
MRI in Late-Onset Rasmussen Encephalitis: A Long-Term Follow-Up Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Radiological Analysis
3. Results
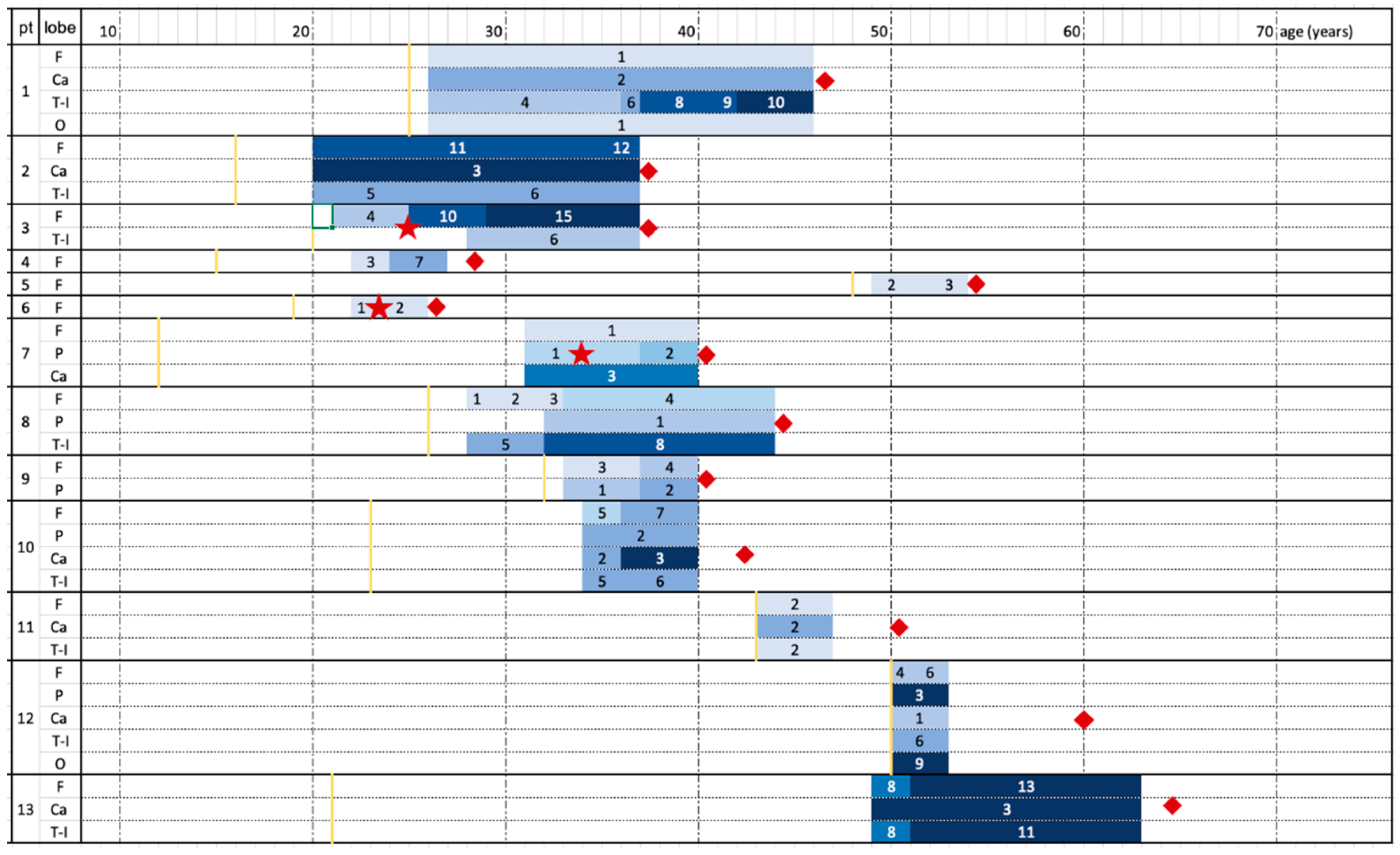
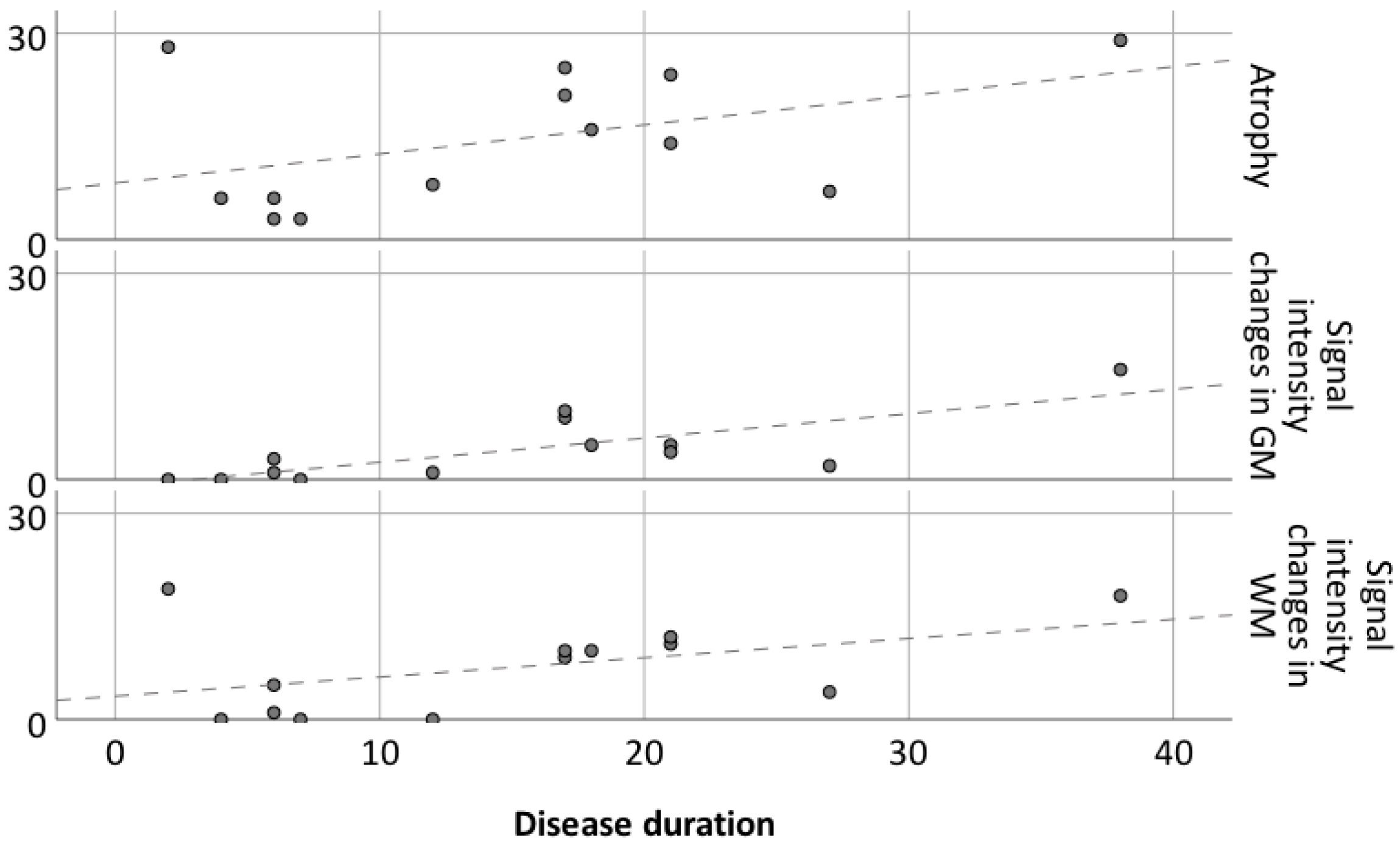
3.1. Atrophic Changes
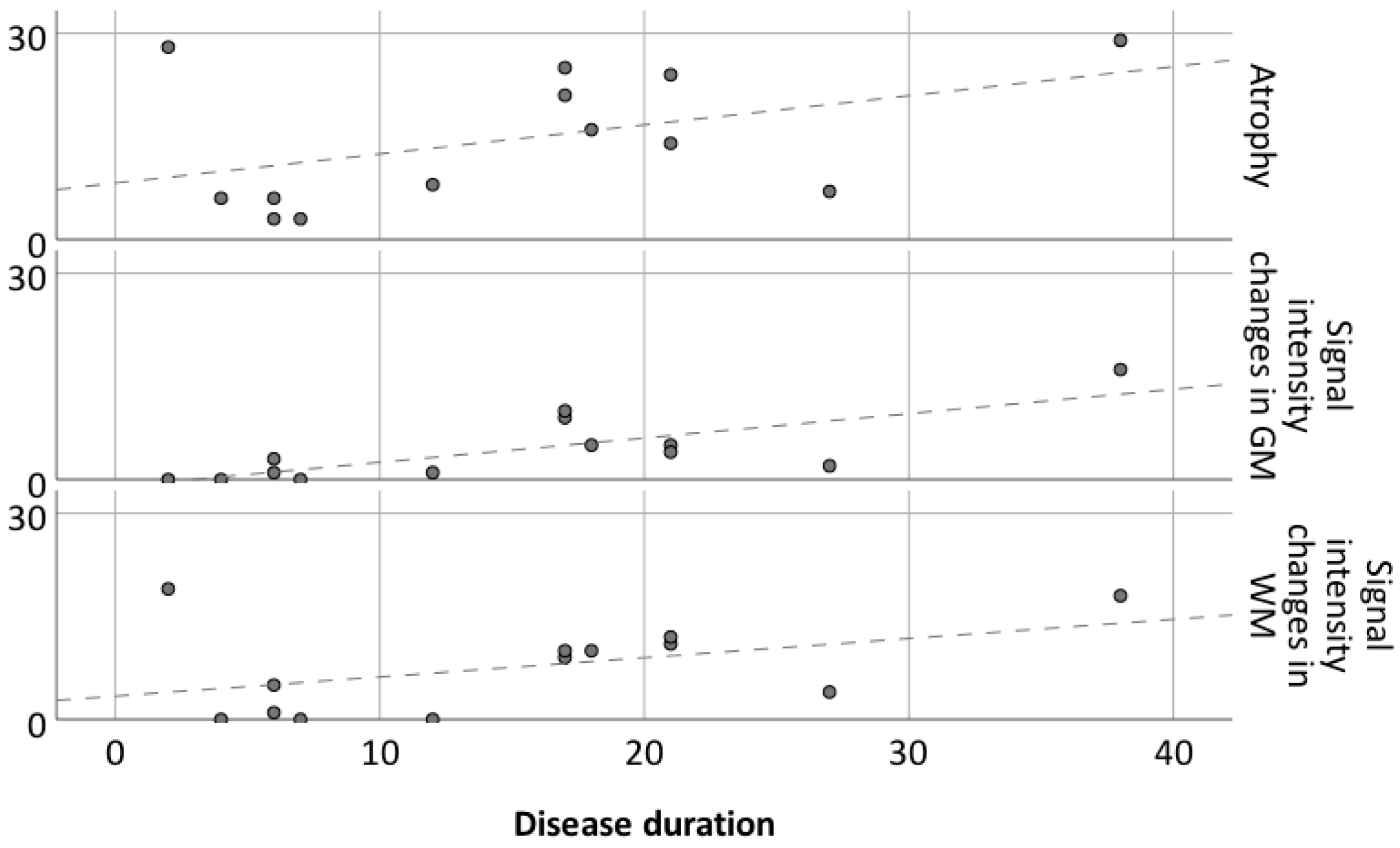
3.2. Changes in Signal Intensity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bien, C.G.; Tiemeier, H.; Sassen, R.; Kuczaty, S.; Urbach, H.; von Lehe, M.; Becker, A.J.; Bast, T.; Herkenrath, P.; Karenfort, M.; et al. Rasmussen encephalitis: Incidence and course under randomized therapy with tacrolimus or intravenous immunoglobulins. Epilepsia 2013, 54, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Hart, Y.M.; Andermann, F.; Fish, D.R.; Dubeau, F.; Robitaille, Y.; Rasmussen, T.; Berkovic, S.; Marino, R.; Yakoubian, E.M.; Spillane, K.; et al. Chronic encephalitis and epilepsy in adults and adolescents: A variant of Rasmussen’s syndrome? Neurology 1997, 48, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Villani, F.; Pincherle, A.; Antozzi, C.; Chiapparini, L.; Granata, T.; Michelucci, R.; Rubboli, G.; Simone, I.; Bellomo, R.; Spreafico, R. Adult-onset Rasmussen’s encephalitis: Anatomical-electrographic-clinical features of 7 Italian cases. Epilepsia 2006, 47, 41–46. [Google Scholar] [CrossRef]
- Deleo, F.; Matricardi, S.; Didato, G.; Pappalardo, I.; Villani, F. The dilemma of adult-onset Rasmussen encephalitis clinical assessment: Proposal for a new bedside tool to evaluate disease progression. Epilepsy Behav. 2015, 46, 249–251. [Google Scholar] [CrossRef]
- Rasmussen, T.; Olszewski, J.; Lloyd-Smith, D. Focal seizures due to chronic localized encephalitis. Neurology 1958, 8, 435. [Google Scholar] [CrossRef]
- Varadkar, S.; Bien, C.G.; Kruse, C.A.; Jensen, F.E.; Bauer, J.; Pardo, C.A.; Vincent, A.; Mathern, G.W.; Cross, J.H. Rasmussen’s encephalitis: Clinical features, pathobiology, and treatment advances. Lancet Neurol. 2014, 13, 195–205. [Google Scholar] [CrossRef] [Green Version]
