
Usefulness of 3D CT/MRI Fusion Imaging for the Evaluation of Lumbar Disc Herniation and Kambin’s Triangle


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
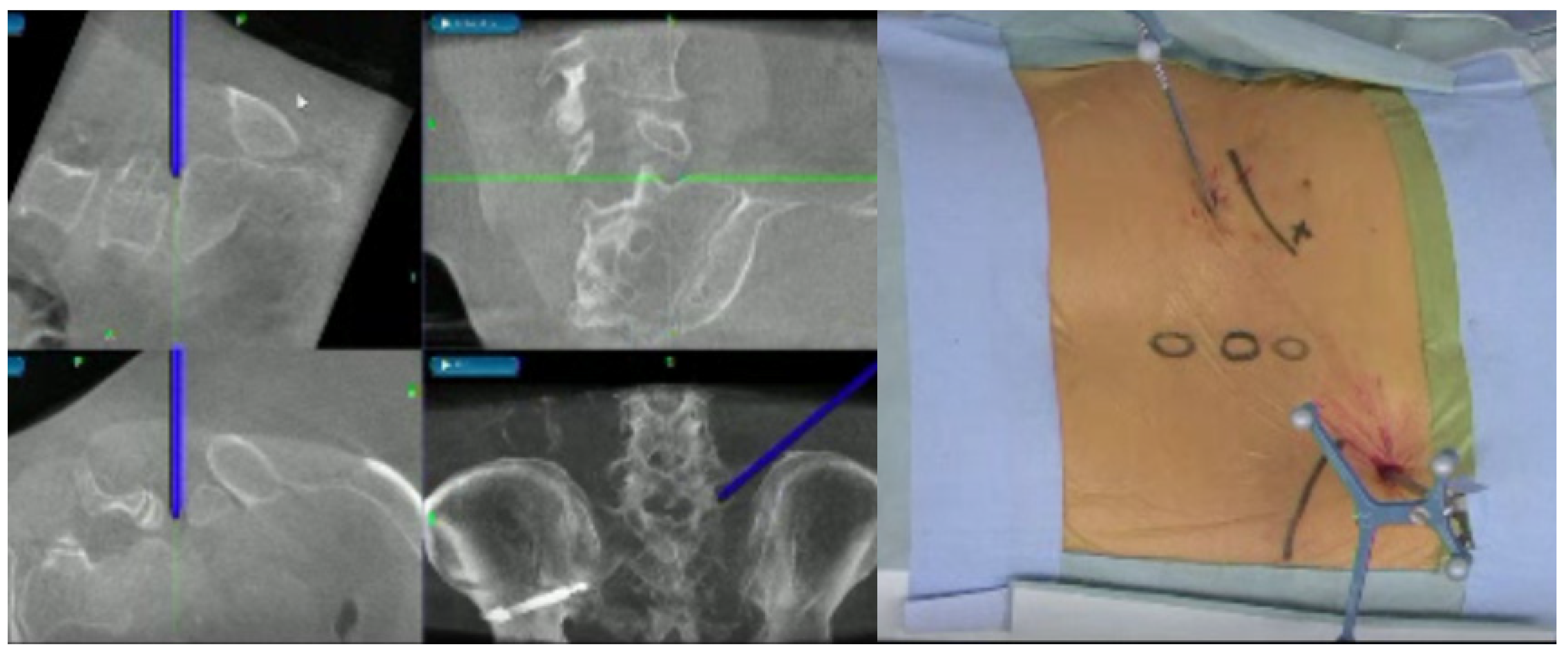
2.2. Image Technique
2.3. CT-MRI Fusion Image
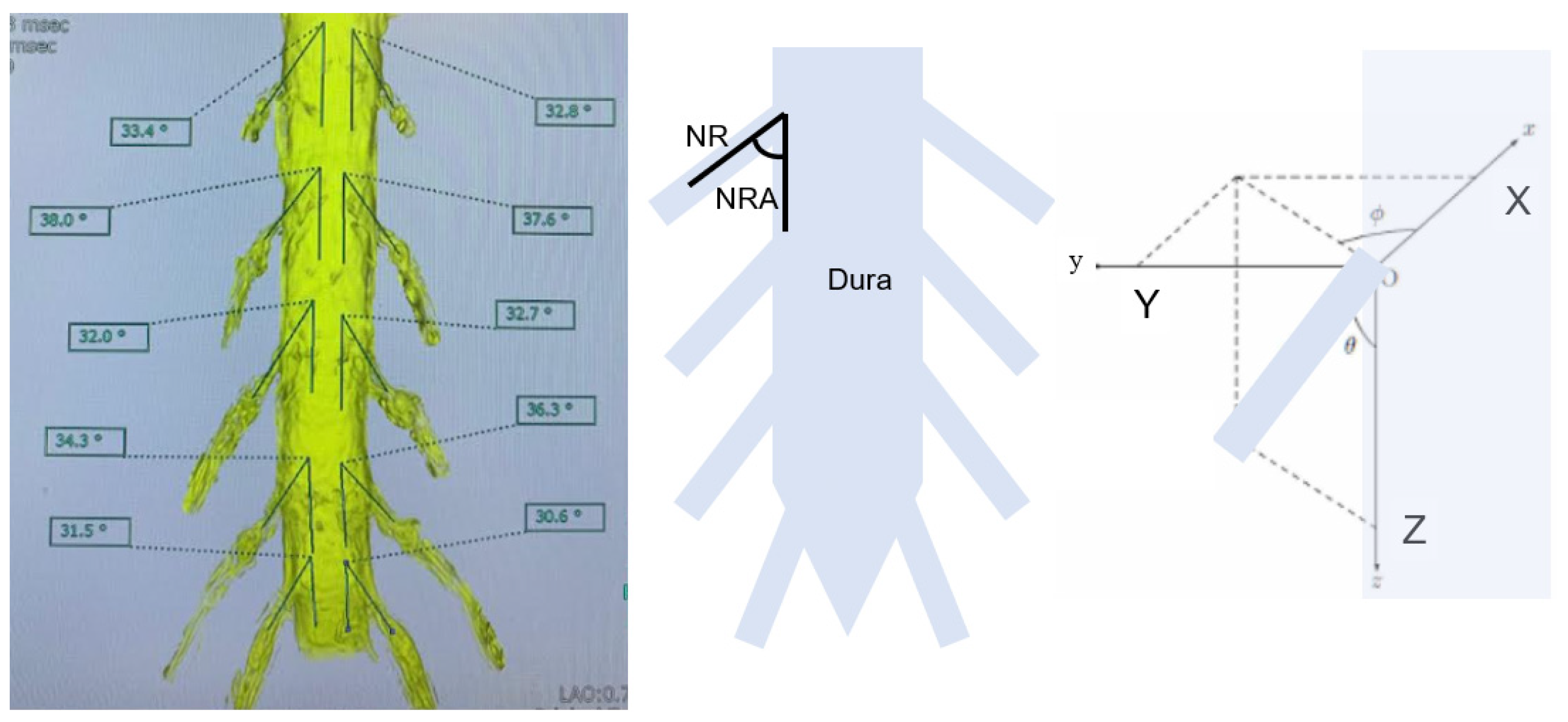
2.4. Evaluation of Merged Images
2.5. Statistical Analysis
3. Results
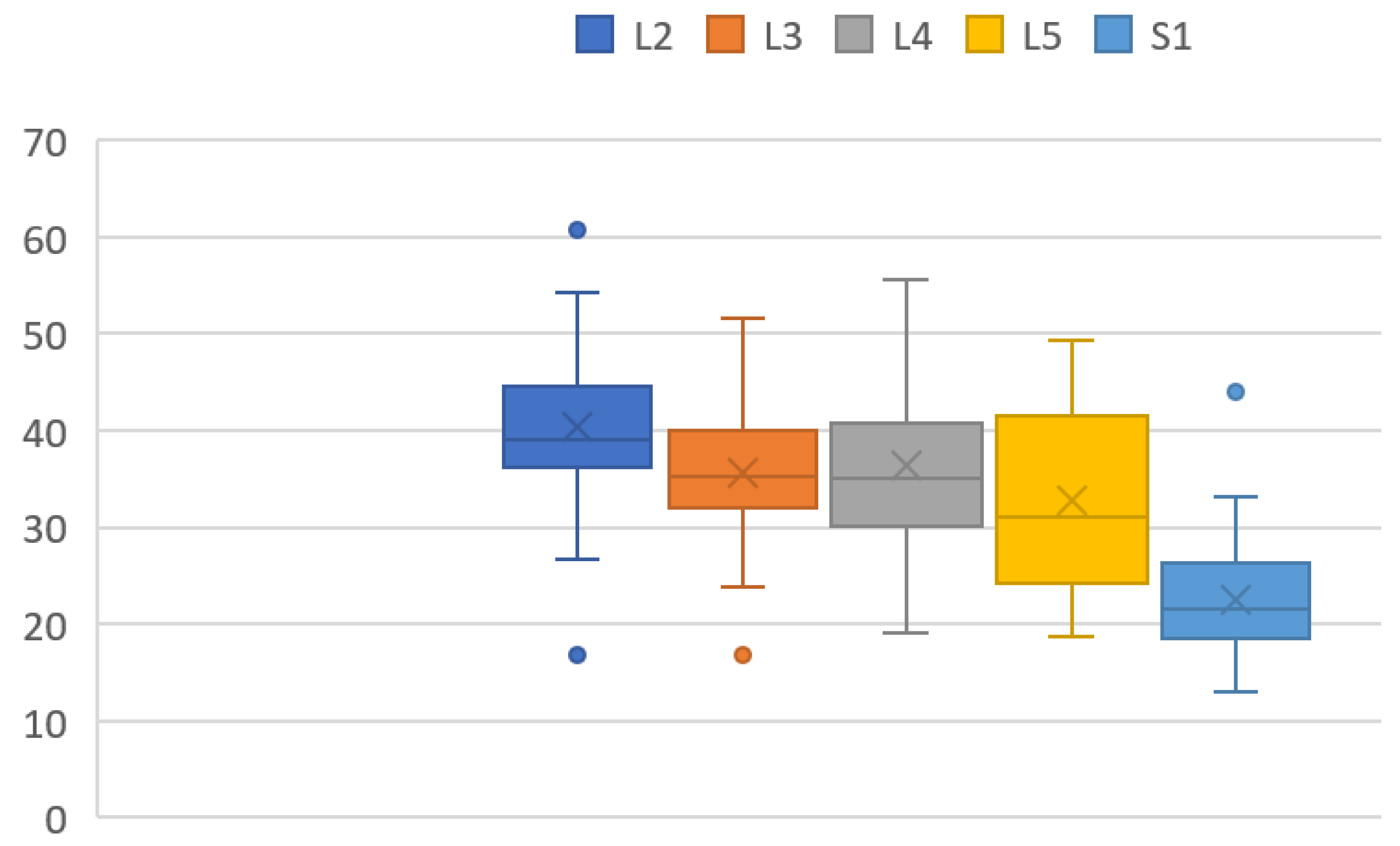
3.1. 3-D Nerve Root Angle (3DNRA)
3.2. Superior Articular Process to Exiting Nerve Distance (SAP-ENR Distance)
3.3. Possible Needle (1 mm) Passage at 60° and 45°
3.4. Possible Dilater (5 mm) Passage at 60° and 45°
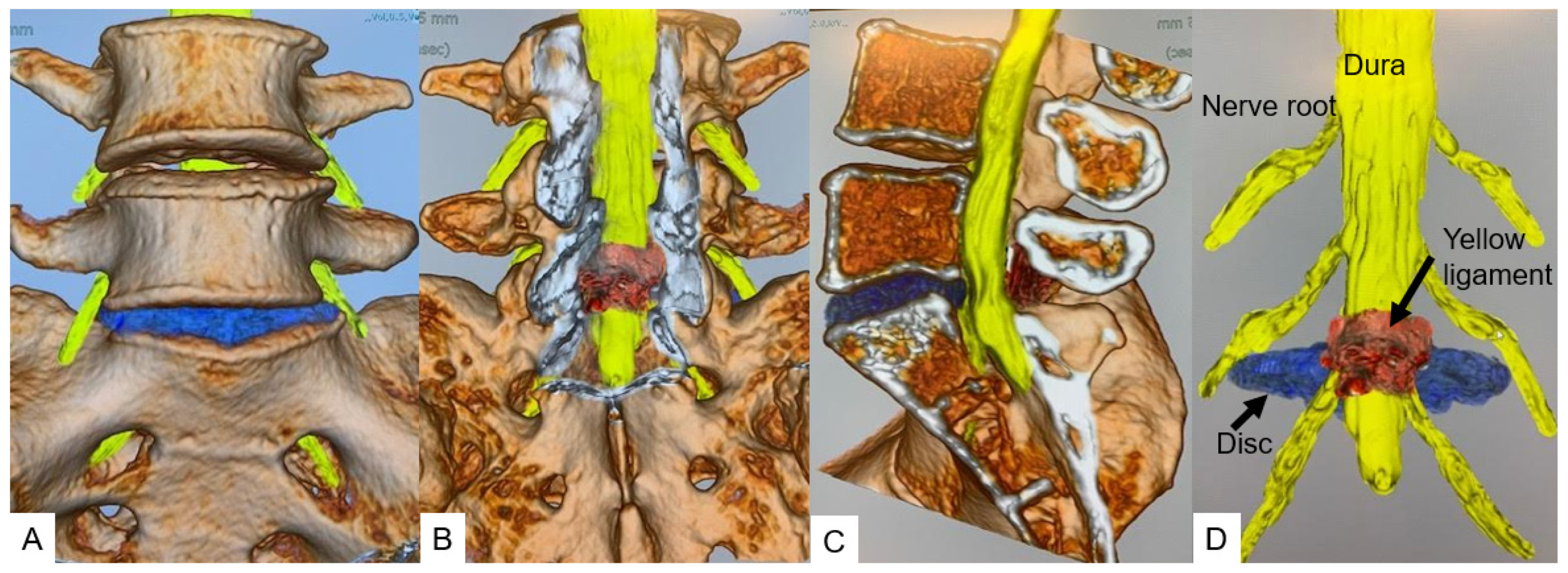
3.5. Herniated Disc Visualization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yeung, A.T.; Tsou, P.M. Posterolateral endoscopic excision for lumbar disc herniation: Surgical technique, outcome, and complications in 307 consecutive cases. Spine 2022, 27, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Kolcun, J.P.G.; Brusko, G.D.; Basil, G.W.; Epstein, R.; Wang, M.Y. Endoscopic transforaminal lumbar interbody fusion without general anesthesia: Operative and clinical outcomes in 100 consecutive patients with a minimum 1-year follow-up. Neurosurg. Focus 2019, 46, E14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kambin, P.; Sampson, S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs. Report of interim results. Clin. Orthop. Relat. Res. 1986, 207, 37–43. [Google Scholar] [CrossRef]
