

Anterior Cruciate Ligament Tear Detection Based on Deep Convolutional Neural Network


Abstract
:1. Introduction
- The investigation of CPDCNN for improving the deep feature discrimination to represent the complex features of knee MRI images for ACL tear detection;
- The performance estimation of the proposed CPDCNN using the public MRNet dataset based on various evaluation metrics such as accuracy, precision, recall rate, and the F1 score.
2. Related Work
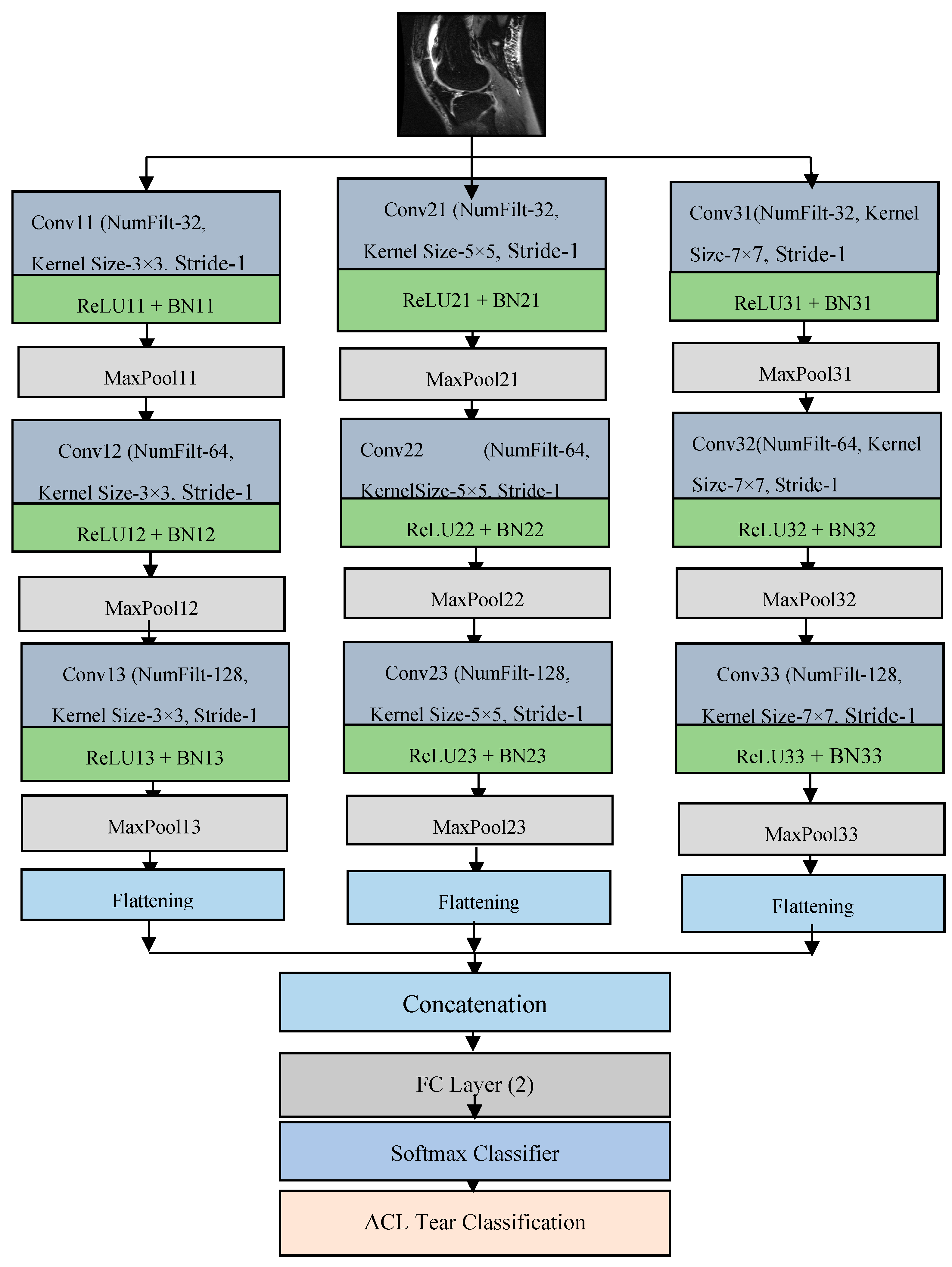
3. Proposed Methodology
3.1. Convolutional Layer
3.2. ReLU Layer
3.3. Batch Normalization
3.4. Maximum Pooling Layer
3.5. Fully Connected Layer
3.6. Softmax Layer
4. Experimental Results
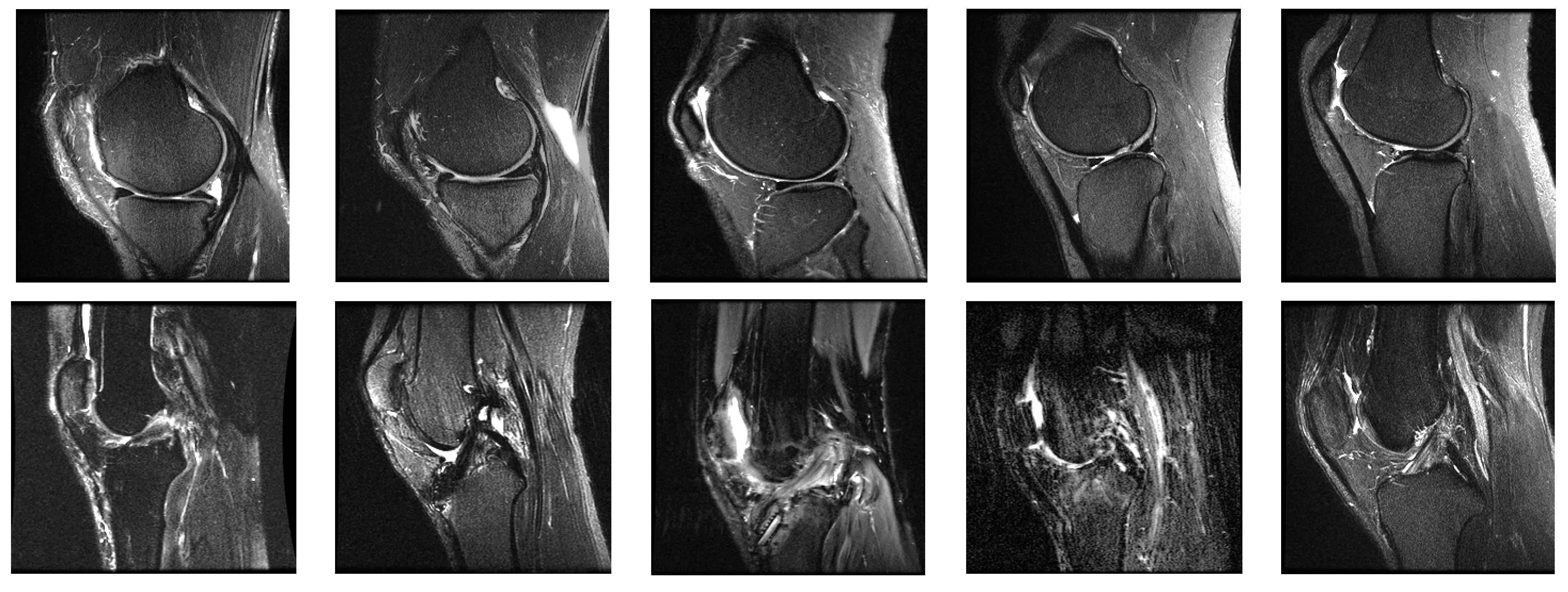
4.1. System Configurations and Dataset
4.2. Performance Metrics
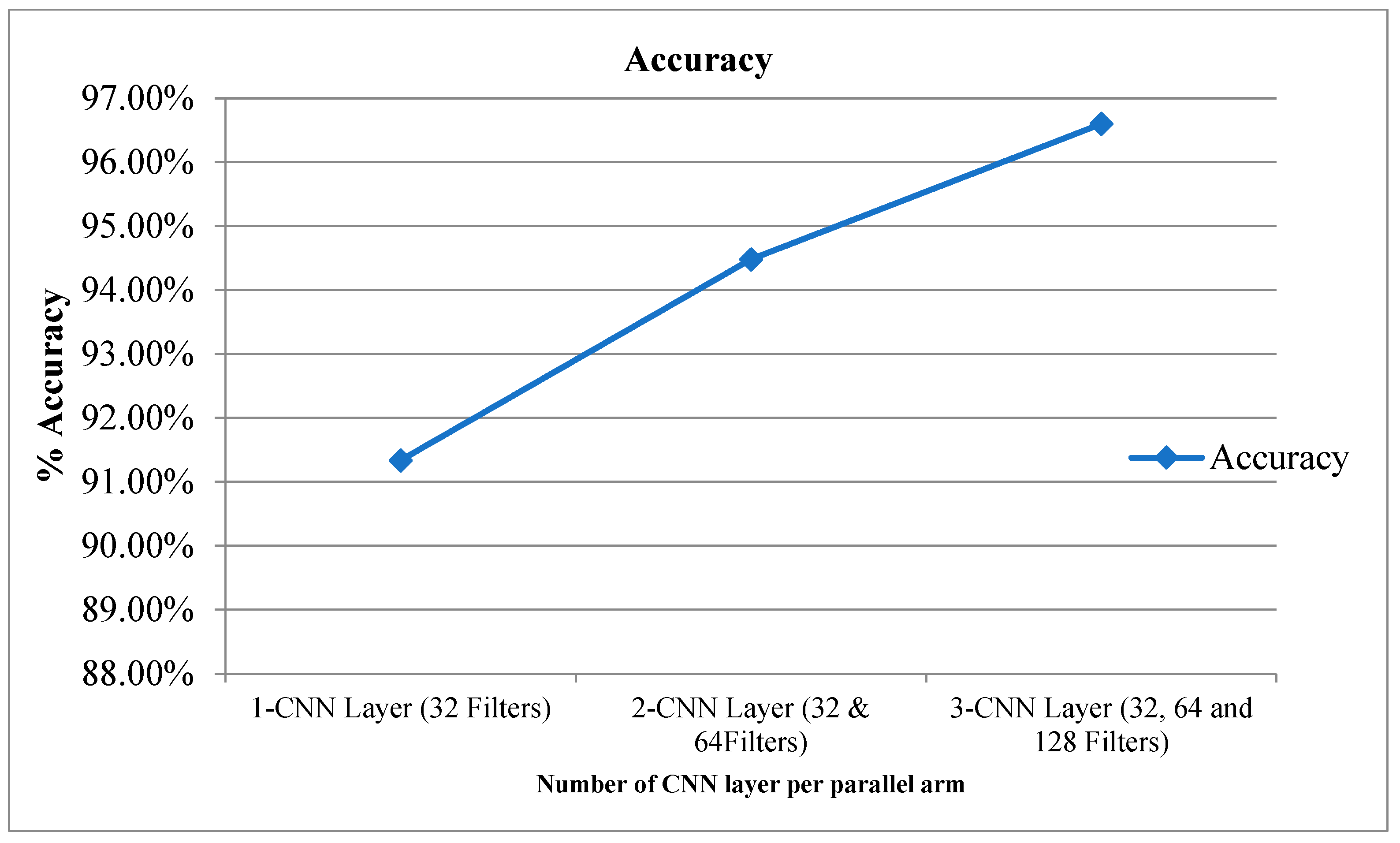
4.3. Network Parameters
5. Discussion
6. Conclusions and Future Scope
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, F.; Jang, H.; Kijowski, R.; Bradshaw, T.; McMillan, A.B. Deep learning MR imaging–based attenuation correction for PET/MR imaging. Radiology 2018, 286, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Liu, J.Z.; Cauley, S.F.; Rosen, B.R.; Rosen, M.S. Image reconstruction by domain-transform manifold learning. Nature 2018, 555, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Berk, N.; Pedoia, V.; Majumdar, S. Use