- Pardo, C.A.; Vining, E.P.G.; Guo, L.; Skolasky, R.L.; Carson, B.S.; Freeman, J.M. The Pathology of Rasmussen Syndrome: Stages of Cortical Involvement and Neuropathological Studies in 45 Hemispherectomies. Epilepsia 2004, 45, 516–526. [Google Scholar] [CrossRef]
- Bien, C.G.; Bauer, J.; Deckwerth, T.L.; Wiendl, H.; Deckert, M.; Wiestler, O.D.; Schramm, J.; Elger, C.E.; Lassmann, H. Destruction of neurons by cytotoxic T cells: A new pathogenic mechanism in rasmussen’s encephalitis. Ann. Neurol. 2002, 51, 311–318. [Google Scholar] [CrossRef]
- Schwab, N.; Bien, C.G.; Waschbisch, A.; Becker, A.; Vince, G.H.; Dornmair, K.; Wiendl, H. CD8+ T-cell clones dominate brain infiltrates in Rasmussen encephalitis and persist in the periphery. Brain 2009, 132, 1236–1246. [Google Scholar] [CrossRef] [Green Version]
- Schneider-Hohendorf, T.; Mohan, H.; Bien, C.G.; Breuer, J.; Becker, A.; Görlich, D.; Kuhlmann, T.; Widman, G.; Herich, S.; Elpers, C.; et al. CD8(+) T-cell pathogenicity in Rasmussen encephalitis elucidated by large-scale T-cell receptor sequencing. Nat. Commun. 2016, 7, 11153. [Google Scholar] [CrossRef]
- Bien, C.G.; Granata, T.; Antozzi, C.; Cross, J.H.; Dulac, O.; Kurthen, M.; Lassman, H.; Mantegazza, R.; Villemure, J.G.; Spreafico, R.; et al. Pathogenesis, diagnosis and treatment of Rasmussen encephalitis: A European consensus statement. Brain 2005, 128, 454–471. [Google Scholar] [CrossRef] [Green Version]
- Gitlevich, T.; Lado, F.; Moshé, S. Kozhevnikov-Rasmussen Syndrome: A Historical Perspective Spanning Two Centuries. J. Pediatr. Epilepsy 2016, 5, 168–175. [Google Scholar] [CrossRef]
- Villani, F.; Spreafico, R.; Farina, L.; Giovagnoli, A.R.; Bernasconi, P.; Granata, T.; Avanzini, G. Positive response to immunomodulatory therapy in an adult patient with Rasmussen’s encephalitis. Neurology 2001, 56, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Bien, C.G.; Schramm, J. Treatment of Rasmussen encephalitis half a century after its initial description: Promising prospects and a dilemma. Epilepsy Res. 2009, 86, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Stabile, A.; Deleo, F.; Didato, G.; Pastori, C.; Antozzi, C.; de Curtis, M.; Villani, F. Adult-onset Rasmussen encephalitis treated with mitoxantrone. Eur. J. Neurol. 