
Detection of Microorganisms in Body Fluids via MTT-PMS Assay

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Reagents and Protocol Development
2.3. Patient Selection
2.3.1. Intraocular Fluid
2.3.2. Urine Sample
2.4. Statistical Analysis
3. Results
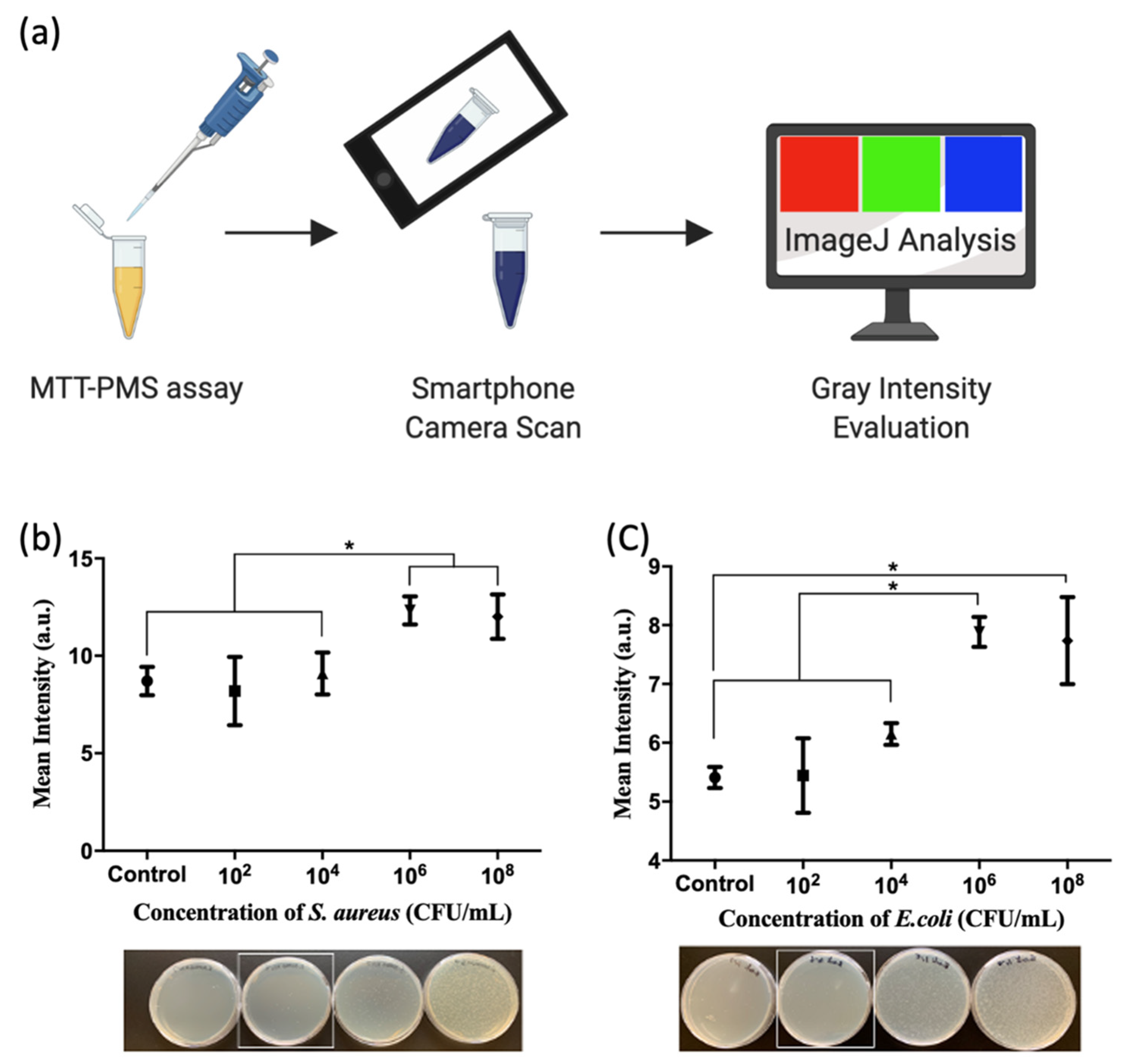
3.1. Development of MTT-PMS Bacterial Detection Assay
3.2. Clinical Evaluation of MTT-PMS Assay for Living Microorganism Detection
3.2.1. MTT-PMS Assay of Human Intraocular Fluid
3.2.2. MTT-PMS Assay of Human Urine Samples
4. Discussion
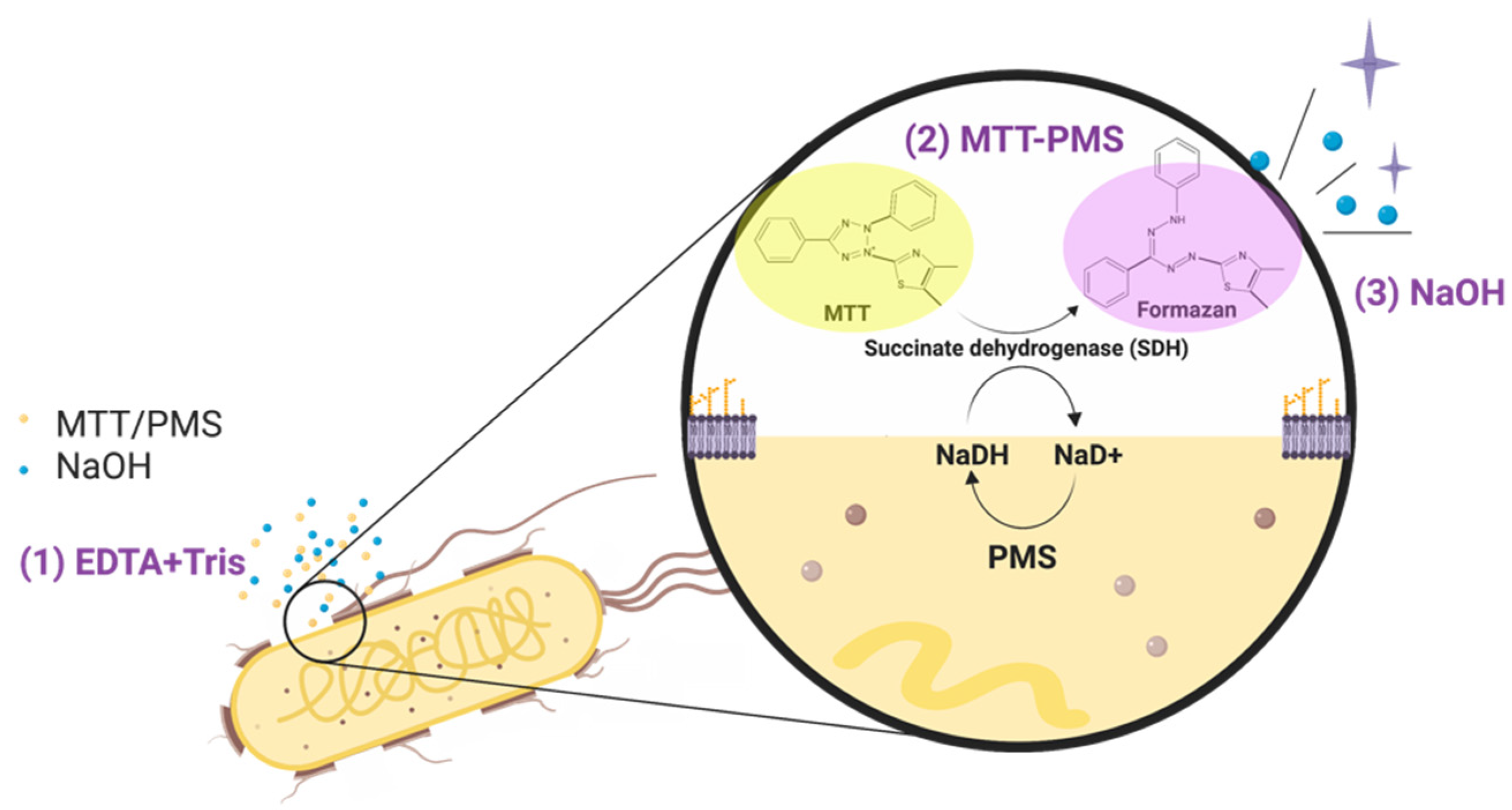
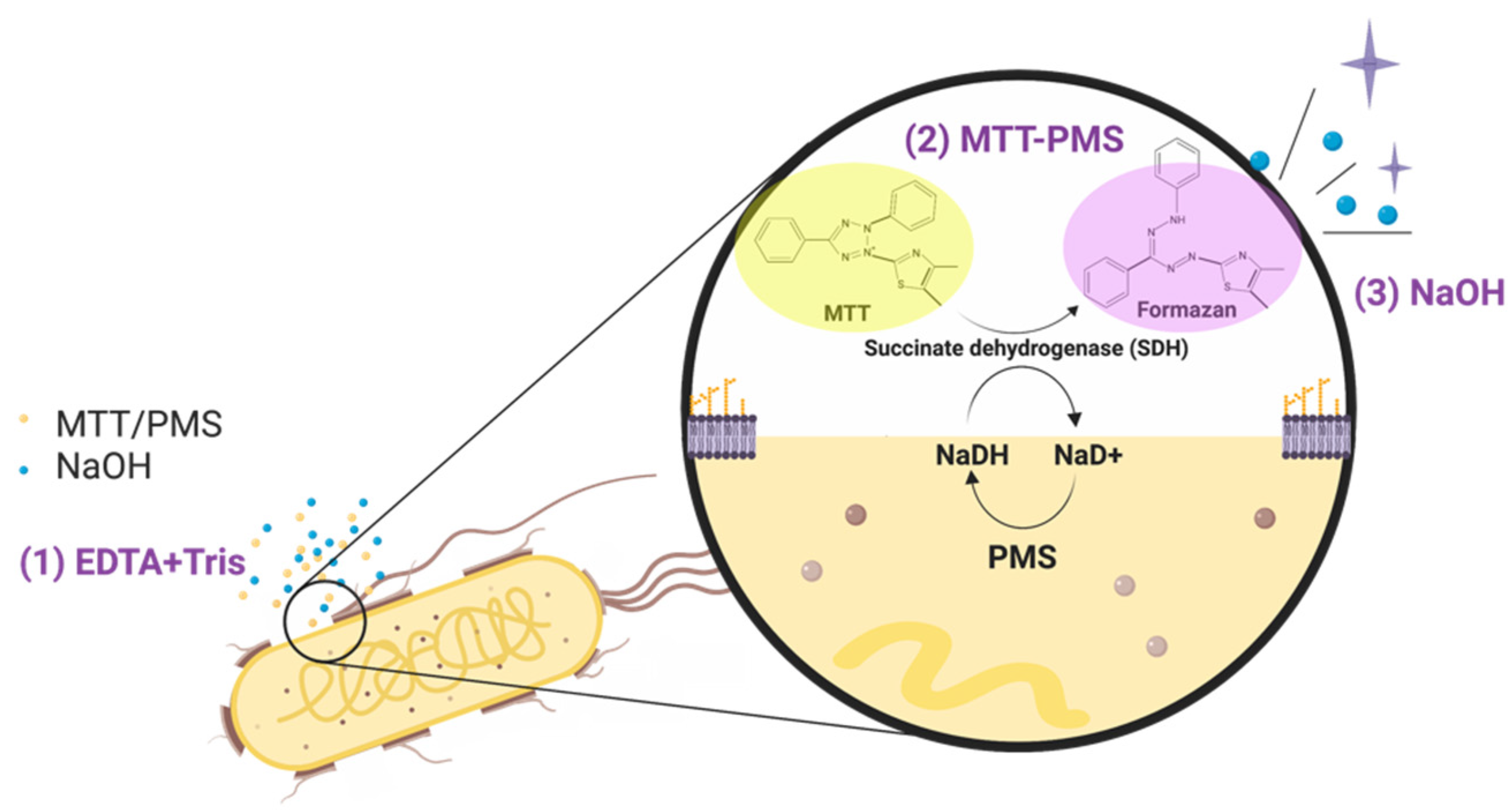
- It could be used as a “rule-out” test for infectious diseases screening. A negative MTT-PMS assay result may indicate a low possibility of “live” microorganism presence [26,64]. Using screening methods before conventional microorganism culture may reduce the potential risk of stratification of febrile patients and guide initial treatment [23].
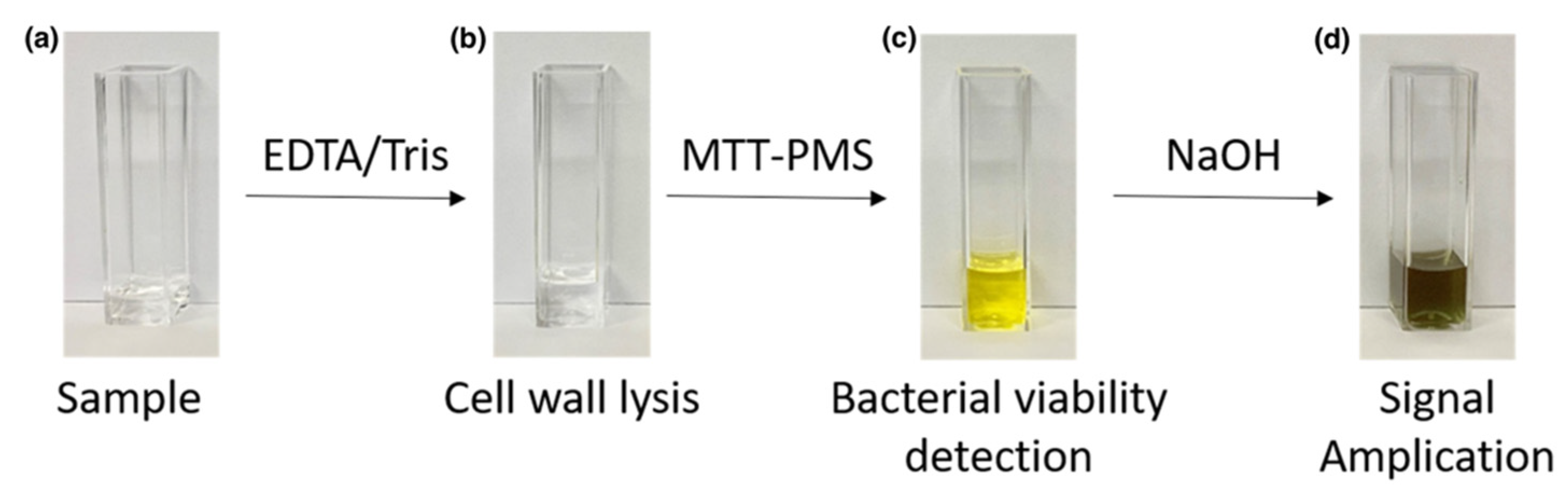
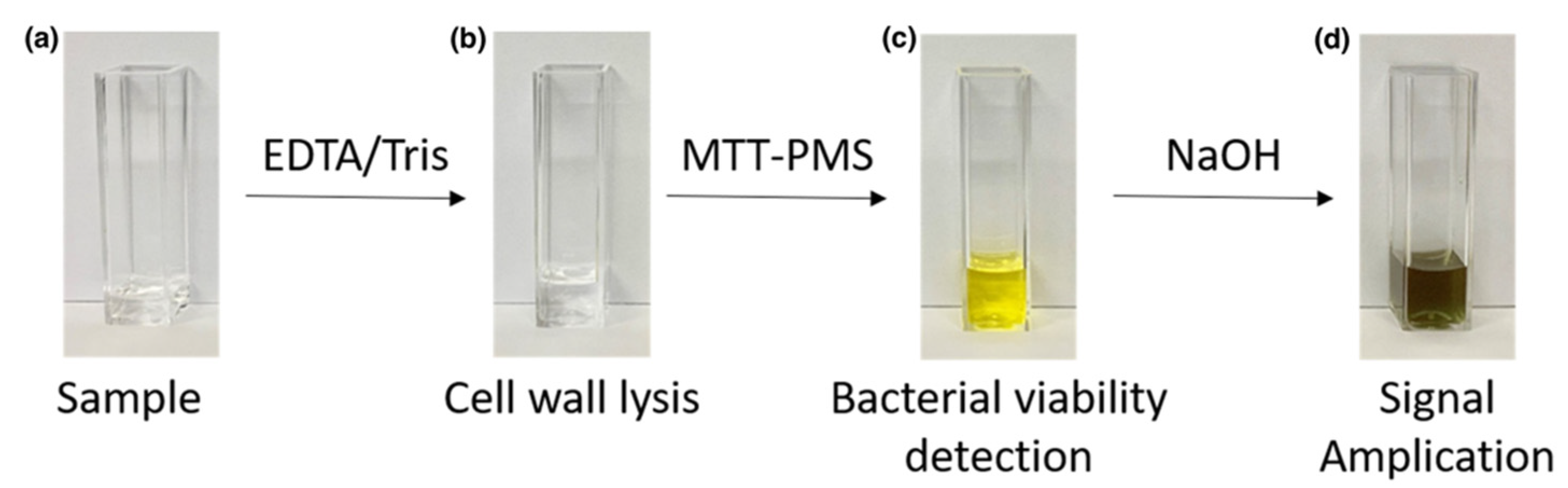
- Rapid results. By adding reagents to improve bacterial wall penetration, facilitating the provision of an additional electron acceptor, and enhancing the resulting signal, this MTT-PMS assay has been optimized to quickly detect the presence of microorganisms and provide real-time semi-quantitative screening of infectious diseases within 15 min.
- Semi-quantitative readout. This process provides rapid and semi-quantitative information regarding the presence of microorganisms without sophisticated equipment or trained technicians.
- Potential POCT device. This MTT-PMS assay may be integrated into a paper-based device and colorimetric analysis can be performed using a smartphone color-recognition application [16,60,61,62,63]. Moreover, the MTT-PMS assay can further be embedded into a disposable paper-based device and evaluated with a smartphone or an open-source application (Image J). These features indicate the MTT-PMS assay has the potential to be commercialized.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [Green Version]
- Mitsakakis, K.; D’Acremont, V.; Hin, S.; von Stetten, F.; Zengerle, R. Diagnostic tools for tackling febrile illness and enhancing patient management. Microelectron. Eng. 2018, 201, 26–59. [Google Scholar] [CrossRef]
