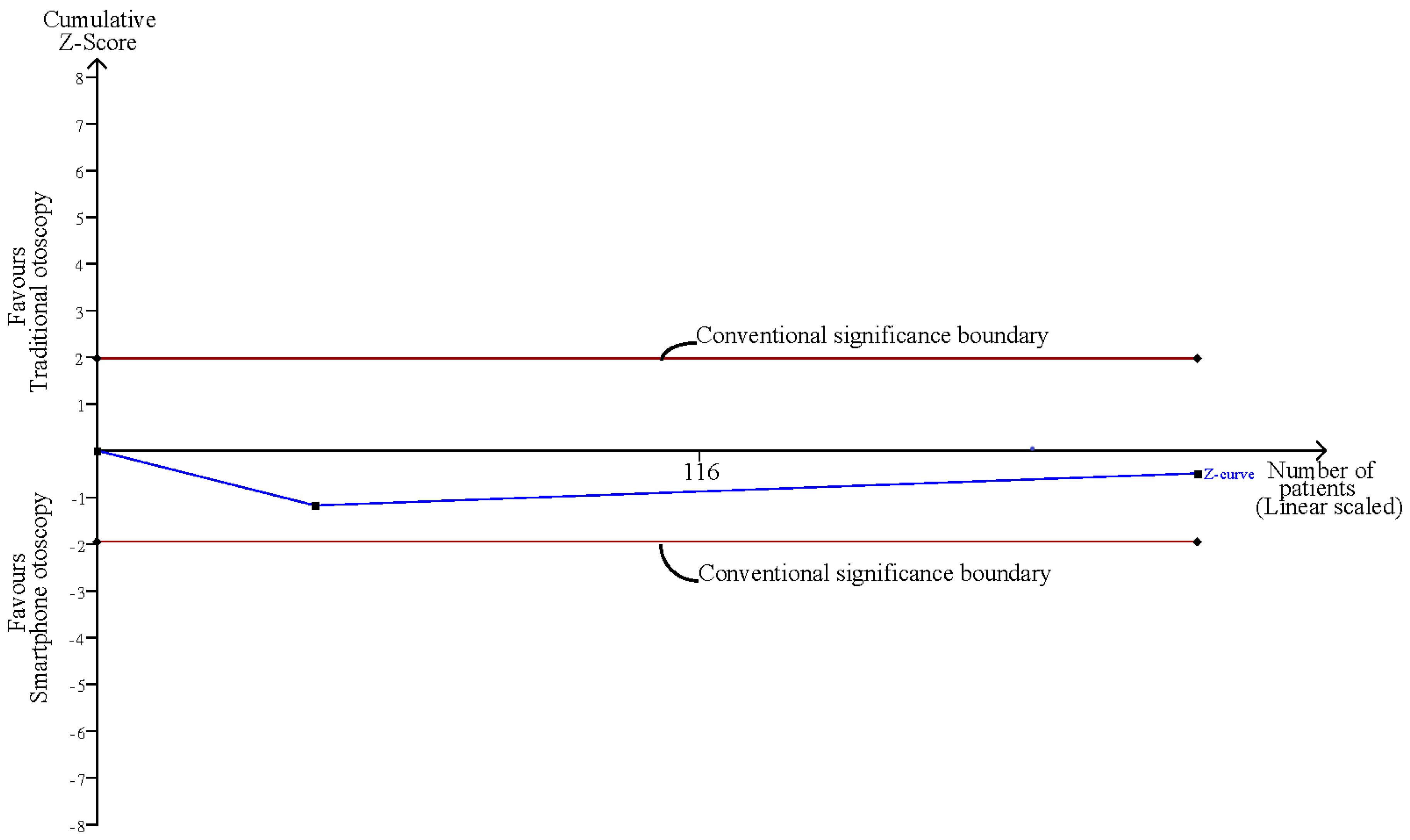
3.6. Sensitivity Analysis after Excluding Normal Ear Conditions
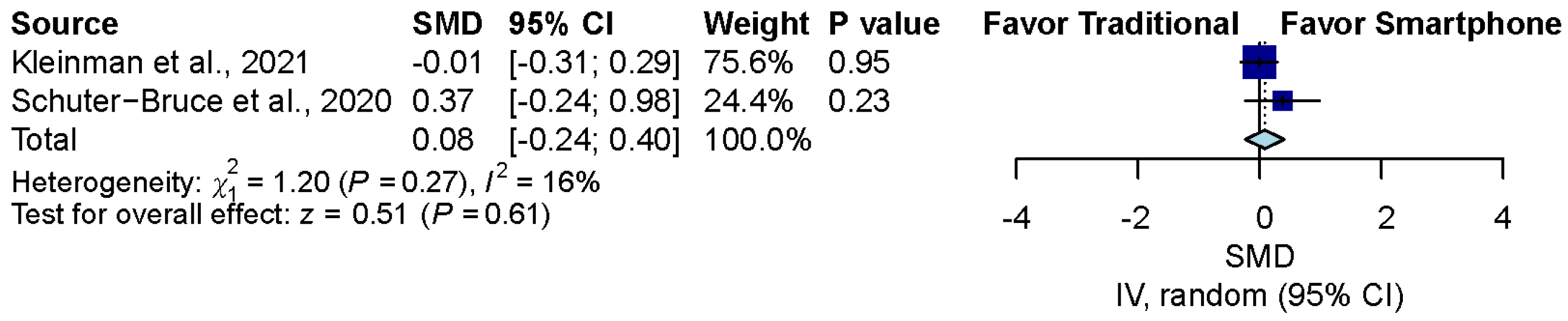
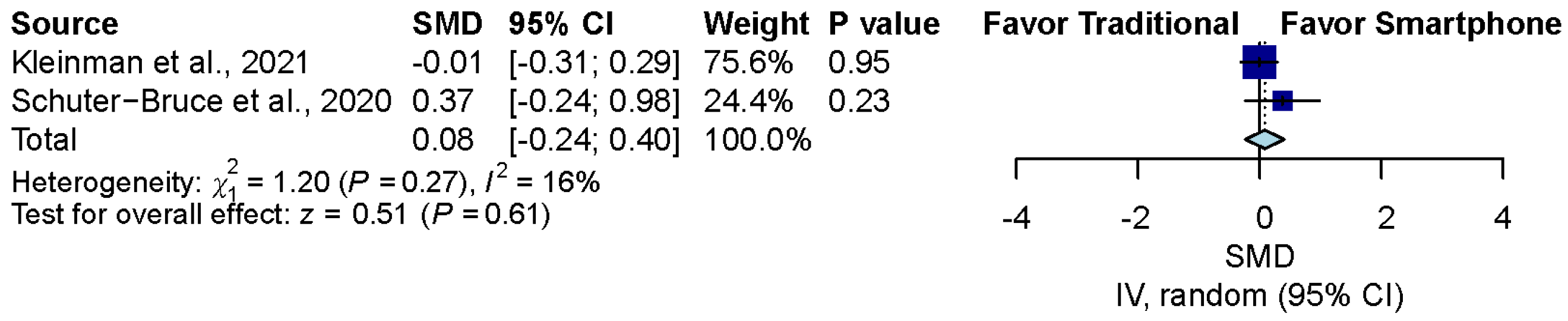
3.7. Confidence Comparison between Smartphone-Enabled Otoscopy and Traditional Otoscopy
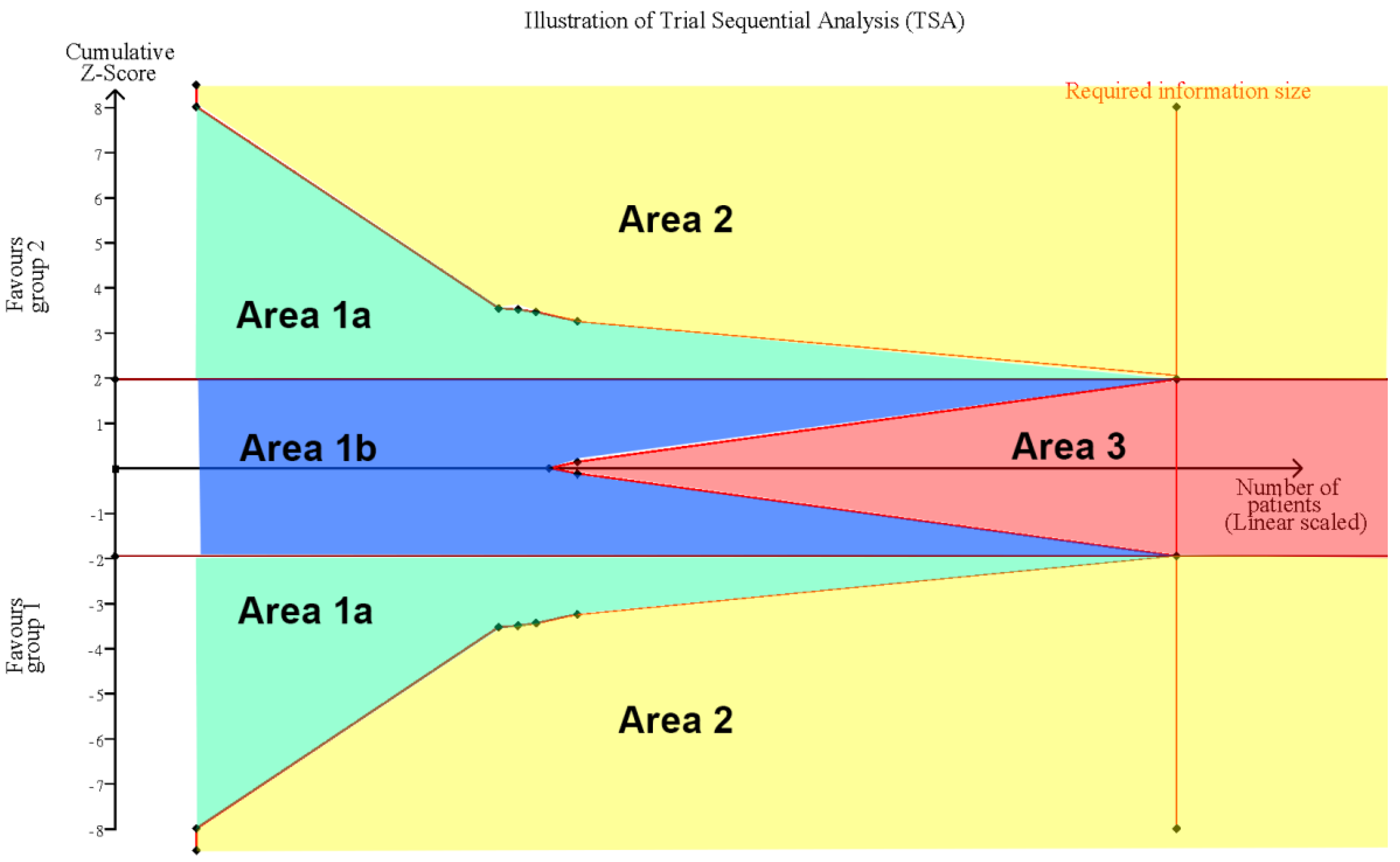
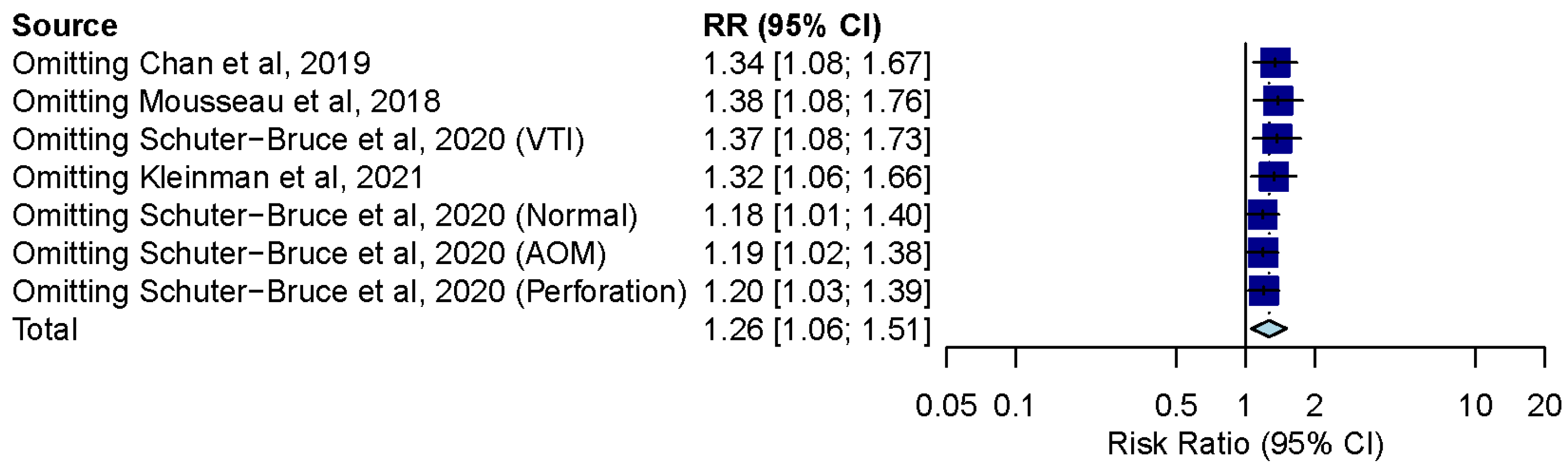
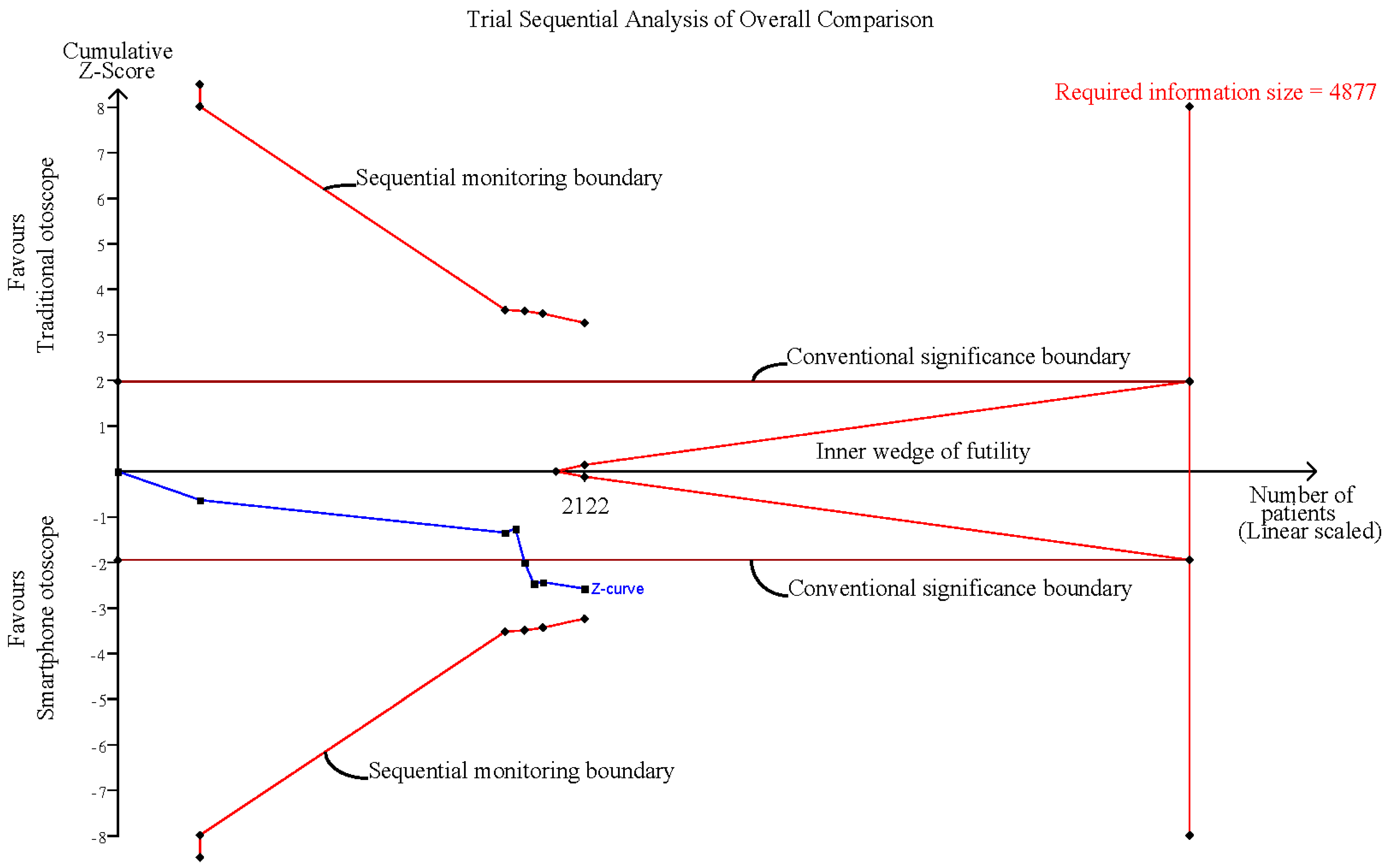
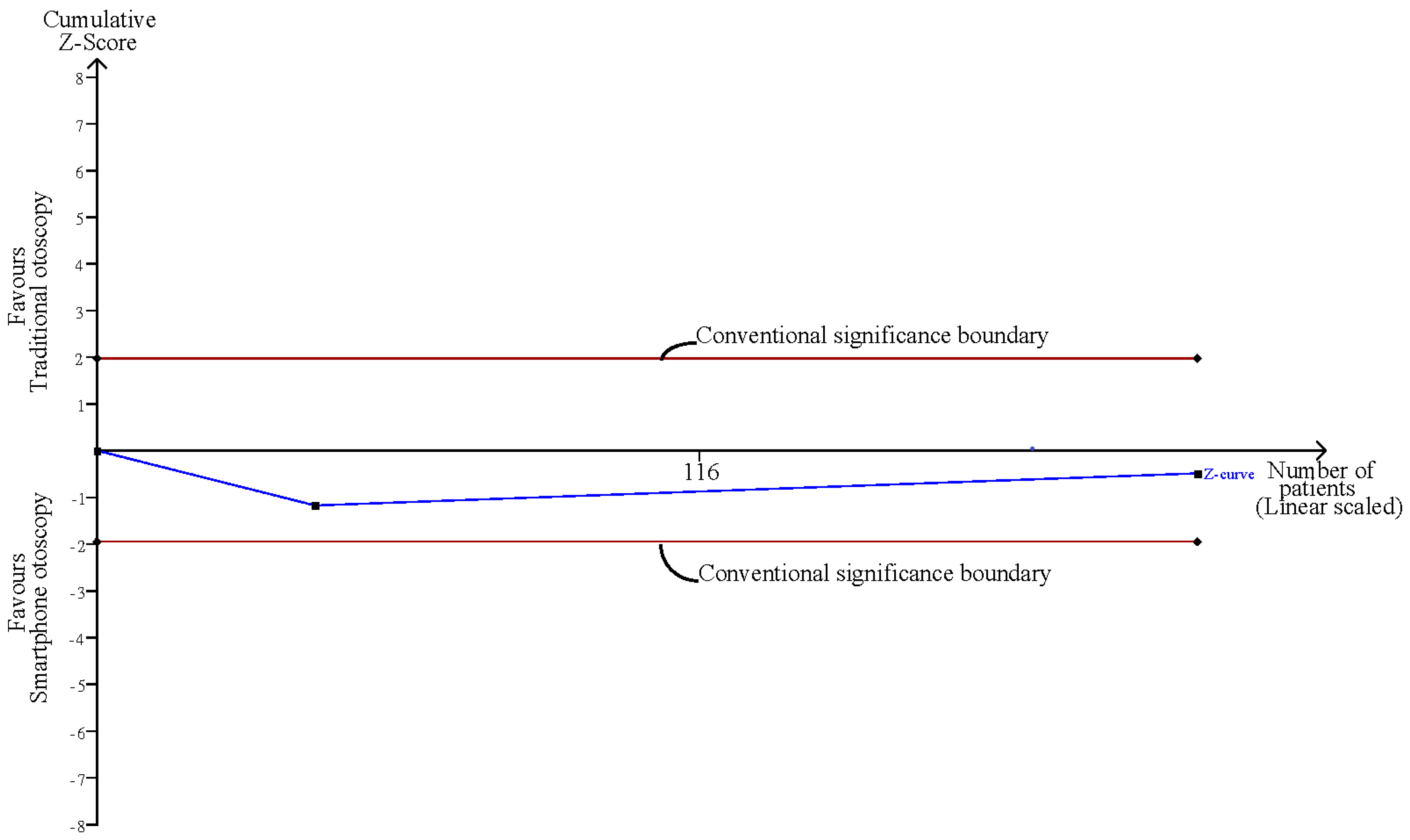
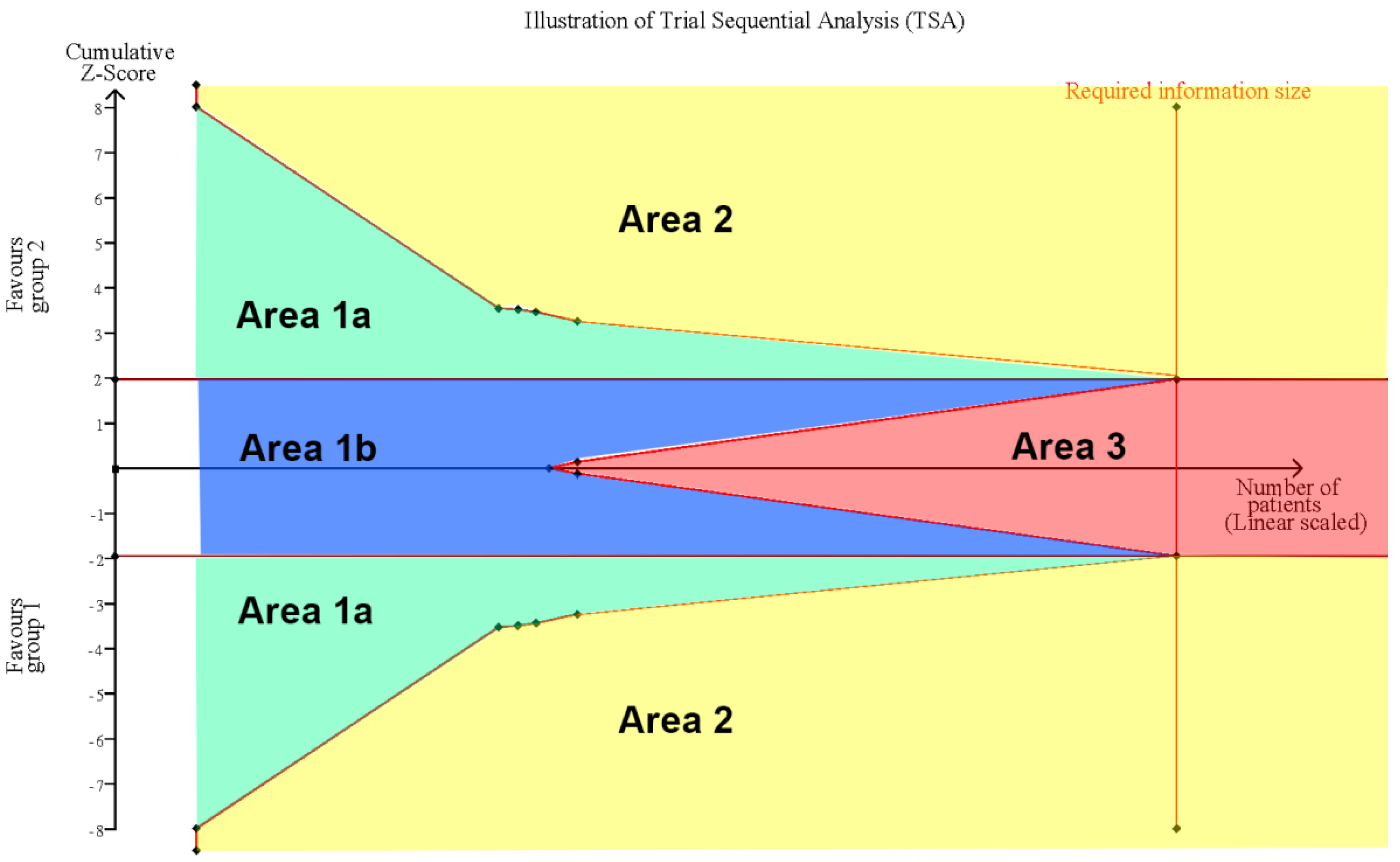
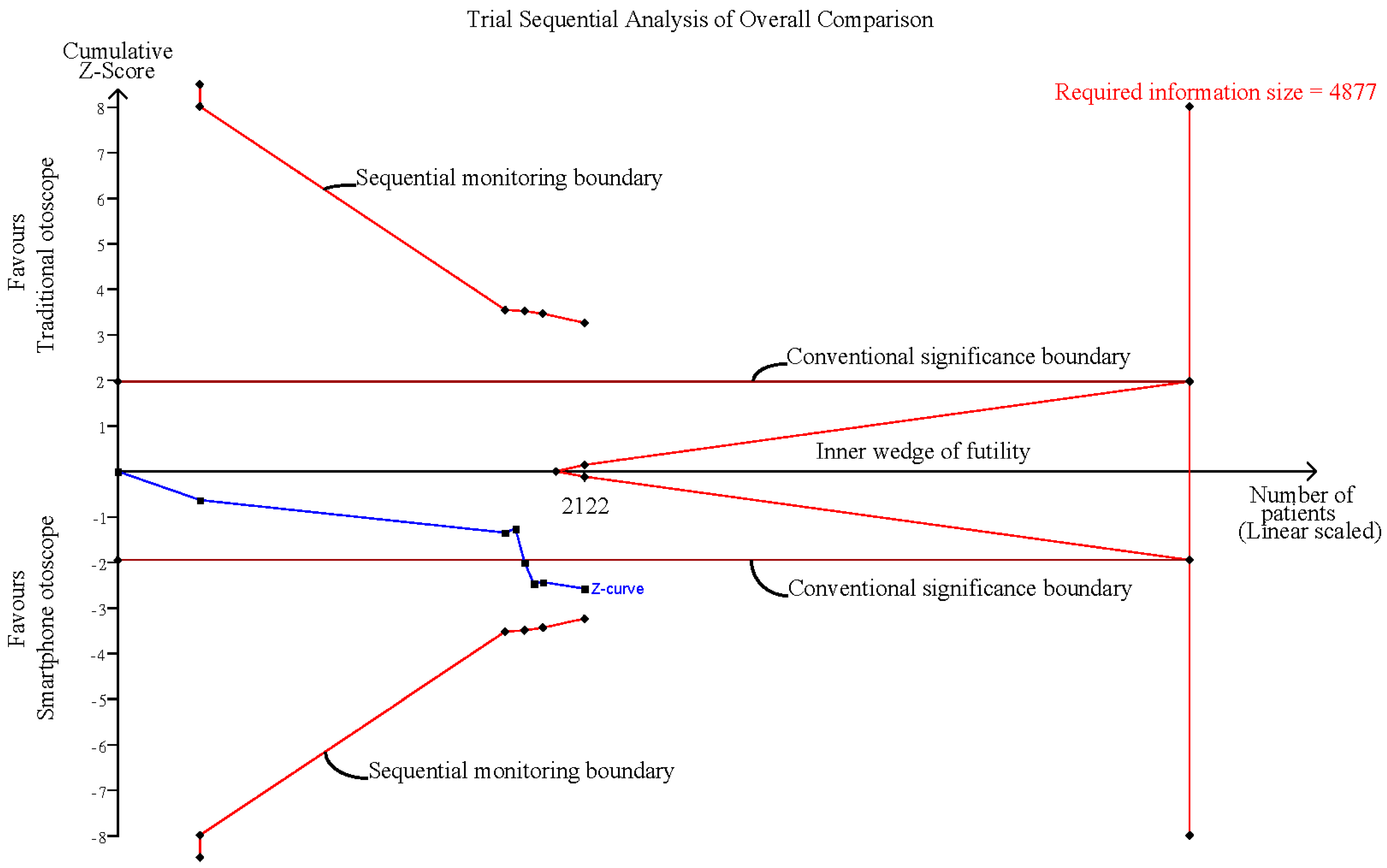
3.8. Influence Analysis and Trial Sequential Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- Rogers, D.J.; Boseley, M.E.; Adams, M.T.; Makowski, R.L.; Hohman, M.H. Prospective comparison of handheld pneumatic otoscopy, binocular microscopy, and tympanometry in identifying middle ear effusions in children. Int. J. Pediatr. Otorhinolaryngol. 2010, 74, 1140–1143. [Google Scholar] [CrossRef] [PubMed]
- Frithioff, A.; Guldager, M.J.; Andersen, S.A.W. Current Status of Handheld Otoscopy Training: A Systematic Review. Ann. Otol. Rhinol. Laryngol. 2021, 130, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- Guldager, M.J.; Melchiors, J.; Andersen, S.A.W. Development and Validation of an Assessment Tool for Technical Skills in Handheld Otoscopy. Ann. Otol. Rhinol. Laryngol. 2020, 129, 715–721. [Google Scholar] [CrossRef] [PubMed]
- von Buchwald, J.H.; Frendø, M.; Guldager, M.J.; Melchiors, J.; Andersen, S.A.W. Content validity evidence for a simulation-based test of handheld otoscopy skills. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 2313–2320. [Google Scholar] [CrossRef] [PubMed]
- Niermeyer, W.L.; Philips, R.H.W.; Essi, G.F., Jr.; Moberly, A.C. Diagnostic accuracy and confidence for otoscopy: Are medical students receiving sufficient training? Laryngoscope 2019, 129, 1891–1897. [Google Scholar] [CrossRef]
- Legros, J.M.; Hitoto, H.; Garnier, F.; Dagorne, C.; Parot-Schinkel, E.; Fanello, S. Clinical qualitative evaluation of the diagnosis of acute otitis media in general practice. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 23–30. [Google Scholar] [CrossRef]
