
Prediction for Mitosis-Karyorrhexis Index Status of Pediatric Neuroblastoma via Machine Learning Based 18F-FDG PET/CT Radiomics

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Evaluation of the MKI
2.3. Image Acquisition
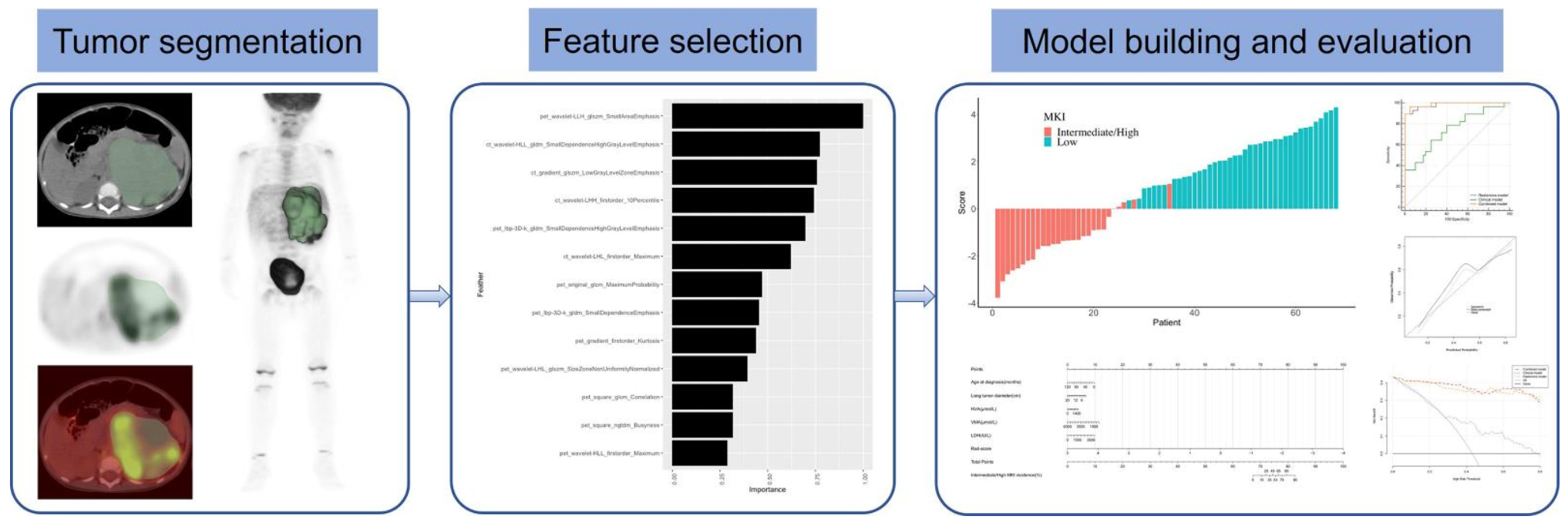
2.4. Region of Interest Segmentation and Radiomics Features Extraction
2.5. Machine Learning and Radiomics Features Selection
2.6. Model Construction and Evaluating Performance of the Models
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics
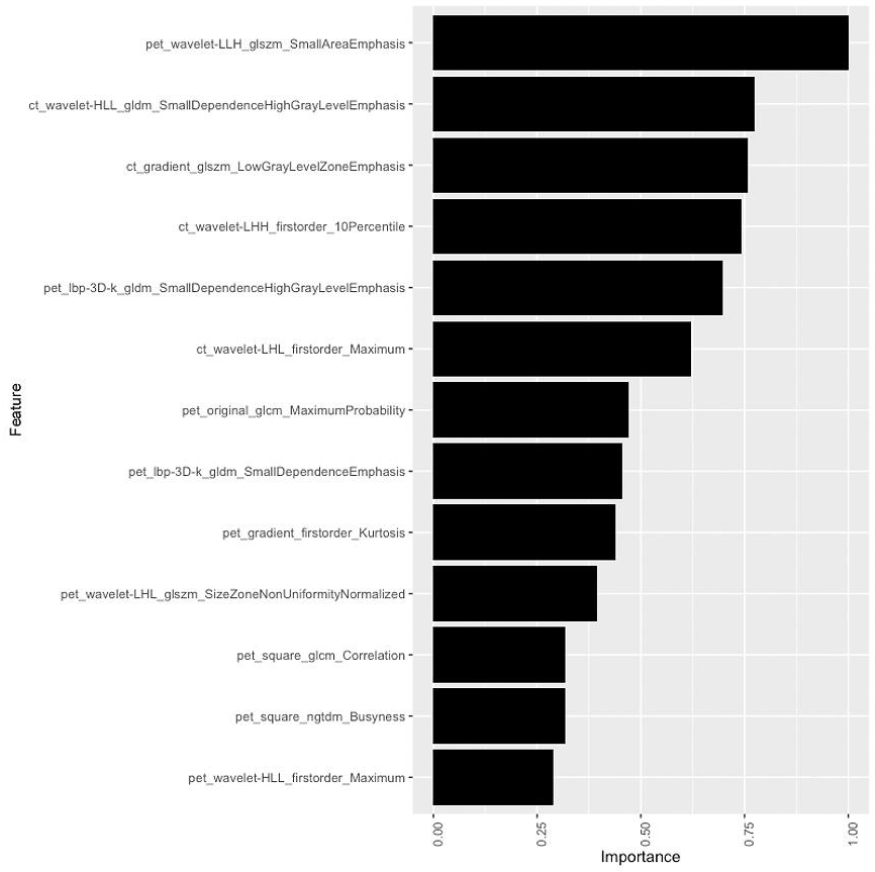
3.2. Radiomics Features Selection and Radiomics Model Construction
3.3. Clinical Model and Radiomics Nomogram Construction
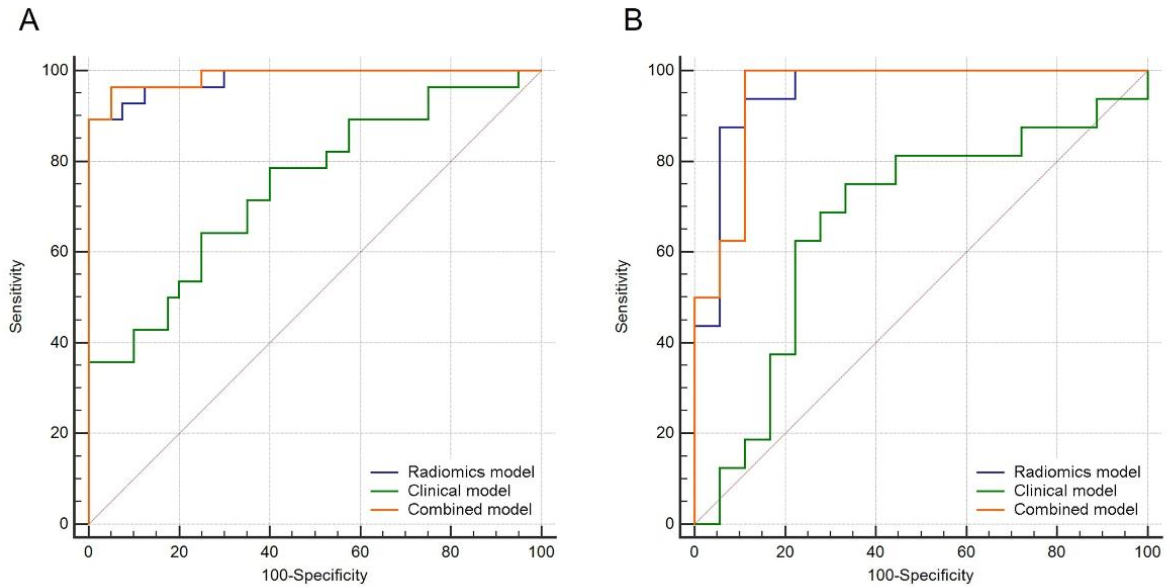
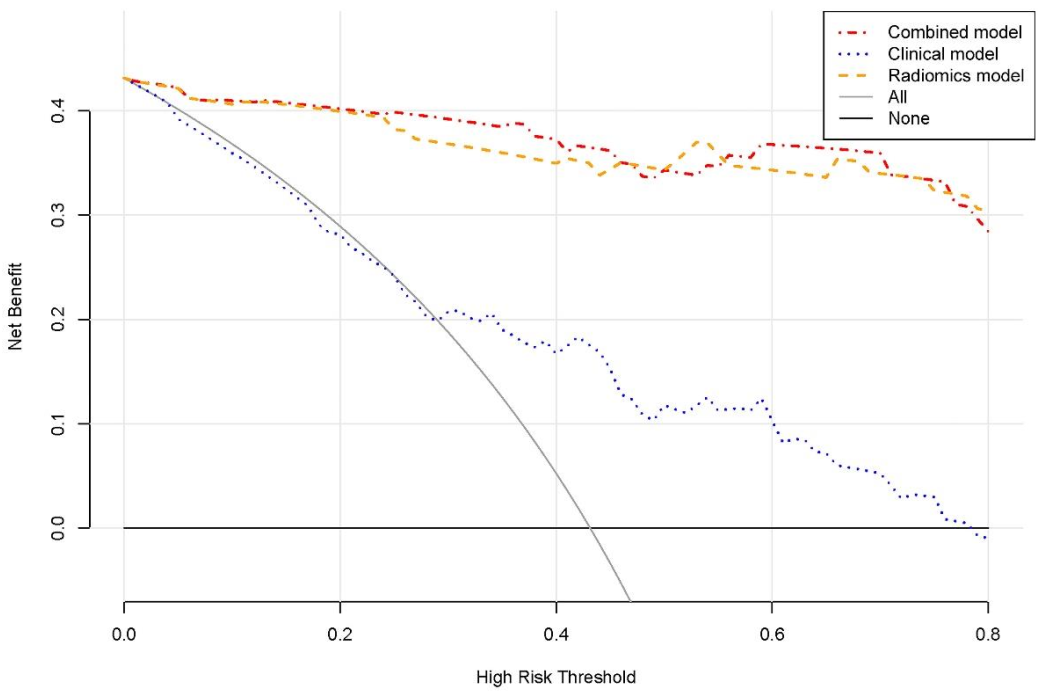
3.4. Performance of Prediction Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Orr, K.E.; McHugh, K. The new international neuroblastoma response criteria. Pediatr. Radiol. 2019, 49, 1433–1440. [Google Scholar] [CrossRef]
- Aravindan, N.; Somasundaram, D.B.; Herman, T.S.; Aravindan, S. Significance of hematopoietic surface antigen CD34 in neuroblastoma prognosis and the genetic landscape of CD34-expressing neuroblastoma CSCs. Cell Biol. Toxicol. 2021, 37, 461–478. [Google Scholar] [CrossRef]
- Maris, J.M.; Hogarty, M.D.; Bagatell, R.; Cohn, S.L. Neuroblastoma. Lancet 2007, 369, 2106–2120. [Google Scholar] [CrossRef]
- Sokol, E.; Desai, A.V.; Applebaum, M.A.; Valteau-Couanet, D.; Park, J.R.; Pearson, A.D.J.; Schleiermacher, G.; Irwin, M.S.; Hogarty, M.; Naranjo, A.; et al. Age, Diagnostic Category, Tumor Grade, and Mitosis-Karyorrhexis Index Are Independently Prognostic in Neuroblastoma: An INRG Project. J. Clin. Oncol. 2020, 38, 1906–1918. [Google Scholar] [CrossRef] [PubMed]
- Atikankul, T.; Atikankul, Y.; Santisukwongchote, S.; Marrano, P.; Shuangshoti, S.; Thorner, P.S. MIB-1 Index as a Surrogate for Mitosis-Karyorrhexis Index in Neuroblastoma. Am. J. Surg. Pathol. 2015, 39, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Irwin, M.S.; Naranjo, A.; Zhang, F.F.; Cohn, S.L.; London, W.B.; Gastier-Foster, J.M.; Ramirez, N.C.; Pfau, R.; Reshmi, S.; Wagner, E.; et al. Revised Neuroblastoma Risk Classification System: A Report from the Children’s Oncology Group. J. Clin. Oncol. 2021, 39, 3229–3241. [Google Scholar] [CrossRef]