2018, 25, e125–e126. [Google Scholar] [CrossRef]
- Marras, C.E.; Granata, T.; Franzini, A.; Freri, E.; Villani, F.; Casazza, M.; De Curtis, M.; Ragona, F.; Ferroli, P.; D’Incerti, L.; et al. Hemispherotomy and functional hemispherectomy: Indications and outcome. Epilepsy Res. 2010, 89, 104–112. [Google Scholar] [CrossRef]
- Granata, T.; Matricardi, S.; Ragona, F.; Freri, E.; Casazza, M.; Villani, F.; Deleo, F.; Tringali, G.; Gobbi, G.; Tassi, L.; et al. Hemispherotomy in Rasmussen encephalitis: Long-term outcome in an Italian series of 16 patients. Epilepsy Res. 2014, 108, 1106–1119. [Google Scholar] [CrossRef]
- Villani, F.; Didato, G.; Deleo, F.; Tringali, G.; Garbelli, R.; Granata, T.; Marras, C.E.; Cordella, R.; Spreafico, R. Long-term outcome after limited cortical resections in two cases of adult-onset Rasmussen encephalitis. Epilepsia 2014, 55, e38–e43. [Google Scholar] [CrossRef]
- Chiapparini, L.; Granata, T.; Farina, L.; Ciceri, E.; Erbetta, A.; Ragona, F.; Freri, E.; Fusco, L.; Gobbi, G.; Capovilla, G.; et al. Diagnostic imaging in 13 cases of Rasmussen’s encephalitis: Can early MRI suggest the diagnosis? Neuroradiology 2003, 45, 171–183. [Google Scholar] [CrossRef]
- Kim, S.J.; Park, Y.D.; Pillai, J.J.; Lee, M.R.; Smith, J.R. A Longitudinal MRI Study in Children with Rasmussen Syndrome. Pediatr. Neurol. 2002, 27, 282–288. [Google Scholar] [CrossRef]
- Venkatesan, A.; Tunkel, A.R.; Bloch, K.C.; Lauring, A.S.; Sejvar, J.; Bitnun, A.; Stahl, J.P.; Mailles, A.; Drebot, M.; Rupprecht, C.E.; et al. Case definitions, diagnostic algorithms, and priorities in encephalitis: Consensus statement of the international encephalitis consortium. Clin. Infect. Dis. 2013, 57, 1114–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derry, C.; Dale, R.C.; Thom, M.; Miller, D.H.; Giovannoni, G. Unihemispheric cerebral vasculitis mimicking Rasmussen’s encephalitis. Neurology 2002, 58, 327. [Google Scholar] [CrossRef] [PubMed]
