


Is the Diagnosis of Generalized Stage IV (Severe) Periodontitis Compatible with the Survival of Extended Stabilizing Prosthetic Restorations? A Medium-Term Retrospective Study


 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
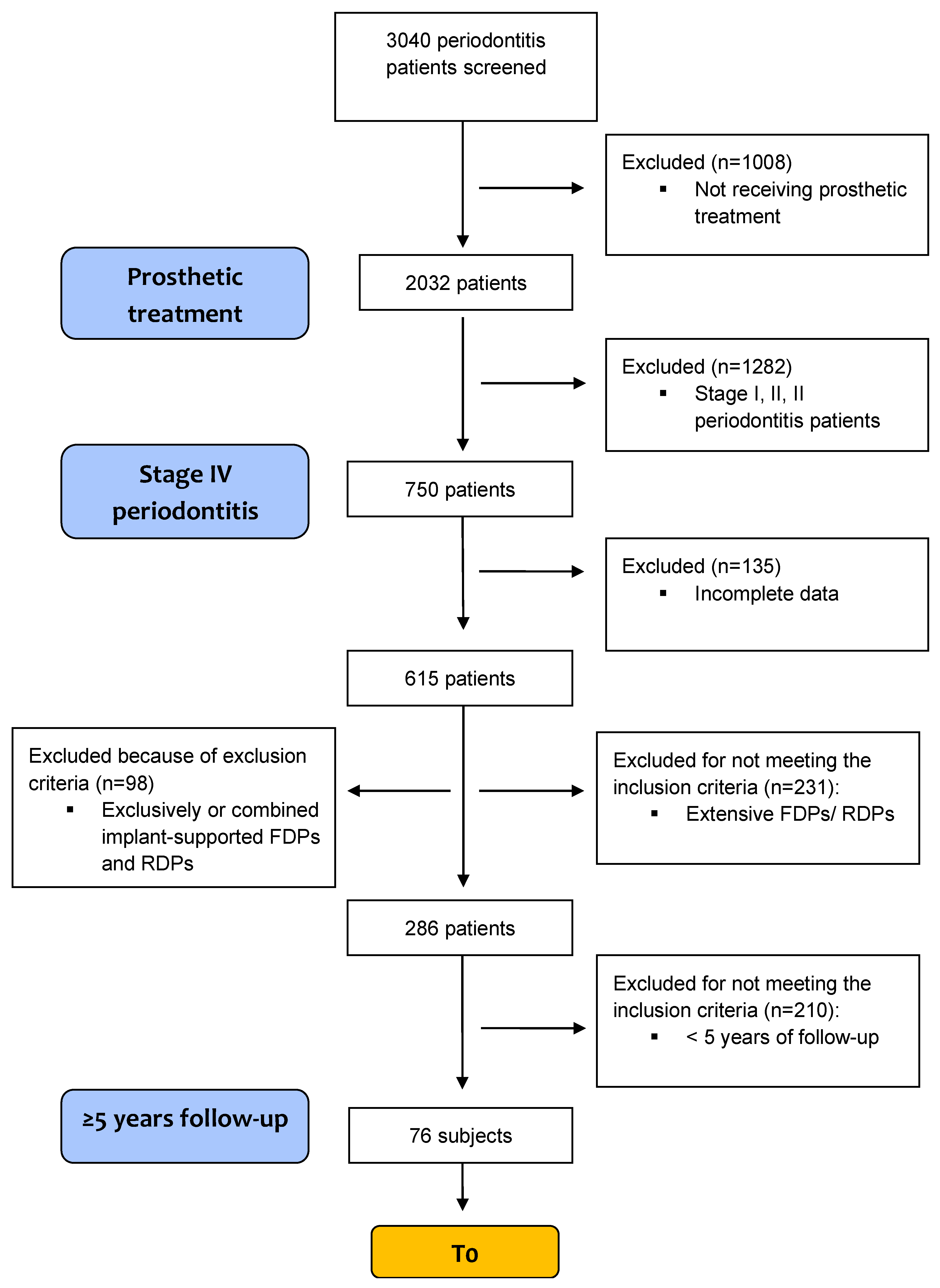
2.1. Study Population
2.1.1. Inclusion Criteria
- Patients that underwent APT and attended SPT in the same private practice in Timisoara, Romania;
- Intraoral or panoramic radiograph available at T0 and T1;
- Completion of APT at least 5 years prior to last examination. If the prosthodontic reconstruction was lost after fewer than 5 years, the respective period of function was included in the analysis;
- Extensive FDPs (bridge with at least six units, i.e., abutments and pontics, and supported exclusively by teeth) and/or RDPs with at least four abutment teeth.