- Klijanienko, J.; Couturier, J.; Brisse, H.; Pierron, G.; Freneaux, P.; Berger, F.; Maciorowski, Z.; Sastre-Garau, X.; Michon, J.; Schleiermacher, G. Diagnostic and prognostic information obtained on fine-needle aspirates of primary neuroblastic tumors: Proposal for a cytology prognostic score. Cancer Cytopathol. 2011, 119, 411–423. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, H.; Huang, K.; Liu, H.; Ding, H.; Zhang, L.; Zhang, T.; Yu, W.; He, L. CT-Based Radiomics Signature with Machine Learning Predicts MYCN Amplification in Pediatric Abdominal Neuroblastoma. Front. Oncol. 2021, 11, 687884. [Google Scholar] [CrossRef] [PubMed]
- Khanna, O.; Fathi Kazerooni, A.; Farrell, C.J.; Baldassari, M.P.; Alexander, T.D.; Karsy, M.; Greenberger, B.A.; Garcia, J.A.; Sako, C.; Evans, J.J.; et al. Machine Learning Using Multiparametric Magnetic Resonance Imaging Radiomic Feature Analysis to Predict Ki-67 in World Health Organization Grade I Meningiomas. Neurosurgery 2021, 89, 928–936. [Google Scholar] [CrossRef]
- Sung, A.J.; Weiss, B.D.; Sharp, S.E.; Zhang, B.; Trout, A.T. Prognostic significance of pretreatment 18F-FDG positron emission tomography/computed tomography in pediatric neuroblastoma. Pediatr. Radiol. 2021, 51, 1400–1405. [Google Scholar] [CrossRef] [PubMed]
- Kushner, B.H.; Yeung, H.W.; Larson, S.M.; Kramer, K.; Cheung, N.K. Extending positron emission tomography scan utility to high-risk neuroblastoma: Fluorine-18 fluorodeoxyglucose positron emission tomography as sole imaging modality in follow-up of patients. J. Clin. Oncol. 2001, 19, 3397–3405. [Google Scholar] [CrossRef]
- Kang, S.Y.; Rahim, M.K.; Kim, Y.I.; Cheon, G.J.; Kang, H.J.; Shin, H.Y.; Kang, K.W.; Chung, J.K.; Kim, E.E.; Lee, D.S. Clinical Significance of Pretreatment FDG PET/CT in MIBG-Avid Pediatric Neuroblastoma. Nucl. Med. Mol. Imaging 2017, 51, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Kaiser, L.; Holzgreve, A.; Ruf, V.C.; Suchorska, B.; Wenter, V.; Quach, S.; Herms, J.; Bartenstein, P.; Tonn, J.C.; et al. Prediction of TERTp-mutation status in IDH-wildtype high-grade gliomas using pre-treatment dynamic [18F]FET PET radiomics. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4415–4425. [Google Scholar] [CrossRef]