of 2D U-Net convolutional neural networks for automated cartilage and meniscus segmentation of knee MR imaging data to determine relaxometry and morphometry. Radiology 2018, 288, 177–185. [Google Scholar]
- Liu, F.; Zhou, Z.; Jang, H.; Samsonov, A.; Zhao, G.; Kijowski, R. Deep convolutional neural network and 3D deformable approach for tissue segmentation in musculoskeletal magnetic resonance imaging. Magn. Reson. Med. 2018, 79, 2379–2391. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Zhao, G.; Kijowski, R.; Liu, F. Deep convolutional neural network for segmentation of knee joint anatomy. Magn. Reson. Med. 2018, 80, 2759–2770. [Google Scholar] [CrossRef]
- Liu, F.; Zhou, Z.; Samsonov, A.; Blankenbaker, D.; Larison, W.; Kanarek, A.; Lian, K.; Kambhampati, S.; Kijowski, R. Deep learning approach for evaluating knee MR images: Achieving high diagnostic performance for cartilage lesion detection. Radiology 2018, 289, 160–169. [Google Scholar] [CrossRef]
- Joseph, F.D.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat. Med. 2018, 24, 1342–1350. [Google Scholar]
- John, A.; González, F.A.; Ramos-Pollán, R.; Oliveira, J.L.; Lopez, M.A.G. Representation learning for mammography mass lesion classification with convolutional neural networks. Comput. Methods Programs Biomed. 2016, 127, 248–257. [Google Scholar]