- El Bcheraoui, C.; Mokdad, A.H.; Dwyer-Lindgren, L.; Bertozzi-Villa, A.; Stubbs, R.W.; Morozoff, C.; Shirude, S.; Naghavi, M.; Murray, C.J.L. Trends and Patterns of Differences in Infectious Disease Mortality Among US Counties, 1980-2014. JAMA J. Am. Med. Assoc. 2018, 319, 1248–1260. [Google Scholar] [CrossRef]
- Vila, J.; Gómez, M.D.; Salavert, M.; Bosch, J. Métodos de diagnóstico rápido en microbiología clínica: Necesidades clínicas. Enferm. Infecc. Microbiol. Clín. 2017, 35, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Reali, S.; Najib, E.Y.; Balázs, K.E.T.; Tan, A.C.H.; Váradi, L.; Hibbs, D.E.; Groundwater, P.W. Novel diagnostics for point-of-care bacterial detection and identification. RSC Adv. 2019, 9, 21486–21497. [Google Scholar] [CrossRef] [Green Version]
- Craig, J.; Williams, G.J.; Jones, M.; Codarini, M.; Macaskill, P.; Hayen, A.; Irwig, L.; Fitzgerald, D.A.; Isaacs, D.; McCaskill, M. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: Prospective cohort study of 15 781 febrile illnesses. BMJ 2010, 340, c1594. [Google Scholar] [CrossRef] [Green Version]
- Buck, C.; Bundschu, J.; Bartmann, P.; Pohlandt, F.; Gallati, H. Interleukin-6: A Sensitive Parameter for the Early Diagnosis of Neonatal Bacterial Infection. Pediatrics 1994, 93, 54–58. [Google Scholar] [CrossRef]
- Virkki, R.; Juven, T.; Rikalainen, H.; Svedström, E.; Mertsola, J.; Ruuskanen, O. Differentiation of bacterial and viral pneumonia in children. Thorax 2002, 57, 438–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Multani, A.; Allard, L.S.; Wangjam, T.; Sica, R.A.; Epstein, D.J.; Rezvani, A.R.; Ho, R.Y. Missed diagnosis and misdiagnosis of infectious diseases in hematopoietic cell transplant recipients: An autopsy study. Blood Adv. 2019, 3, 3602–3612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reddy, B.; Hassan, U.; Seymour, C.; Angus, D.C.; Isbell, T.S.; White, K.; Weir, W.; Yeh, L.; Vincent, A.; Bashir, R. Point-of-care sensors for the management of sepsis. Nat. Biomed. Eng. 2018, 2, 640–648. [Google Scholar] [CrossRef]
- Puttaswamy, S.; Lee, B.D.; Sengupta, S. Novel Electrical Method for Early Detection of Viable Bacteria in Blood Cultures. J. Clin. Microbiol. 2011, 49, 2286–2289. [Google Scholar] [CrossRef] [Green Version]