- Chang, C.; Zhou, S.; Yu, H.; Zhao, W.; Ge, Y.; Duan, S.; Wang, R.; Qian, X.; Lei, B.; Wang, L.; et al. A clinically practical radiomics-clinical combined model based on PET/CT data and nomogram predicts EGFR mutation in lung adenocarcinoma. Eur. Radiol. 2021, 31, 6259–6268. [Google Scholar] [CrossRef] [PubMed]
- Umutlu, L.; Kirchner, J.; Bruckmann, N.M.; Morawitz, J.; Antoch, G.; Ingenwerth, M.; Bittner, A.K.; Hoffmann, O.; Haubold, J.; Grueneisen, J.; et al. Multiparametric Integrated 18F-FDG PET/MRI-Based Radiomics for Breast Cancer Phenotyping and Tumor Decoding. Cancers 2021, 13, 2928. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Saltz, J.H.; Yang, V.W. State of machine and deep learning in histopathological applications in digestive diseases. World J. Gastroenterol. 2021, 27, 2545–2575. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, N.; Rohilla, M.; Trehan, A.; Bansal, D.; Kakkar, N.; Srinivasan, R. Mitosis-Karyorrhexis Index evaluation by digital image visual analysis for application of International Neuroblastoma Pathology Classification in FNA biopsy. Cancer Cytopathol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Stauss, J.; Franzius, C.; Pfluger, T.; Juergens, K.U.; Biassoni, L.; Begent, J.; Kluge, R.; Amthauer, H.; Voelker, T.; Hojgaard, L.; et al. Guidelines for 18F-FDG PET and PET-CT imaging in paediatric oncology. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1581–1588. [Google Scholar] [CrossRef]
- Delbeke, D.; Coleman, R.E.; Guiberteau, M.J.; Brown, M.L.; Royal, H.D.; Siegel, B.A.; Townsend, D.W.; Berland, L.L.; Parker, J.A.; Hubner, K.; et al. Procedure guideline for tumor imaging with 18F-FDG PET/CT 1.0. J. Nucl. Med. 2006, 47, 885–895. [Google Scholar]
- Mao, Z.; Xia, M.; Jiang, B.; Xu, D.; Shi, P. Incipient Fault Diagnosis for High-Speed Train Traction Systems via Stacked Generalization. IEEE Trans. Cybern. 2020. [Google Scholar] [CrossRef]