2.1.2. Exclusion Criteria
- Exclusively- or combined implant-supported FDPs and RDPs;
- Re-examination period ≤ 5 years, or discontinuation of therapy by the patient.
2.2. Periodontal Treatment
2.3. Patient’s Charts Evaluation
2.4. Evaluation of Radiographs
2.5. Prosthetic/Rehabilitation Considerations and Follow-Up
2.6. Statistical Analysis
3. Results
3.1. Demographics
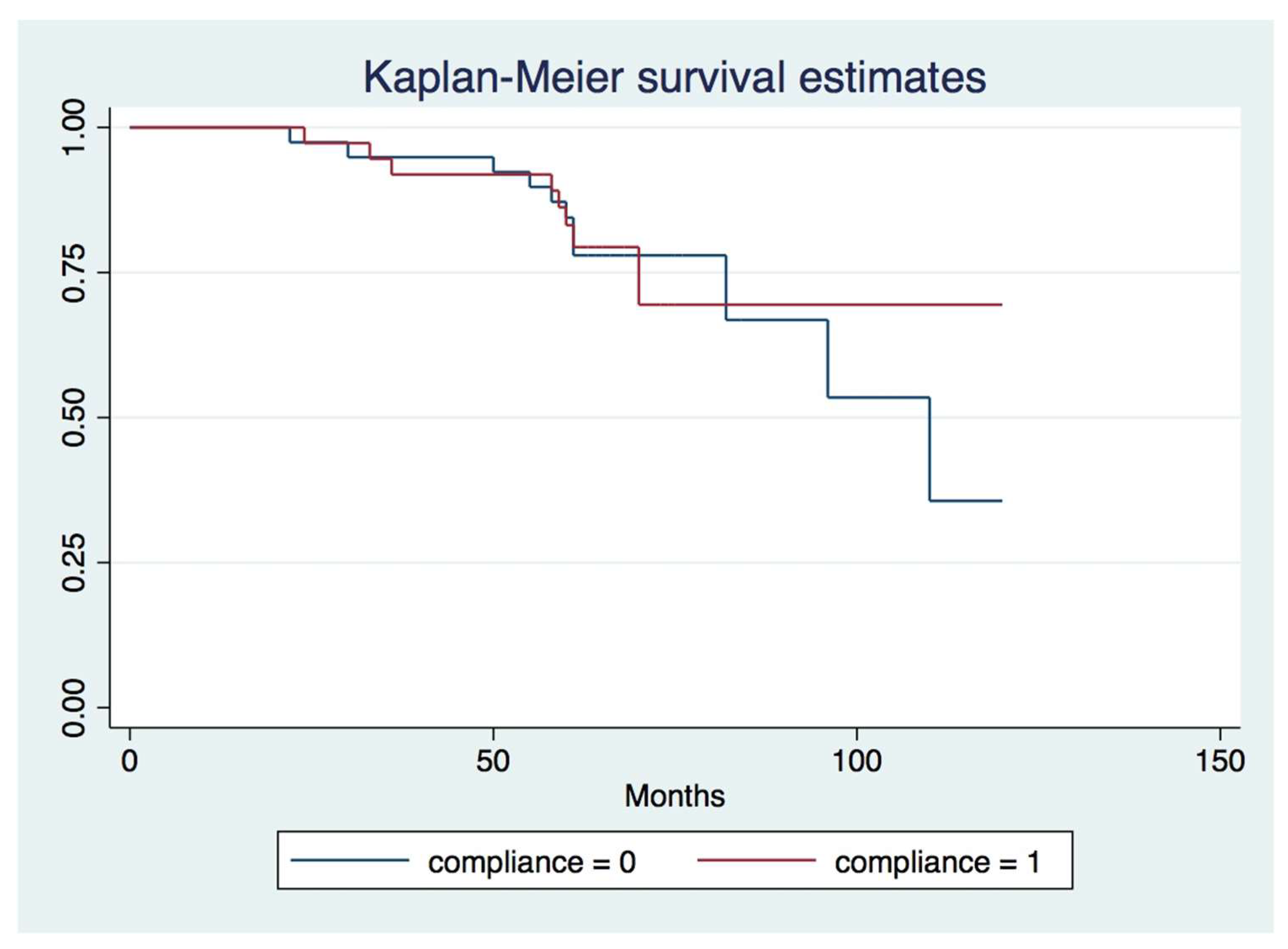
3.2. Survival Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pretzl, B.; Kaltschmitt, J.; Kim, T.S.; Reitmeir, P.; Eickholz, P. Tooth loss after active periodontal therapy. 2: Tooth-related factors: Tooth-related factors for tooth loss. J. Clin. Periodontol. 2008, 35, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Hirschfeld, L.; Wasserman, B. A Long-Term Survey of Tooth Loss in 600 Treated Periodontal Patients. J. Periodontol. 1978, 49, 225–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farooqi, O.A.; Wehler, C.J.; Gibson, G.; Jurasic, M.M.; Jones, J.A. Appropriate recall interval for periodontal maintenance: A systematic review. J. Evid. Based Dent. Pract. 2015, 15, 171–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Wet, L.M.; Slot, D.E.; Van der Weijden, G.A. Supportive periodontal treatment: Pocket depth changes and tooth loss. Int. J. Dent. Hyg. 2018, 16, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Matuliene, G.; Pjetursson, B.E.; Salvi, G.E.; Schmidlin, K.; Brägger, U.; Zwahlen, M.; Lang, N.P. Influence of residual pockets on progression of periodontitis and tooth loss: Results after 11 years of maintenance. J. Clin. Periodontol. 2008, 35, 685–695. [Google Scholar] [CrossRef] [PubMed]
- Graetz, C.; Plaumann, A.; Schlattmann, P.; Kahl, M.; Springer, C.; Sälzer, S.; Gomer, K.; Dörfer, C.; Schwendicke, F. Long-term tooth retention in chronic periodontitis—Results after 18 years of a conservative periodontal treatment regimen in a university setting. J. Clin. Periodontol. 2017, 44, 169–177. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Steffen, P.; Muller-Campanile, V.; Suvan, J.; Lang, N.P. Initial extractions and tooth loss during supportive care in a periodontal population seeking comprehensive care: Extractions in periodontal patients. J. Clin. Periodontol. 2000, 27, 824–831. [Google Scholar] [CrossRef] [Green Version]
- Machtei, E.E.; Hirsch, I. Retention of Hopeless Teeth: The Effect on the Adjacent Proximal Bone Following Periodontal Surgery. J. Periodontol. 2007, 78, 2246–2252. [Google Scholar] [CrossRef] [Green Version]
- Graetz, C.; Dörfer, C.E.; Kahl, M.; Kocher, T.; Fawzy El-Sayed, K.; Wiebe, J.F.; Gomer, K.; Rühling, A. Retention of questionable and hopeless teeth in compliant patients treated for aggressive periodontitis: Retention of questionable and hopeless teeth. J. Clin. Periodontol. 2011, 38, 707–714. [Google Scholar] [CrossRef] [Green Version]