- Mark, C.; Bilbily, A.; Colak, E.; Dowdell, T.; Gray, B.; Perampaladas, K.; Barfett, J. Training and validating a deep convolutional neural network for computer-aided detection and classification of abnormalities on frontal chest radiographs. Investig. Radiol. 2017, 52, 281–287. [Google Scholar]
- Marios, A.; Christodoulidis, S.; Ebner, L.; Christe, A.; Mougiakakou, A. Lung pattern classification for interstitial lung diseases using a deep convolutional neural network. IEEE Trans. Med. Imaging 2016, 35, 1207–1216. [Google Scholar]
- Lee, J.K.; Yao, L.; Phelps, C.T.; Wirth, C.R.; Czajka, J.O.H.N.; Lozman, J. Anterior cruciate ligament tears: MR imaging compared with arthroscopy and clinical tests. Radiology 1988, 166, 861–864. [Google Scholar] [CrossRef] [PubMed]
- Partezani, H.P.V.; Helito, C.P.; Rodrigues, M.B. Anterolateral ligament MRI of the knee in ACL injuries: MRI abnormalities association with instability. Eur. Radiol. 2022, 2022, 1–9. [Google Scholar]
- Nicholas, B.; Rajpurkar, P.; Ball, R.L.; Irvin, J.; Park, A.; Jones, E.; Bereket, M.; Patel, B.N.; Yeom, K.W.; Shpanskaya, K.; et al. Deep-learning-assisted diagnosis for knee magnetic resonance imaging: Development and retrospective validation of MRNet. PLoS Med. 2018, 15, e1002699. [Google Scholar]
- Lai, Z.; Deng, H. Medical Image Classification Based on Deep Features Extracted by Deep Model and Statistic Feature Fusion with Multilayer Perceptron. Comput. Intell. Neurosci. 2018, 2018, 2061516. [Google Scholar] [CrossRef]