- Elith, J.; Leathwick, J.R.; Hastie, T. A working guide to boosted regression trees. J. Anim. Ecol. 2008, 77, 802–813. [Google Scholar] [CrossRef]
- Kobayashi, C.; Monforte-Munoz, H.L.; Gerbing, R.B.; Stram, D.O.; Matthay, K.K.; Lukens, J.N.; Seeger, R.C.; Shimada, H. Enlarged and prominent nucleoli may be indicative of MYCN amplification: A study of neuroblastoma (Schwannian stroma-poor), undifferentiated/poorly differentiated subtype with high mitosis-karyorrhexis index. Cancer 2005, 103, 174–180. [Google Scholar] [CrossRef]
- Teshiba, R.; Kawano, S.; Wang, L.L.; He, L.; Naranjo, A.; London, W.B.; Seeger, R.C.; Gastier-Foster, J.M.; Look, A.T.; Hogarty, M.D.; et al. Age-dependent prognostic effect by Mitosis-Karyorrhexis Index in neuroblastoma: A report from the Children’s Oncology Group. Pediatr. Dev. Pathol. 2014, 17, 441–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohn, S.L.; Pearson, A.D.; London, W.B.; Monclair, T.; Ambros, P.F.; Brodeur, G.M.; Faldum, A.; Hero, B.; Iehara, T.; Machin, D.; et al. The International Neuroblastoma Risk Group (INRG) classification system: An INRG Task Force report. J. Clin. Oncol. 2009, 27, 289–297. [Google Scholar] [CrossRef]
- Di Giannatale, A.; Di Paolo, P.L.; Curione, D.; Lenkowicz, J.; Napolitano, A.; Secinaro, A.; Toma, P.; Locatelli, F.; Castellano, A.; Boldrini, L. Radiogenomics prediction for MYCN amplification in neuroblastoma: A hypothesis generating study. Pediatr. Blood Cancer 2021, 68, e29110. [Google Scholar] [CrossRef]
- Starosolski, Z.; Courtney, A.N.; Srivastava, M.; Guo, L.; Stupin, I.; Metelitsa, L.S.; Annapragada, A.; Ghaghada, K.B. A Nanoradiomics Approach for Differentiation of Tumors Based on Tumor-Associated Macrophage Burden. Contrast Media Mol. Imaging 2021, 2021, 6641384. [Google Scholar] [CrossRef]