- Checchi, L.; Montevecchi, M.; Gatto, M.R.A.; Trombelli, L. Retrospective study of tooth loss in 92 treated periodontal patients: Tooth loss in treated patients. J. Clin. Periodontol. 2002, 29, 651–656. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, S159–S172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yi, S.W.; Ericsson, I.; Carlsson, G.E.; Wennström, J.L. Long-term follow-up of cross-arch fixed partial dentures in patients with ad- vanced periodontal destruction Evaluation of the supporting tissues. Acta Odontol. Scand. 1995, 53, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Geramy, A.; Adibrad, M.; Sahabi, M. The effects of splinting periodontally compromised removable partial denture abutments on bone stresses: A three-dimensional finite element study. J. Dent. Sci. 2010, 5, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lundgren, D.; Nyman, S.; Heijl, L.; Carlsson, G.E. Functional analysis of fixed bridges on abutment teeth with reduced periodontal support. J. Oral Rehabil. 1975, 2, 105–116. [Google Scholar] [CrossRef]
- Lundgren, D.; Laurell, L. Occlusal forces in prosthetically restored dentitions: A methodological study. J. Oral Rehabil. 1984, 11, 29–37. [Google Scholar] [CrossRef]
- Lundgren, D.; Laurell, L. Occlusal force pattern during chewing and biting in dentitions restored with fixed bridges of cross-arch extension: I. Bilateral end abutments. J. Oral Rehabil. 1986, 13, 57–71. [Google Scholar] [CrossRef]
- Laurell, L.; Lundgren, D. Periodontal ligament areas and occlusal forces in dentitions restored with cross-arch bilateral end abut- ment bridges. J. Clin. Periodontol. 1985, 12, 850–860. [Google Scholar] [CrossRef]
- Laurell, L.; Lundgren, D. Chewing ability in patients restored with cross-arch fixed partial dentures. J. Prosthet. Dent. 1985, 54, 720–725. [Google Scholar] [CrossRef]
- Fardal, Ø.; Linden, G.J. Long-term outcomes for cross-arch stabilizing bridges in periodontal maintenance patients—A retrospective study. J. Clin. Periodontol. 2010, 37, 299–304. [Google Scholar] [CrossRef]
- Müller, S.; Eickholz, P.; Reitmeir, P.; Eger, T. Long-term tooth loss in periodontally compromised but treated patients according to the type of prosthodontic treatment. A retrospective study. J. Oral Rehabil. 2013, 40, 358–367. [Google Scholar] [CrossRef]
- Cabanilla, L.L.L.; Neely, A.L.; Hernandez, F. The relationship between periodontal diagnosis and prognosis and the survival of prosthodontic abutments: A retrospective study. Quintessence Int. 2009, 40, 821–831. [Google Scholar] [PubMed]
- Wenz, H.J.; Hertrampf, K.; Lehmann, K.M. Clinical longevity of removable partial dentures retained by telescopic crowns: Outcome of the double crown with clearance fit. Int. J. Prosthodont. 2001, 14, 207–213. [Google Scholar] [PubMed]
- Seo, J.G.; Cho, J.H. Clinical outcomes of rigid and non-rigid telescopic double-crown-retained removable dental prostheses: An analytical review. J. Adv. Prosthodont. 2020, 12, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ante, I.H. The fundamental principles of abutment. Mich. D Soc. Bull. 1926, 8, 14–23. [Google Scholar]
- Lulic, M.; Brägger, U.; Lang, N.P.; Zwahlen, M.; Salvi, G.E. Ante’s (1926) law revisited: A systematic review on survival rates and complications of fixed dental prostheses (FDPs) on severely reduced periodontal tissue support. Clin. Oral Implant. Res. 2007, 18, 63–72. [Google Scholar] [CrossRef]