- Lagier, J.-C.; Edouard, S.; Pagnier, I.; Mediannikov, O.; Drancourt, M.; Raoult, D. Current and Past Strategies for Bacterial Culture in Clinical Microbiology. Clin. Microbiol. Rev. 2015, 28, 208–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, C.-I.; Kim, J.; Park, D.W.; Kim, B.-N.; Ha, U.-S.; Lee, S.-J.; Yeo, J.; Min, S.K.; Lee, H.; Wie, S.-H. Clinical Practice Guidelines for the Antibiotic Treatment of Community-Acquired Urinary Tract Infections. Infect. Chemother. 2018, 50, 67–100. [Google Scholar] [CrossRef]
- Pfister, H.W.; Brouwer, M.C.; Esposito, S.; Dzupova, O.; Van De Beek, D.; Leib, S.; Pagliano, P.; Cabellos, C.; Sipahi, O.R.; Mourvillier, B.; et al. ESCMID guideline: Diagnosis and treatment of acute bacterial meningitis. Clin. Microbiol. Infect. 2016, 22, S37–S62. [Google Scholar] [CrossRef]
- Sanders, E.R. Aseptic Laboratory Techniques: Plating Methods. J. Vis. Exp. 2012, 63, e3064. [Google Scholar] [CrossRef]
- Liao, Y.-H.; Muthuramalingam, K.; Tung, K.-H.; Chuan, H.-H.; Liang, K.-Y.; Hsu, C.-P.; Cheng, C.-M. Portable Device for Quick Detection of Viable Bacteria in Water. Micromachines 2020, 11, 1079. [Google Scholar] [CrossRef] [PubMed]
- Carbonnelle, E.; Mesquita, C.; Bille, E.; Day, N.; Dauphin, B.; Beretti, J.-L.; Ferroni, A.; Gutmann, L.; Nassif, X. MALDI-TOF mass spectrometry tools for bacterial identification in clinical microbiology laboratory. Clin. Biochem. 2011, 44, 104–109. [Google Scholar] [CrossRef]
- Järvinen, A.-K.; Laakso, S.; Piiparinen, P.; Aittakorpi, A.; Lindfors, M.; Huopaniemi, L.; Piiparinen, H.; Mäki, M. Rapid identification of bacterial pathogens using a PCR- and microarray-based assay. BMC Microbiol. 2009, 9, 161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, S.; Kariya, M.; Nagano, K.; Yokoyama, S.-I.; Fukao, T.; Yamazaki, Y.; Mori, H. New Rapid Enzyme-Linked Immunosorbent Assay to Detect Antibodies against Bacterial Surface Antigens Using Filtration Plates. Biol. Pharm. Bull. 2002, 25, 986–990. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.; Lifson, M.A.; Inci, F.; Liang, L.-G.; Sheng, Y.-F.; Demirci, U. Advances in addressing technical challenges of point-of-care diagnostics in resource-limited settings. Expert Rev. Mol. Diagn. 2016, 16, 449–459. [Google Scholar] [CrossRef]
- Santibañez, S.; Bellis, K.S.; Bay, A.; Chung, C.L.; Bradley, K.; Gibson, D.; Shultz, A. Strengthening Rural States’ Capacity to Prepare for and Respond to Emerging Infectious Diseases, 2013–2015. South. Med. J. 2019, 112, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Sokhna, C.; Mediannikov, O.; Fenollar, F.; Bassene, H.; Diatta, G.; Tall, A.; Trape, J.-F.; Drancourt, M.; Raoult, D. Point-of-Care Laboratory of Pathogen Diagnosis in Rural Senegal. PLoS Neglected Trop. Dis. 2013, 7, e1999. [Google Scholar] [CrossRef] [PubMed]