- Zhao, W.; Wu, Y.; Xu, Y.; Sun, Y.; Gao, P.; Tan, M.; Ma, W.; Li, C.; Jin, L.; Hua, Y.; et al. The Potential of Radiomics Nomogram in Non-invasively Prediction of Epidermal Growth Factor Receptor Mutation Status and Subtypes in Lung Adenocarcinoma. Front. Oncol. 2019, 9, 1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.; Wu, C.; Zheng, H.; Wang, L.; Guan, W.; Duan, S.; Wang, D. Radiogenomics of neuroblastoma in pediatric patients: CT-based radiomics signature in predicting MYCN amplification. Eur. Radiol. 2021, 31, 3080–3089. [Google Scholar] [CrossRef]
- Liu, Y.; Kim, J.; Balagurunathan, Y.; Li, Q.; Garcia, A.L.; Stringfield, O.; Ye, Z.; Gillies, R.J. Radiomic Features Are Associated with EGFR Mutation Status in Lung Adenocarcinomas. Clin. Lung Cancer 2016, 17, 441–448.e6. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Chen, B.; Liu, X.; Song, J.; Fang, M.; Hu, C.; Dong, D.; Li, W.; Tian, J. Quantitative Biomarkers for Prediction of Epidermal Growth Factor Receptor Mutation in Non-Small Cell Lung Cancer. Transl. Oncol. 2018, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Xing, H.; Hao, Z.; Zhu, W.; Sun, D.; Ding, J.; Zhang, H.; Liu, Y.; Huo, L. Preoperative prediction of pathological grade in pancreatic ductal adenocarcinoma based on 18F-FDG PET/CT radiomics. EJNMMI Res. 2021, 11, 19. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.; Xu, L.; Cao, Z.; Wan, Y.; Xue, Y.; Jiang, Y.; Yen, E.; Luo, C.; Wang, J.; Rong, Y.; et al. Extracting and Selecting Robust Radiomic Features from PET/MR Images in Nasopharyngeal Carcinoma. Mol. Imaging Biol. 2020, 22, 1581–1591. [Google Scholar] [CrossRef]
- Zhang, L.; Dong, D.; Li, H.; Tian, J.; Ouyang, F.; Mo, X.; Zhang, B.; Luo, X.; Lian, Z.; Pei, S.; et al. Development and validation of a magnetic resonance imaging-based model for the prediction of distant metastasis before initial treatment of nasopharyngeal carcinoma: A retrospective cohort study. EBioMedicine 2019, 40, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.; Hero, B.; Hunneman, D.H.; Berthold, F. Tumour markers are poor predictors for relapse or progression in neuroblastoma. Eur. J. Cancer 2003, 39, 1899–1903. [Google Scholar] [CrossRef]
