

Risk of Mortality Prediction Involving Time-Varying Covariates for Patients with Heart Failure Using Deep Learning
 ,
,
Abstract
1. Introduction
2. Materials and Methods
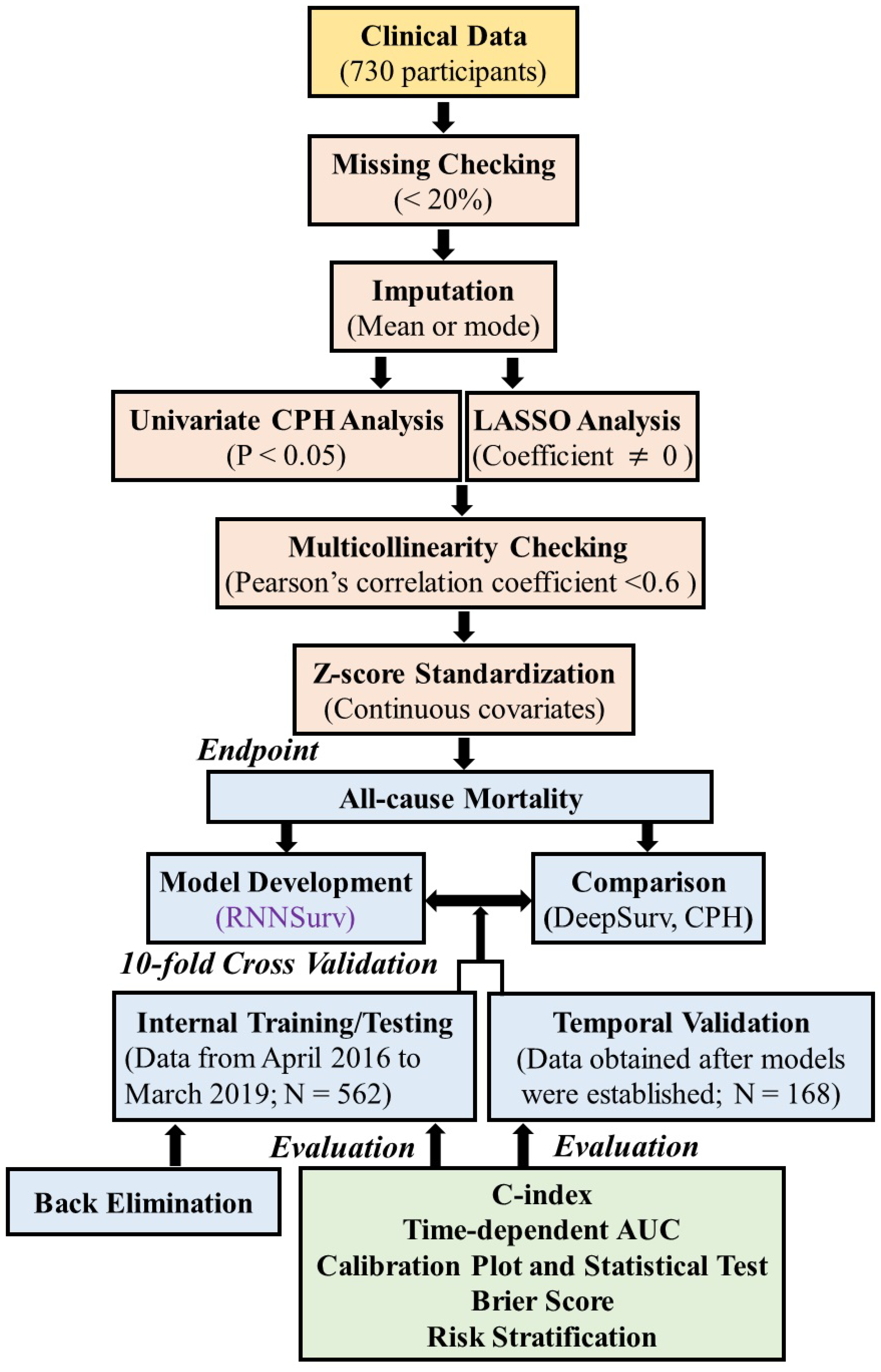
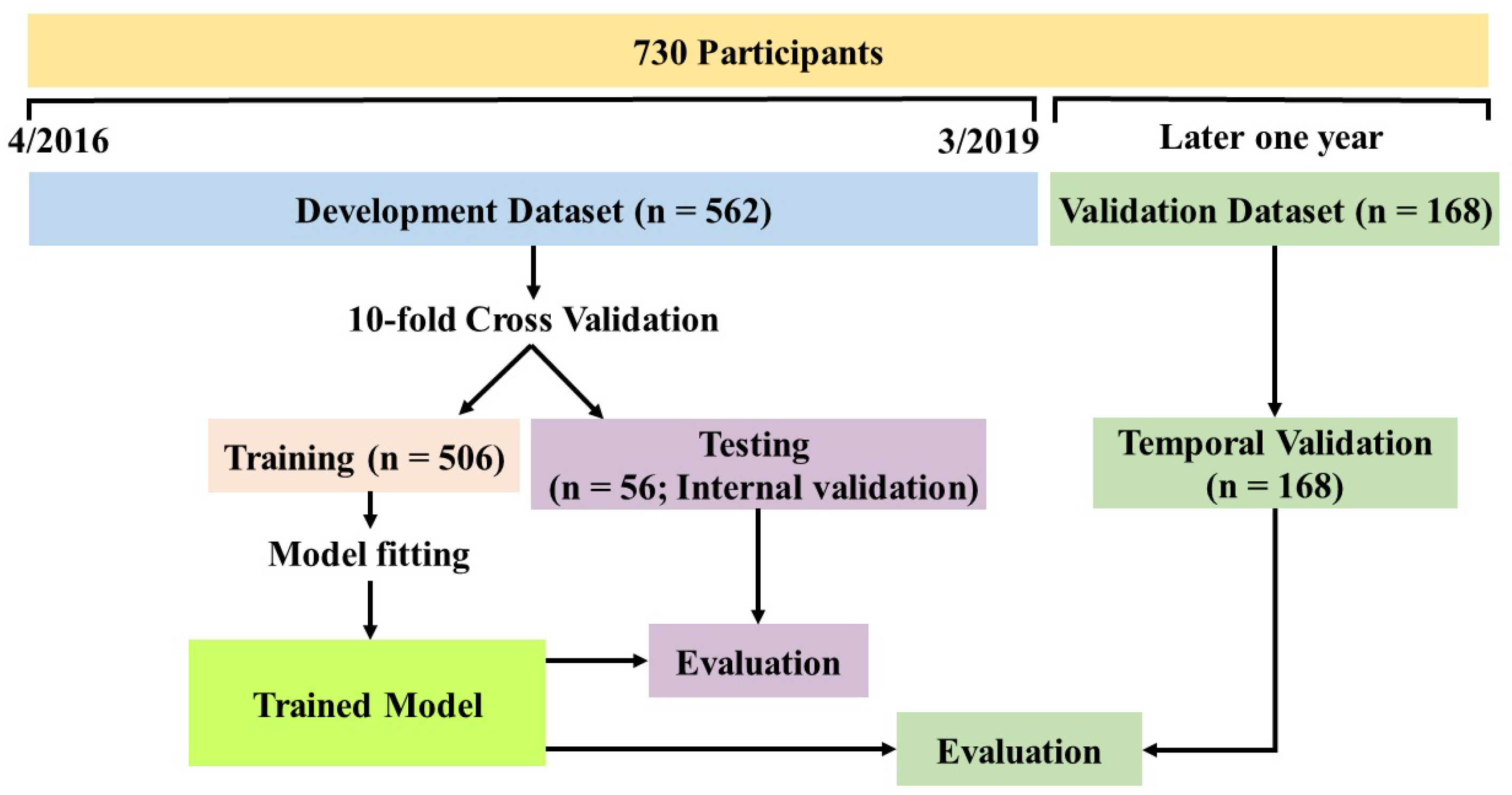
2.1. Study Design and Data Collection
2.2. Outcome Definition
2.3. Preprocessing and Statistical Analysis
2.4. Model Development and Validation
2.5. Performance Evaluation
3. Results
3.1. Characteristics of Patients and Candidate Predictors
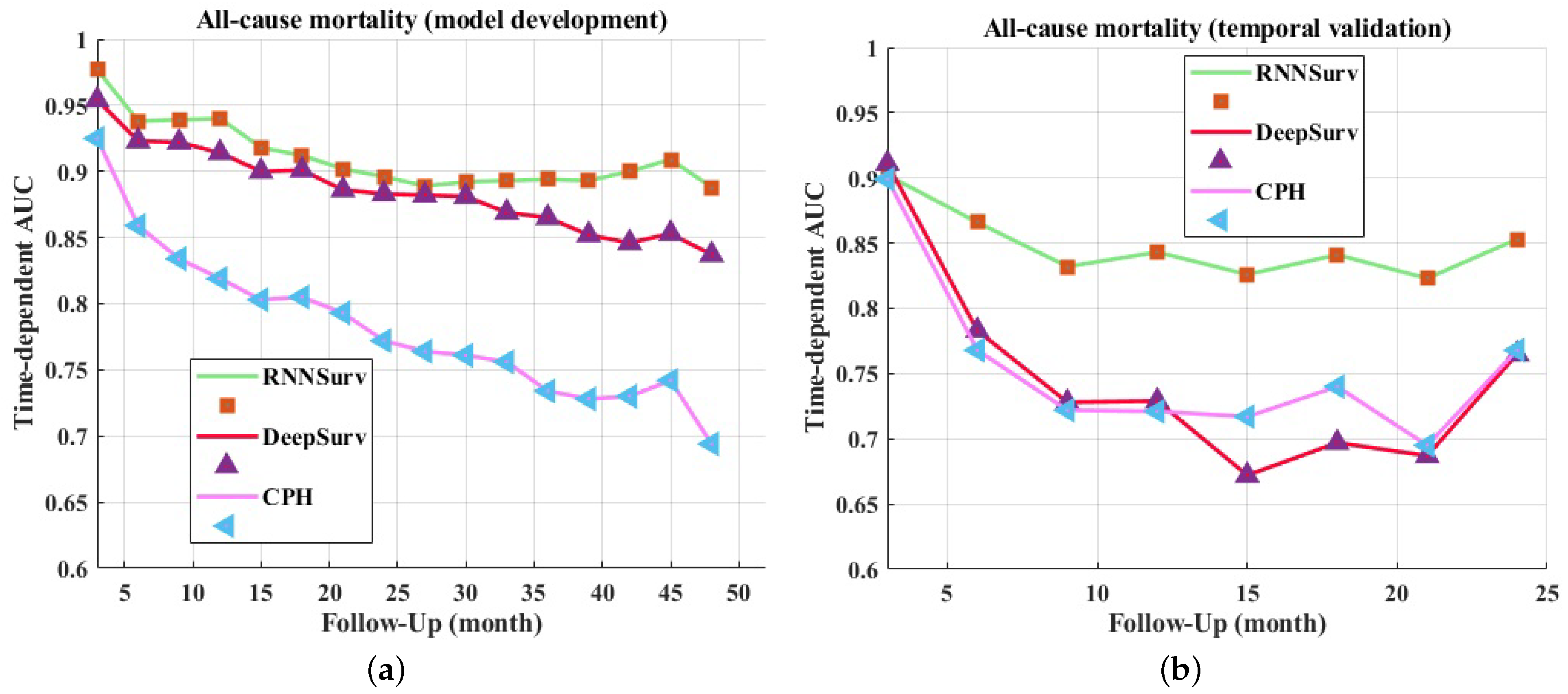
3.2. Discrimination Evaluation
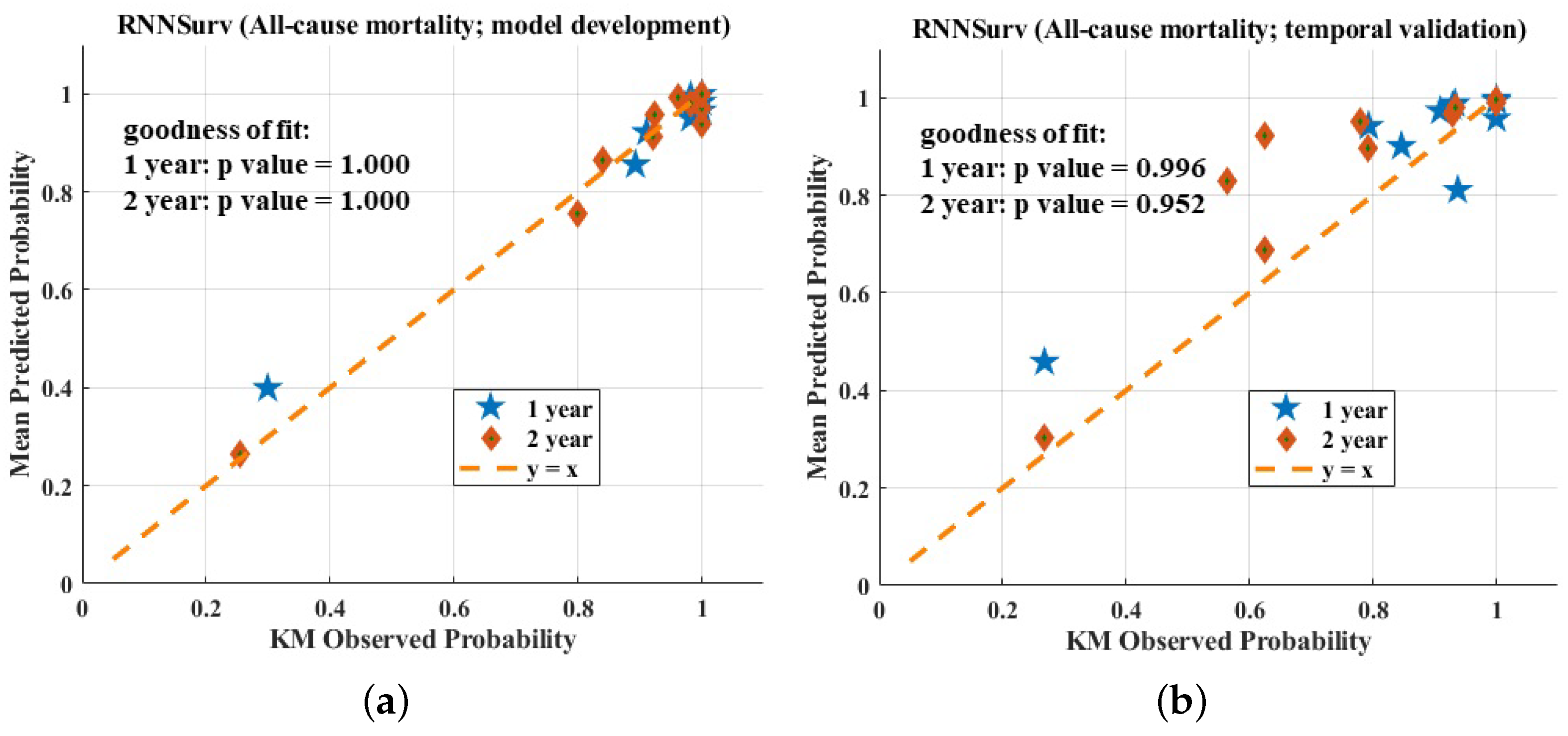
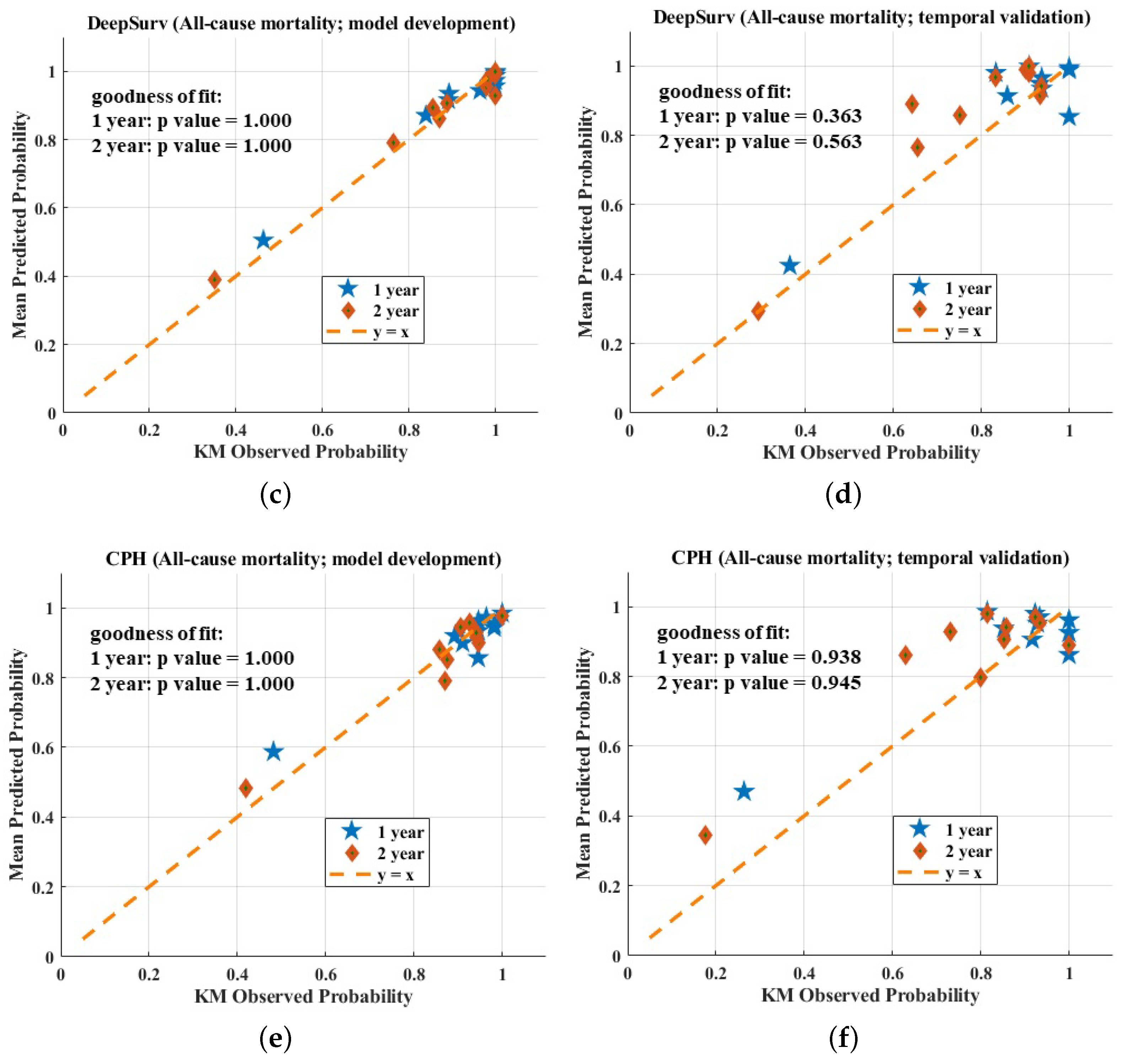
3.3. Calibration Evaluation
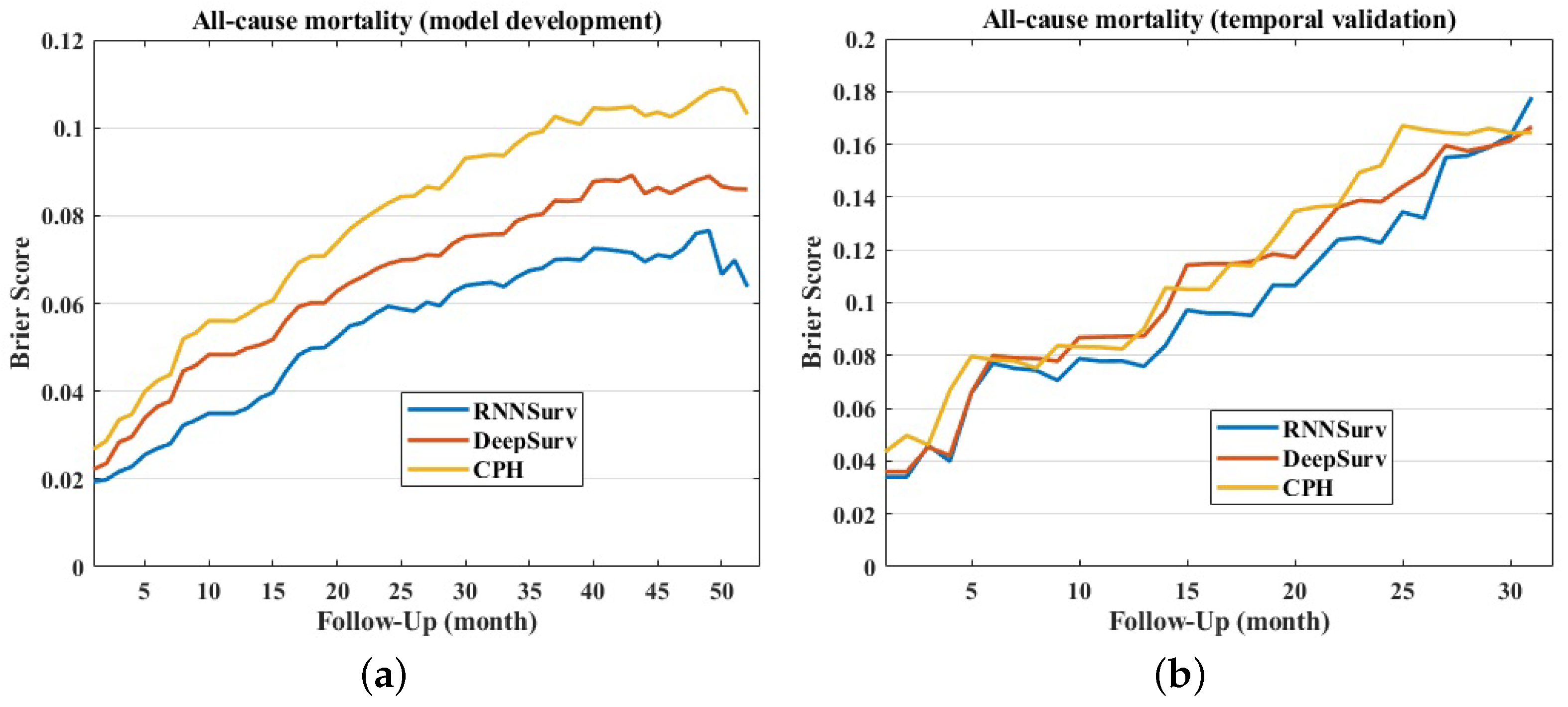
3.4. Overall Evaluation
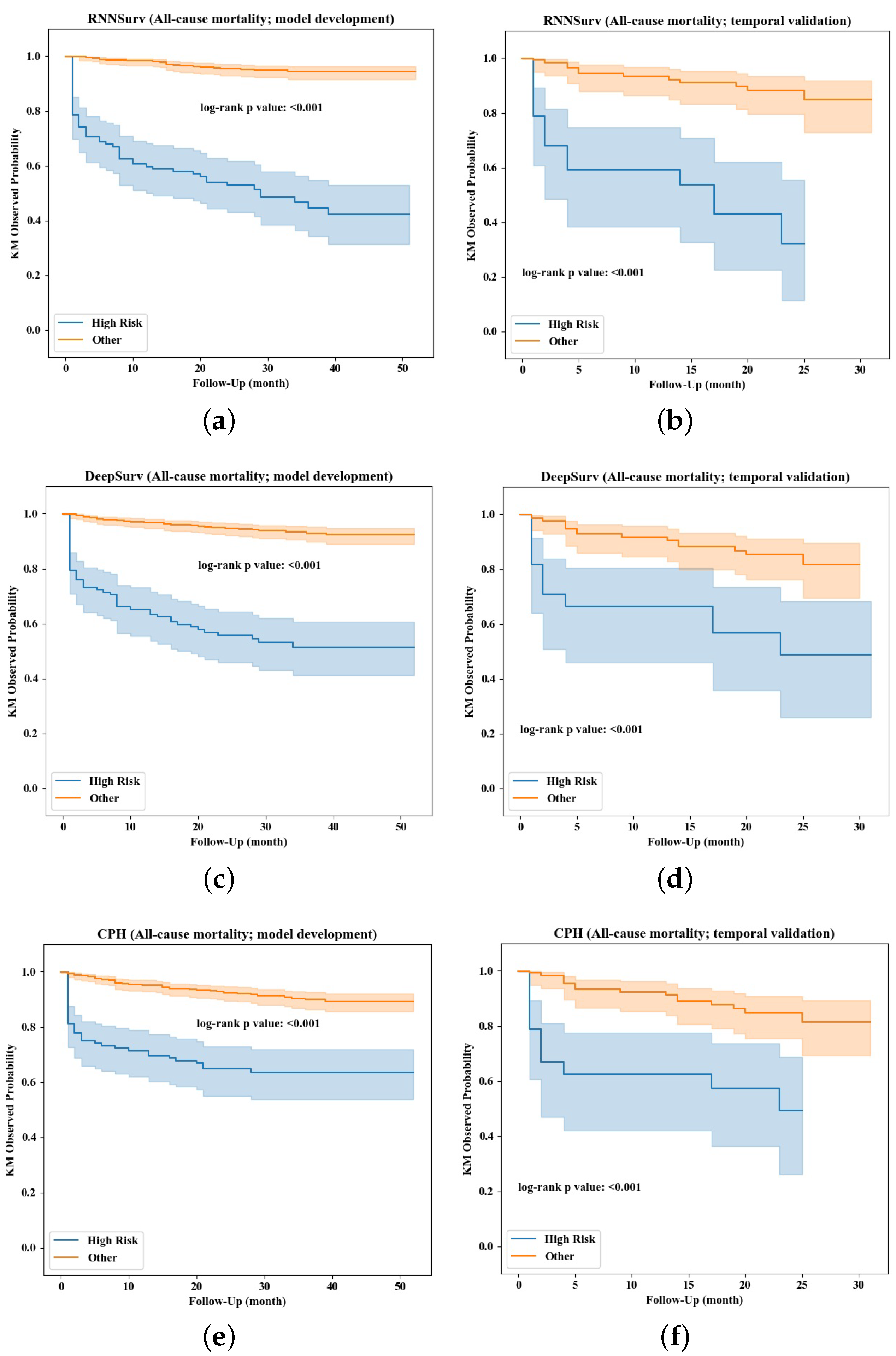
3.5. Risk Stratification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ACEi/ARB | Angiotensin-converting enzyme inhibitor/angiotensin receptor blocker |
| ADL | Activities of daily living |
| AUC | Area under receiver operating characteristic curve |
| BMI | Body mass index |
| CPH | Cox proportional hazard |
| CRP | C-reactive protein |
| DBP | Diastolic blood pressure |
| DPC | Diagnosis procedure combination |
| eGFR | Estimated glomerular filtration rate |
| FC | Fully connected |
| HF | Heart failure |
| HGB | Hemoglobin |
| HR | Heart rate |
| HR_A | HR measured at admission |
| HR_A | HR measured at discharge |
| IHD | Ischemic heart disease |
| IDL | Independence in daily life for the elderly with cognitive impairment |
| LVEF | Left ventricular ejection fraction |
| MR | Mitral regurgitation |
| NT-proBNP | NT-proB-type natriuretic peptide |
| NYHA | New York Heart Association |