- Liu, F.; Guan, B.; Zhou, Z.; Samsonov, A.; Rosas, H.; Lian, K.; Sharma, R.; Kanarek, A.; Kim, J.; Guermazi, A.; et al. Fully automated diagnosis of anterior cruciate ligament tears on knee MR images by using deep learning. Radiol. Artif. Intell. 2019, 1, 180091. [Google Scholar] [CrossRef] [PubMed]
- Emre, Ö.; Akdoğan, V.; Korkmaz, M.; Orhan, E.R. Automatic Segmentation of Meniscus in Multispectral MRI Using Regions with Convolutional Neural Network (R-CNN). J. Digit. Imaging 2020, 33, 916–929. [Google Scholar]
- Tsai, C.; Kiryati, N.; Konen, E.; Eshed, I.; Mayer, A. Knee Injury Detection using MRI with Efficiently-Layered Network (ELNet). arXiv 2020, arXiv:2005.02706. [Google Scholar]
- Christoph, G.; Marbach, G.; Civardi, F.; Fucentese, S.F.; Fritz, J.; Sutter, R.; Pfirrmann, C.W.A.; Fritz, B. Deep Convolutional Neural Network–Based Diagnosis of Anterior Cruciate Ligament Tears: Performance Comparison of Homogenous Versus Heterogeneous Knee MRI Cohorts with Different Pulse Sequence Protocols and 1.5-T and 3-T Magnetic Field Strengths. Investig. Radiol. 2020, 55, 499. [Google Scholar]
- Kingma, D.P.; Adam, J.B. A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- MRNet Dataset. Available online: https://stanfordmlgroup.github.io/competitions/mrnet/ (accessed on 5 August 2021).