- Bien, C.G.; Widman, G.; Urbach, H.; Sassen, R.; Kuczaty, S.; Wiestler, O.D.; Schramm, J.; Elger, C.E. The natural history of Rasmussen’s encephalitis. Brain 2002, 125, 1751–1759. [Google Scholar] [CrossRef]
- Bhatjiwale, M.G.; Polkey, C.; Cox, T.C.; Dean, A.; Deasy, N. Rasmussen’s encephalitis: Neuroimaging findings in 21 patients with a closer look at the basal ganglia. Pediatr. Neurosurg. 1998, 29, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-C.; Weng, H.-H.; Tsai, Y.; Huang, Y.-C.; Hsiao, M.-C.; Wu, C.-Y.; Lin, Y.-H.; Hsu, H.-L.; Lee, J.-D. Periictal magnetic resonance imaging in status epilepticus. Epilepsy Res. 2009, 86, 72–81. [Google Scholar] [CrossRef]
- Meletti, S.; Monti, G.; Mirandola, L.; Vaudano, A.E.; Giovannini, G. Neuroimaging of status epilepticus. Epilepsia 2018, 59, 113–119. [Google Scholar] [CrossRef]
- Larionov, S.; König, R.; Urbach, H.; Sassen, R.; Elger, C.E.; Bien, C.G. MRI brain volumetry in Rasmussen encephalitis: The fate of affected and “unaffected” hemispheres. Neurology 2005, 64, 885–887. [Google Scholar] [CrossRef]
- Dupont, S.; Gales, A.; Sammey, S.; Vidailhet, M.; Lambrecq, V. Late-onset Rasmussen Encephalitis: A literature appraisal. Autoimmun. Rev. 2017, 16, 803–810. [Google Scholar] [CrossRef] [Green Version]
- Geller, E.; Faerber, E.N.; Legido, A.; Melvin, J.J.; Hunter, J.V.; Wang, Z.; de Chadarevian, J.P. Rasmussen encephalitis: Complementary role of multitechnique neuroimaging. AJNR Am. J. Neuroradiol. 1998, 19, 445–449. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient (Sex) | Age at Onset (Symptom) | Disease Duration (Years) | Clinical Features at Last Follow-Up | Immunotherapy | Age at Surgery |
|---|---|---|---|---|---|
| 1 (F) | 25 (seizures, behavioural disorder) | 20 | Focal deficit, seizures, cognitive and behavioural disorder | Steroids, IvIg, AZA, MMF | - |