- Nyman, S.; Lindhe, J. A longitudinal study of combined periodontal and prosthetic treatment of patients with advanced periodontal disease. J. Periodontol. 1979, 50, 163–169. [Google Scholar] [CrossRef] [Green Version]
- Faggion, C.M.; Petersilka, G.; Lange, D.E.; Gerss, J.; Flemmig, T.F. Prognostic model for tooth survival in patients treated for periodon- titis. J. Clin. Periodontol. 2007, 34, 226–231. [Google Scholar] [CrossRef]
- McGuire, M.K.; Nunn, M.E. Prognosis Versus Actual Outcome. III. The Effectiveness of Clinical Parameters in Accurately Predicting Tooth Survival. J. Periodontol. 1996, 67, 666–674. [Google Scholar] [CrossRef] [Green Version]
- Chambrone, L.A.; Chambrone, L. Tooth loss in well-maintained patients with chronic periodontitis during long-term supportive therapy in Brazil. J. Clin. Periodontol. 2006, 33, 759–764. [Google Scholar] [CrossRef]
- Dannewitz, B.; Krieger, J.K.; Husing, J.; Eickholz, P. Loss of molars in periodontally treated patients: A retrospective analysis five years or more after active periodontal treatment. J. Clin. Periodontol. 2006, 33, 53–61. [Google Scholar] [CrossRef]
- Leung, W.K.; Ng, D.K.C.; Jin, L.; Corbet, E.F. Tooth loss in treated periodontitis patients responsible for their supportive care arrangements. J. Clin. Periodontol. 2006, 33, 265–275. [Google Scholar] [CrossRef]
- Eickholz, P.; Kaltschmitt, J.; Berbig, J.; Reitmeir, P.; Pretzl, B. Tooth loss after active periodontal therapy. 1: Patient-related factors for risk, prognosis, and quality of outcome: Patient-related factors for tooth loss. J. Clin. Periodontol. 2008, 35, 165–174. [Google Scholar] [CrossRef]
- Muzzi, L.; Nieri, M.; Cattabriga, M.; Rotundo, R.; Cairo, F.; Pini Prato, G.P. The Potential Prognostic Value of Some Periodontal Factors for Tooth Loss: A Retrospective Multilevel Analysis on Periodontal Patients Treated and Maintained Over 10 Years. J. Periodontol. 2006, 77, 2084–2089. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Bernal, G.; Rungcharassaeng, K.; Kan, J.Y. Clinical complications in fixed prosthodontics. J. Prosthet. Dent. 2003, 90, 31–41. [Google Scholar] [CrossRef] [Green Version]
- Raustia, A.M.; Näpänkangas, R.; Salonen, M.A.M. Complications and primary failures related to fixed metal ceramic bridge prostheses made by dental students. J. Oral Rehabil. 1998, 25, 677–680. [Google Scholar] [CrossRef]
- Hämmerle, C.H.; Ungerer, M.C.; Fantoni, P.C.; Brägger, U.; Bürgin, W.; Lang, N.P. Long-term analysis of biologic and technical aspects of fixed partial dentures with cantilevers. Int. J. Prosthodont. 2000, 13, 409–415. [Google Scholar]
- Owall, B.; Cronström, R. First two-year complications of fixed partial dentures, eight units or more. Swedish Guarantee Insurance claims. Acta Odontol. Scand. 2000, 58, 72–76. [Google Scholar] [CrossRef]