- Oeschger, T.; McCloskey, D.; Kopparthy, V.; Singh, A.; Erickson, D. Point of care technologies for sepsis diagnosis and treatment. Lab Chip 2019, 19, 728–737. [Google Scholar] [CrossRef]
- Drain, P.; Hyle, E.P.; Noubary, F.; Freedberg, K.A.; Wilson, D.; Bishai, W.R.; Rodriguez, W.; Bassett, I.V. Diagnostic point-of-care tests in resource-limited settings. Lancet Infect. Dis. 2014, 14, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Vashist, S.K. Point-of-Care Diagnostics: Recent Advances and Trends. Biosensors 2017, 7, 62. [Google Scholar] [CrossRef] [Green Version]
- Grela, E.; Kozłowska, J.; Grabowiecka, A. Current methodology of MTT assay in bacteria—A review. Acta Histochem. 2018, 120, 303–311. [Google Scholar] [CrossRef]
- Braissant, O.; Astasov-Frauenhoffer, M.; Waltimo, T.; Bonkat, G. A Review of Methods to Determine Viability, Vitality, and Metabolic Rates in Microbiology. Front. Microbiol. 2020, 11, 547458. [Google Scholar] [CrossRef]
- Muelas-Serrano, S.; Nogal-Ruiz, J.J.; Gómez-Barrio, A. Setting of a colorimetric method to determine the viability of Trypanosoma cruzi epimastigotes. Parasitol. Res. 2000, 86, 999–1002. [Google Scholar] [CrossRef]
- Cedillo-Rivera, R.; Ramírez, A.; Muñoz, O. A rapid colorimetric assay with the tetrazolium salt MTT and phenazine methosulfate (PMS) for viability of Entamoeba histolytica. Arch. Med. Res. 1992, 23, 59–61. [Google Scholar]
- Silverthorn, D.U.; Ober, W.C.; Garrison, C.W.; Silverthorn, A.C.; Johnson, B.R. Human Physiology: An Integrated Approach; Benjamin-Cummings, Pearson: San Francisco, CA, USA, 2010. [Google Scholar]
- Rasband, W.S. ImageJ; Version 1.53d; U.S. National Institutes of Health: Bethesda, MD, USA, 1997–2021. Available online: https://imagej.nih.gov/ij/ (accessed on 25 March 2021).
- Denizot, F.; Lang, R. Rapid colorimetric assay for cell growth and survival. Modifications to the tetrazolium dye procedure giving improved sensitivity and reliability. J. Immunol. Methods 1986, 89, 271–277. [Google Scholar] [CrossRef]
- Tsukatani, T.; Suenaga, H.; Higuchi, T.; Akao, T.; Ishiyama, M.; Ezoe, K.; Matsumoto, K. Colorimetric cell proliferation assay for microorganisms in microtiter plate using water-soluble tetrazolium salts. J. Microbiol. Methods 2008, 75, 109–116. [Google Scholar] [CrossRef]