| RNN | Recurrent neural network |
| RVSP | Right ventricular systolic pressure |
| SBP | Systolic blood pressure |
| TR | Tricuspid regurgitation |
| VD | Vfascular disease |
References
- Roger, V.L. Epidemiology of heart failure: A contemporary perspective. Circ. Res. 2021, 128, 1421–1434. [Google Scholar] [CrossRef]
- McMurray, J.J.; Stewart, S. Epidemiology, aetiology, and prognosis of heart failure. Heart 2000, 83, 596–602. [Google Scholar] [CrossRef]
- Okura, Y.; Ramadan, M.M.; Ohno, Y.; Mitsuma, W.; Tanaka, K.; Ito, M.; Suzuki, K.; Tanabe, N.; Kodama, M.; Aizawa, Y. Impending epidemic: Future projection of heart failure in Japan to the year 2055. Circ. J. 2008, 72, 489–491. [Google Scholar] [CrossRef]
- Hamaguchi, S.; Kinugawa, S.; Tsuchihashi-Makaya, M.; Goto, D.; Yamada, S.; Yokoshiki, H.; Tsutsui, H. Characteristics, management, and outcomes for patients during hospitalization due to worsening heart failure—A report from the Japanese Cardiac Registry of Heart Failure in Cardiology (JCARE-CARD). J. Cardiol. 2013, 62, 95–101. [Google Scholar] [CrossRef]
- Kanaoka, K.; Okayama, S.; Nakai, M.; Sumita, Y.; Nishimura, K.; Kawakami, R.; Okura, H.; Miyamoto, Y.; Yasuda, S.; Tsutsui, H.; et al. Hospitalization costs for patients with acute congestive heart failure in Japan. Circ. J. 2019, 83, 1025–1031. [Google Scholar] [CrossRef]
- Cox, D.R. Regression models and life-tables. J. R. Stat. Soc. Ser. B (Methodol.) 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Kim, D.W.; Lee, S.; Kwon, S.; Nam, W.; Cha, I.; Kim, H.J. Deep learning-based survival prediction of oral cancer patients. Sci. Rep. 2019, 9, 6994. [Google Scholar] [CrossRef]