- Rosenfeld, R.M. Diagnostic certainty for acute otitis media. Int. J. Pediatr. Otorhinolaryngol 2002, 64, 89–95. [Google Scholar] [CrossRef]
- Jones, W.S. Video otoscopy: Bringing otoscopy out of the “black box”. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1875–1883. [Google Scholar] [CrossRef]
- Richards, J.R.; Gaylor, K.A.; Pilgrim, A.J. Comparison of traditional otoscope to iPhone otoscope in the pediatric ED. Am. J. Emerg. Med. 2015, 33, 1089–1092. [Google Scholar] [CrossRef]
- Spiro, D.M.; Welker, M.A.; Arnold, D.H.; Meckler, G.D. A proposal to limit otoscopy to reduce unnecessary use of antibiotics: A call for research. Expert Rev. Anti-Infect. Ther. 2011, 9, 177–181. [Google Scholar] [CrossRef]
- Kleinman, K.; Psoter, K.J.; Nyhan, A.; Solomon, B.S.; Kim, J.M.; Canares, T. Evaluation of digital otoscopy in pediatric patients: A prospective randomized controlled clinical trial. Am. J. Emerg. Med. 2021, 46, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Binol, H.; Niazi, M.K.K.; Essig, G.; Shah, J.; Mattingly, J.K.; Harris, M.S.; Elmaraghy, C.; Teknos, T.; Taj-Schaal, N.; Yu, L.; et al. Digital Otoscopy Videos Versus Composite Images: A Reader Study to Compare the Accuracy of ENT Physicians. Laryngoscope 2021, 131, E1668–E1676. [Google Scholar] [CrossRef] [PubMed]
- Moberly, A.C.; Zhang, M.; Yu, L.; Gurcan, M.; Senaras, C.; Teknos, T.N.; Elmaraghy, C.A.; Taj-Schaal, N.; Essig, G.F. Digital otoscopy versus microscopy: How correct and confident are ear experts in their diagnoses? J. Telemed. Telecare 2017, 24, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Myburgh, H.C.; van Zijl, W.H.; Swanepoel, D.; Hellström, S.; Laurent, C. Otitis Media Diagnosis for Developing Countries Using Tympanic Membrane Image-Analysis. EBioMedicine 2016, 5, 156–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rappaport, K.M.; McCracken, C.C.; Beniflah, J.; Little, W.K.; Fletcher, D.A.; Lam, W.A.; Shane, A.L. Assessment of a Smartphone Otoscope Device for the Diagnosis and Management of Otitis Media. Clin. Pediatr. 2015, 55, 800–810. [Google Scholar] [CrossRef]
