
Impact of Macroscopic On-Site Evaluation (MOSE) on Accuracy of Endoscopic Ultrasound-Guided Fine-Needle Biopsy (EUS-FNB) of Pancreatic and Extrapancreatic Solid Lesions: A Prospective Study

 ,
,  ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. EUS-FNB Procedure
2.2. Sample Management
2.3. Cyto-Histological Evaluation
2.4. Gold Standard for Diagnosis
2.5. Outcomes
2.6. Statistical Analysis
3. Results
3.1. Adequacy and Diagnostic Accuracy of MOSE Compared to Conventional FNB
3.2. Procedure-Related Complications
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Larghi, A.; Verna, E.C.; Ricci, R.; Seerden, T.C.; Galasso, D.; Carnuccio, A.; Uchida, N.; Rindi, G.; Costamagna, G. EUS-guided fine-needle tissue acquisition by using a 19-gauge needle in a selected patient population: A prospective study. Gastrointest. Endosc. 2011, 74, 504–510. [Google Scholar] [CrossRef] [PubMed]
- Iwashita, T.; Yasuda, I.; Mukai, T.; Doi, S.; Nakashima, M.; Uemura, S.; Mabuchi, M.; Shimizu, M.; Hatano, Y.; Hara, A.; et al. Macroscopic on-site quality evaluation of biopsy specimens to improve the diagnostic accuracy during EUS-guided FNA using a 19-gauge needle for solid lesions: A single-center prospective pilot study (MOSE study). Gastrointest. Endosc. 2015, 81, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Kin, T.; Katanuma, A.; Yane, K.; Takahashi, K.; Osanai, M.; Takaki, R.; Matsumoto, K.; Gon, K.; Matsumori, T.; Tomonari, A.; et al. Diagnostic ability of EUS-FNA for pancreatic solid lesions with conventional 22-gauge needle using the slow pull technique: A prospective study. Scand. J. Gastroenterol. 2015, 50, 900–907. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Grimm, I.S.; Ali, B.; Nollan, R.; Tombazzi, C.; Ismail, M.K.; Baron, T.H. A meta-analysis of endoscopic ultrasound–fine-needle aspiration compared to endoscopic ul-trasound–fine-needle biopsy: Diagnostic yield and the value of onsite cytopathological assessment. Endosc. Int. Open 2017, 5, E363–E375. [Google Scholar] [PubMed] [Green Version]