- Hathaway, Q.A.; Yanamala, N.; Budoff, M.J.; Sengupta, P.P.; Zeb, I. Deep neural survival networks for cardiovascular risk prediction: The Multi-Ethnic Study of Atherosclerosis (MESA). Comput. Biol. Med. 2021, 139, 104983. [Google Scholar] [CrossRef]
- Katzman, J.L.; Shaham, U.; Cloninger, A.; Bates, J.; Jiang, T.; Kluger, Y. DeepSurv: Personalized treatment recommender system using a Cox proportional hazards deep neural network. BMC Med. Res. Methodol. 2018, 18, 24. [Google Scholar] [CrossRef]
- She, Y.; Jin, Z.; Wu, J.; Deng, J.; Zhang, L.; Su, H.; Jiang, G.; Liu, H.; Xie, D.; Cao, N.; et al. Development and validation of a deep learning model for non–small cell lung cancer survival. JAMA Netw. Open. 2020, 3, e205842. [Google Scholar] [CrossRef]
- Liang, W.; Yao, J.; Chen, A.; Lv, Q.; Zanin, M.; Liu, J.; Wong, S.; Li, Y.; Lu, J.; Liang, H.; et al. Early triage of critically ill COVID-19 patients using deep learning. Nat. Commun. 2020, 11, 3543. [Google Scholar] [CrossRef]
- Fisher, L.D.; Lin, D.Y. Time-dependent covariates in the Cox proportional-hazards regression model. Annu. Rev. Public Health 1999, 20, 145–157. [Google Scholar] [CrossRef]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef]
- Zhou, X.; Nakamura, K.; Sahara, N.; Asami, M.; Toyoda, Y.; Enomoto, Y.; Hara, H.; Noro, M.; Sugi, K.; Moroi, M.; et al. Exploring and identifying prognostic phenotypes of patients with heart failure guided by explainable machine learning. Life 2022, 12, 776. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Čelutkienė, J.; Chioncel, O.; Cleland, J.G.F.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar]