- Wallace, J.; Kanegaonkar, R. The role of smartphone applications in clinical practice: A review. J. Laryngol. Otol. 2020, 134, 96–103. [Google Scholar] [CrossRef]
- Cai, Y.; Zheng, Y.J.; Gulati, A.; Butrymowicz, A.; Krauter, R.; Pletcher, S.D.; Sharon, J.D.; Goldberg, A.N.; Chang, J.L. Patient Use of Low-cost Digital Videoscopes and Smartphones for Remote Ear and Oropharyngeal Examinations. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 336–342. [Google Scholar] [CrossRef]
- Bae, J.K.; Vavilin, A.; You, J.S.; Kim, H.; Ryu, S.Y.; Jang, J.H.; Jung, W. Smartphone-Based Endoscope System for Advanced Point-of-Care Diagnostics: Feasibility Study. JMIR Mhealth Uhealth 2017, 5, e99. [Google Scholar] [CrossRef]
- Williams, R.; Lee, J.D.E.; Muzaffar, J.; Clutton-Brock, T.; Coulson, C. Usability and Practicality of a Novel Mobile Attachment for Aural Endoscopy (endoscope-i): Formative Usability Study. JMIR Biomed Eng 2020, 5, e18850. [Google Scholar] [CrossRef]
- Wintergerst, M.W.M.; Jansen, L.G.; Holz, F.G.; Finger, R.P. A Novel Device for Smartphone-Based Fundus Imaging and Documentation in Clinical Practice: Comparative Image Analysis Study. JMIR Mhealth Uhealth 2020, 8, e17480. [Google Scholar] [CrossRef]
- Kim, A.J.; Yang, J.; Jang, Y.; Baek, J.S. Acceptance of an Informational Antituberculosis Chatbot Among Korean Adults: Mixed Methods Research. JMIR Mhealth Uhealth 2021, 9, e26424. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Mihai, C.; Tüshaus, L.; Scebba, G.; Distler, O.; Karlen, W. Wound Image Quality From a Mobile Health Tool for Home-Based Chronic Wound Management With Real-Time Quality Feedback: Randomized Feasibility Study. JMIR Mhealth Uhealth 2021, 9, e26149. [Google Scholar] [CrossRef] [PubMed]
- Keum, J.; Chung, M.J.; Kim, Y.; Ko, H.; Sung, M.J.; Jo, J.H.; Park, J.Y.; Bang, S.; Park, S.W.; Song, S.Y.; et al. Usefulness of Smartphone Apps for Improving Nutritional Status of Pancreatic Cancer Patients: Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e21088. [Google Scholar] [CrossRef] [PubMed]