| 2 (F) | 16 (seizures) | 21 | Focal deficit, seizures, EPC, cognitive and behavioural disorder | Steroids, IvIg, PAI, MTX, MMF | - |
| 3 (F) | 20 (focal deficit, EPC, seizures) | 17 | Focal deficit, seizures, cognitive and behavioural disorder | Steroids, IvIg, PAI, MTX, PEX, AZA, RTX | 25 |
| 4 (M) | 15 (EPC) | 28 | Focal deficit, seizures, EPC, cognitive and behavioural disorder | Steroids, IvIg, MMF | - |
| 5 (M) | 48 (focal deficit, EPC, seizures) | 5 | Focal deficit, EPC, seizures | Steroids, IvIg, MMF | - |
| 6 (F) | 19 (EPC, seizures) | 7 | Focal deficit, EPC, seizures | Steroids, IvIg, AZA | 24 |
| 7 (F) | 12 (focal deficit, seizures) | 27 | Focal deficit, seizures, cognitive and behavioural disorder | Steroids, IvIg, MMF | - |
| 8 (F) | 26 (focal deficit, seizures) | 18 | Focal deficit | Steroids, IvIg, AZA, PEX, | 33 |
| 9 (M) | 33 (focal deficit, EPC) | 7 | Focal deficit, EPC, seizures | Steroids, IvIg, AZA | - |
| 10 (F) | 23 (seizures) | 18 * | Focal deficit, seizures, EPC, cognitive and behavioural disorder | Steroids, IvIg, MTX, AZA, cyclophosphamide | - |
| 11 (M) | 43 (status epilepticus) | 5 | Focal deficit | Steroids, IvIg | - |
| 12 (F) | 50 (focal deficit) | 5 | Focal deficit, cognitive and behavioural disorder | Steroids, IvIg | 50 |
| 13 (F) | 21 (focal deficit, seizures, cognitive disorder) | 25 * | Focal deficit, seizures, EPC, cognitive and behavioural disorder | Steroids, IvIg, PEX, PAI | - |
| Patient (Affected Side) | No. Of MRI Examinations | Time between Follow-Ups (Months, Mean ± DS) | MRI Timing | MRI Findings | |
|---|---|---|---|---|---|
| Patient Age | Years from Onset | Atrophy on T1 | |||
| 1 (L) | 13 | 19 ± 30 | 27 | 2 | Fi (1), Ca (2), I (2),ps (1),Tm (1) |
| 37 | 12 | Fi (1), Ca (2), I (3), ps (1), Tp (1), Tm (1),Ti (1) | |||
| 38 | 13 | Fi (1), Ca (2), I (3), ps (2), Tp (1), Tm (2), Ti (1) | |||
| 42 | 17 | Fi (1), Ca (2), I (3), ps (2), Tp (2), Tm (2), Ti (1) | |||
| 43 | 18 | Fi (1), Ca (2), I (3), ps (3), Tp (2), Tm (2), Ti (1) | |||