- Kara, A.C.; Hardalaç, F. Detection and classification of knee injuries from MR images using the MRNet dataset with progressively operating deep learning methods. Mach. Learn. Knowl. Extr. 2021, 3, 1009–1029. [Google Scholar] [CrossRef]
- David, A.; McGuinness, K.; Smeaton, A.F. A comparative study of existing and new deep learning methods for detecting knee injuries using the MRNet dataset. In 2020 International Conference on Intelligent Data Science Technologies and Applications (IDSTA); IEEE: Piscataway, NJ, USA, 2020; pp. 149–155. [Google Scholar]
- Ismail, I.; Anwar, S.M.; Torigian, D.A.; Bagci, U. Deep learning for musculoskeletal image analysis. In 2019 53rd Asilomar Conference on Signals, Systems, and Computers; IEEE: Piscataway, NJ, USA, 2019; pp. 1481–1485. [Google Scholar]
- Awan, M.J.; Rahim, M.S.M.; Salim, N.; Mohammed, M.A.; Garcia-Zapirain, B.; Abdulkareem, K.H. Efficient detection of knee anterior cruciate ligament from magnetic resonance imaging using deep learning approach. Diagnostics 2021, 11, 105. [Google Scholar] [CrossRef] [PubMed]
- Alexia, T.; Lassalle, L.; Zille, P.; Guillin, R.; Pluot, E.; Adam, C.; Charachon, M.; Brat, H.; Wallaert, M.; d’Assignies, G.; et al. Deep learning to detect anterior cruciate ligament tear on knee MRI: Multi-continental external validation. Eur. Radiol. 2022, 2022, 1–10. [Google Scholar]
- Yusuke, M.; Akagi, R.; Maki, S.; Shiko, Y.; Tozawa, R.; Kimura, S.; Yamaguchi, S.; Kawasaki, Y.; Ohtori, S.; Sasho, T. Automated detection of anterior cruciate ligament tears using a deep convolutional neural network. BMC Musculoskelet. Disord. 2022, 23, 1–7. [Google Scholar]
- Vansh, K.; Tyagi, N.; Manocha, B.; Arora, A.; Roy, S.; Nagrath, P. Detection of anterior cruciate ligament tear using deep learning and machine learning techniques. In Data Analytics and Management; Springer: Singapore, 2021; pp. 9–22. [Google Scholar]
- Rizk, B.; Lassalle, L.; Pluot, E.; Guillin, R.; Zille, P.; Tran, A.; D’Assignies, G. Performance Comparison of a Deep Learning Algorithm and Human Readers on Detection of Anterior Cruciate Ligament Tear. In Seminars in Musculoskeletal Radiology; Thieme Medical Publishers, Inc.: New York, NY, USA, 2022; Volume 26, p. A121. [Google Scholar]
- Shaju, J.K.; Joshy, N.A.; Singh, A.R.; Jadhav, R. SmartACL: Anterior Cruciate Ligament Tear Detection by Analyzing MRI Scans. In Innovations in Computational Intelligence and Computer Vision; Springer: Singapore, 2022; pp. 373–381. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Layer | Filter Dimensions | Padding | Stride | Activation Map | Total Trainable Parameters |
|---|---|---|---|---|---|
| Input Image | 256 × 256 × 1 | ||||
| Conv11 | 3 × 3 × 32 | [1,1] | [1,1] | 256 × 256 × 32 | 4640 |
| BN11 | 256 × 256× 32 | 64 | |||
| ReLU11 | 256 × 256 × 32 | ||||
| MaxPool11 | [2,2] | 128 × 128 × 32 | |||
| Conv12 | 3 × 3 × 64 | [1,1] | [1,1] | 128 × 128 × 64 | 18,496 |
| BN12 | 128 × 128 × 64 | 128 | |||