- Choi, I.; Ahn, J.O.; So, W.S.; Lee, S.J.; Choi, I.J.; Kim, H. Exiting root injury in transforaminal endoscopic discectomy: Preoperative image considerations for safety. Eur. Spine J. 2013, 22, 2481–2487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, P.; Zhang, Y.; Pan, A.; Ding, Y.; Zhang, L.; Xu, C.; Yang, J.; Hai, Y. The feasibility for a novel minimally invasive surgery-percutaneous endoscopic transforaminal lumbar interbody fusion (PE-TLIF) for the treatment of lumbar degenerative diseases: A cadaveric experiment. J. Orthop. Surg. Res. 2020, 15, 387. [Google Scholar] [CrossRef]
- Ozer, A.F.; Suzer, T.; Can, H.; Falsafi, M.; Aydin, M.; Sasani, M.; Oktenoglu, T. Anatomic Assessment of Variations in Kambin’s Triangle: A Surgical and Cadaver Study. World Neurosurg. 2017, 100, 498–503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pairaiturkar, P.P.; Sudame, O.S.; Pophale, C.S. Evaluation of Dimensions of Kambin’s Triangle to Calculate Maximum Permissible Cannula Diameter for Percutaneous Endoscopic Lumbar Discectomy: A 3-Dimensional Magnetic Resonance Imaging Based Study. J. Korean Neurosurg. Soc. 2019, 62, 414–421. [Google Scholar] [CrossRef]
- Aoyama, R.; Anazawa, U.; Hotta, H.; Watanabe, I.; Takahashi, Y.; Matsumoto, S. The Utility of Augmented Reality in Spinal Decompression Surgery Using CT/MRI Fusion Image. Cureus 2021, 13, e18187. [Google Scholar] [CrossRef]