- Ishikawa, T.; Kawashima, H.; Ohno, E.; Tanaka, H.; Sakai, D.; Iida, T.; Nishio, R.; Yamamura, T.; Furukawa, K.; Nakamura, M.; et al. Clinical Impact of EUS-Guided Fine Needle Biopsy Using a Novel Franseen Needle for Histological Assessment of Pancreatic Diseases. Can. J. Gastroenterol. Hepatol. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, D.-W.; Oh, D.; Hong, S.-M.; Song, T.; Park, D.; Lee, S.; Lee, S.; Kim, M.-H. The impact of macroscopic on-site evaluation using filter paper in EUS-guided fine-needle biopsy. Endosc. Ultrasound 2019, 8, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Polkowski, M.; Jenssen, C.C.; Kaye, P.V.; Carrara, S.; Deprez, P.; Ginès, A.; Fernández-Esparrach, G.G.; Eisendrath, P.; Aithal, G.P.; Arcidiacono, P.P.; et al. Technical aspects of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Technical Guideline-March 2017. Endoscopy 2017, 49, 989–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capurso, G.; Archibugi, L.; Petrone, M.C.; Arcidiacono, P.G. Slow-pull compared to suction technique for EUS-guided sampling of pancreatic solid lesions: A meta-analysis of randomized controlled trials. Endosc. Int. Open 2020, 8, E636–E643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Mitri, R.; Rimbaş, M.; Attili, F.; Fabbri, C.; Carrara, S.; Di Maurizio, L.; Inzani, F.; Repici, A.; Gasbarrini, A.; Costamagna, G.; et al. Performance of a new needle for endoscopic ultrasound-guided fine-needle biopsy in patients with pancreatic solid lesions: A retrospective multicenter study. Endosc. Ultrasound 2018, 7, 329–334. [Google Scholar]