| ReLU12 | 128 × 128 × 64 | ||||
| MaxPool12 | [2,2] | 64 × 64 × 64 | |||
| Conv13 | 3 × 3 × 128 | [1,1] | [1,1] | 64 × 64 × 128 | 73,856 |
| BN13 | 64 × 64 × 128 | 256 | |||
| ReLU13 | 64 × 64 × 128 | ||||
| MaxPool13 | 32 × 32 × 128 | ||||
| Conv21 | 3 × 3 × 32 | [1,1] | [1,1] | 256×256 × 32 | 4640 |
| BN21 | 256 × 256 × 32 | 64 | |||
| ReLU21 | 256 × 256 × 32 | ||||
| MaxPool21 | [2,2] | 128 × 128 × 32 | |||
| Conv22 | 3 × 3 × 64 | [1,1] | [1,1] | 128 × 128 × 64 | 18,496 |
| BN22 | 128 × 128 × 64 | 128 | |||
| ReLU22 | 128 × 128 × 64 | ||||
| MaxPool22 | [2,2] | 64 × 64 × 64 | |||
| Conv23 | 3 × 3 × 128 | [1,1] | [1,1] | 64 × 64 × 128 | 73,856 |
| BN23 | 64 × 64 × 128 | 256 | |||
| ReLU23 | 64 × 64 × 128 | ||||
| MaxPool23 | 32 × 32× 128 | ||||
| Conv31 | 3 × 3 × 32 | [1,1] | [1,1] | 256 × 256 × 32 | 4640 |
| BN31 | 256 × 256 × 32 | 64 | |||
| ReLU31 | 256 × 256 × 32 | ||||
| MaxPool31 | [2,2] | 128 × 128 × 32 | |||
| Conv32 | 3 × 3 × 64 | [1,1] | [1,1] | 128 × 128 × 64 | 18,496 |
| BN32 | 128 × 128 × 64 | 128 | |||
| ReLU32 | 128 × 128 × 64 | ||||
| MaxPool32 | [2,2] | 64 × 64 × 64 | |||
| Conv33 | 3 × 3 × 128 | [1,1] | [1,1] | 64 × 64 × 128 | 73,856 |
| BN33 | 64 × 64 × 128 | 256 | |||
| ReLU33 | 64 × 64 × 128 | ||||
| MaxPool33 | 32 × 32 × 128 | ||||
| FC (2 layers) | 1 × 1 × 2 | 786,434 | |||
| Softmax | 1 × 1 × 2 |
| Layers | Accuracy | Recall | Precision | F1 Score |
|---|---|---|---|---|
| CPDCNN-Adam | 96.60 % | 0.9668 | 0.9554 | 0.9610 |
| CPDCNN-SGDM | 95.88% | 0.9589 | 0.9589 | 0.9589 |
| CPDCNN-RMSProps | 94.48% | 0.9448 | 0.9384 | 0.9415 |
| Author (Year) | Method | % Accuracy | Total Trainable Parameters |
|---|---|---|---|
| Lai et al. (2018) [14] | MLP | 90.15% | |
| Bien et al. (2018) [13] | DCNN | 95.00% | |
| Tsai et al. (2020) [17] | EfficientNet | 91.05% | |
| Kara et al. (2021) [21] | ResNet50 | 81.27% (Sagittal view) | 39,636,608 |
| Azcona et al. (2020) [22] | ResNet18 | 93.40% | ~11 M |
| Irmakci et al. (2019) [23] | ResNet, AlexNet and GoogleNet | AUC = 0.956 (ResNet), 0.938 (AlexNet) and 0.890 (googleNet) | ResNet~11 M |
| Proposed CPDCNN | 96.60 | 786,434 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joshi, K.; Suganthi, K. Anterior Cruciate Ligament Tear Detection Based on Deep Convolutional Neural Network. Diagnostics 2022, 12, 2314. https://doi.org/10.3390/diagnostics12102314
Joshi K, Suganthi K. Anterior Cruciate Ligament Tear Detection Based on Deep Convolutional Neural Network. Diagnostics. 2022; 12(10):2314. https://doi.org/10.3390/diagnostics12102314
Chicago/Turabian StyleJoshi, Kavita, and K. Suganthi. 2022. "Anterior Cruciate Ligament Tear Detection Based on Deep Convolutional Neural Network" Diagnostics 12, no. 10: 2314. https://doi.org/10.3390/diagnostics12102314
APA StyleJoshi, K., & Suganthi, K. (2022). Anterior Cruciate Ligament Tear Detection Based on Deep Convolutional Neural Network. Diagnostics, 12(10), 2314. https://doi.org/10.3390/diagnostics12102314