- Książczyk, M.; Dębska-Kozłowska, A.; Warchoł, I.; Lubiński, A. Enhancing Healthcare Access–Smartphone Apps in Arrhythmia Screening: Viewpoint. JMIR Mhealth Uhealth 2021, 9, e23425. [Google Scholar] [CrossRef]
- Chen, C.-H.; Lin, H.-Y.H.; Wang, M.-C.; Chu, Y.-C.; Chang, C.-Y.; Huang, C.-Y.; Cheng, Y.-F. Diagnostic Accuracy of Smartphone-Based Audiometry for Hearing Loss Detection: Meta-analysis. JMIR Mhealth Uhealth 2021, 9, e28378. [Google Scholar] [CrossRef] [PubMed]
- Alexander, G.C.; Tajanlangit, M.; Heyward, J.; Mansour, O.; Qato, D.M.; Stafford, R.S. Use and Content of Primary Care Office-Based vs Telemedicine Care Visits During the COVID-19 Pandemic in the US. JAMA Netw. Open 2020, 3, e2021476. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.E.; Rathi, V.K.; Kozin, E.D.; Naunheim, M.R.; Xiao, R.; Gray, S.T. Telemedicine Services Provided to Medicare Beneficiaries by Otolaryngologists Between 2010 and 2018. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 816–821. [Google Scholar] [CrossRef]
- Patel, S.Y.; Mehrotra, A.; Huskamp, H.A.; Uscher-Pines, L.; Ganguli, I.; Barnett, M.L. Trends in Outpatient Care Delivery and Telemedicine During the COVID-19 Pandemic in the US. JAMA Intern. Med. 2021, 181, 388–391. [Google Scholar] [CrossRef]
- Prasad, A.; Brewster, R.; Newman, J.G.; Rajasekaran, K. Optimizing your telemedicine visit during the COVID-19 pandemic: Practice guidelines for patients with head and neck cancer. Head Neck 2020, 42, 1317–1321. [Google Scholar] [CrossRef]
- Yordanov, Y.; Dechartres, A.; Lescure, X.; Apra, C.; Villie, P.; Marchand-Arvier, J.; Debuc, E.; Dinh, A.; Jourdain, P. Covidom, a Telesurveillance Solution for Home Monitoring Patients With COVID-19. J. Med. Internet Res. 2020, 22, e20748. [Google Scholar] [CrossRef]
- Dron, L.; Dillman, A.; Zoratti, M.J.; Haggstrom, J.; Mills, E.J.; Park, J.J.H. Clinical Trial Data Sharing for COVID-19–Related Research. J. Med. Internet Res. 2021, 23, e26718. [Google Scholar] [CrossRef] [PubMed]