- Cho, E.; Park, C.H.; Kim, T.H.; Cho, C.M.; Seo, D.W.; Kim, J.; Choi, J.H.; Moon, S.-H. A prospective, randomized, multicenter clinical trial comparing 25 gauge and 20 gauge biopsy needles for endoscopic ultrasound guided sampling of solid pancreatic lesions. Surg. Endosc. 2020, 34, 1310–1317. [Google Scholar] [CrossRef] [PubMed]
- Ishiwatari, H.; Kaneko, J.; Sasaki, K.; Satoh, T.; Sato, J.; Matsubayashi, H.; Yabuuchi, Y.; Kishida, Y.; Yoshida, M.; Ito, S.; et al. Macroscopic on-site evaluation of biopsy specimens for accurate pathological diagnosis during EUS-guided fine needle biopsy using 22-G Franseen needle. Endosc. Ultrasound 2020, 9, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, J.; Ishiwatari, H.; Sasaki, K.; Yasuda, I.; Takahashi, K.; Imura, J.; Iwashita, T.; Uemura, S.; Hatano, Y.; Miyazaki, T.; et al. Macroscopic visible core length can predict the histological sample quantity in endo-scopic ultrasound-guided tissue acquisition: Multicenter prospective study. Dig. Endosc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Kuwatani, M.; Sugiura, R.; Yane, K.; Taya, Y.; Ihara, H.; Onodera, M.; Eto, K.; Sano, I.; Kudo, T.; Mitsuhashi, T.; et al. Prospective, multicenter, observational study of tissue acquisition through EUS-guided fine-needle biopsy using a 25G Franseen needle. Endosc. Ultrasound 2019, 8, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Chong, C.C.N.; Lakhtakia, S.; Nguyen, N.; Hara, K.; Chan, W.K.; Puri, R.; Almadi, M.A.; Ang, T.L.; Kwek, A.; Yasuda, I.; et al. Endoscopic ultrasound-guided tissue acquisition with or without macroscopic on-site evaluation: Randomized controlled trial. Laryngo-Rhino-Otologie 2020, 52, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Ki EL, L.; Lemaistre, A.I.; Fumex, F.; Gincul, R.; Lefort, C.; Lepilliez, V.; Pujol, B.; Napoléon, B. Macroscopic onsite evaluation using endoscopic ultrasound fine needle biopsy as an alternative to rapid onsite evaluation. Endosc. Int. Open 2019, 7, E189–E194. [Google Scholar]
