
Evaluation of Clinical and Immunohistochemical Factors Relating to Melanoma Metastasis: Potential Roles of Nestin and Fascin in Melanoma


Abstract
:1. Introduction
2. Materials and Methods
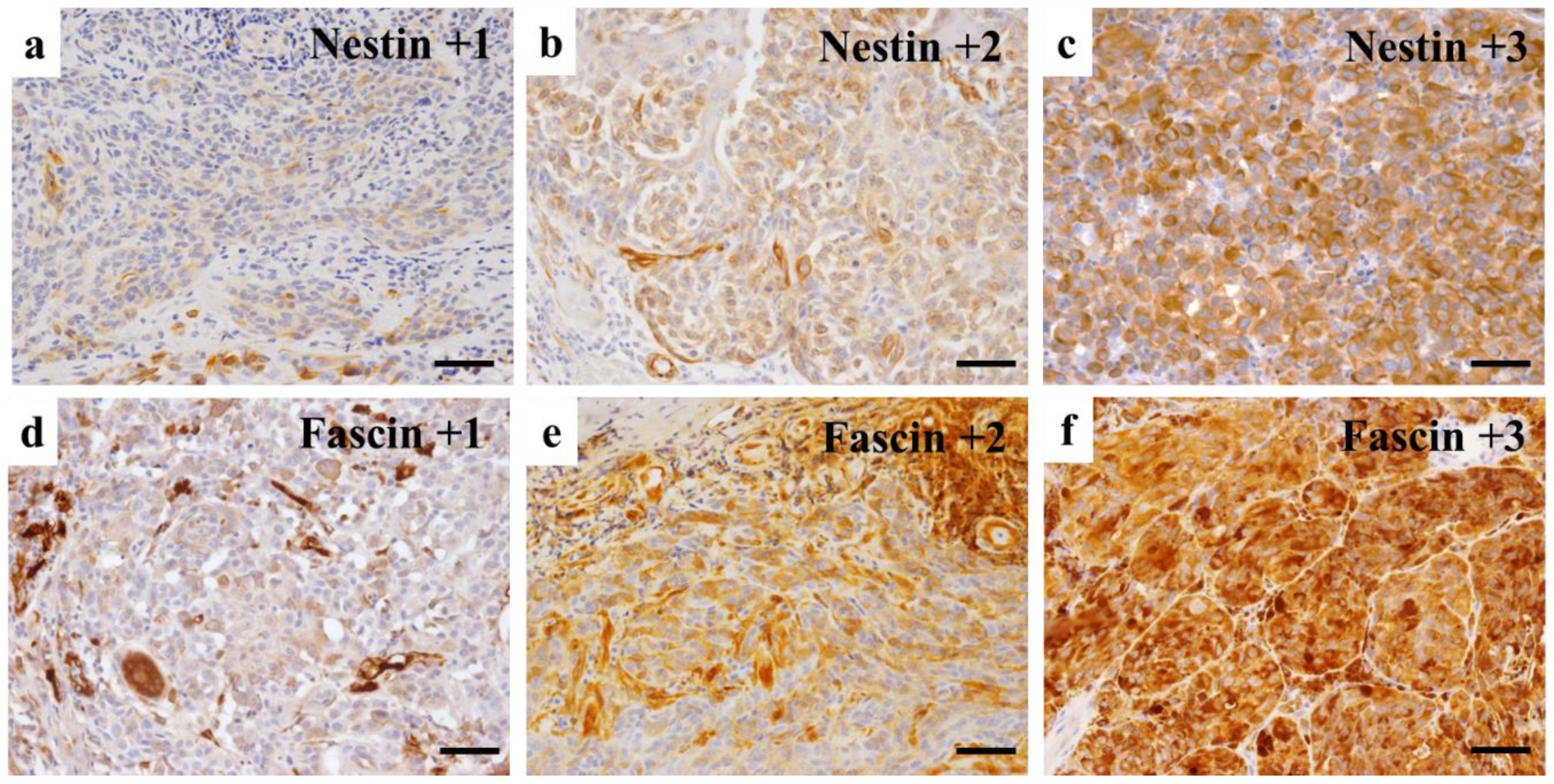
3. Immunohistochemical Evaluation
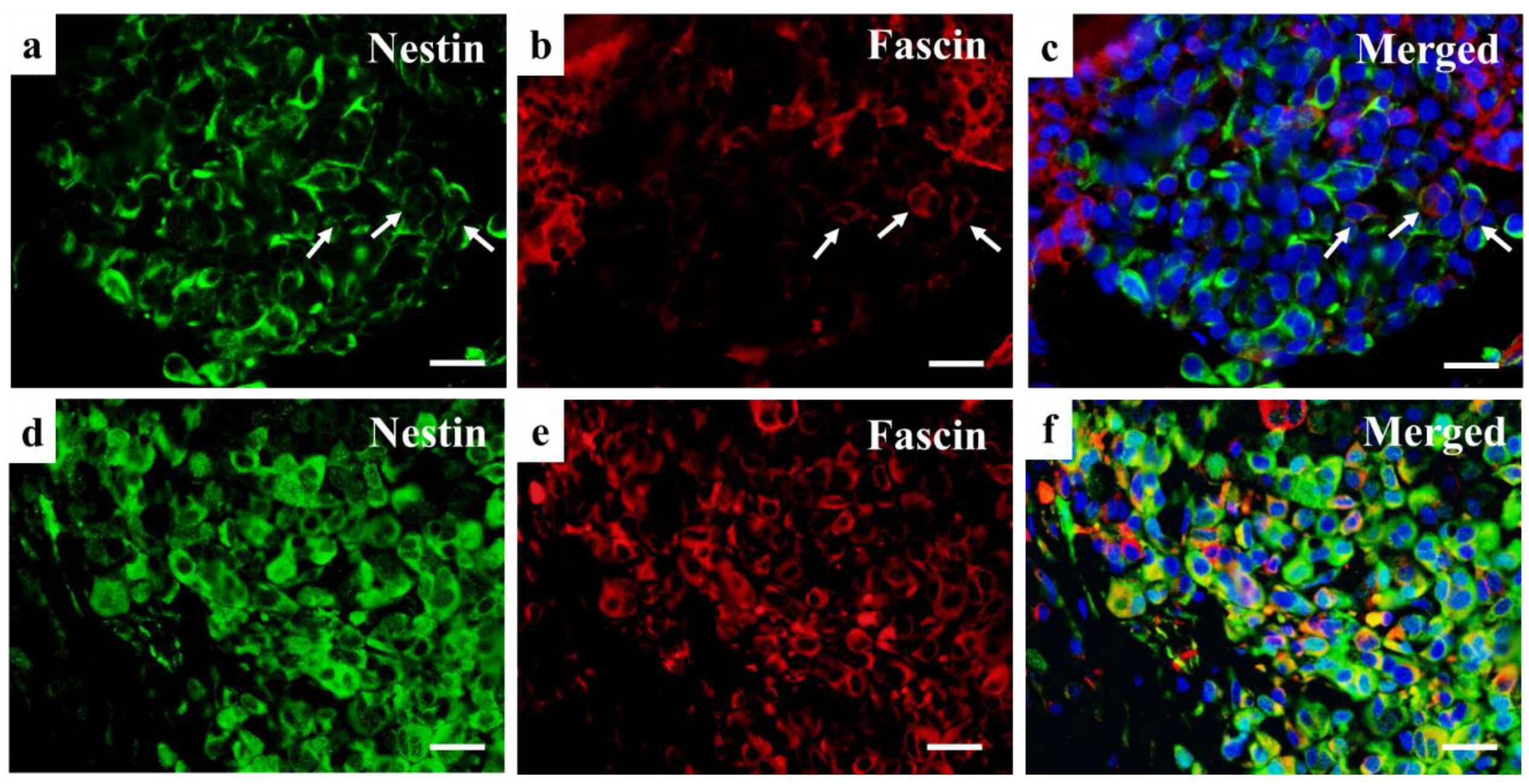
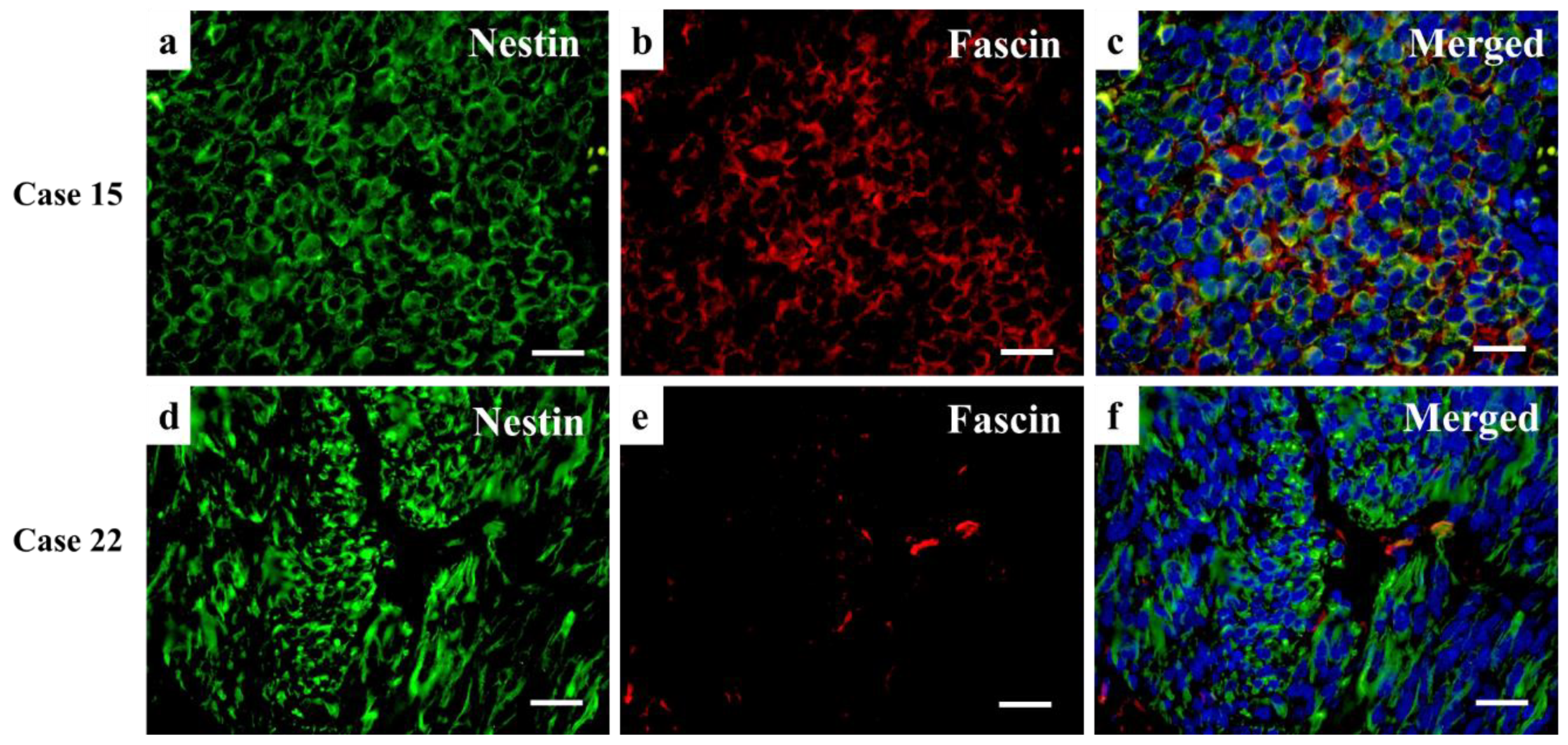
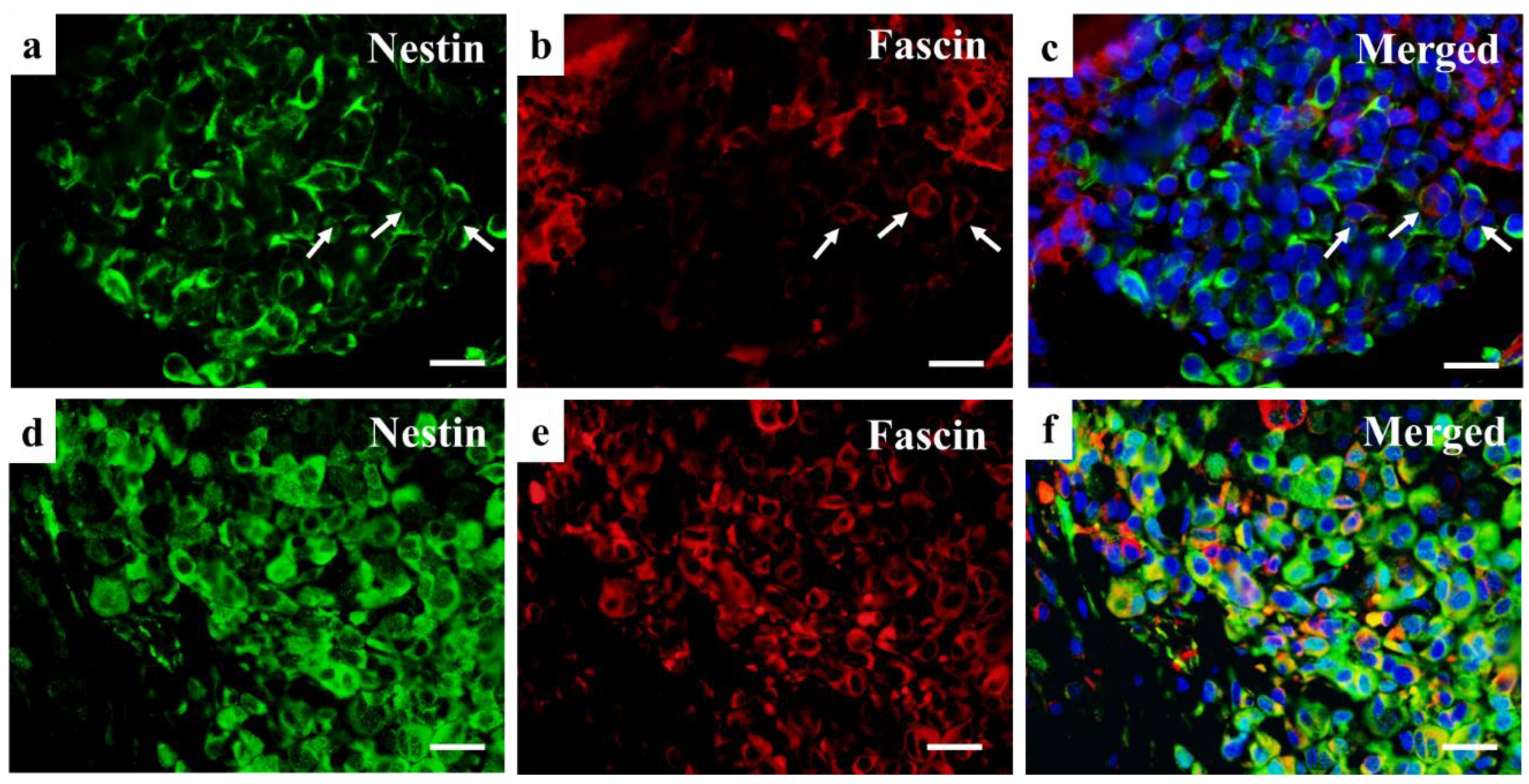
4. Double Immunofluorescence
5. Statistical Analysis
6. Results
7. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Namikawa, K.; Yamazaki, N. Targeted therapy and immunotherapy for melanoma in Japan. Curr. Treat. Options Oncol. 2019, 20, 7. [Google Scholar] [CrossRef] [Green Version]
- Elder, D.E.; Bastian, B.C.; Cree, I.A.; Massi, D.; Scolyer, R.A. The 2018 World health organization classification of cutaneous, mucosal, and uveal melanoma: Detailed analysis of 9 distinct subtypes defined by their evolutionary pathway. Arch. Pathol. Lab. Med. 2020, 144, 500–522. [Google Scholar] [CrossRef] [Green Version]
- Elder, D.E.; Barnhill, R.L.; Bastian, B.C. Melanocytic tumour classification and the pathway concept of melanoma pathogenesis. In WHO Classification of Skin Tumors, 4th ed.; Elder, D.E., Massi, D., Scolyer, R.A., Willemze, R., Eds.; World Health Organization Classification of Tumours; JARC: Lyon, France, 2018; Volume 11, pp. 66–71. [Google Scholar]
- Keung, E.Z.; Gershenwald, J.E. The eighth edition American joint committee on cancer (AJCC) melanoma staging system: Implications for melanoma treatment and care. Expert Rev. Anticancer Ther. 2018, 18, 775–784. [Google Scholar] [CrossRef]