- Finnegan, S.; Percival, S. EDTA: An Antimicrobial and Antibiofilm Agent for Use in Wound Care. Adv. Wound Care 2015, 4, 415–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, K.J.; Rice, C.V. Revised model of calcium and magnesium binding to the bacterial cell wall. BioMetals 2014, 27, 1361–1370. [Google Scholar] [CrossRef] [Green Version]
- Leive, L. The barrier function of the gram-negative envelope. Ann. N. Y. Acad. Sci. 1974, 235, 109–129. [Google Scholar] [CrossRef] [PubMed]
- Schnaitman, C.A. Protein Composition of the Cell Wall and Cytoplasmic Membrane of Escherichia coli. J. Bacteriol. 1970, 104, 890–901. [Google Scholar] [CrossRef] [Green Version]
- Kuan, C.-M.; York, R.L.; Cheng, C.-M. Lignocellulose-based analytical devices: Bamboo as an analytical platform for chemical detection. Sci. Rep. 2016, 5, 18570. [Google Scholar] [CrossRef] [Green Version]
- Estrela, C.; Estrela, C.; Barbin, E.L.; Spanó, J.C.E.; Marchesan, M.; Pecora, J.D. Mechanism of action of sodium hypochlorite. Braz. Dent. J. 2002, 13, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wang, F.; Tao, X.; Cheng, H. Ammonia-containing dimethyl sulfoxide: An improved solvent for the dissolution of formazan crystals in the 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) assay. Anal. Biochem. 2012, 421, 324–326. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.R.; Mazzulli, T.; Hazen, K.C.; Good, C.E.; Abdelhamed, A.M.; Lo, P.; Shum, B.; Roman, K.P.; Robinson, D.C. Multicenter clinical evaluation of BacT/Alert Virtuo blood culture system. J. Clin. Microbiol. 2017, 55, 2413–2421. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.C.; Lee, S.; Kim, S.; Cho, O.-H.; Park, H.; Yu, S.-M. Comparison of Clinical Performance Between BacT/Alert Virtuo and BacT/Alert 3D Blood Culture Systems. Ann. Lab. Med. 2019, 39, 278–283. [Google Scholar] [CrossRef] [Green Version]
- Silverthorn, D.U. Human Physiology: An Integrated Approach; E-Book; Pearson Higher: San Francisco, CA, USA, 2018. [Google Scholar]
- Medina, M.; Castillo-Pino, E. An introduction to the epidemiology and burden of urinary tract infections. Ther. Adv. Urol. 2019, 11, 1756287219832172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, C.; Parker, A.; Jefferson, B.; Cartmell, E. The Characterization of Feces and Urine: A Review of the Literature to Inform Advanced Treatment Technology. Crit. Rev. Environ. Sci. Technol. 2015, 45, 1827–1879. [Google Scholar] [CrossRef] [Green Version]