- Mangiavillano, B.; Frazzoni, L.; Togliani, T.; Fabbri, C.; Tarantino, I.; De Luca, L.; Staiano, T.; Binda, C.; Signoretti, M.; Eusebi, L.H.; et al. Macroscopic on-site evaluation (MOSE) of specimens from solid lesions acquired during EUS-FNB: Multicenter study and comparison between needle gauges. Endosc. Int. Open 2021, 9, E901–E906. [Google Scholar] [CrossRef] [PubMed]
- So, H.; Seo, D.W.; Hwang, J.S.; Ko, S.W.; Oh, D.; Song, T.J.; Park, D.H.; Lee, S.K.; Kim, M.-H. Macroscopic on-site evaluation after EUS-guided fine needle biopsy may replace rapid on-site evaluation. Endosc. Ultrasound 2021, 10, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Van Riet, P.A.; Erler, N.S.; Bruno, M.J.; Cahen, D.L. Comparison of fine-needle aspiration and fine-needle biopsy devices for endoscopic ultrasound-guided sampling of solid lesions: A systemic review and meta-analysis. Endoscopy 2020. [Google Scholar] [CrossRef] [PubMed]
- Crinò, S.F.; Manfrin, E.; Scarpa, A.; Baldaque-Silva, F.; Carrara, S.; de Nucci, G.; Di Mitri, R.; Ginés, A.; Iglesias-Garcia, J.; Itoi, T.; et al. EUS-FNB with or without on-site evaluation for the diagnosis of solid pancreatic lesions (FROSENOR): Protocol for a multicenter randomized non-inferiority trial. Dig. Liver Dis. 2019, 51, 901–906. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
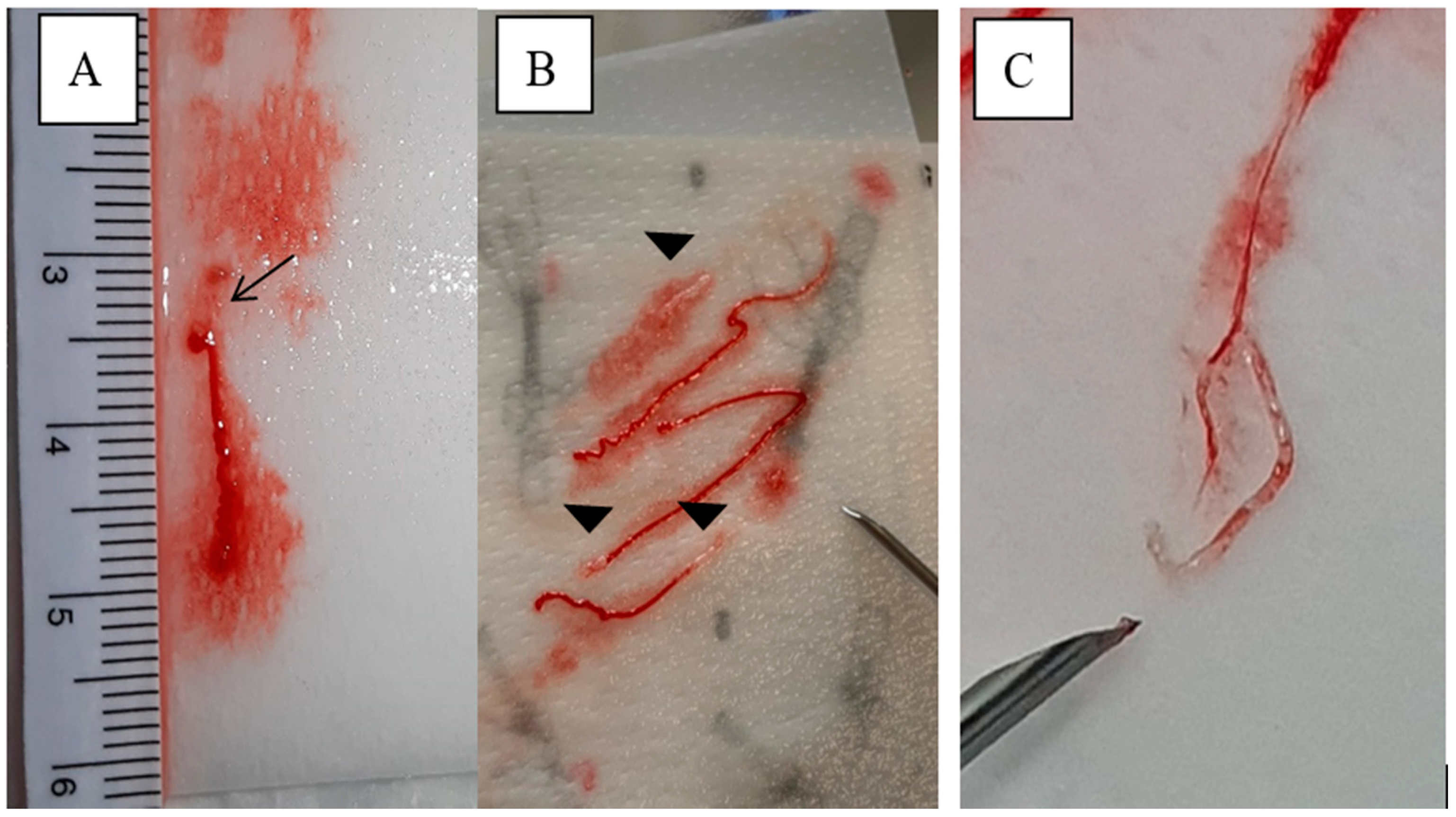
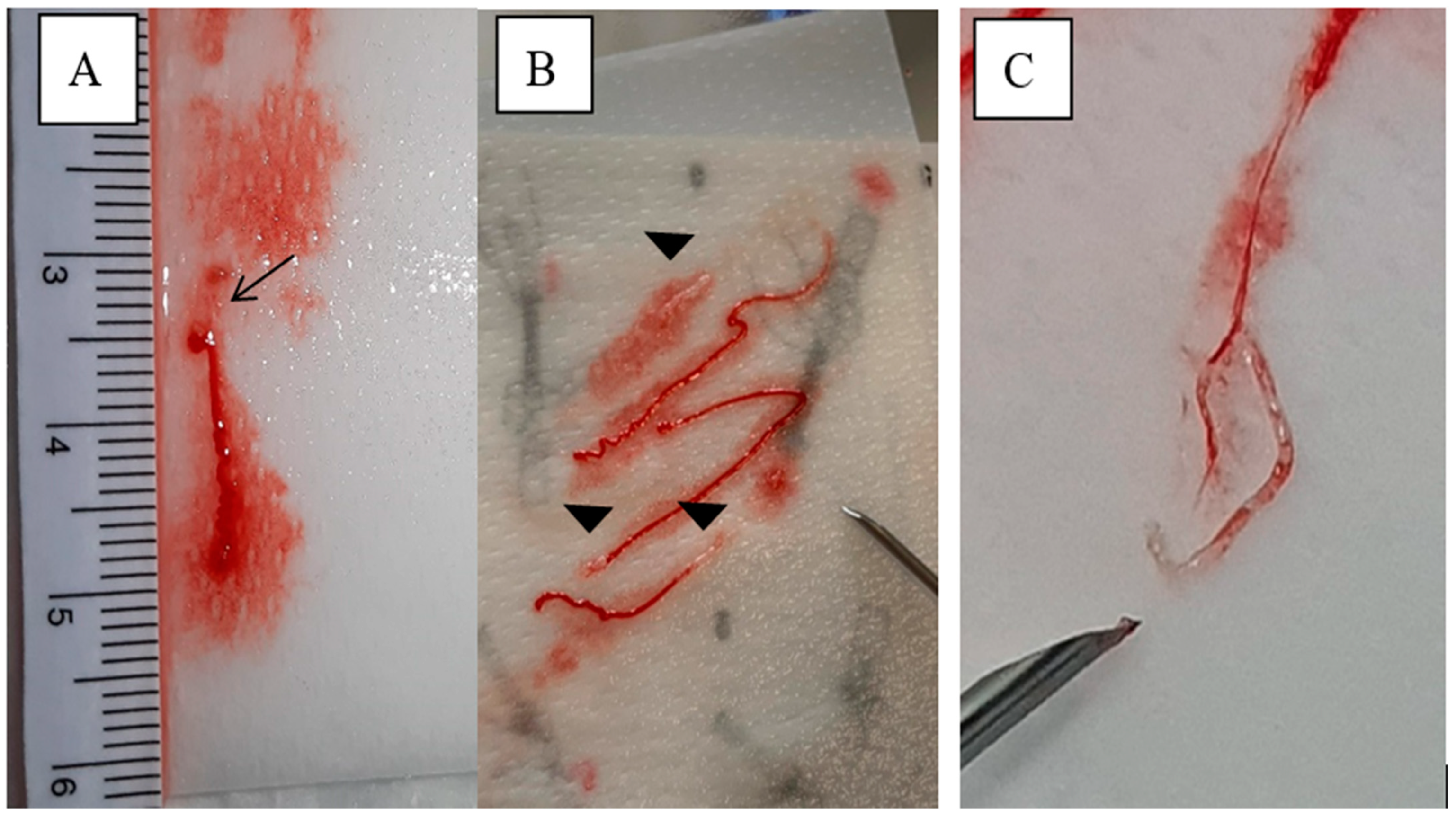
| MOSE Score | Contents of the Biopsy | Classification of the Sample |
|---|---|---|
| 0 | punctio sicca/no material | negative (−) |
| 1 | only necrotic or haematic material | acceptable (+) |
| 2 | ≥1 core tissue ≤ 2 mm yellowish-white | positive (+) |
| 3 | ≥1 core tissue > 2 mm yellowish-white | positive (+) |
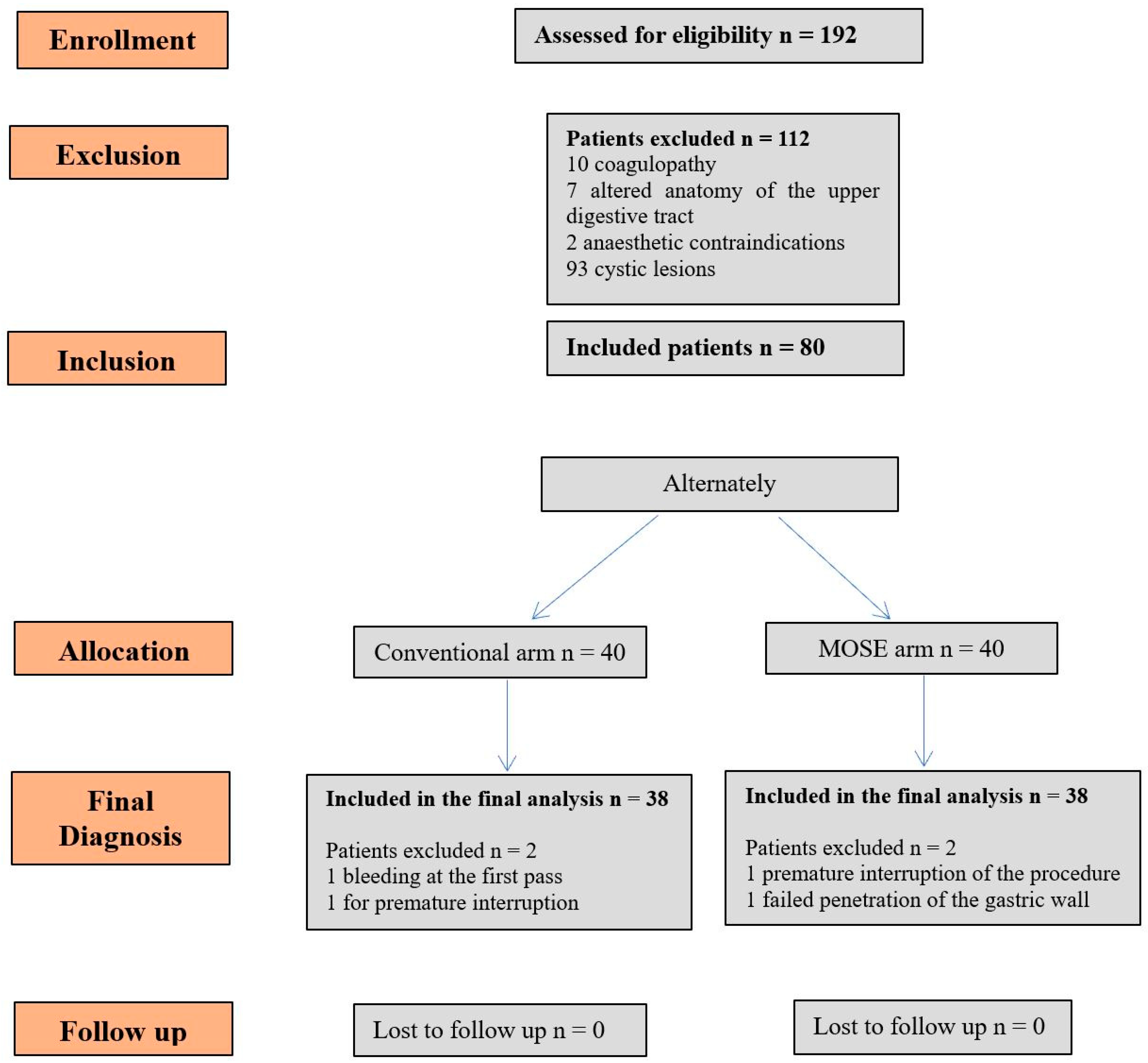
| MOSE (n = 38) | Conventional (n = 38) | p Value | |
|---|---|---|---|
| Male sex, n (%) | 24 (63.2%) | 23 (60.5%) | 0.81 |