- Available online: https://ganjoho.jp/public/cancer/melanoma/print.html (accessed on 20 December 2021).
- Rastrelli, M.; Tropea, S.; Rossi, C.R.; Alaibac, M. Melanoma: Epidemiology, risk factors, pathogenesis, diagnosis and classification. In Vivo 2014, 28, 1005–1011. [Google Scholar]
- Yildiz, L.; Kefeli, M.; Aydin, O.; Kandemir, B. Fascin expression in melanocytic lesions of the skin. Eur. J. Dermatol. EJD 2009, 19, 445–450. [Google Scholar] [CrossRef]
- Yamada, N.; Mori, T.; Murakami, M.; Noguchi, S.; Sakai, H.; Akao, Y.; Maruo, K. Fascin-1 expression in canine cutaneous and oral melanocytic tumors. Vet. Comp. Oncol. 2012, 10, 303–311. [Google Scholar] [CrossRef]
- Kang, J.; Wang, J.; Yao, Z.; Hu, Y.; Ma, S.; Fan, Q.; Gao, F.; Sun, Y.; Sun, J. Fascin induces melanoma tumorigenesis and stemness through regulating the Hippo pathway. Cell Commun. Signal. CCS 2018, 16, 37. [Google Scholar] [CrossRef] [Green Version]
- Goncharuk, V.N.; Ross, J.S.; Carlson, J.A. Actin-binding protein fascin expression in skin neoplasia. J. Cutan. Pathol. 2002, 29, 430–438. [Google Scholar] [CrossRef]
- Ma, Y.; Faller, W.J.; Sansom, O.J.; Brown, E.R.; Doig, T.N.; Melton, D.W.; Machesky, L.M. Fascin expression is increased in metastatic lesions but does not correlate with progression nor outcome in melanoma. Melanoma Res. 2015, 25, 169–172. [Google Scholar] [CrossRef]
- Kuk, S.K.; Won, C.H.; Lee, W.J.; Shin, W.J.; Yoon, H.J.; Hong, S.D.; Hong, S.P.; Lee, J. Prognostic significance of nestin in primary malignant melanoma of the oral cavity. Melanoma Res. 2016, 26, 457–463. [Google Scholar] [CrossRef]