- Kodama, K.; Sakamoto, T.; Kubota, T.; Takimura, H.; Hongo, H.; Chikashima, H.; Shibasaki, Y.; Yada, T.; Node, K.; Nakayama, T.; et al. Construction of a heart failure database collating administrative claims data and electronic medical record data to evaluate risk factors for in-hospital death and prolonged hospitalization. Circ. Rep. 2019, 1, 582–592. [Google Scholar] [CrossRef]
- Park, S.Y.; Park, J.E.; Kim, H.; Park, S.H. Review of statistical methods for evaluating the performance of survival or other time-to-event prediction models (from conventional to deep learning approaches). Korean J. Radiol. 2021, 22, 1697–1707. [Google Scholar] [CrossRef]
- Zhou, X.; Nakamura, K.; Sahara, N.; Takagi, T.; Toyoda, Y.; Enomoto, Y.; Hara, H.; Noro, M.; Sugi, K.; Moroi, M.; et al. Deep learning-based recurrence prediction of atrial fibrillation after catheter ablation. Circ. J. 2022, 86, 299–308. [Google Scholar] [CrossRef]
- Ng, K.; Steinhubl, S.R.; deFilippi, C.; Dey, S.; Stewart, W.F. Early detection of heart failure using electronic health records: Practical implications for time before diagnosis, data diversity, data quantity, and data density. Circ. Cardiovasc. Qual. Outcomes 2016, 9, 649–658. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. B 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Mesquita, J.; Ferreira, A.M.; Cavaco, D.; Moscoso Costa, F.; Carmo, P.; Marques, H.; Morgado, F.; Mendes, M.; Adragão, P. Development and validation of a risk score for predicting atrial fibrillation recurrence after a first catheter ablation procedure–ATLAS score. EP Eur. 2018, 20, f428–f435. [Google Scholar] [CrossRef]
- Shalabi, L.A.; Shaaban, Z.; Kasasbeh, B. Data mining: A preprocessing engine. J. Comput. Sci. 2006, 2, 735–739. [Google Scholar] [CrossRef]