- Nagamatsu, M.; Ruparel, S.; Tanaka, M.; Fujiwara, Y.; Uotani, K.; Arataki, S.; Yamauchi, T.; Takeshita, Y.; Takamoto, R.; Tanaka, M.; et al. Assessment of 3D Lumbosacral Vascular Anatomy for OLIF51 by Non-Enhanced MRI and CT Medical Image Fusion Technique. Diagnostics 2021, 11, 1744. [Google Scholar] [CrossRef]
- Dandy, W.E. Loose cartilage from intervertebral disk simulating tumor of the spinal cord. Clin. Orthop. Relat. Res. 1989, 238, 4–8. [Google Scholar] [CrossRef]
- Yamada, K.; Nagahama, K.; Abe, Y.; Hyugaji, Y.; Takahata, M.; Iwasaki, N. Morphological analysis of Kambin’s triangle using 3D CT/MRI fusion imaging of lumbar nerve root created automatically with artificial intelligence. Eur. Spine J. 2021, 30, 2191–2199. [Google Scholar] [CrossRef] [PubMed]
- Nagahama, K.; Ito, M.; Abe, Y.; Murota, E.; Hiratsuka, S.; Takahata, M. Early clinical results of percutaneous endoscopic transforaminal lumbar interbody fusion: A new modifed technique for treating degenerative lumbar spondylolisthesis. Spine Surg. Relat. Res. 2019, 3, 327–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, P.H.; Kim, H.S.; Jang, I.T. A Narrative Review of Development of Full-Endoscopic Lumbar Spine Surgery. Neurospine 2020, 17 (Suppl. 1), S20–S33. [Google Scholar] [CrossRef]