- Akiyama, M.; Matsuda, Y.; Ishiwata, T.; Naito, Z.; Kawana, S. Inhibition of the stem cell marker nestin reduces tumor growth and invasion of malignant melanoma. J. Investig. Dermatol. 2013, 133, 1384–1387. [Google Scholar] [CrossRef] [Green Version]
- Gomes, C.B.F.; Zechin, K.G.; Xu, S.; Stelini, R.F.; Nishimoto, I.N.; Zhan, Q.; Xu, T.; Qin, G.; Treister, N.S.; Murphy, G.F.; et al. TET2 negatively regulates nestin expression in human melanoma. Am. J. Pathol. 2016, 186, 1427–1434. [Google Scholar] [CrossRef] [Green Version]
- Allred, D.C.; Harvey, J.M.; Berardo, M.; Clark, G.M. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod. Pathol. 1998, 11, 155–168. [Google Scholar]
- Kawai, R.; Sugita, Y.; Suzumura, T.; Hattori, T.; Yoshida, W.; Kubo, K.; Maeda, H. Melanoma inhibitory activity and melanoma inhibitory activity 2 as novel immunohistochemical markers of oral epithelial dysplasia. J. Clin. Med. 2021, 10, 3661. [Google Scholar] [CrossRef]
- Kim, M.Y.; Jung, A.R.; Kim, G.E.; Yang, J.; Ha, U.-S.; Hong, S.-H.; Choi, Y.J.; Moon, M.H.; Kim, S.W.; Lee, J.Y.; et al. High FOXM1 expression is a prognostic marker for poor clinical outcomes in prostate cancer. J. Cancer 2019, 10, 749–756. [Google Scholar] [CrossRef]
- Matsuda, Y.; Naito, Z.; Kawahara, K.; Nakazawa, N.; Korc, M.; Ishiwata, T. Nestin is a novel target for suppressing pancreatic cancer cell migration, invasion and metastasis. Cancer Biol. Ther. 2011, 11, 512–523. [Google Scholar] [CrossRef] [Green Version]
- Bernal, A.; Arranz, L. Nestin-expressing progenitor cells: Function, identity and therapeutic implications. Cell. Mol. Life Sci. CMLS 2018, 75, 2177–2195. [Google Scholar] [CrossRef] [Green Version]