- Qin, H.; Yang, S.; Cai, S.; Ren, Q.; Han, W.; Yang, W.; Cheng, H.; Ma, X.; Wang, H. Clinical characteristics and risk factors of 47 cases with ruptured neuroblastoma in children. BMC Cancer 2020, 20, 243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhao, X.; Zhao, Y.; Zhang, J.; Zhang, Z.; Wang, J.; Wang, Y.; Dai, M.; Han, J. Value of pre-therapy 18F-FDG PET/CT radiomics in predicting EGFR mutation status in patients with non-small cell lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1137–1146. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients (n = 102) | Training Set (n = 68) | Validation Set (n = 34) | p Value |
|---|---|---|---|---|
| Age at diagnosis (months) | 33.5 (17.0–52.3) | 34.5 (16.3–51.8) | 33.5 (19.8–64.5) | 0.817 |
| Sex | 0.888 | |||
| Female | 55 (53.9) | 37 (54.4) | 18 (52.9) | |
| Male | 47 (46.1) | 31 (45.6) | 16 (47.1) | |
| Long tumor diameter (cm) | 9.4 (6.5–12.0) | 10.2 (7.0–12.0) | 7.6 (5.1–12.1) | 0.094 |
| INPC group | 0.287 | |||
| favorable | 31 (30.4) | 23 (33.8) | 8 (23.5) | |
| unfavorable | 71 (69.6) | 45 (66.2) | 26 (76.5) | |
| MYCN status | 0.553 | |||
| Amplified | 15 (14.7) | 9 (13.2) | 6 (17.6) | |
| Not amplified | 87 (85.3) | 59 (86.8) | 28 (82.4) | |
| INRG stage | 0.447 | |||
| L1, L2, MS | 31 | 19 (27.9) | 12 (35.3) | |
| M | 71 | 49 (72.1) | 22 (64.7) | |
| COG risk group | 0.923 | |||
| low | 14 (13.7) | 7 (10.3) | 7 (20.6) | |
| intermediate | 21 (20.6) | 17 (25.0) | 4 (11.8) | |
| high | 67 (65.7) | 44 (64.7) | 23 (67.6) | |
| Mitosis-karyorrhexis index | 0.572 | |||
| Low | 58 (56.9) | 40 (58.8) | 18 (52.9) | |
| Intermediate and high | 44 (43.1) | 28 (41.2) | 16 (47.1) | |
| PET/CT findings | ||||
| SUVmax | 4.8 (3.9–6.1) | 4.7 (4.0–6.2) | 4.9 (2.9–6.0) | 0.580 |
| SUVmean | 2.0 (1.6–2.5) | 2.0 (1.6–2.6) | 1.9 (1.4–2.5) | 0.482 |
| MTV (mL) | 167.7 (72.9–397.5) | 192.9 (92.8–389.4) | 126.9 (35.8–473.6) | 0.194 |
| TLG | 348.5 (141.4–848.6) | 391.8 (160.7–776.6) | 206.3 (68.9–1028.8) | 0.191 |
| Initial laboratory findings | ||||
| NSE (ng/mL) | 219.1 (65.4–626.3) | 192.3 (69.3–531.1) | 282.8 (47.9–686.6) | 0.683 |
| LDH (IU/L) | 553.5 (341.8–1018.3) | 495.0 (348.8–1046.8) | 591.5 (339.3–998.3) | 0.790 |
| Ferritin (ng/mL) | 118.3 (59.2–318.4) | 117.2 (48.4–300.9) | 150.9 (69.8–503.5) | 0.407 |