- Schweiberger, K.; Hoberman, A.; Iagnemma, J.; Schoemer, P.; Squire, J.; Taormina, J.; Wolfson, D.; Ray, K.N. Practice-Level Variation in Telemedicine Use in a Pediatric Primary Care Network During the COVID-19 Pandemic: Retrospective Analysis and Survey Study. J. Med. Internet Res. 2020, 22, e24345. [Google Scholar] [CrossRef] [PubMed]
- Feldman, J.; Szerencsy, A.; Mann, D.; Austrian, J.; Kothari, U.; Heo, H.; Barzideh, S.; Hickey, M.; Snapp, C.; Aminian, R.; et al. Giving Your Electronic Health Record a Checkup After COVID-19: A Practical Framework for Reviewing Clinical Decision Support in Light of the Telemedicine Expansion. JMIR Med Inf. 2021, 9, e21712. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Huang, S.; Qiu, C.; Liu, S.; Deng, J.; Jiao, B.; Tan, X.; Ai, L.; Xiao, Y.; Belliato, M.; et al. Monitoring and Management of Home-Quarantined Patients With COVID-19 Using a WeChat-Based Telemedicine System: Retrospective Cohort Study. J. Med. Internet Res. 2020, 22, e19514. [Google Scholar] [CrossRef] [PubMed]
- Moshtaghi, O.; Sahyouni, R.; Haidar, Y.M.; Huang, M.; Moshtaghi, A.; Ghavami, Y.; Lin, H.W.; Djalilian, H.R. Smartphone-Enabled Otoscopy in Neurotology/Otology. Otolaryngol. Head Neck Surg. 2017, 156, 554–558. [Google Scholar] [CrossRef] [Green Version]
- Hakimi, A.A.; Lalehzarian, A.S.; Lalehzarian, S.P.; Azhdam, A.M.; Nedjat-Haiem, S.; Boodaie, B.D. Utility of a smartphone-enabled otoscope in the instruction of otoscopy and middle ear anatomy. Eur. Arch. Otorhinolaryngol. 2019, 276, 2953–2956. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Trial Sequential Analysis Software. Copenhagen Trial Unit, C.f.C.I.R., Rigshospitalet, Copenhagen. 2016. Available online: http://www.ctu.dk/tsa/ (accessed on 2 January 2022.).
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 39. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.N.; Silverstein, A.; Bryan, L.N.; McCracken, C.E.; Little, W.K.; Shane, A.L. Comparison of a Smartphone Otoscope and Conventional Otoscope in the Diagnosis and Management of Acute Otitis Media. Clin. Pediatr. 2019, 58, 302–306. [Google Scholar] [CrossRef]