- Lendahl, U.; Zimmerman, L.B.; McKay, R.D. CNS stem cells express a new class of intermediate filament protein. Cell 1990, 60, 585–595. [Google Scholar] [CrossRef]
- Neradil, J.; Veselska, R. Nestin as a marker of cancer stem cells. Cancer Sci. 2015, 106, 803–811. [Google Scholar] [CrossRef]
- Kleeberger, W.; Bova, G.S.; Nielsen, M.E.; Herawi, M.; Chuang, A.-Y.; Epstein, J.I.; Berman, D.M. Roles for the stem cell associated intermediate filament Nestin in prostate cancer migration and metastasis. Cancer Res. 2007, 67, 9199–9206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, Y.; Hayashi, Y.; Sakaki, H.; Murakami, I. Fascin-1 is associated with recurrence in solitary fibrous tumor/hemangiopericytoma. Mol. Clin. Oncol. 2021, 15, 199. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, Y.; Osanai, M.; Lee, G.-H. Fascin-1 expression correlates with repression of E-cadherin expression in hepatocellular carcinoma cells and augments their invasiveness in combination with matrix metalloproteinases. Cancer Sci. 2011, 102, 1228–1235. [Google Scholar] [CrossRef]
- Wang, C.-Q.; Tang, C.H.; Chang, H.T.; Li, X.N.; Zhao, Y.M.; Su, C.M.; Hu, G.-N.; Zhang, T.; Sun, X.-X.; Zng, Y.; et al. Fascin-1 as a novel diagnostic marker of triple-negative breast cancer. Cancer Med. 2016, 5, 1983–1988. [Google Scholar] [CrossRef] [PubMed]
- Arlt, M.J.; Kuzmanov, A.; Snedeker, J.G.; Fuchs, B.; Silvan, U.; Sabile, A.A. Fascin-1 enhances experimental osteosarcoma tumor formation and metastasis and is related to poor patient outcome. BMC Cancer 2019, 19, 83. [Google Scholar] [CrossRef]