| Age, mean (SD), years | 67.2 (9.95) | 69.9 (11.2) | 0.59 |
| Size of lesion, median (IQR), mm | 31.5 (25–40) | 30.5 (20–40) | 0.54 |
| Indication, n (%) | |||
| -Pancreatic lesion | 24 (63.2%) | 25 (65.8%) | |
| -Lymphadenopathy | 7 (18.4%) | 7 (18.4%) | |
| -Subepithelial lesion | 4 (10.5%) | 5 (13.2%) | |
| -Others | 3 (7.9%) | 1 (2.6%) | |
| Mean number of needle passes (SD) | 3.8 (0.84) | 3.7 (0.61) | 0.46 |
| FNB site | |||
| -Esophagus | 4 (10.5%) | 3 (7.9%) | |
| -Stomach | 22 (57.9%) | 22 (57.9%) | |
| -Duodenum | 12 (31.6%) | 13 (34.2%) |
| MOSE Arm | Type of Lesion |
|---|---|
| Pancreatic lesions (24) | 17 ductal adenocarcinoma |
| 3 chronic pancreatitis | |
| 2 neuroendocrine tumor (NET) | |
| 1 acinar carcinoma with NET foci | |
| 1 regular pancreas | |
| Extrapancreatic lesions (16) | 7 neoplastic/metastatic lymph node |
| 4 stromal lesions (GIST/leiomyoma) | |
| 2 inflammatory lymph node | |
| 2 ampullary adenocarcinoma | |
| CONVENTIONAL Arm | |
| Pancreatic lesions (25) | 20 ductal adenocarcinoma |
| 3 neuroendocrine tumor (NET) | |
| 2 chronic pancreatitis | |
| Extrapancreatic lesions (15) | 5 neoplastic/metastatic lymph node |
| 2 stromal lesion (GIST/leiomyoma) | |
| 2 inflammatory lymph node | |
| 2 cholangiocarcinoma | |
| 1 squamous cell carcinoma of the oesophagus | |
| 1 carcinosarcoma | |
| 1 undifferentiated gastric adenocarcinoma | |
| 1 vascular malformation with calcifications |
| MOSE (n = 38) | Conventional (n = 38) | p Value | |
|---|---|---|---|
| Diagnostic adequacy | 79% | 82.2% | >0.05 |
| Sensitivity | 78% | 81.50% | >0.05 |
| Specificity | 100% | 100% | >0.05 |
| PPV | 100% | 100% | >0.05 |
| NPV | 41.6% | 41.9% | >0.05 |
| Diagnostic accuracy | 79% | 82.2% | >0.05 |
| MOSE Score | N Samples | Adequacy (%) | Accuracy (%) |
|---|---|---|---|
| 0—negative | 0 | 0 (0%) | 0 |
| 1—acceptable | 23 | 23 (100%) | 10 (43.5) |