- Mousseau, S.; Lapointe, A.; Gravel, J. Diagnosing acute otitis media using a smartphone otoscope; a randomized controlled trial. Am. J. Emerg. Med. 2018, 36, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- Schuster-Bruce, J.R.; Ali, A.; Van, M.; Rogel-Salazar, J.; Ofo, E.; Shamil, E. A randomised trial to assess the educational benefit of a smartphone otoscope in undergraduate medical training. Eur. Arch. Otorhinolaryngol. 2021, 278, 1799–1804. [Google Scholar] [CrossRef] [PubMed]
- Powell, J.; Cooles, F.A.; Carrie, S.; Paleri, V. Is undergraduate medical education working for ENT surgery? A survey of UK medical school graduates. J. Laryngol. Otol. 2011, 125, 896–905. [Google Scholar] [CrossRef] [PubMed]
- Jones, W.S.; Kaleida, P.H.; Lopreiato, J.O. Assessment of pediatric residents’ otoscopic interpretive skills by videotaped examinations. Ambul. Pediatr. 2004, 4, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Doshi, J.; Carrie, S. A survey of undergraduate otolaryngology experience at Newcastle University Medical School. J. Laryngol. Otol. 2006, 120, 770–773. [Google Scholar] [CrossRef] [PubMed]
- Hu, A.; Sardesai, M.G.; Meyer, T.K. A need for otolaryngology education among primary care providers. Med. Educ. Online 2012, 17, 17350. [Google Scholar] [CrossRef]
- Blomgren, K.; Pitkäranta, A. Is it possible to diagnose acute otitis media accurately in primary health care? Fam. Pract. 2003, 20, 524–527. [Google Scholar] [CrossRef]
- Damery, L.; Lescanne, E.; Reffet, K.; Aussedat, C.; Bakhos, D. Interest of video-otoscopy for the general practitioner. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 13–17. [Google Scholar] [CrossRef]
- Tötterman, M.; Jukarainen, S.; Sinkkonen, S.T.; Klockars, T. A Comparison of Four Digital Otoscopes in a Teleconsultation Setting. Laryngoscope 2020, 130, 1572–1576. [Google Scholar] [CrossRef]
- Cha, D.; Shin, S.H.; Kim, J.; Eo, T.S.; Na, G.; Bae, S.; Jung, J.; Kim, S.H.; Moon, I.S.; Choi, J.; et al. Feasibility of Asynchronous and Automated Telemedicine in Otolaryngology: Prospective Cross-Sectional Study. JMIR Med. Inf. 2020, 8, e23680. [Google Scholar] [CrossRef]