- Harrell, F.E.; Califf, R.M.; Pryor, D.B.; Lee, K.L.; Rosati, R.A. Evaluating the yield of medical tests. JAMA 1982, 247, 2543–2546. [Google Scholar] [CrossRef]
- Lambert, J.; Chevret, S. Summary measure of discrimination in survival models based on cumulative/dynamic time-dependent ROC curves. Stat. Methods Med. Res. 2016, 25, 2088–2102. [Google Scholar] [CrossRef]
- Park, S.H.; Han, K. Methodologic guide for evaluating clinical performance and effect of artificial intelligence technology for medical diagnosis and prediction. Radiology 2018, 286, 800–809. [Google Scholar] [CrossRef]
- Brier, G.W. Verification of forecasts expressed in terms of probability. Mon. Weather Rev. 1950, 78, 1–3. [Google Scholar] [CrossRef]
- Wang, P.; Li, Y.; Reddy, C.K. Machine learning for survival analysis: A survey. ACM Comput. Surv. 2019, 51, 1–36. [Google Scholar] [CrossRef]
- Bazoukis, G.; Stavrakis, S.; Zhou, J.; Bollepalli, S.C.; Tse, G.; Zhang, Q.; Singh, J.P.; Armoundas, A.A. Machine learning versus conventional clinical methods in guiding management of heart failure patients—A systematic review. Heart Fail. Rev. 2021, 26, 23–34. [Google Scholar] [CrossRef]
- Liu, S.; Yang, Z.; Pan, K.; Zhu, X.; Chen, W. Estimation of left ventricular ejection fraction using cardiovascular hemodynamic parameters and pulse morphological characteristics with machine learning lgorithms. Nutrients 2022, 14, 4051. [Google Scholar] [CrossRef]
- Levy, W.C.; Mozaffarian, D.; Linker, D.T.; Sutradhar, S.C.; Anker, S.D.; Cropp, A.B.; Anand, I.; Maggioni, A.; Burton, P.; Sullivan, M.D.; et al. The Seattle Heart Failure Model: Prediction of survival in heart failure. Circulation 2016, 113, 1424–1433. [Google Scholar] [CrossRef]