- Novosad, B.D.; Callegan, M.C. Severe bacterial endophthalmitis: Towards improving clinical outcomes. Expert Rev. Ophthalmol. 2010, 5, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Al-Omran, A.M.; Abboud, E.B.; Abu El-Asrar, A.M. Microbiologic spectrum and visual outcome of posttraumatic endophthalmitis. Retina 2007, 27, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Jackson, T.; Eykyn, S.J.; Graham, E.M.; Stanford, M.R. Endogenous bacterial endophthalmitis: A 17-year prospective series and review of 267 reported cases. Surv. Ophthalmol. 2003, 48, 403–423. [Google Scholar] [CrossRef]
- Durand, M.L.; Miller, J.W.; Young, L.H. Endophthalmitis; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Deshmukh, D.; Joseph, J.; Chakrabarti, M.; Sharma, S.; Jayasudha, R.; Sama, K.C.; Sontam, B.; Tyagi, M.; Narayanan, R.; Shivaji, S. New insights into culture negative endophthalmitis by unbiased next generation sequencing. Sci. Rep. 2019, 9, 844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malekzadeh, D.; Osmon, D.R.; Lahr, B.D.; Hanssen, A.D.; Berbari, E.F. Prior Use of Antimicrobial Therapy is a Risk Factor for Culture-negative Prosthetic Joint Infection. Clin. Orthop. Relat. Res. 2010, 468, 2039–2045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mambatta, A.K.; Rashme, V.L.; Menon, S.; Jayarajan, J.; Harini, S.; Kuppusamy, J. Reliability of dipstick assay in predicting urinary tract infection. J. Fam. Med. Prim. Care 2015, 4, 265–268. [Google Scholar] [CrossRef]
- Stepanenko, A.; Dmitrenko, V. Pitfalls of the MTT assay: Direct and off-target effects of inhibitors can result in over/underestimation of cell viability. Gene 2015, 574, 193–203. [Google Scholar] [CrossRef]
- Postnikova, G.B.; Shekhovtsova, E.A. Hemoglobin and myoglobin as reducing agents in biological systems. Redox reactions of globins with copper and iron salts and complexes. Biochemistry (Moscow) 2016, 81, 1735–1753. [Google Scholar] [CrossRef]
- Ono, J.; Yoshimura, H. Prevention of hemoglobin interference on the formazan reaction. Clin. Chim. Acta 2008, 390, 115–121. [Google Scholar] [CrossRef]
- Nguyen, T.; Chidambara, V.A.; Andreasen, S.Z.; Golabi, M.; Huynh, V.N.; Linh, Q.T.; Bang, D.D.; Wolff, A. Point-of-care devices for pathogen detections: The three most important factors to realise towards commercialization. TrAC Trends Anal. Chem. 2020, 131, 116004. [Google Scholar] [CrossRef]