- Kim, H.S.; Raorane, H.D.; Wu, P.H.; Yi, Y.J.; Jang, I.T. Evolution of endoscopic transforaminal lumbar approach for degenerative lumbar disease. J. Spine Surg. 2020, 6, 424–437. [Google Scholar] [CrossRef] [PubMed]
- Fanous, A.A.; Tumialán, L.M.; Wang, M.Y. Kambin’s triangle: Definition and new classification schema. J. Neurosurg. Spine 2019, 32, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Mikawa, Y.; Watanabe, R.; An, H.S. Morphometric analysis of the lumbosacral nerve roots and dorsal root ganglia by magnetic resonance imaging. Spine 1996, 21, 1005–1009. [Google Scholar] [CrossRef] [PubMed]
- Min, J.H.; Kang, S.H.; Lee, J.B.; Cho, T.H.; Suh, J.K.; Rhyu, I.J. Morphometric analysis of the working zone for endoscopic lumbar discectomy. J. Spinal Disord. Tech. 2005, 18, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yang, J.; Hai, Y.; Yin, P.; Ding, Y.; Xu, C.; Gao, H. Relationship of the exiting nerve root and superior articular process in Kambin’s triangle: Assessment of lumbar anatomy using cadavers and computed tomography imaging. World Neurosurg. 2020, 137, e336–e342. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Ma, X.; Zhao, D.; Yang, H.; Xu, B.; Wang, Z.; Yang, Q. Full Endoscopic Lumbar Foraminoplasty with Periendoscopic Visualized Trephine Technique for Lumbar Disc Herniation with Migration and/or Foraminal or Lateral Recess Stenosis. World Neurosurg. 