- Mentz, R.J.; Mulder, H.; Mosterd, A.; Sweitzer, N.K.; Senni, M.; Butler, J.; Ezekowitz, J.A.; Lam, C.S.P.; Pieske, B.; Ponikowski, P.; et al. Clinical outcome predictions for the VerICiguaT Global Study in subjects with heart failure with reduced ejection fraction (VICTORIA) trial: VICTORIA outcomes model. J. Card. Fail. 2021, 27, 949–956. [Google Scholar] [CrossRef]
- Simpson, J.; Jhund, P.S.; Lund, L.H.; Padmanabhan, S.; Claggett, B.L.; Shen, L. Prognostic models derived in PARADIGM-HF and validated in ATMOSPHERE and the Swedish Heart Failure Registry to predict mortality and morbidity in chronic heart failure. JAMA Cardiol. 2020, 5, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, F.; Torp-Pedersen, C.; Seibaek, M.; Burchardt, H.; Køber, L.; DIAMOND study group. Effect of age on short and long-term mortality in patients admitted to hospital with congestive heart failure. Eur. Heart J. 2004, 25, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Kajimoto, K.; Sato, N.; Investigators of the Acute Decompensated Heart Failure Syndromes (ATTEND) Registry. Sex differences in New York Heart Association functional classification and survival in acute heart failure patients with preserved or reduced ejection fraction. Can. J. Cardiol. 2020, 36, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Shamagian, L.G.; Román, A.V.; Pérez, M.P.; Otero, I.G.; Lamela, A.V.; González-Juanatey, J.R. Renal failure is an independent predictor of mortality in hospitalized heart failure patients and is associated with a worse cardiovascular risk profile. Rev. Esp. Cardiol. 2006, 59, 99–108. [Google Scholar] [CrossRef]