- Kralik, P.; Slana, I.; Kralova, A.; Babak, V.; Whitlock, R.H.; Pavlik, I. Development of a predictive model for detection of Mycobacterium avium subsp. paratuberculosis in faeces by quantitative real time PCR. Vet. Microbiol. 2011, 149, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Kralik, P.; Ricchi, M. A Basic Guide to Real Time PCR in Microbial Diagnostics: Definitions, Parameters, and Everything. Front. Microbiol. 2017, 8, 108. [Google Scholar] [CrossRef] [Green Version]
- Kong, D.; Liu, L.; Xing, C.; Kuang, H.; Xu, C. Sensitive and highly specific detection of Cronobacter sakazakii based on monoclonal sandwich ELISA. Food Agric. Immunol. 2015, 26, 566–576. [Google Scholar] [CrossRef] [Green Version]
- Matsuura, K.; Wang, W.-H.; Ching, A.; Chen, Y.; Cheng, C.-M. Paper-Based Resazurin Assay of Inhibitor-Treated Porcine Sperm. Micromachines 2019, 10, 495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuura, K.; Huang, H.-W.; Chen, M.-C.; Chen, Y.; Cheng, C.-M. Relationship between Porcine Sperm Motility and Sperm Enzymatic Activity using Paper-based Devices. Sci. Rep. 2017, 7, srep46213. [Google Scholar] [CrossRef]
- Lin, S.-C.; Hsu, M.-Y.; Kuan, C.-M.; Wang, H.-K.; Chang, C.-L.; Tseng, F.-G.; Cheng, C.-M. Cotton-based Diagnostic Devices. Sci. Rep. 2015, 4, 6976. [Google Scholar] [CrossRef] [Green Version]
- Tsao, Y.; Yang, C.; Wen, Y.; Chang, T.; Matsuura, K.; Chen, Y.; Cheng, C. Point-of-care semen analysis of patients with infertility via smartphone and colorimetric paper-based diagnostic device. Bioeng. Transl. Med. 2021, 6, 10176. [Google Scholar] [CrossRef]
- Wang, H.; Cheng, H.; Wang, F.; Wei, D.; Wang, X. An improved 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide (MTT) reduction assay for evaluating the viability of Escherichia coli cells. J. Microbiol. Methods 2010, 82, 330–333. [Google Scholar] [CrossRef]
- Benov, L. Effect of growth media on the MTT colorimetric assay in bacteria. PLoS ONE 2019, 14, e0219713. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age | Sex | Eye Site | Disease Diagnosis | Underlying Disease | Sample Type | Culture Result | MTT-PMS Assay Results | |
|---|---|---|---|---|---|---|---|---|---|
| Group 1 | 1 | 62 | F | OD * | Endophthalmitis (exogenous) | Right breast cancer | Aqueous | G(+) ‡ cocci 1+ ‡‡ | 104–106 |