- Don, D.M.; Koempel, J.A.; Fisher, L.M.; Wee, C.P.; Osterbauer, B. Prospective Evaluation of a Smartphone Otoscope for Home Tympanostomy Tube Surveillance: A Pilot Study. Ann. Otol. Rhinol. Laryngol. 2020, 130, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Steinhubl, S.R.; Muse, E.D.; Topol, E.J. Can Mobile Health Technologies Transform Health Care? JAMA 2013, 310, 2395–2396. [Google Scholar] [CrossRef] [PubMed]
- Ohlstein, J.F.; Garner, J.; Takashima, M. Telemedicine in Otolaryngology in the COVID-19 Era: Initial Lessons Learned. Laryngoscope 2020, 130, 2568–2573. [Google Scholar] [CrossRef] [PubMed]
- Yuan, N.; Pevnick, J.M.; Botting, P.G.; Elad, Y.; Miller, S.J.; Cheng, S.; Ebinger, J.E. Patient Use and Clinical Practice Patterns of Remote Cardiology Clinic Visits in the Era of COVID-19. JAMA Netw. Open 2021, 4, e214157. [Google Scholar] [CrossRef]
- Garbutt, J.; Jeffe, D.B.; Shackelford, P. Diagnosis and Treatment of Acute Otitis Media: An Assessment. Pediatrics 2003, 112, 143. [Google Scholar] [CrossRef]
- Ren, Y.; Sethi, R.K.V.; Stankovic, K.M. Acute Otitis Media and Associated Complications in United States Emergency Departments. Otol. Neurotol. 2018, 39, 1005–1011. [Google Scholar] [CrossRef]
- Bluestone, C.D. Clinical course, complications and sequelae of acute otitis media. Pediatr. Infect. Dis. J. 2000, 19, S37–S46. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Type | Country | Setting | Ear Condition | Sample (Smartphone/Traditional) | Event Rate (Event/Total) | Mean Age of Examinee (SD) | Level of Examiner | Smartphone-Enabled Otoscopy | Operating System of Smartphone |
|---|---|---|---|---|---|---|---|---|---|---|
| Kleinman et al. [11] 2021 | RCT | USA | ED | AOM | 188 (92/96) | Smartphone group: 69/92 | 6.25 year (3.84) | Resident: 91% (171) Medical student: 9% (17) | CellScope Oto | iOS |
| Traditional group: 61/96 | ||||||||||