- Rudolf, H.; Mügge, A.; Trampisch, H.J.; Scharnagl, H.; März, W.; Kara, K. NT-proBNP for risk prediction of cardiovascular events and all-cause mortality: The getABI-study. Int. J. Cardiol. Heart Vasc. 2020, 29, 100553. [Google Scholar] [CrossRef] [PubMed]
- Dunlay, S.M.; Manemann, S.M.; Chamberlain, A.M.; Cheville, A.L.; Jiang, R.; Weston, S.A.; Roger, V.L. Activities of daily living and outcomes in heart failure. Circ. Heart Fail. 2015, 8, 261–267. [Google Scholar] [CrossRef]
- Gohbara, M.; Nishimura, K.; Nakai, M.; Sumita, Y.; Endo, T.; Matsuzawa, Y.; Konishi, M.; Kosuge, M.; Ebina, T.; Tamura, K.; et al. Low activities of daily living associated with increased cardiovascular disease mortality in Japan: Analysis of health records from a Nationwide Claim-Based Database, JROAD-DPC. Circ. Rep. 2019, 1, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, I.; Wong, M.V.; Huang, J.K.F.; Gong, M.; Waleed, K.B.; Xia, Y.; Lee, S.; Roever, L.; Liu, T.; Tse, G.; et al. Diagnostic and prognostic value of serum C-reactive protein in heart failure with preserved ejection fraction: A systematic review and meta-analysis. Heart Fail. Rev. 2021, 26, 1141–1150. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | Model Development (10-Fold Cross Validation) | Validation | All of the Data | Predictors |
|---|---|---|---|---|
| RNNSurv | Train: 0.820 ± 0.022 Test: 0.807 ± 0.057 | 0.809 ± 0.022 (RNNSuev vs. DeepSurv: p value < 0.001; (RNNSuev vs. CPH: p value < 0.001;) | Development: 0.890 Validation: 0.839 | Invariant predictors: Age, length of stay, IHD, NYHA at discharge, frailty, LVEF, TR, ACEi/ARB, NT-proBNP, HGB; Time-varying predictors: eGFR, SBP, DBP, HR, low ADL |