2021, 148, e658–e666. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.P.; Wang, S.L.; Hu, W.X.; Chen, B.L.; Du, Y.X.; Zhao, S.; Rao, S.Y.; Su, G.Y.; Lin, R.; Chen, S.; et al. Percutaneous Full-Endoscopic Lumbar Foraminoplasty and Decompression by Using a Visualization Reamer for Lumbar Lateral Recess and Foraminal Stenosis in Elderly Patients. World Neurosurg. 2020, 136, e83–e89. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N = 23 | |
|---|---|
| Gender (male:female) | 10:13 |
| Age (mean ± S.D.) (year) | 58.2 ± 18.2 |
| Height (mean ± S.D.) (cm) | 160.6 ± 11.2 |
| Body weight (mean ± S.D.) (kg) | 63.5 ± 16.3 |
| Body mass index (mean ± S.D.) (kg/m2) | 24.4 ± 4.2 |
| Disc Level | Angle of Rotation (°) | Right (mm) | Left (mm) | Mean (mm) |
|---|---|---|---|---|
| L2/3 | 45 | 4.9 ± 2.3 | 5.7 ± 2.7 | 5.3 ± 2.5 |
| L2/3 | 60 | 3.9 ± 2.0 | 4.3 ± 2.4 | 4.1 ± 2.1 |
| L3/4 | 45 | 4.3 ± 2.3 | 4.3 ± 2.0 | 4.3 ± 2.3 |
| L3/4 | 60 | 4.0 ± 2.8 | 3.7 ± 2.2 | 3.8 ± 2.4 |
| L4/5 | 45 | 6.4 ± 3.9 | 7.1 ± 4.0 | 6.8 ± 4.0 |
| L4/5 | 60 | 5.6 ± 3.8 | 6.1 ± 3.6 | 5.9 ± 3.6 |
| Disc Level | Angle of Rotation (°) | Needle Passage (%) | Dilater Passage (%) |
|---|---|---|---|
| L2/3 | 45 | 96.7 |  |
| L2/3 | 60 | 89.1 | |
| L3/4 | 45 | 89.1 | |
| L3/4 | 60 | 87.0 | |
| L4/5 | 45 | 94.5 | |