| 2 | 62 | F | OD | Endophthalmitis (exogenous) | Right breast cancer | Vitreous | G(+) ‡ cocci 1+ | 106–108 | |
| 3 | 62 | F | OD | Endophthalmitis (exogenous) | Right breast cancer | Aqueous | N/A | 106–108 | |
| 4 | 47 | F | OD | Endophthalmitis (endogenous) | Sepsis, Right breast cancer | Aqueous | Aqueous: no anaerobic pathogen. † | 106–108 | |
| 5 | 73 | F | OS * | Endophthalmitis (exogenous) | Diabetes mellitus, Hypertension | Vitreous | Candida parapsilosis complex 1+ | >108 | |
| Group 2 ** | 1 | 68 | M | OS | Endophthalmitis (exogenous) | Hypertension, ESRD with HD | Vitreous | No growth | 0 |
| Comparison of Urine Culture Report >105 CFU/mL, n = 116 | ||||
| Urine Culture >105 CFU/mL (n) | ||||
| Positive | Negative | Total | ||
| MTT-PMS assay 105 (n) | Positive | 20 | 47 | 67 |
| Negative | 10 | 39 | 49 | |
| Total | 30 | 86 | 116 | |
| Sensitivity | Specificity | Accuracy | PPV * | NPV ** |
| 66.67% | 45.35% | 50.86% | 29.85% | 79.59% |
| Comparison of Urine Culture Report >105 CFU/mL, n = 59, OB– † | ||||
| Urine Culture >105 CFU/mL (n) | ||||
| Positive | Negative | Total | ||
| MTT-PMS assay105 (n) | Positive | 9 | 28 | 37 |
| Negative | 0 | 22 | 22 | |
| Total | 9 | 50 | 59 | |
| Sensitivity | Specificity | Accuracy | PPV * | NPV ** |
| 100.00% | 44.00% | 52.54% | 24.32% | 100.00% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Tsao, Y.-T.; Yeh, P.-T.; Liao, Y.-H.; Lee, Y.-T.; Liao, W.-T.; Wang, Y.-C.; Shen, C.-F.; Cheng, C.-M. Detection of Microorganisms in Body Fluids via MTT-PMS Assay. Diagnostics 2022, 12, 46. https://doi.org/10.3390/diagnostics12010046
Chen C-H, Tsao Y-T, Yeh P-T, Liao Y-H, Lee Y-T, Liao W-T, Wang Y-C, Shen C-F, Cheng C-M. Detection of Microorganisms in Body Fluids via MTT-PMS Assay. Diagnostics. 2022; 12(1):46. https://doi.org/10.3390/diagnostics12010046
Chicago/Turabian StyleChen, Cheng-Han, Yu-Ting Tsao, Po-Ting Yeh, Yu-Hsiang Liao, Yi-Tzu Lee, Wan-Ting Liao, Yung-Chih Wang, Ching-Fen Shen, and Chao-Min Cheng. 2022. "Detection of Microorganisms in Body Fluids via MTT-PMS Assay" Diagnostics 12, no. 1: 46. https://doi.org/10.3390/diagnostics12010046
APA StyleChen, C.-H., Tsao, Y.-T., Yeh, P.-T., Liao, Y.-H., Lee, Y.-T., Liao, W.-T., Wang, Y.-C., Shen, C.-F., & Cheng, C.-M. (2022). Detection of Microorganisms in Body Fluids via MTT-PMS Assay. Diagnostics, 12(1), 46. https://doi.org/10.3390/diagnostics12010046