| 2 (L) | 14 | 15 ± 14 | 21 | 5 | Fi (3), Fm (3), F (3), Op (2), Ca (3), pv (2), I (2), Tp (1), ps (2) |
| 25 | 9 | Fi (3), Fm (3), F (3), Op (2), Ca (3), pv (2), I (3), Tp (1), ps (2) | |||
| 30 | 14 | Fi (3), Fm (3), F (3), Op (2), Ca (3), pv (3), I (3), Tp (1), ps (2) | |||
| 37 | 21 | Fi (3), Fm (3), F (3), Op (2), pc (1), Ca (3), pv (3), I (3), Tp (1), ps (2) | |||
| 3 (L) | 17 | 11 ± 12 | 22 | 2 | F (1), Fi (1), Fm (1), Op (1), pv (1) |
| 24 | 4 | F (1), Fi (1), Fm (1), Op (1), pv (1) | |||
| 25 | 5 | F (2), Fi (2), Fm (2), Op (2), pv (2) | |||
| 29 | 9 | F (3), Fi (3), Fm (3), Op (3), pv (3), I (2), Tm (1), Tp (1), ps (1) | |||
| 30 | 10 | F (3), Fi (3), Fm (3), Op (3), pv (3), I (2), Tm (1), Tp (1), ps (2) | |||
| 34 | 14 | F (3), Fi (3), Fm (3), Op (3), pv (3), I (3), Tm (1), Tp (1), ps (2) | |||
| 4 (R) | 8 | 7 ± 5 | 23 | 8 | F (1), Fm (1), Op (1), pv (1) |
| 25 | 10 | F (2), Fm (2), Op (2), pv (2), pc (1) | |||
| 5 (R) | 9 | 6 ± 3 | 50 | 2 | F (1), pc (1) |
| 53 | 5 | F (1), pc (2) | |||
| 6 (L) | 10 | 5 ± 4 | 23 | 4 | pc (1) |
| 24 | 5 | pc (2) | |||
| 26 | 7 | pc (2), pv (1) | |||
| 7 (R) | 5 | 21 ± 32 | 32 | 20 | pc (1), P (1), pv (1), Ca (3) |
| 38 | 26 | pc (1), P (2), pv (1), Ca (3) | |||
| 8 (R) | 19 | 10 ± 8 | 29 | 3 | Op (1), pv (2), I (2), ps (2), Tp (1) |
| 33 | 7 | Op (2), pc (1), P (1), pv (2), I (3), ps (3), Tp (2) | |||
| 34 | 8 | Op (3), pc (1), P (1), pv (3), I (3), ps (3), Tp (2) | |||
| 9 (R) | 6 | 14 ± 12 | 32 | 0 | F (1), pc (2), P (1) |
| 36 | 4 | F (1), pc (3), P (2) | |||
| 10 (L) | 13 | 14 ± 12 | 35 | 12 | F (2), Fm (1), Op (2), P (1), Ca (2), pv (1), I (3), ps (1), Tp (1) |
| 37 | 14 | F (3), Fm (2), Op (3), P (2), Ca (3), pv (2), I (3), ps (2), Tp (1) | |||
| 11 (R) | 7 | 9 ± 8 | 43 | 0 | Fi (1), Fm (1), Ca (2), I (1), ps (1) |
| 12 (L) | 5 | 5 ± 7 | 50 | 0 | F (1), Fi (1), Fm (1), Op (1), P (3), Ca (1), pv (3), ps (3), Tp (3) |
| 50 | 0 | F (2), Fi (1), Fm (1), Op (2), P (3), Ca (1), pv (3), ps (3), Tp (3) | |||