| L4/5 | 60 | 84.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagamatsu, M.; Maste, P.; Tanaka, M.; Fujiwara, Y.; Arataki, S.; Yamauchi, T.; Takeshita, Y.; Takamoto, R.; Torigoe, T.; Tanaka, M.; et al. Usefulness of 3D CT/MRI Fusion Imaging for the Evaluation of Lumbar Disc Herniation and Kambin’s Triangle. Diagnostics 2022, 12, 956. https://doi.org/10.3390/diagnostics12040956
Nagamatsu M, Maste P, Tanaka M, Fujiwara Y, Arataki S, Yamauchi T, Takeshita Y, Takamoto R, Torigoe T, Tanaka M, et al. Usefulness of 3D CT/MRI Fusion Imaging for the Evaluation of Lumbar Disc Herniation and Kambin’s Triangle. Diagnostics. 2022; 12(4):956. https://doi.org/10.3390/diagnostics12040956
Chicago/Turabian StyleNagamatsu, Masakazu, Praful Maste, Masato Tanaka, Yoshihiro Fujiwara, Shinya Arataki, Taro Yamauchi, Yoshiyuki Takeshita, Rika Takamoto, Tsukasa Torigoe, Masato Tanaka, and et al. 2022. "Usefulness of 3D CT/MRI Fusion Imaging for the Evaluation of Lumbar Disc Herniation and Kambin’s Triangle" Diagnostics 12, no. 4: 956. https://doi.org/10.3390/diagnostics12040956
APA StyleNagamatsu, M., Maste, P., Tanaka, M., Fujiwara, Y., Arataki, S., Yamauchi, T., Takeshita, Y., Takamoto, R., Torigoe, T., Tanaka, M., Tanaka, R., & Moriue, S. (2022). Usefulness of 3D CT/MRI Fusion Imaging for the Evaluation of Lumbar Disc Herniation and Kambin’s Triangle. Diagnostics, 12(4), 956. https://doi.org/10.3390/diagnostics12040956