| HVA (μmol/L) | 35.6 (11.0–107.2) | 37.4 (13.8–111.9) | 23.2 (3.9–103.4) | 0.233 |
| VMA (μmol/L) | 149.5 (31.1–537.0) | 188.1 (41.8–544.8) | 106.8 (27.3–464.7) | 0.268 |
| Characteristics | Training Set | Validation Set | ||||
|---|---|---|---|---|---|---|
| Low (n = 40) | Intermediate/High (n = 28) | p Value | Low (n = 18) | Intermediate/High (n = 16) | p Value | |
| Age at diagnosis (months) | 39.5 (16.3–52.8) | 30 (16.3–47.8) | 0.537 | 41 (20.8–69.0) | 26.5 (16.0–38.5) | 0.164 |
| Sex | 0.541 | 1.000 | ||||
| Female | 23 (57.5) | 14 (50.0) | 10 (55.6) | 8 (50.0) | ||
| Male | 17 (42.5) | 14 (50.0) | 8 (44.4) | 8 (50.0) | ||
| Long tumor diameter (cm) | 8.5 (6.5–11.9) | 10.6 (9.0–12.2) | 0.079 | 6.7 (4.6–12.6) | 9.9 (5.8–11.9) | 0.325 |
| INPC group | 0.198 | 0.693 | ||||
| favorable | 16 (40.0) | 7 (25.0) | 5 (27.8) | 3 (18.8) | ||
| unfavorable | 24 (60.0) | 21 (75.0) | 13 (72.2) | 13 (81.3) | ||
| MYCN status | 0.192 | 0.387 | ||||
| Amplified | 3 (7.5) | 6 (21.4) | 2 (11.1) | 4 (25.0) | ||
| Not amplified | 37 (92.5) | 22 (78.6) | 16 (88.9) | 12 (75.0) | ||
| INRG stage | 0.651 | 0.729 | ||||
| L1, L2, MS | 12 (30.0) | 7 (25.0) | 7 (38.9) | 5 (31.3) | ||
| M | 28 (70.0) | 21 (75.0) | 11 (61.1) | 11 (68.8) | ||
| COG risk group | 0.707 | 0.443 | ||||
| low | 4 (10.0) | 3 (10.7) | 5 (27.8) | 2 (12.5) | ||
| intermediate | 11 (27.5) | 6 (21.4) | 2 (11.1) | 2 (12.5) | ||
| high | 25 (62.5) | 19 (67.9) | 11 (61.1) | 12 (75.0) | ||
| PET/CT findings | ||||||
| SUVmax | 4.4 (4.0–5.8) | 5.0 (4.1–6.7) | 0.174 | 4.3 (2.4–5.9) | 5.5 (4.1–6.2) | 0.102 |
| SUVmean | 1.9 (1.6–2.4) | 2.2 (1.7–2.7) | 0.148 | 1.7 (1.3–2.3) | 2.3 (1.6–2.9) | 0.050 |
| MTV (mL) | 185.9 (80.8–389.4) | 218.3 (127.8–396.1) | 0.360 | 68.5 (8.6–257.4) | 239.7 (80.8–565.9) | 0.088 |
| TLG | 369.9 (141.2–644.7) | 567.1 (211.9–1054.1) | 0.204 | 138.6 (12.0–640.8) | 593.9 (157.3–1463.4) | 0.039 |
| Initial laboratory findings | ||||||
| NSE (ng/mL) | 177.7 (60.7–340.6) | 260.2 (91.3–747.9) | 0.195 | 143.1 (28.3–552.3) | 459.0 (141.7–736.9) | 0.164 |
| LDH (IU/L) | 485 (357.3–738.8) | 762 (329.0–1418.5) | 0.189 | 545.0 (285.0–896.5) | 659.0 (358.0–1019.0) | 0.246 |