| 2—positive | 31 | 29 (93.5) | 20 (65.5) |
| 3—positive | 60 | 59 (98.3) | 47 (78.3) |
| Total | 114 | 111/114 (97.4) | 77/114 (67.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaia, S.; Rizza, S.; Bruno, M.; Ribaldone, D.G.; Maletta, F.; Sacco, M.; Pacchioni, D.; Rizzi, F.; Saracco, G.M.; Fagoonee, S.; et al. Impact of Macroscopic On-Site Evaluation (MOSE) on Accuracy of Endoscopic Ultrasound-Guided Fine-Needle Biopsy (EUS-FNB) of Pancreatic and Extrapancreatic Solid Lesions: A Prospective Study. Diagnostics 2022, 12, 428. https://doi.org/10.3390/diagnostics12020428
Gaia S, Rizza S, Bruno M, Ribaldone DG, Maletta F, Sacco M, Pacchioni D, Rizzi F, Saracco GM, Fagoonee S, et al. Impact of Macroscopic On-Site Evaluation (MOSE) on Accuracy of Endoscopic Ultrasound-Guided Fine-Needle Biopsy (EUS-FNB) of Pancreatic and Extrapancreatic Solid Lesions: A Prospective Study. Diagnostics. 2022; 12(2):428. https://doi.org/10.3390/diagnostics12020428
Chicago/Turabian StyleGaia, Silvia, Stefano Rizza, Mauro Bruno, Davide Giuseppe Ribaldone, Francesca Maletta, Marco Sacco, Donatella Pacchioni, Felice Rizzi, Giorgio Maria Saracco, Sharmila Fagoonee, and et al. 2022. "Impact of Macroscopic On-Site Evaluation (MOSE) on Accuracy of Endoscopic Ultrasound-Guided Fine-Needle Biopsy (EUS-FNB) of Pancreatic and Extrapancreatic Solid Lesions: A Prospective Study" Diagnostics 12, no. 2: 428. https://doi.org/10.3390/diagnostics12020428
APA StyleGaia, S., Rizza, S., Bruno, M., Ribaldone, D. G., Maletta, F., Sacco, M., Pacchioni, D., Rizzi, F., Saracco, G. M., Fagoonee, S., & De Angelis, C. G. (2022). Impact of Macroscopic On-Site Evaluation (MOSE) on Accuracy of Endoscopic Ultrasound-Guided Fine-Needle Biopsy (EUS-FNB) of Pancreatic and Extrapancreatic Solid Lesions: A Prospective Study. Diagnostics, 12(2), 428. https://doi.org/10.3390/diagnostics12020428