- Richmond, A.M.; Blake, E.A.; Torkko, K.; Smith, E.E.; Spillman, M.A.; Post, M.D. Fascin is associated with aggressive behavior and poor outcome in uterine carcinosarcoma. Int. J. Gynecol. Cancer 2017, 27, 1895–1903. [Google Scholar] [CrossRef] [PubMed]
- Toi, M.; Hayashi, Y.; Murakami, I. Hepatic stellate cells derived from the nestin-positive cells in septum transversum during rat liver development. Med. Mol. Morphol. 2018, 51, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://training.seer.cancer.gov/melanoma/intro/survival.html (accessed on 20 December 2021).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age | Sex | Primary Tumor Area | Metastasis | Duration till Metastasis | Remained Tumor Cells | Treatment | Fascin | Nestin | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Proportion | Intensity | Allred Score | Proportion | Intensity | Allred Score | ||||||||
| 1 | 30–39 | F | acral cutaneous | - | - | - | C | 2 | 1 | 3 | 2 | 1 | 3 |
| 2 | F | mucosal | - | - | + | C | 2 | 1 | 3 | 3 | 1 | 4 | |
| 3 | 40–49 | M | acral cutaneous | - | - | RX | C | 0 | 0 | 0 | 4 | 3 | 7 |
| 4 | F | non-acral cutaneous | - | - | - | C | 1 | 1 | 2 | 5 | 3 | 8 | |
| 5 | 60–69 | M | mucosal | - | - | - | - | 5 | 3 | 8 | 4 | 3 | 7 |
| 6 | M | non-acral cutaneous | - | - | - | C | 1 | 2 | 3 | 4 | 2 | 6 | |
| 7 | F | non-acral cutaneous | + | 16 | - | C | 5 | 3 | 8 | 5 | 3 | 8 | |
| 8 | F | acral cutaneous | - | - | - | - | 2 | 1 | 3 | 2 | 3 | 5 | |
| 9 | F | mucosal | - | - | RX | C | 4 | 2 | 6 | 4 | 2 | 6 | |