| Ferritin (ng/mL) | 111.8 (42.8–269.1) | 138.1 (65.2–358.5) | 0.294 | 302.3 (42.1–687.9) | 117.1 (90.3–210.2) | 0.297 |
| HVA (μmol/L) | 39.5 (22.3–101.9) | 31.6 (8.7–152.6) | 0.451 | 63.8 (3.4–153.8) | 20.5 (4.0–47.5) | 0.589 |
| VMA (μmol/L) | 255.3 (79.3–587.3) | 59.2 (23.9–375.7) | 0.052 | 195.2 (27.2–614.0) | 48.1 (27.7–290.0) | 0.650 |
| Model | Training Set | Validation Set | ||
|---|---|---|---|---|
| AUC (95%CI) | p | AUC (95%CI) | p | |
| radiomics model | 0.982 (0.916–0.999) | 0.955 (0.823–0.997) | ||
| clinical model | 0.746 (0.625–0.843) | 0.670 (0.488–0.821) | ||
| combined model | 0.988 (0.924–1.000) | 0.951 (0.818–0.996) | ||
| radiomics model vs clinical model | 0.0001 | 0.0086 | ||
| radiomics model vs combined model | 0.2625 | 0.8807 | ||
| clinical model vs combined model | <0.0001 | 0.0046 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, L.; Qian, L.; Yang, S.; Ren, Q.; Zhang, S.; Qin, H.; Wang, W.; Wang, C.; Zhang, H.; Yang, J. Prediction for Mitosis-Karyorrhexis Index Status of Pediatric Neuroblastoma via Machine Learning Based 18F-FDG PET/CT Radiomics. Diagnostics 2022, 12, 262. https://doi.org/10.3390/diagnostics12020262
Feng L, Qian L, Yang S, Ren Q, Zhang S, Qin H, Wang W, Wang C, Zhang H, Yang J. Prediction for Mitosis-Karyorrhexis Index Status of Pediatric Neuroblastoma via Machine Learning Based 18F-FDG PET/CT Radiomics. Diagnostics. 2022; 12(2):262. https://doi.org/10.3390/diagnostics12020262
Chicago/Turabian StyleFeng, Lijuan, Luodan Qian, Shen Yang, Qinghua Ren, Shuxin Zhang, Hong Qin, Wei Wang, Chao Wang, Hui Zhang, and Jigang Yang. 2022. "Prediction for Mitosis-Karyorrhexis Index Status of Pediatric Neuroblastoma via Machine Learning Based 18F-FDG PET/CT Radiomics" Diagnostics 12, no. 2: 262. https://doi.org/10.3390/diagnostics12020262
APA StyleFeng, L., Qian, L., Yang, S., Ren, Q., Zhang, S., Qin, H., Wang, W., Wang, C., Zhang, H., & Yang, J. (2022). Prediction for Mitosis-Karyorrhexis Index Status of Pediatric Neuroblastoma via Machine Learning Based 18F-FDG PET/CT Radiomics. Diagnostics, 12(2), 262. https://doi.org/10.3390/diagnostics12020262