| 13 (L) | 10 | 18 ± 13 | 49 | 24 | F (2), Fi (2), Fm (2), Op (2), Ca (3), pv (1), I (2), ps (2), Tp (2), Tm (2) |
| 51 | 26 | F (3), Fi (3), Fm (3), Op (3), pc (1), Ca (3), pv (2), I (3), ps (3), Tp (3), Tm (2) | |||
| Patient | MRI Timing | MRI Findings | ||
|---|---|---|---|---|
| Patient Age | Years from Onset | SI White Matter | SI Gray Matter | |
| 1 | 27 | 2 | H (1), I (1), Tm (1) | absent |
| 38 | 13 | H (1), I (1), P (3), T (1), Tm (1) | ||
| 39 | 14 | H (1), I (1), P (1), T (1), Tm (2) | ||
| 42 | 17 | H (1), I (1), P (1), T (1), Tm (1) | ||
| 45 | 20 | H (1), I (1), Ci (1), P (2), T (3), Tm (3) | P (2), T (1), Tm (2) | |
| 2 | 21 | 5 | Fm (3), Fi (3), F (3), I (2), Tm (1) (unchanged) | F (1), I (2), Tm (1) (unchanged) |
| 3 | 22 | 2 | absent | absent |
| 23 | 3 | pc (1), F (1), Fm (1) | pc (1) | |
| 24 | 4 | pc (2), F (2), Fm (2) | pc (2), F (1), Fm (1) | |
| 25 | 5 | pc (3), F (3), Fm (2) | pc (3), F (3), Fm (2) | |
| 29 | 9 | pc (2), F (2), Fm (2), I (2) | pc (2), F (2), Fm (2), I (2) | |
| 37 | 17 | pc (2), F (2), Fm (2), I (3) | pc (2), F (2), Fm (2), I (3) | |
| 4 | 23 | 8 | absent (unchanged) | absent |
| 25 | 10 | F (1) | ||
| 5 | 50 | 2 | pc (1), F (1) | pc (1) |
| 54 | 6 | pc (1), F (2), I (2) | pc (1), F (1), I (1) | |
| 6 | 23 | 4 | absent | pc (1) |
| 24 | 5 | pc (2) | pc (2) | |
| 26 | 7 | absent | absent | |
| 7 | 32 | 20 | P (2), Ci (2) (unchanged) | Ci (2) |
| 32 | 20 | Ci (3) | ||
| 38 | 26 | Ci (2) | ||
| 8 | 29 | 3 | Op (1), I (1), Tp (1) | Op (1), I (1), Tp (1) |
| 30 | 4 | Op (1), I (1), Tp (1) | Op (1), I (2), Tp (1) | |
| 31 | 5 | Op (1), I (2), Tp (1) | Op (1), I (2), Tp (1) | |
| 34 | 8 | Op (2), I (2), pc (2), P (2), Tp (1) | Op (1), I (1), Tp (1), pc (1), P (1) | |
| 44 | 18 | Op (2), I (2), pc (3), P (2), Tp (1) | Op (1), I (1), Tp (1), pc (1), P (1) | |
| 9 | 32 | 0 | P (1) (unchanged) | P (1) (unchanged) |
| 10 | 35 | 12 | F (1),Fm (2),Op (1),I (1),O (2),Om (2),ps (2) | F (1), Fm (2), Op (1), I (1), O (2), Om (2), ps (2) |