| 10 | M | non-acral cutaneous | - | - | - | C | 4 | 1 | 5 | 1 | 1 | 2 | |
| 11 | F | mucosal | + | 49 | + | C, R | 5 | 3 | 8 | 5 | 3 | 8 | |
| 12 | F | non-acral cutaneous | - | - | - | C | 2 | 1 | 3 | 3 | 2 | 5 | |
| 13 | F | acral cutaneous | + | 3 | - | - | 5 | 3 | 8 | 5 | 3 | 8 | |
| 14 | 70–79 | F | mucosal | + | 12 | + | R | 5 | 3 | 8 | 5 | 3 | 8 |
| 15 | F | mucosal | + | 5 | RX | R | 5 | 3 | 8 | 5 | 3 | 8 | |
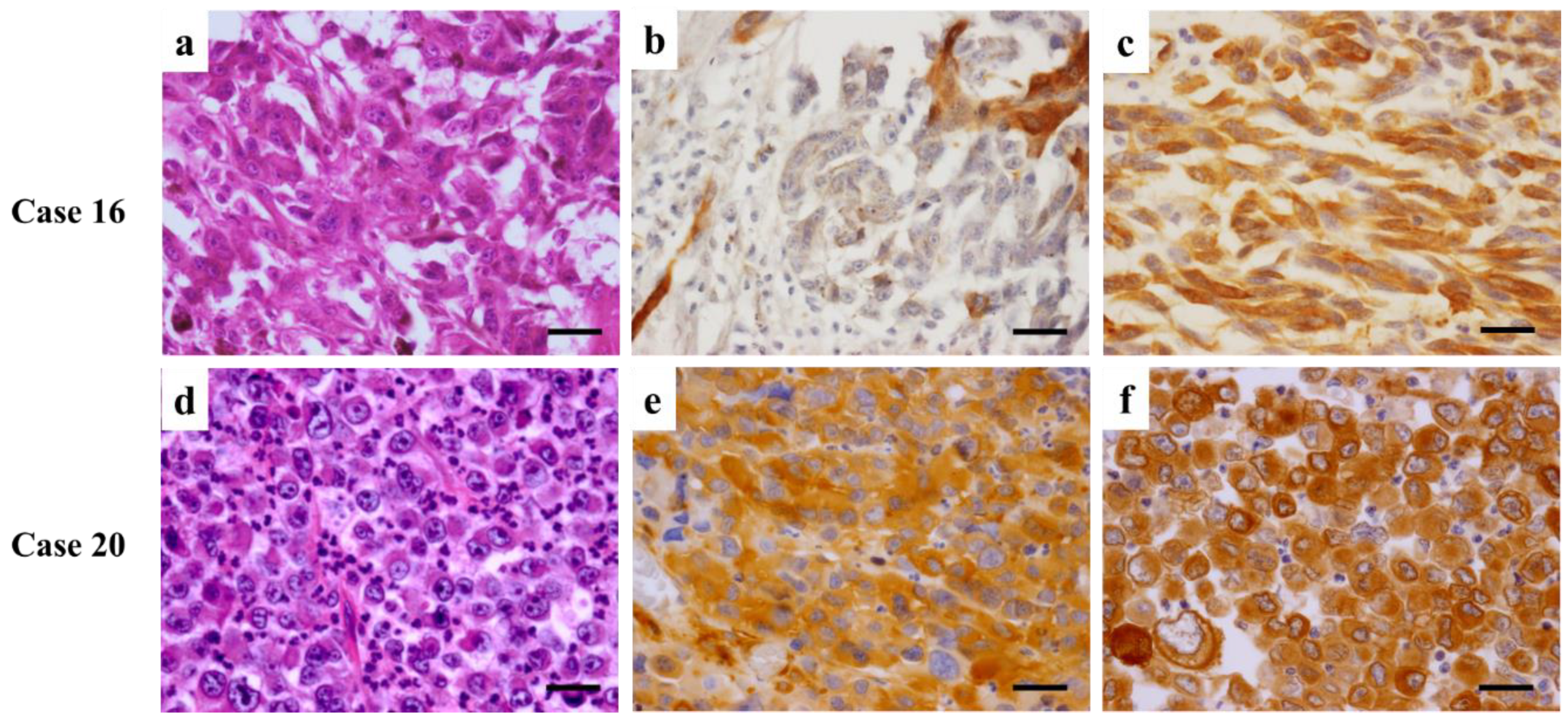
| 16 | F | acral cutaneous | + | 40 | - | - | 1 | 1 | 2 | 5 | 3 | 8 | |
| 17 | M | non-acral cutaneous | + | 6 | - | C | 5 | 2 | 7 | 5 | 3 | 8 | |
| 18 | F | mucosal | + | 1 | + | C, R | 5 | 3 | 8 | 5 | 3 | 8 | |
| 19 | M | acral cutaneous | - | - | - | C | 1 | 1 | 2 | 2 | 2 | 4 | |
| 20 | M | acral cutaneous | + | 1 | - | - * | 5 | 2 | 7 | 5 | 3 | 8 | |
| 21 | F | non-acral cutaneous | + | 9 | - | - * | 5 | 3 | 8 | 5 | 3 | 8 | |
| 22 | M | non-acral cutaneous | + | 20 | RX | - | 0 | 0 | 0 | 5 | 3 | 8 | |
| 23 | 80–89 | F | mucosal | + | 41 | + | C, R | 5 | 3 | 8 | 5 | 3 | 8 |
| 24 | M | non-acral cutaneous | - | - | RX | C | 2 | 1 | 3 | 2 | 2 | 4 | |
| 25 | M | non-acral cutaneous | + | 6 | + | C | 1 | 2 | 3 | 5 | 3 | 8 | |
| 26 | F | acral cutaneous | - | - | - | - | 5 | 2 | 7 | 3 | 3 | 6 | |
| 27 | F | acral cutaneous | + | 11 | RX | C | 5 | 1 | 6 | 5 | 3 | 8 | |
| 28 | M | acral cutaneous | + | 11 | - | - | 1 | 3 | 4 | 5 | 3 | 8 | |
| 29 | F | acral cutaneous | + | 16 | - | - | 5 | 2 | 7 | 5 | 3 | 8 | |
| 30 | 90– | M | acral cutaneous | - | - | - | - | 2 | 2 | 4 | 2 | 1 | 3 |
| Antibody | Source | Dilution |
|---|---|---|