- Walton, J.N. A randomized clinical trial comparing two mandibular implant overdenture designs: 3-year prosthetic outcomes using a six-field protocol. J. Prosthet. Dent. 2003, 90, 570. [Google Scholar] [CrossRef]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berglundh, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S.; Aimetti, M.; et al. Treatment of stage IV periodontitis: The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2022, 49, 4–71. [Google Scholar] [CrossRef]
- Graetz, C.; Schwendicke, F.; Kahl, M.; Dörfer, C.E.; Sälzer, S.; Springer, C.; Schützhold, S.; Kocher, T.; König, J.; Rühling, A. Prosthetic rehabilitation of patients with history of moderate to severe periodontitis: A long-term evaluation. J. Clin. Periodontol. 2013, 40, 799–806. [Google Scholar] [CrossRef]
- Quirynen, M.; Bollen, C.M.L.; Vandekerckhove, B.N.A.; Dekeyser, C.; Papaioannou, W.; Eyssen, H. Full- vs. Partial-mouth Disinfection in the Treatment of Periodontal Infections: Short-term Clinical and Microbiological Observations. J. Dent. Res. 1995, 74, 1459–1467. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; on behalf of the EFP Workshop Participants and Methodological Consultants. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef] [PubMed]
- Al-Shammari, K.F.; Kazor, C.E.; Wang, H.L. Molar root anatomy and management of furcation defects: Molar root anatomy and furcations. J. Clin. Periodontol. 2001, 28, 730–740. [Google Scholar] [CrossRef]
- Fardal, O.; Linden, G.J. Re-treatment profiles during long-term maintenance therapy in a periodontal practice in Norway. J. Clin. Periodontol. 2005, 32, 744–749. [Google Scholar] [CrossRef]
- Bäumer, A.; Pretzl, B.; Cosgarea, R.; Kim, T.S.; Reitmeir, P.; Eickholz, P.; Dannewitz, B. Tooth loss in aggressive periodontitis after active periodontal therapy: Patient-related and tooth-related prognostic factors: Prognostic factors for tooth loss. J. Clin. Periodontol. 2011, 38, 644–651. [Google Scholar] [CrossRef]
- Miller, S.C. Textbook of Periodontia (p. 91); Blakiston and Company: Philadelphia, PA, USA, 1950. [Google Scholar]
- Hamp, S.E.; Nyman, S.; Lindhe, J. Periodontal treatment of multi rooted teeth.. Results after 5 years. J. Clin. Periodontol. 1975, 2, 126–135. [Google Scholar] [CrossRef]
- Lang, N.P.; Tonetti, M.S. Periodontal risk assessment (PRA) for patients in supportive periodontal therapy (SPT). Oral Health Prev. Dent. 2003, 1, 7–16. [Google Scholar] [PubMed]
- Stadler, A.F.; Mendez, M.; Oppermann, R.V.; Gomes, S.C. Tooth Loss in Patients under Periodontal Maintenance in a Private Practice: A Retrospective Study. Braz. Dent. J. 2017, 28, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Costa, F.O.; Miranda Cota, L.O.; Pereira Lages, E.J.; Lima Oliveira, A.P.; Cortelli, S.C.; Cortelli, J.R.; Medeiros Lorentz, T.C.; Costa, J.E. Periodontal risk assessment model in a sample of regular and irregular compliers under maintenance therapy: A 3-year prospective study. J. Periodontol. 2012, 83, 292–300. [Google Scholar] [CrossRef]
- Costa, F.O.; Lages, E.J.P.; Cota, L.O.M.; Lorentz, T.C.M.; Soares, R.V.; Cortelli, J.R. Tooth loss in individuals under periodontal maintenance therapy: 5-year prospective study. J. Periodontal Res. 2014, 49, 121–128. [Google Scholar] [CrossRef]