| DeepSurv | Train: 0.818 ± 0.033 Test: 0.783 ± 0.066 | 0.762 ± 0.022 | Development: 0.872 Validation: 0.755 | Age, length of stay, IHD, LVEF, RVSP, HGB, ACEi/ARB, IDL, NT-proBNP, (NYHA, eGFR, SBP, DBP, HR, low ADL) at discharge |
| CPH | Train: 0.768 ± 0.010 Test: 0.754 ± 0.069 | 0.764 ± 0.002 | Development: 0.767 Validation: 0.762 | Length of stay, IDL, ACEi/ARB, NT-proBNP, (NYHA, eGFR, SBP, low ADL) at discharge |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakamura, K.; Zhou, X.; Sahara, N.; Toyoda, Y.; Enomoto, Y.; Hara, H.; Noro, M.; Sugi, K.; Huang, M.; Moroi, M.; et al. Risk of Mortality Prediction Involving Time-Varying Covariates for Patients with Heart Failure Using Deep Learning. Diagnostics 2022, 12, 2947. https://doi.org/10.3390/diagnostics12122947
Nakamura K, Zhou X, Sahara N, Toyoda Y, Enomoto Y, Hara H, Noro M, Sugi K, Huang M, Moroi M, et al. Risk of Mortality Prediction Involving Time-Varying Covariates for Patients with Heart Failure Using Deep Learning. Diagnostics. 2022; 12(12):2947. https://doi.org/10.3390/diagnostics12122947
Chicago/Turabian StyleNakamura, Keijiro, Xue Zhou, Naohiko Sahara, Yasutake Toyoda, Yoshinari Enomoto, Hidehiko Hara, Mahito Noro, Kaoru Sugi, Ming Huang, Masao Moroi, and et al. 2022. "Risk of Mortality Prediction Involving Time-Varying Covariates for Patients with Heart Failure Using Deep Learning" Diagnostics 12, no. 12: 2947. https://doi.org/10.3390/diagnostics12122947
APA StyleNakamura, K., Zhou, X., Sahara, N., Toyoda, Y., Enomoto, Y., Hara, H., Noro, M., Sugi, K., Huang, M., Moroi, M., Nakamura, M., & Zhu, X. (2022). Risk of Mortality Prediction Involving Time-Varying Covariates for Patients with Heart Failure Using Deep Learning. Diagnostics, 12(12), 2947. https://doi.org/10.3390/diagnostics12122947