| Chan et al. [41] 2019 | RCT | USA | ED | AOM | 1390 (614/776) | Smartphone group: 123/614 | 46.79 month (40.68) | Resident | CellScope Oto | iOS |
| Traditional group: 146/776 | ||||||||||
| Mousseau et al. [42] 2018 | RCT | Canada | ED | AOM | 94 * (188/188) | Smartphone group: 140/188 | 2.25 year (0.61) | Resident | CellScope Oto | iOS |
| Traditional group: 129/188 | ||||||||||
| Schuter-Bruce et al. [43] 2020 | RCT | UK | Simulation | AOM | 42 (20/22) | Smartphone group: 15/20 | Not applicable | Medical student | TYMPA smartphone otoscope | iOS |
| Traditional group: 5/22 | ||||||||||
| Perforation | 42 (20/22) | Smartphone group: 13/20 | ||||||||
| Traditional group: 3/22 | ||||||||||
| VTI | 42 (20/22) | Smartphone group: 20/20 | ||||||||
| Traditional group: 20/22 | ||||||||||
| Normal | 42 (20/22) | Smartphone group: 19/20 | ||||||||
| Traditional group: 11/22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Huang, C.-Y.; Cheng, H.-L.; Lin, H.-Y.H.; Chu, Y.-C.; Chang, C.-Y.; Lai, Y.-H.; Wang, M.-C.; Cheng, Y.-F. Smartphone-Enabled versus Conventional Otoscopy in Detecting Middle Ear Disease: A Meta-Analysis. Diagnostics 2022, 12, 972. https://doi.org/10.3390/diagnostics12040972
Chen C-H, Huang C-Y, Cheng H-L, Lin H-YH, Chu Y-C, Chang C-Y, Lai Y-H, Wang M-C, Cheng Y-F. Smartphone-Enabled versus Conventional Otoscopy in Detecting Middle Ear Disease: A Meta-Analysis. Diagnostics. 2022; 12(4):972. https://doi.org/10.3390/diagnostics12040972
Chicago/Turabian StyleChen, Chih-Hao, Chii-Yuan Huang, Hsiu-Lien Cheng, Heng-Yu Haley Lin, Yuan-Chia Chu, Chun-Yu Chang, Ying-Hui Lai, Mao-Che Wang, and Yen-Fu Cheng. 2022. "Smartphone-Enabled versus Conventional Otoscopy in Detecting Middle Ear Disease: A Meta-Analysis" Diagnostics 12, no. 4: 972. https://doi.org/10.3390/diagnostics12040972
APA StyleChen, C.-H., Huang, C.-Y., Cheng, H.-L., Lin, H.-Y. H., Chu, Y.-C., Chang, C.-Y., Lai, Y.-H., Wang, M.-C., & Cheng, Y.-F. (2022). Smartphone-Enabled versus Conventional Otoscopy in Detecting Middle Ear Disease: A Meta-Analysis. Diagnostics, 12(4), 972. https://doi.org/10.3390/diagnostics12040972