- Lindhe, J.; Nyman, S.; Lang, N.P. Treatment planning. Clin. Periodontol. Implant. Dent. 2003, 3, 420–437. [Google Scholar]
- Valderhaug, J.; Ellingsen, J.E.; Jokstad, A. Oral hygiene, periodontal conditions and carious lesions in patients treated with dental bridges: A 15-year clinical and radiographic follow-up study. J. Clin. Periodontol. 1993, 20, 482–489. [Google Scholar] [CrossRef] [PubMed]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Laurell, L.; Lundgren, D.; Falk, H.; Hugoson, A. Long-term prognosis of extensive polyunit cantilevered fixed partial dentures. J. Prosthet. Dent. 1991, 66, 545–552. [Google Scholar] [CrossRef]
- Karlsson, S. Failures and length of service in fixed prosthodontics after long-term function. A longitudinal clinical study. Swed. Dent. J. 1989, 13, 185–192. [Google Scholar]
- Svärdström, G.; Wennström, J.L. Periodontal treatment decisions for molars: An analysis of influencing factors and long-term outcome. J. Periodontol. 2000, 71, 579–585. [Google Scholar] [CrossRef]
- Reichen-Graden, S.; Lang, N.P. Periodontal and pulpal conditions of abutment teeth. Status after four to eight years following the incorporation of fixed reconstructions. Schweiz. Mon. Fur Zahnmed. = Rev. Mens. Suisse D’odonto-Stomatol. = Riv. Mens. Svizz. Di Odontol. E Stomatol. 1989, 99, 1381–1385. [Google Scholar]
- Hegdahl, T.; Silness, J. Preparation areas resisting displacement of artificial crowns. J. Oral Rehabil. 1977, 4, 201–207. [Google Scholar] [CrossRef]
- Pjetursson, B.E.; Lang, N.P. Prosthetic treatment planning on the basis of scientific evidence. J. Oral Rehabil. 2008, 35, 72–79. [Google Scholar] [CrossRef]
- Brägger, U.; Hirt-Steiner, S.; Schnell, N.; Schmidlin, K.; Salvi, G.E.; Pjetursson, B.; Matuliene, G.; Zwahlen, M.; Lang, N.P. Complication and failure rates of fixed den tal prostheses in patients treated for periodontal disease. Clin. Oral Implant. Res. 2011, 22, 70–77. [Google Scholar] [CrossRef]
- Naumann, M.; von Stein-Lausnitz, M.; Rosentritt, M.; Walter, C.; Meyer-Lückel, H.; Sterzenbach, G. Impact of simulated reduced alveolar bone support, increased tooth mobility, and distal post-supported, root-treated abutment tooth on load capability of all-ceramic zirconia-supported cantilever FDP. Clin. Oral Investig. 2018, 22, 2799–2807. [Google Scholar] [CrossRef]
- Uzgur, Z.; Uzgur, R.; Çolak, H.; Ercan, E.; Dallı, M. Analysis of Endodontic Complications Following Fixed Prosthodontic Rehabilitation. Int. J. Prosthodont. 2016, 29, 565–569. [Google Scholar] [CrossRef] [Green Version]
- Heling, I.; Gorfil, C.; Slutzky, H.; Kopolovic, K.; Zalkind, M.; Slutzky-Goldberg, I. Endodontic failure caused by inadequate restorative procedures: Review and treatment recommendations. J. Prosthet. Dent. 2002, 87, 674–678. [Google Scholar] [CrossRef]
- Bergenholtz, G.; Nyman, S. Endodontic complications following periodontal and prosthetic treatment of patients with advanced periodontal disease. J. Periodontol. 1984, 55, 63–68. [Google Scholar] [CrossRef]
- Tada, S.; Allen, P.F.; Ikebe, K.; Matsuda, K.I.; Maeda, Y. Impact of periodontal maintenance on tooth survival in patients with removable partial dentures. J. Clin. Periodontol. 2015, 42, 46–53. [Google Scholar] [CrossRef]