| Anti-nestin mouse monoclonal antibody | Santa Cruz Biotechnology (Santa Cruz, CA, USA) | 1:100 |
| Anti-fascin mouse monoclonal antibody | Dako (Carpinteria, CA, USA) | 1:50 |
| Biotinylated rabbit anti-mouse IgG antibody | Dako (Glostrup, Denmark) | 1:200 |
| FITC-labeled streptavidin | Dako (Carpinteria, CA, USA) | 1:200 |
| Texas Red-labeled anti-mouse IgG antibody | Molecular Probes (Eugene, OR, USA) | 1:200 |
| N-Histofine Simple Stain MAX PO (MULTI) | Nichirei Biosciences Inc., (Tokyo, Japan) | ready to use |
| Chemical Agent | Source | |
| 4′,6-diamidino-2-phenylindole: DAPI | Sigma (Aldrich, St. Louis, MO, USA) | |
| 3,3′-Diaminobenzidine, tetrahydrochloride: DAB | Sigma (Aldrich, St. Louis, MO, USA) | |
| p Value | Cutt-Off Point | |
|---|---|---|
| Sex | ns | |
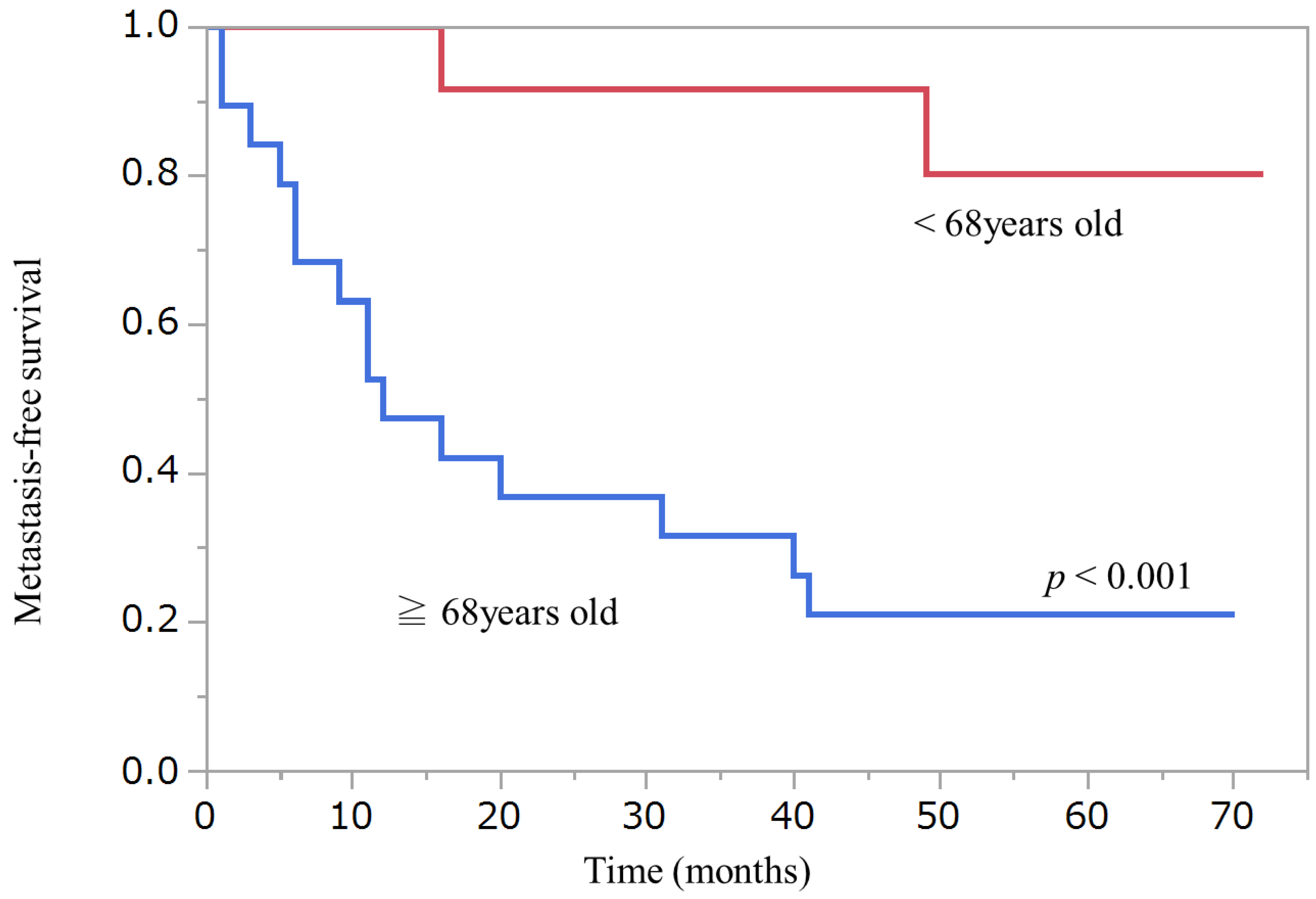
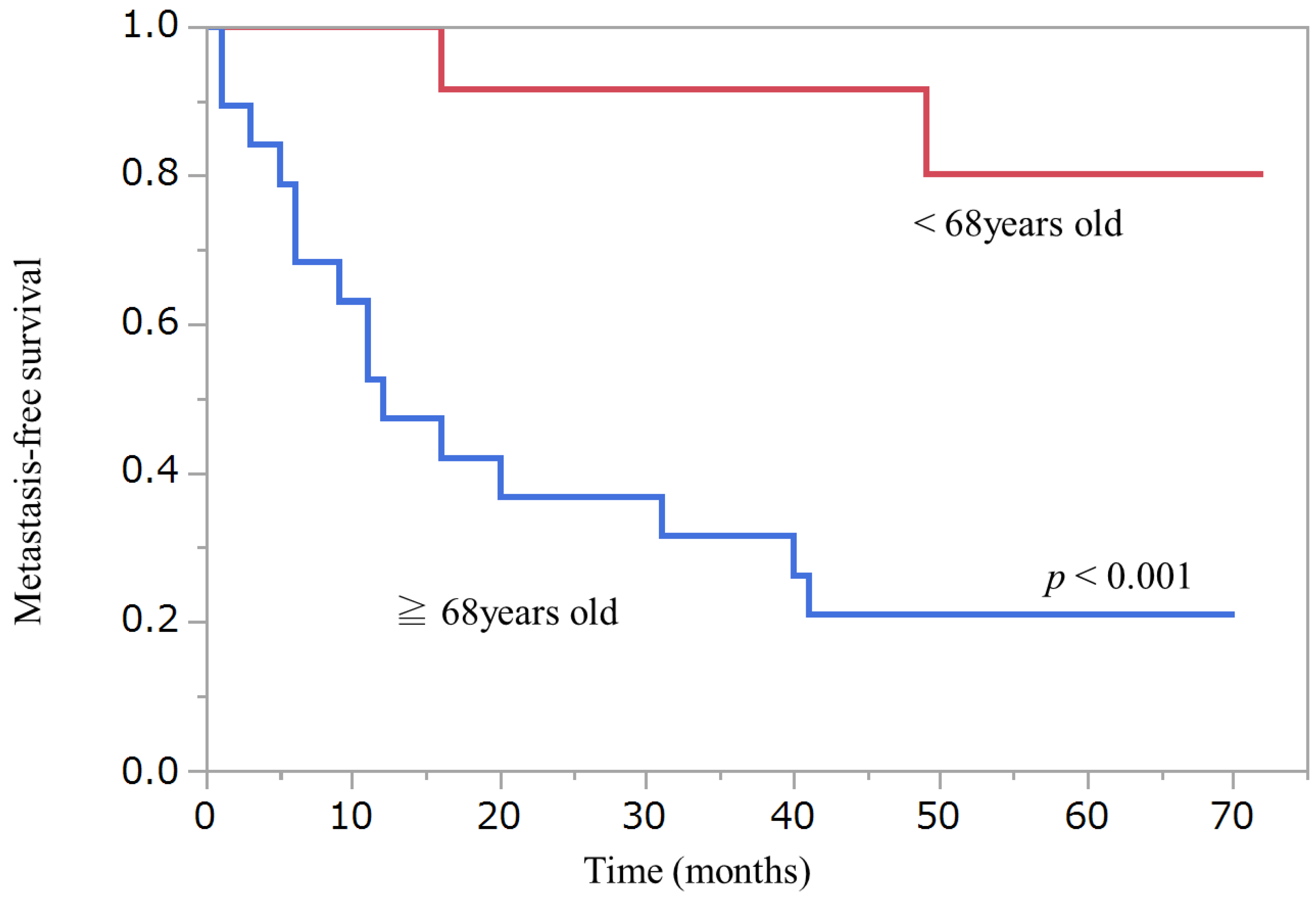
| Onset age | p < 0.001 | 68 years old |
| Primary tumor area | ns | |
| Remained cancer cells at the margin | ns | |
| Treatment | ns | |
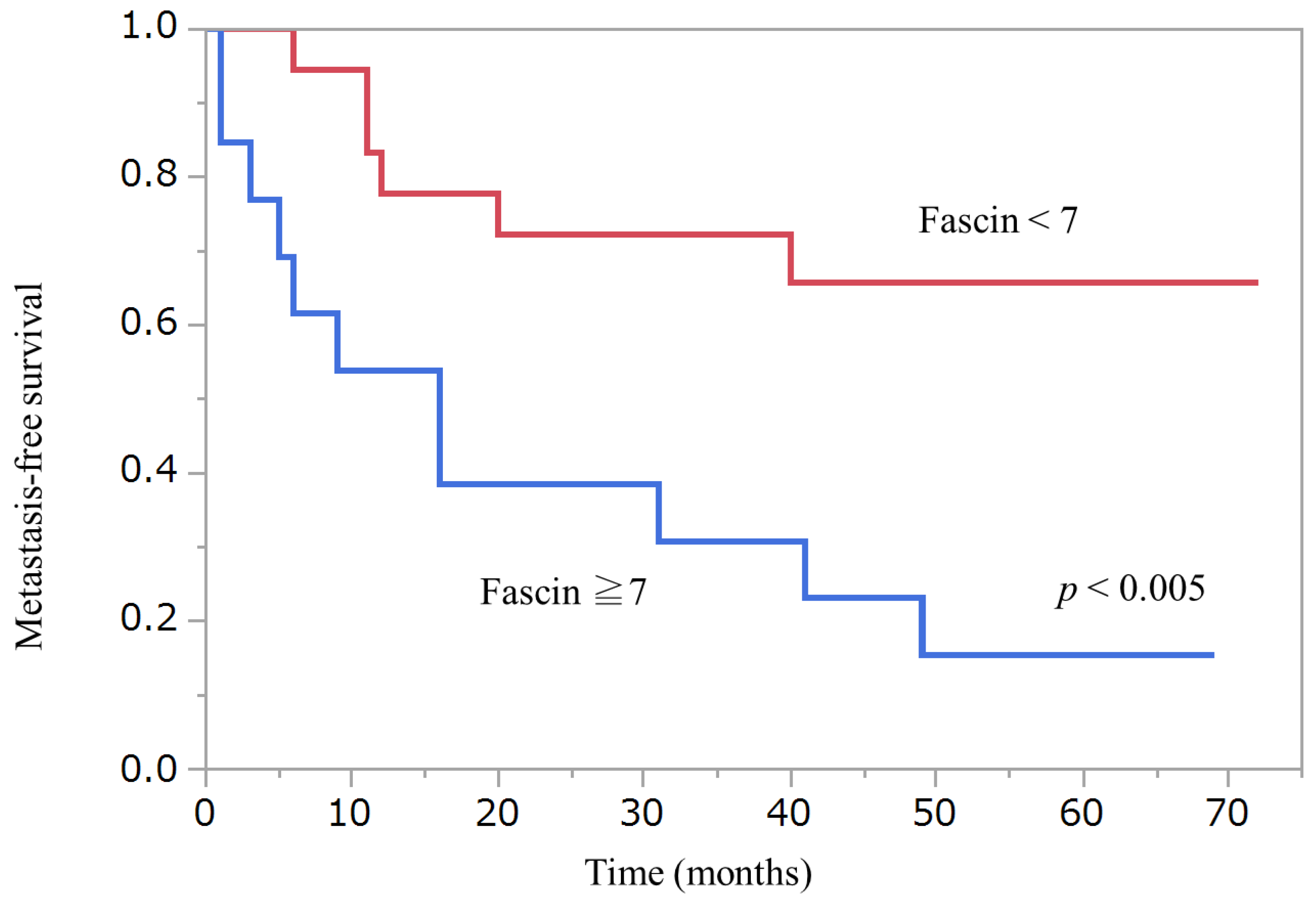
| Fascin at the primary lesion | p < 0.005 | 7 (Allred Score) |
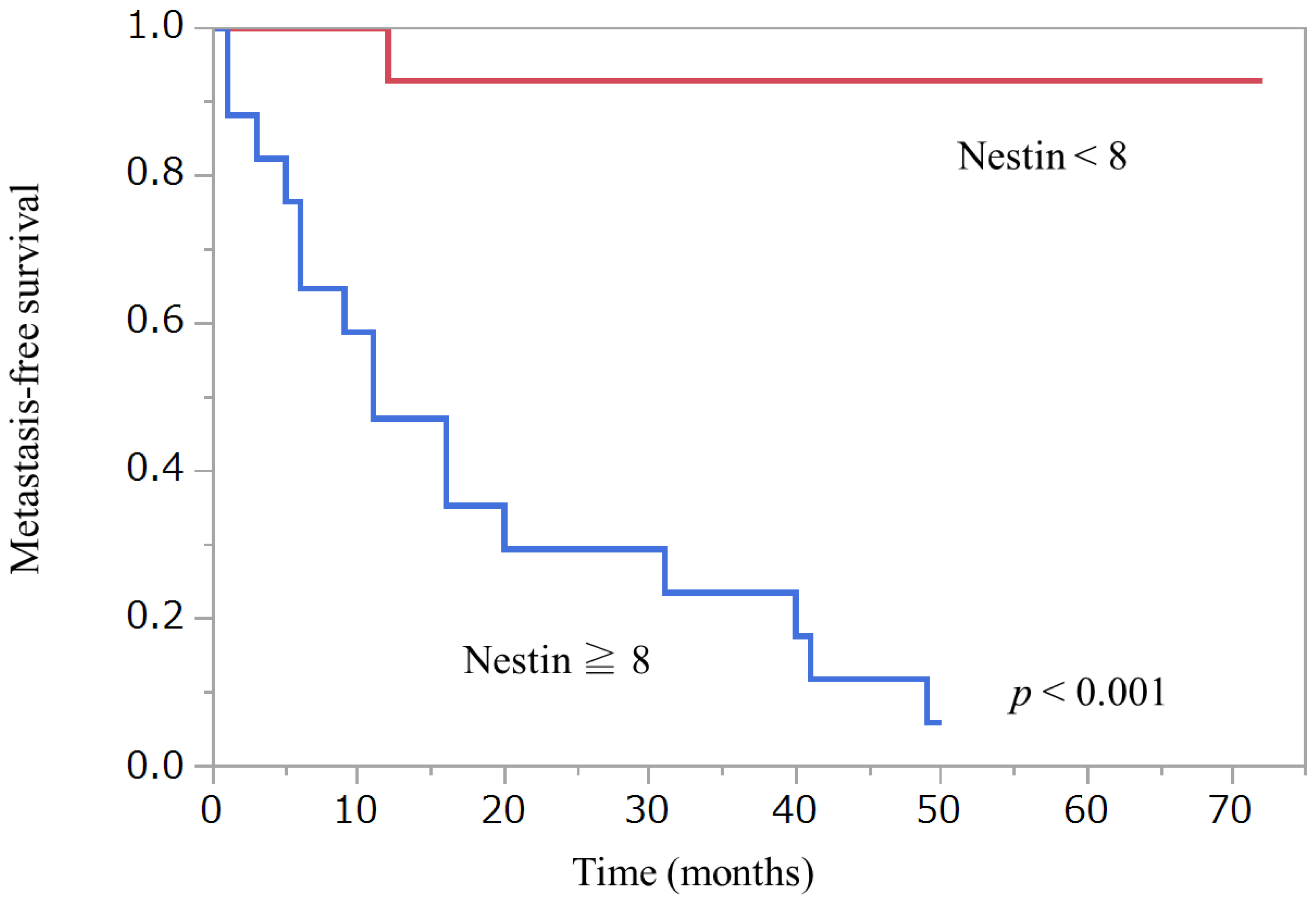
| Nestin at the primary lesion | p < 0.001 | 8 (Allred Score) |
| Case | Allred Score of Nestin | Allred Score of Fascin | ||
|---|---|---|---|---|
| Primary | Metastasis | Primary | Metastasis | |
| 7 | 8 | 8 | 8 | 8 |
| 11 | 8 | 8 | 8 | 8 |
| 16 | 8 | 8 | 2 | 8 |
| 18 | 8 | 8 | 8 | 8 |
| 20 | 8 | 8 | 7 | 8 |
| 21 | 8 | 4 | 8 | 4 |
| 23 | 8 | 8 | 8 | 8 |
| 25 | 8 | 7 | 3 | 0 |
| 27 | 8 | 2 | 6 | 2 |
| 28 | 8 | 8 | 4 | 8 |
| NS | NS | |||