| 37 | 14 | F (2), Fm (2), Op (1), I (1), O (1), Om (1), ps (2) | F (2), Fm (2), Op (1), I (1), O (1), Om (1), ps (2) | |
| 11 | 43 | 0 | absent (unchanged) | Fi (2), Fm (1), I (1) |
| 44 | 1 | Fi (1), Fm (1), I (1) | ||
| 47 | 4 | absent | ||
| 12 | 50 | 0 | F (1),I (1),O (2),Om (2),pv (2),ps (2),Tm (2),Tp (2),Ti (2),T (2) | Om (1) |
| 50 | 0 | F (2),I (2),O (2),Om (2),pv (2),ps (2), Tm (2),Tp (2),Ti (2),T (2) (stable) | absent (stable) | |
| 52 | 2 | |||
| 13 | 49 | 24 | F (3), Fi (3), Op (3), I (2), P (1), pv (2), ps (1), Tm (1), Tp (1) | F (3), Fi (3), Fm (3), Op (3), I (3) |
| 51 | 26 | F (3), Fi (3), Op (3), I (2), P (1), pv (2), ps (1), Tm (1), Tp (1) | F (3), Fi (3), Fm (3), Op (3), I (3) | |
| 63 | 38 | F (3), Fi (3), Op (3), I (2), P (2), pv (2), ps (1), Tm (1), Tp (1) | F (3), Fi (3), Fm (3), Op (3), I (3), P (1) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doniselli, F.M.; Deleo, F.; Criscuolo, S.; Stabile, A.; Pastori, C.; Di Giacomo, R.; Didato, G.; Chiapparini, L.; Villani, F. MRI in Late-Onset Rasmussen Encephalitis: A Long-Term Follow-Up Study. Diagnostics 2022, 12, 502. https://doi.org/10.3390/diagnostics12020502
Doniselli FM, Deleo F, Criscuolo S, Stabile A, Pastori C, Di Giacomo R, Didato G, Chiapparini L, Villani F. MRI in Late-Onset Rasmussen Encephalitis: A Long-Term Follow-Up Study. Diagnostics. 2022; 12(2):502. https://doi.org/10.3390/diagnostics12020502
Chicago/Turabian StyleDoniselli, Fabio Martino, Francesco Deleo, Stefania Criscuolo, Andrea Stabile, Chiara Pastori, Roberta Di Giacomo, Giuseppe Didato, Luisa Chiapparini, and Flavio Villani. 2022. "MRI in Late-Onset Rasmussen Encephalitis: A Long-Term Follow-Up Study" Diagnostics 12, no. 2: 502. https://doi.org/10.3390/diagnostics12020502
APA StyleDoniselli, F. M., Deleo, F., Criscuolo, S., Stabile, A., Pastori, C., Di Giacomo, R., Didato, G., Chiapparini, L., & Villani, F. (2022). MRI in Late-Onset Rasmussen Encephalitis: A Long-Term Follow-Up Study. Diagnostics, 12(2), 502. https://doi.org/10.3390/diagnostics12020502