- Matsuda, K.I.; Ikebe, K.; Enoki, K.; Tada, S.; Fujiwara, K.; Maeda, Y. Incidence and association of root fractures after prosthetic treatment. J. Prosthodont. Res. 2011, 55, 137–140. [Google Scholar] [CrossRef]
- Martin-Cabezas, R.; Seelam, N.; Petit, C.; Agossa, K.; Gaertner, S.; Tenenbaum, H.; Davideau, J.L.; Huck, O. Association between periodontitis and arterial hypertension: A systematic review and meta-analysis. Am. Heart J. 2016, 180, 98–112. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Frequency | Percent | |
|---|---|---|
| Sex (n, %) | ||
| F | 41 | 53.95 |
| M | 35 | 46.05 |
| Age (years, mean ± SD) | ||
| 57.3 ± 7.70 | ||
| Smoking Status (N, %) | ||
| Smoker | 7 | 9.21 |
| Non-smoker | 69 | 90.79 |
| Compliance | ||
| ICs | 39 | 51.32 |
| RCs | 37 | 48.68 |
| Systemic Disorders (N, %) | ||
| Unreported | 69 | 90.79 |
| Cardiovascular (HTN, IHD) | 3 | 3.95 |
| Autoimmune | 1 | 1.32 |
| DM type II | 3 | 3.95 |
| RDPs (19) | FDPs (57) | |
|---|---|---|
| Compliance N(%) | ||
| ICs | 11 (57.89) | 28 (49.12) |
| RCs | 8 (42.10) | 29 (50.87) |
| Jaw, N(%) | ||
| Mandible | 3 (15.78) | 17 (29.82%) |
| Maxilla | 16 (84.21) | 40 (70,17%) |
| Type of preparation, N(%) | ||
| Supragingial | - | 3 (5.26) |
| Subgingival | 19 (100) | 56 (94.74) |
| Edentation according to Kennedy’s Classification, N(%) | ||
| Class I | 14 (73.6) | - |
| Class II | 4 (21.05) | - |
| Class III | 1 (0.52) | 56 (94.73) |
| Class IV | - | 1 (1.75) |
| Usage period (months, mean± SD) | 71.9371.93 ± 17.88 | 66.84 ± 14.15 |
| Abutment teeth, N | 105 | 436 |
| Pontic units, N | 27 | 127 |
| No Tooth Loss (N, %) | Periodontal (N, %) | Endo-Perio (N, %) | Fracture (N, %) | Overall p-Value | |
|---|---|---|---|---|---|
| Type of tooth | |||||
| No tooth loss | 57 (100) | - | - | - | * 0.000 |
| Incisor | - | 2 (66.67) | 0 (0.00) | 1 (33.33) | |
| Premolar | - | 6 (85.71) | 1 (14.29) | ||
| Molar | - | 8 (88.89) | 1 (11.11) | - | |
| Smoking status | |||||
| Smoker | 6 (85.71) | 1 (14.29) | - | - | 1.000 |
| Non-smoker | 51 (73.91) | 15 (21.74) | 1 (1.45) | 2 (2.90) | |
| Systemic diseases | |||||
| Reported as healthy | 53 (76.81) | 14 (20.29) | - | 2 (2.90) | * 0.033 |
| Cardio-vascular | 1 (33.33) | 2 (66.67) | - | - | |
| Autoimmune | 1 (100) | ||||
| DM type II | 3 (100) | - | - | - | |
| Sex | |||||
| Female | 33 (80.49) | 5 (12.20) | 1 (2.44) | 2 (4.88) | 0.067 |
| Male | 24 (68.57) | 11 (31.43) | - | - | |
| RDPs N, (%) | FDPs N, (%) | p-Value | |
|---|---|---|---|
| Technical complications | |||
| Ceramic fracture | 3 (10.53) | 3 (5.26) | 0.108 |
| Mobility | 4 (5.26) | 4 (7.02) | |
| Loss of retention | 3 (21.05) | 3 (5.26) | |
| No complications | 47 (63.16) | 47 (82.46) | |
| Biological complications | |||
| No complications | 16 (84.21) | 55 (96.49) | 0.04 * |
| Root caries | 1 (5.26) | 2 (3.51) | |
| Endo Complications | 2 (10.53) | - | |
| PPD | CAL | FMBS | FMPS | RBL | ||
|---|---|---|---|---|---|---|
| Baseline | ICs | 2.85 ± 0.30 | 3.10 ± 0.46 | 16.92 ± 5.09 | 9.94 ± 5.37 | 60.1 ± 9.58 |