| Relation with Sun-Exposure | Tissue | Body Area | Rate of Metastasis |
|---|---|---|---|
| sun-exposure melanoma (10) * | non-acral cutaneous (10) | head and neck (3) | 2/3 |
| body trunk (3) | 2/3 | ||
| limb (4) | 1/4 | ||
| nonsolar melanoma (20) | acral cutaneous (12) | finger (1) | 1/1 |
| toe (7) | 3/7 | ||
| sole (3) | 2/3 | ||
| nail head (1) | 0/1 | ||
| mucosal (8) | nasal cavity (6) | 5/6 | |
| conjunctiva (2) | 0/2 | ||
| Total (30) | 16/30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamoto, Y.; Hayashi, Y.; Sakaki, H.; Murakami, I. Evaluation of Clinical and Immunohistochemical Factors Relating to Melanoma Metastasis: Potential Roles of Nestin and Fascin in Melanoma. Diagnostics 2022, 12, 219. https://doi.org/10.3390/diagnostics12010219
Yamamoto Y, Hayashi Y, Sakaki H, Murakami I. Evaluation of Clinical and Immunohistochemical Factors Relating to Melanoma Metastasis: Potential Roles of Nestin and Fascin in Melanoma. Diagnostics. 2022; 12(1):219. https://doi.org/10.3390/diagnostics12010219
Chicago/Turabian StyleYamamoto, Yumiko, Yoshihiro Hayashi, Hideyuki Sakaki, and Ichiro Murakami. 2022. "Evaluation of Clinical and Immunohistochemical Factors Relating to Melanoma Metastasis: Potential Roles of Nestin and Fascin in Melanoma" Diagnostics 12, no. 1: 219. https://doi.org/10.3390/diagnostics12010219
APA StyleYamamoto, Y., Hayashi, Y., Sakaki, H., & Murakami, I. (2022). Evaluation of Clinical and Immunohistochemical Factors Relating to Melanoma Metastasis: Potential Roles of Nestin and Fascin in Melanoma. Diagnostics, 12(1), 219. https://doi.org/10.3390/diagnostics12010219