| RCs | 2.76 ± 0.29 | 3.28 ± 0.55 | 15.08 ± 7.20 | 9.54 ± 5.28 | 63.10 ± 9.14 | |
| p-value a | 0.16 | 0.12 | 0.20 | 0.73 | 0.17 | |
| Final examination | ICs | 3.56 ± 0.53 | 3.90 ± 0.66 | 31.07 ± 13.36 | 16.33 ± 7.56 | 65.97 ± 14.87 |
| RCs | 3.31 ± 0.53 | 3.92 ± 0.62 | 24.40 ± 11.76 | 13.70 ± 8.53 | 68.13 ± 9.87 | |
| p-value a | 0.04 * | 0.88 | 0.02 * | 0.15 | 0.46 | |
| Difference to baseline | ICs | 0.70 ± 0.40 | 0.8 ± 0.52 | 14.15 ± 11.50 | 6.38 ± 4.39 | 5.84 ± 9.63 |
| RCs | 0.55 ± 0.38 | 0.64 ± 0.38 | 9.32 ± 10.02 | 4.16 ± 6.57 | 5.02 ± 3.73 | |
| p-value b | 0.63 | 0.10 | 0.05 | 0.13 | 0.08 |
| ICs | p-Value | RCs | p-Value | |||
|---|---|---|---|---|---|---|
| T0 | T1 | T0 | T1 | |||
| PPD | 2.85 ± 0.30 | 3.56 ± 0.53 | 0.00 * | 2.76 ± 0.29 | 3.31 ± 0.53 | 0.00 * |
| difference | 0.70 ± 0.40 | 0.55 ± 0.38 | ||||
| CAL | 3.10 ± 0.46 | 3.90 ± 0.66 | 0.00 * | 3.28 ± 0.55 | 3.92 ± 0.62 | 0.00 * |
| difference | 0.8 ± 0.52 | 0.64 ± 0.38 | ||||
| FMBS | 16.92 ± 5.09 | 31.07 ± 13.36 | 0.00 * | 15.08 ± 7.20 | 24.40 ± 11.76 | 0.00 * |
| difference | 14.15 ± 11.50 | 9.32 ± 10.02 | ||||
| FMPS | 9.94 ± 5.37 | 16.33 ± 7.56 | 0.00 * | 9.54 ± 5.28 | 13.70 ± 8.53 | 0.00 * |
| difference | 6.38 ± 4.39 | 4.16 ± 6.57 | ||||
| RBL | 60.12 ± 9.58 | 65.97 ± 14.87 | 0.00 * | 63.10 ± 9.14 | 68.13 ± 9.87 | 0.00 * |
| difference | 5.84 ± 9.63 | 5.02 ± 3.73 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rădulescu, V.; Boariu, M.; Rusu, D.; Boldeanu, C.; Christodorescu, R.; Roman, A.; Surlin, P.; Didilescu, A.C.; Vela, O.; Kardaras, G.; et al. Is the Diagnosis of Generalized Stage IV (Severe) Periodontitis Compatible with the Survival of Extended Stabilizing Prosthetic Restorations? A Medium-Term Retrospective Study. Diagnostics 2022, 12, 3053. https://doi.org/10.3390/diagnostics12123053
Rădulescu V, Boariu M, Rusu D, Boldeanu C, Christodorescu R, Roman A, Surlin P, Didilescu AC, Vela O, Kardaras G, et al. Is the Diagnosis of Generalized Stage IV (Severe) Periodontitis Compatible with the Survival of Extended Stabilizing Prosthetic Restorations? A Medium-Term Retrospective Study. Diagnostics. 2022; 12(12):3053. https://doi.org/10.3390/diagnostics12123053
Chicago/Turabian StyleRădulescu, Viorelia, Marius Boariu, Darian Rusu, Camelia Boldeanu, Ruxandra Christodorescu, Alexandra Roman, Petra Surlin, Andreea Cristiana Didilescu, Octavia Vela, Giorgios Kardaras, and et al. 2022. "Is the Diagnosis of Generalized Stage IV (Severe) Periodontitis Compatible with the Survival of Extended Stabilizing Prosthetic Restorations? A Medium-Term Retrospective Study" Diagnostics 12, no. 12: 3053. https://doi.org/10.3390/diagnostics12123053
APA StyleRădulescu, V., Boariu, M., Rusu, D., Boldeanu, C., Christodorescu, R., Roman, A., Surlin, P., Didilescu, A. C., Vela, O., Kardaras, G., Veja, I., Martu, I., & Stratul, S.-I. (2022). Is the Diagnosis of Generalized Stage IV (Severe) Periodontitis Compatible with the Survival of Extended Stabilizing Prosthetic Restorations? A Medium-Term Retrospective Study. Diagnostics, 12(12), 3053. https://doi.org/10.3390/diagnostics12123053